


ABSTRACT
Background Infection is a serious surgical complication that significantly increases morbidity and mortality rates as well as health care expenses. Increased bacterial resistance to antibiotics makes the treatment of such events even more troublesome.
Objective To report on a surgical infection case treated with ozone as a complementary therapy.
Methods and Materials A female, 65 years old, submitted to a complex surgical procedure for adult kyphotic deformity correction that presented with early postsurgical infection. The patient was treated with revision surgery and antibiotics that improved the condition but were unable to delete the infection. Ozone, in its gaseous form, was injected subcutaneously and paravertebrally twice weekly for 3 weeks.
Results After 3 weeks of treatment, the wound healed completely. Follow-up visits and laboratory exams for up to 1 year after surgery showed no recurrence of infection.
Conclusions Although just a single case, topical ozone therapy for surgical infections showed promising potential in this specific case.
INTRODUCTION
Infection is a serious and, eventually, life-threatening complication of spinal surgery with a high postoperative morbidity and mortality rate and an important increase in health care expenses.1 Literature reports indicate postsurgical infection ranging between 0.5% and 18.8%.2,3 More complex procedures, such as deformity corrections and long posterior instrumentations, bear a higher risk of infection, while low-complexity procedures, such as microscopically assisted ones, have low or very low infection rates.4,5
Surgical infections have been indicated as having 3 possible sources: an external, environmental source, originating from surgical instrumentation or theater air; an external, biological source, taking place from the skin near the incision site; and an internal source, arising from internal mucous membranes, such as gastrointestinal, genitourinary, or oropharyngeal sites of endogenous, usually chronic infections. In order to become clinically evident, infections require a sufficient bacterial load, sufficient tissue damage, and a significant lowering of immune response of the host.6,7 The most frequent pathogens giving rise to infections are the aerobic ones; however, anaerobic microorganisms were found responsible for infections in approximately 38% of cases. The scarce information on these last ones is a consequence of a more difficult and costly procedure to verify them.4,6 Indeed, it seems that the combined action of aerobic and anaerobic pathogens is frequently involved in the occurrence of the surgical infection.8
Risk factors such as obesity, diabetes, age over 60, chronic infections, prolonged operating time, blood loss, postoperative pain, anxiety, depression, and so on have been recognized as significant risk factors increasing the incidence of infection after spinal surgery.9,10 To date, there is no univocal idea on the mechanisms of infection growth. One theory favors infection as a direct mechanical effect of bacterial virulence. Others are more inclined to indicate the type of bacteria as being responsible for infection arousal.11–13
Ozone is a triatomic allotrope of oxygen with a high electrovoltaic potential. Its known bactericidal, fungicidal, and viristatic action is largely used in food and water industry.14,15 The mechanism through which it explicates the bactericidal action is believed to lie in its capacity to destroy the protein and lipid reactive sites on the cell membranes of bacteria.16 Laboratory findings indicate ozone as having high destructive potential on vegetative and planktonic forms of bacteria immersed in water and/or saline solution.17 Results on its activity on biofilms are not so univocal; however, ozone seems to have better destructive capacity than common treatment with antibiotics.18–24 Toxicological tests indicated that ozone, when applied in acute and subacute doses, does not damage biological tissue.25
This is a report on a case of resistant postoperative spine surgery infection treated successfully with the intrawound application of the gaseous form of ozone.
CASE REPORT
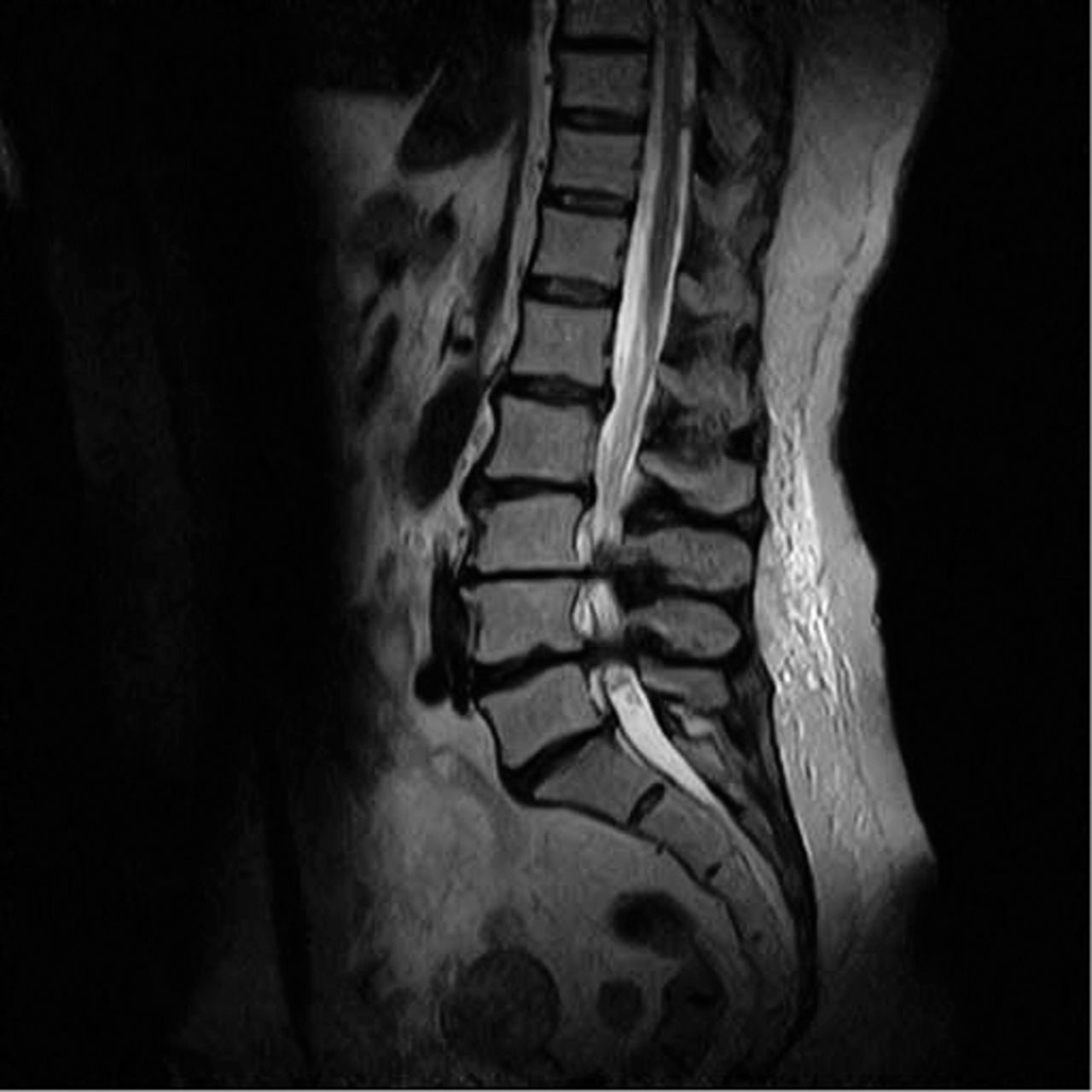
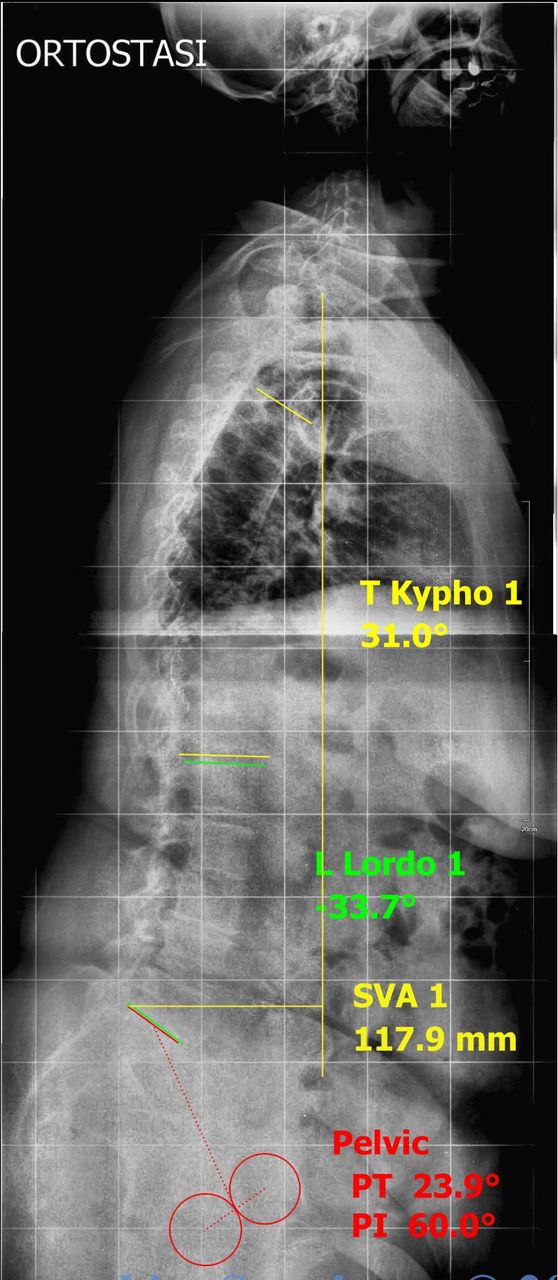
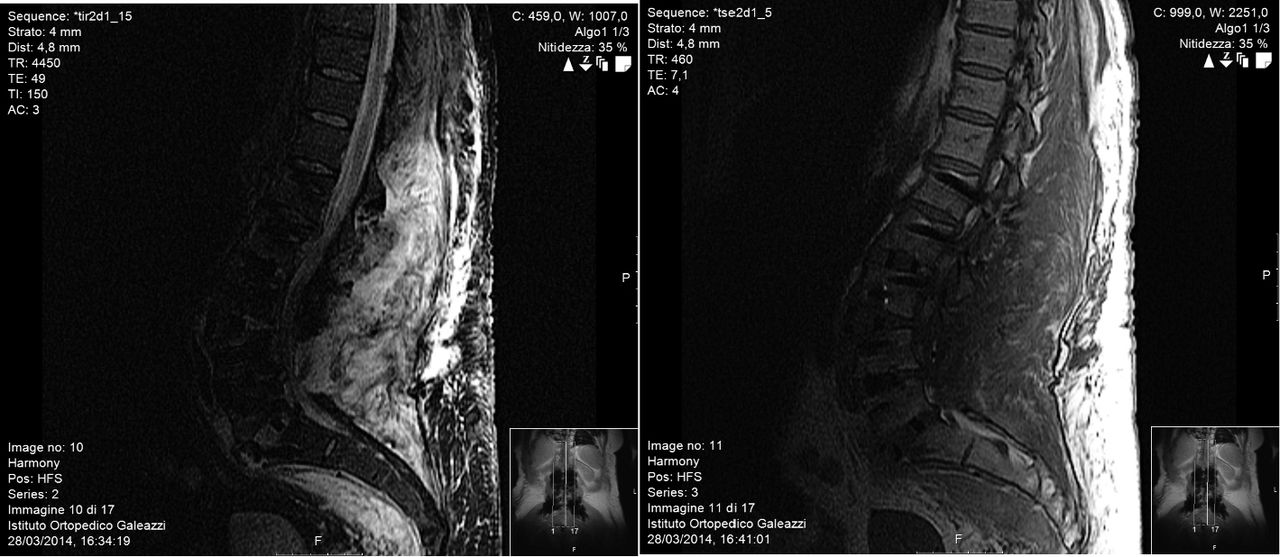
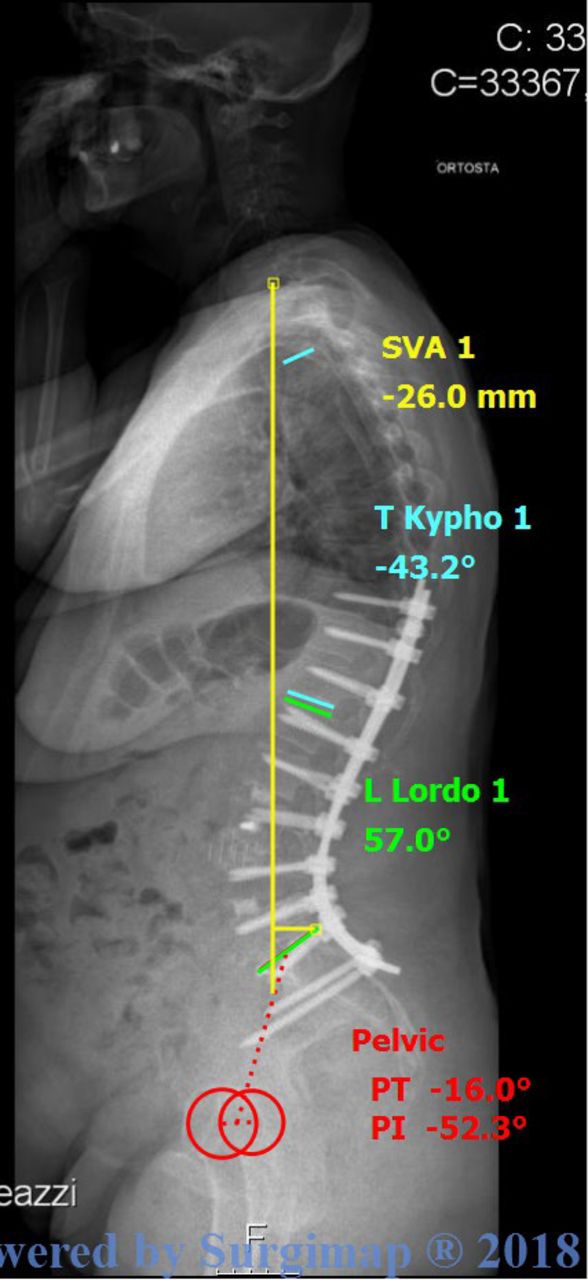
A female, 65 years of age, presented to the outpatient clinic due to progressively worsening low back pain that started 3 years before with recent radiation of pain to both of her lower extremities, mainly to the right side. Radiological examination showed a case of spinal stenosis at L3/L4 and L4/L5 levels with significant sagittal imbalance: pelvic index 60°, pelvic tilt 23.9°, lumbar lordosis 33.7°, and C7 plumb line +117.9 mm (Figures 1 and 2). The patient's body mass index was 33.06, and bone densitometry showed a t score of −0.6. No significant comorbidities or risk factors were reported. The patient was submitted to a complex spinal surgical procedure for sagittal imbalance correction and decompression. An anterior approach at L5/S1 was done with an anterior lumbar interbody fusion (ALIF) cage insertion; the patient was turned laterally, and an anterior column release lateral interbody fusion (LLIF) cage was positioned at L3/L4, obtaining approximately 30° of sagittal correction. Moreover, from the same lateral approach, another 2 lordotic LLIF cages were positioned at L4/L5 and L2/L3 levels for further improvement of the balance and anterior support to the spine. The patient was positioned prone on the Risser frame, and a decompression of the lumbar spine with pedicle screw instrumentation from the ileum up to L1 was done. On the fifth postoperative day, the patient presented with hyperthermia (39.1°C) and wound discharge. The following day, a blood culture was taken, and the result was positive for Enterococus faecalis. C-reactive protein (CRP) showed values of 16.59 mg/dL. Magnetic resonance imaging (MRI) showed diffuse inflammatory changes of the paravertebral muscles and localized collections (Figures 3 and 4). Due to the previously mentioned findings, a revision surgery with debridement was done. During the surgery, a loosening of the upper screws was found, and an extension of the instrumentation up to D10 was performed (Figure 5). Multiple tissue swabs taken during the surgery confirmed the results of the blood culture test. The infectious disease specialist advised the following treatment: ampicillin 3 g 4 times per day and gentamicin 320 mg per day. After 15 days and significant improvement in health conditions, the medication was changed to augmentin 1 g 3 times per day. On discharge from the hospital, the patient's blood values showed a significant reduction of inflammatory markers: white blood cells 4790 mL/L and CRP 3.28 mg/L.

Preoperative T2 weighted sagittal magnetic resonance images.
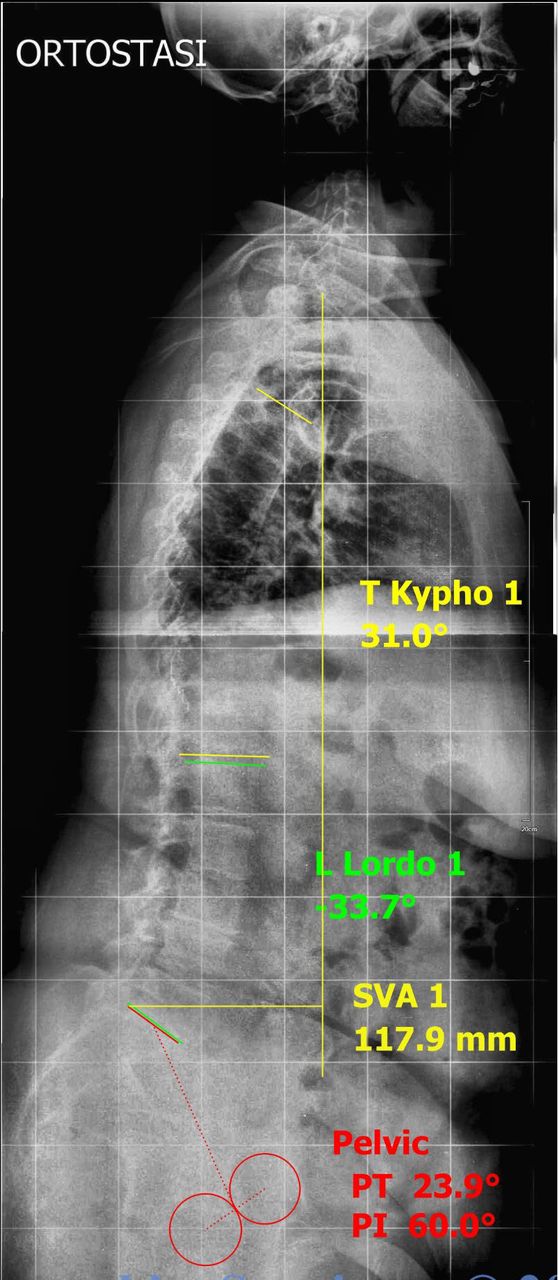
Preoperative x-ray.
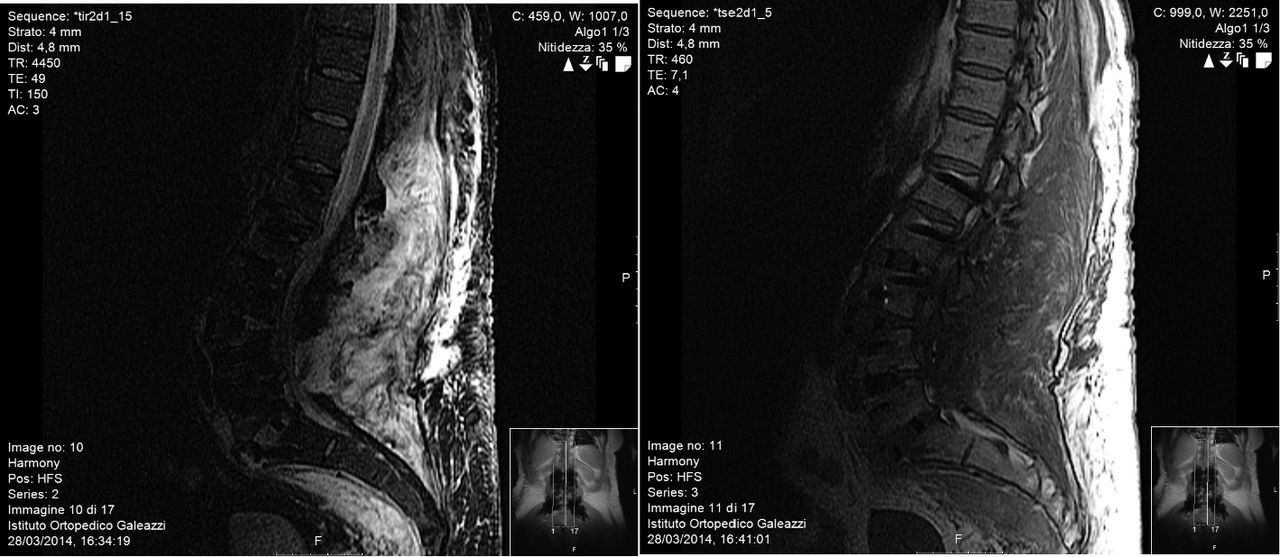
Postoperative T2 and short-TI inversion recovery weighted sagittal magnetic resonance images.

Postoperative x-ray.
On discharge, the patient continued with the antibiotic treatment and was followed closely with weekly outpatient visits. The surgical wound healing was not optimal, as 2 wound fistulas were still discharging yellowish, dense liquid. The wound continued to show redness and tenderness. More than a month after discharge from the hospital, the CRP values remained high (3.5 mg/dL), and the wound drainage fistulas continued discharging. The patient started showing general health deterioration with severe fatigue and loss of appetite. Before proceeding with a new revision surgery, a decision was made to try ozone therapy, as it has known bactericidal effects. An oxygen-ozone mixture in gaseous form was injected inside the wound with the following modality: The procedure was done in outpatient clinic with the patient lying in lateral decubitus. A 16-gauge cannula was inserted inside the fistula, and the syringe suction was applied to remove the subcutaneous liquid collection. Approximately 120 mL of yellowish and dense liquid was removed. Using a 60-mL syringe, an ozone-oxygen mixture in a concentration of 20 μg of ozone/mL of oxygen was injected into the subcutaneous space. Eight syringes were applied for a total of 480 mL. Then another two 60-mL injections were introduced deep inside the paravertebral muscles using 20-gauge, 7-cm needles. These procedure was repeated twice weekly for 2 weeks and then again once in the third week. Already during the second week of treatment (third treatment), the wound presented in significantly better condition. The fistulas were still open, but the secretion although still yellowish was no longer dense. There was no more redness of the wound, and back pain diminished significantly. At the last session, the patient presented in much better general health condition with significantly less pain and fatigue compared to the first session. The previously described fistulas were completely closed, so we had to puncture the skin for the last session. No more collection could be found even on suction. The skin around the wound was flat, and redness was no longer seen. The patient repeated her blood exams for inflammatory markers a week after the last session, and these showed normal values (CRP 1 mg/dL, pro-calcitonin < 0.05 μg/L).
The patient was followed up for a period of 1 year, during which repeated blood exams, initially done once monthly for 2 months and then at 6 and 12 months, showed no laboratory signs of infection.
DISCUSSION
Due to the rise of multiresistant bacteria and a decrease in the effectiveness of antibiotics, nosocomial infections are becoming a serious concern.26,27 Consequently, alternative treatment methods of traditional and complementary medicine have been brought back in use. Ozone has become part of the complementary medicine and is widely used for the treatment of different medical conditions, among which are the treatment of bacterial, viral, and fungal infections.28 Ozone causes inactivation of bacteria, viruses, fungi, yeast, and protozoa. It disrupts the integrity of the bacterial cell envelope by oxidation of phospholipids and lipoproteins. Ozone, at a low concentration of 0.1 ppm, is sufficient to inactivate bacterial cells, including their spores. Basic research from Italy and Cuba led independently to the findings that ozone application can modulate the immune system, balancing its inflammatory/anti-inflammatory cytokines and stimulating 2,3-diphosphoglycerate, leading to an increase in the amount of oxygen released to the tissues. Ozone activates the Krebs cycle by enhancing oxidative carboxylation of pyruvate and stimulating the production of adenosine triphosphate. It also causes a significant reduction of nicotinamide adenine nucleotide and helps to oxidize cytochrome c. There is stimulation of production of enzymes that act as free radical and cell wall protectors: glutathione peroxidase, catalase, and superoxide dismutase.29,30 Recently, reports were published on the human body being able to generate ozone as part of its oxidative armamentarium in fighting infection.31
The applied concentration of the ozone-oxygen mixture that the authors chose was based both on the fact that even the lowest doses of ozone do react positively on bacteria and on the authors' experience of ozone usage for paravertebral injection in other medical conditions, such as low back pain, sciatica, or neurogenic claudication. The frequency of the ozone application deemed to be sufficient was based on an empirical judgment of wound improvement.
This case illustrates a severe and resistant postsurgical infection treated initially with revision surgery and a prolonged regime of antibiotics. Nonetheless, only partial healing was obtained. Adding the ozone to the treatment took over the “status quo” situation and switched the patient on the healing side of the process. Of course, the ongoing antibiotics and the repeated evacuation of subcutaneous purulent fluid prior to every ozone application could also have been one of the factors that influenced the wound healing. The possibility that the ozone might have increased the activity of the antibiotics on bacteria is also an option. Data show that preconditioning of the antibiotics with ozone does increase their bactericidal capacity.32
Experimental work of different authors indicates that ozone is a highly active bactericidal substance in vitro on both vegetative and planktonic forms of bacteria. It also seems to show superior results in the treatment of biofilms as compared to antibiotics.17,19–24 Ozone therapy for infections seems to have similarities with hyperbaric oxygen treatment. Animal studies comparing these 2 modalities in acute pancreas infection showed positive results for both treatments with a clear prevalence for ozone therapy.33 Literature review found a few published articles on the use of ozone for the prevention and treatment of surgical infections in clinical settings.34,35 The authors state that ozone treatment of infections showed promising results and indicate ozone as having a possible role in prevention of surgical infections as well.
Of course, a single case is not a proven demonstration of clinical benefit; however, it possibly indicates a new complementary treatment modality that is worthwhile to explore, particularly in the era of ever-growing bacterial resistance to antibiotics.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2019 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.