


ABSTRACT
Background: Giant pseudomeningoceles are an uncommon complication of spine surgery. Surgical management and extirpation can be difficult, and guidelines remain unclear.
Methods: Here, we present a 56-year-old female patient with a history of grade III L5–S1 spondylolisthesis who was treated with 2 prior spine surgeries. The patient was treated with bone grafting for pseudarthrosis and instrumentation from L4 to ilium. After unsuccessful intraoperative and postoperative cerebrospinal fluid drainage and dural repair, the patient presented to the emergency room with debilitating positional headaches.
Results: The patient underwent dural repair with bovine pericardial patch inlay sutured with 7-0 prolene, blood patch, and a dural sealant. Plastic surgery performed a layered closure, using acellular dermal matrix over the dural closure. The bilateral paraspinal flaps were advanced medially to cover the entirety of the acellular dermal matrix, and the fasciocutaneous flaps were then advanced to the midline for a watertight closure. At 3-month follow-up, the patient was headache free and had returned to her activities of daily living.
Conclusions: We conclude that early consultation with plastic surgery can be greatly beneficial to effectively extirpate dead space and resolve giant sacral pseudomeningoceles, especially if there is concern of persistent cerebrospinal fluid leakage due to relatively immobile avascular soft tissue as a result of prior revision surgery.
- giant pseudomeningocele
- durotomy
- pseudomeningocele
- management of pseudomeningocele
- revision surgery
- postural headaches
- positional headaches
INTRODUCTION
A pseudomeningocele is an extravasation of cerebrospinal fluid that occurs due to an abnormal communication between the dural-arachnoid layer and extradural tissues. The cause of pseudomeningoceles has been described as congenital, traumatic, and iatrogenic, with the most common being iatrogenic.1–4 Although potentially asymptomatic,3,5–7 pseudomeningoceles have been reported with a multitude of symptoms, including postural headaches, intermittent back pain, muscle spasm, radicular syndromes, tinnitus, photophobia, neck stiffness, and nausea and vomiting.3,4,8–11
The prevalence of pseudomeningoceles following spine surgery has not been clearly established and can potentially be underestimated, as asymptomatic patients may go underreported and perhaps are discovered only incidentally during revision surgeries.3,6 Swanson et al12 reported a .07% prevalence following a review of 1700 postlaminectomy patients in 1946, while Teplick et al7 reported a 2% prevalence following a review of 400 symptomatic postlaminectomy patients in 1983. Iatrogenic pseudomeningoceles have been related to incidental durotomy as a complication of spine surgery. While the occurrence of durotomy has been reported as up to 5% in primary surgeries and 17% in revision procedures,13–16 little is known about the etiology and risk factors behind the progression to a pseudomeningocele. The higher incidence in the lumbosacral region is thought to be a consequence of the greater frequency of lumbar operations relative to other regions of the spine as well as postoperative increases in intrathecal pressures in the lumbar region.3,17,18 These factors can contribute to an unresolved durotomy that, along with a potentially asymptomatic and clinically unmanaged period, can contribute to the progression to a giant pseudomeningocele.19
We present here a case study on the management of a giant (>8 cm20) iatrogenic sacral pseudomeningocele, resulting from dead space from multiple spinal operations and persistent cerebrospinal fluid (CSF) leakage despite multiple attempted primary repairs.
CASE REPORT
Presentation
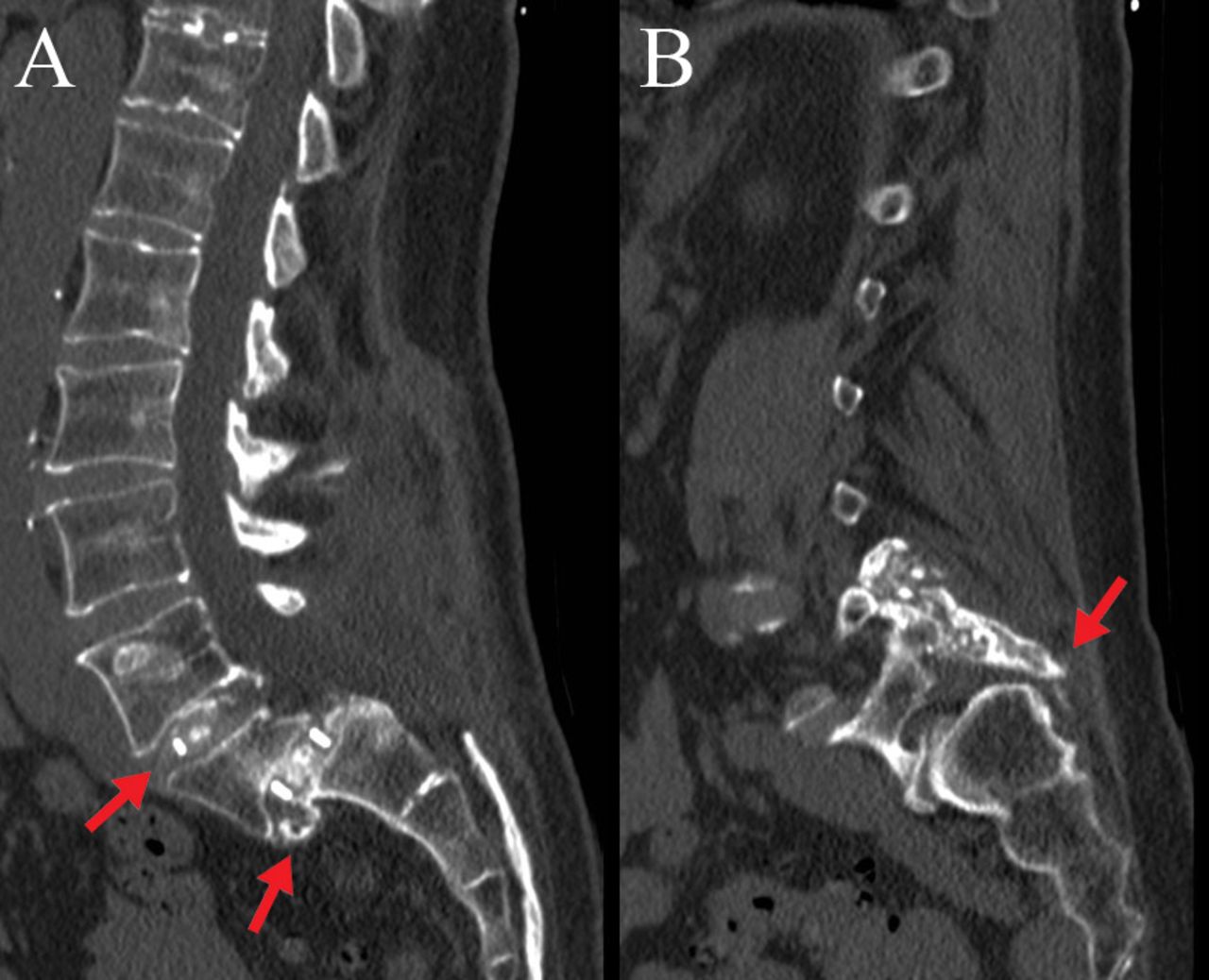
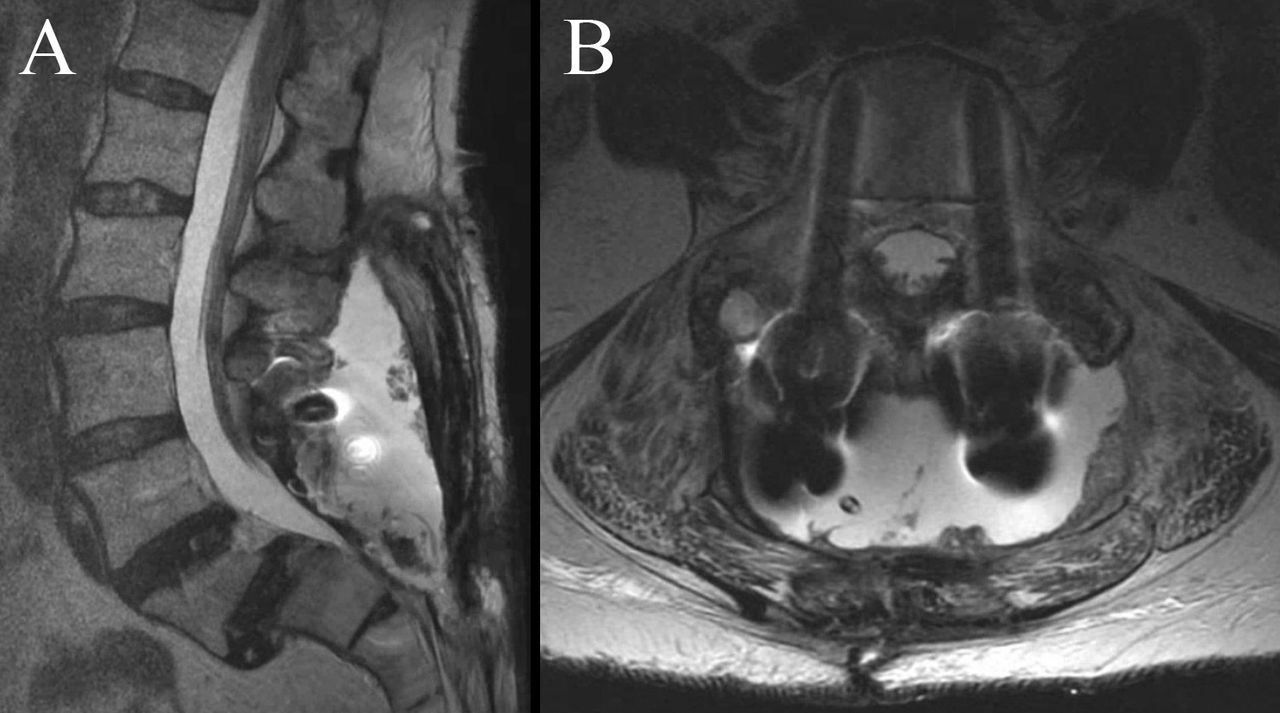
A 56-year-old female presented with a history of a grade III L5–S1 spondylolisthesis treated with 2 prior spine surgeries at an outside hospital. The first surgery was an L4–S1 full laminectomy, L4–L5 and L5–S1 transforaminal lumbar interbody fusion, and L4–ilium posterior spinal instrumentation and fusion. Due to a postoperative radiculopathy from pedicle screw malpositioning and concerns of prominence of her distal construct, her instrumentation was removed 8 months later during a second surgery. She presented more than 1 year after her index surgery with chronic low back pain and was found to have a pseudarthrosis at her prior surgical site (Figure 1). The surgical plan at this time was placement of instrumentation from L4 to ilium with additional bone grafting to treat the pseudarthrosis. Preoperative magnetic resonance imaging demonstrated a likely small pseudomeningocele above her sacral laminectomy (Figure 2).
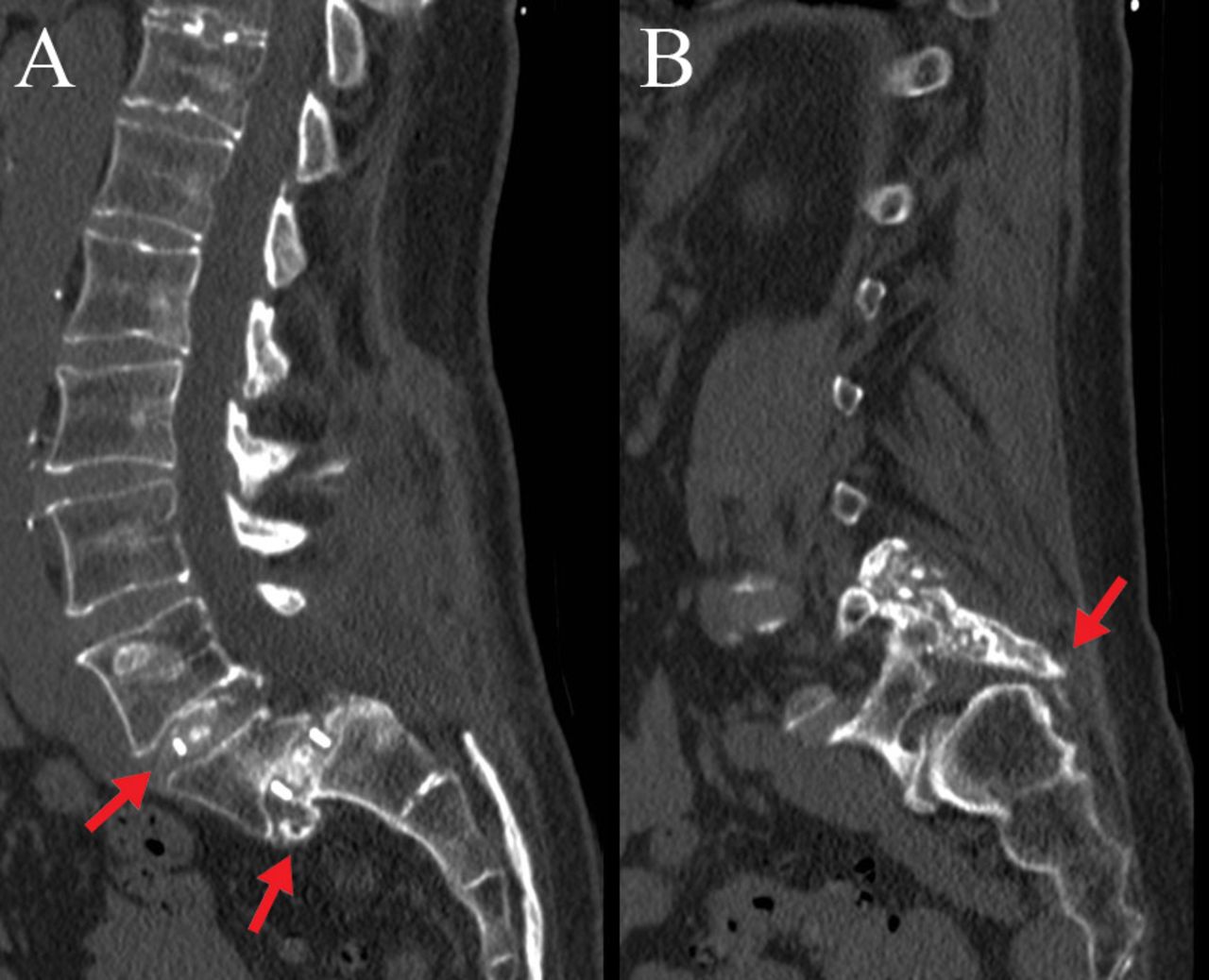
Computed tomography showing (A) sagittal and (B) parasagittal views of pseudarthrosis and failure of fusion.
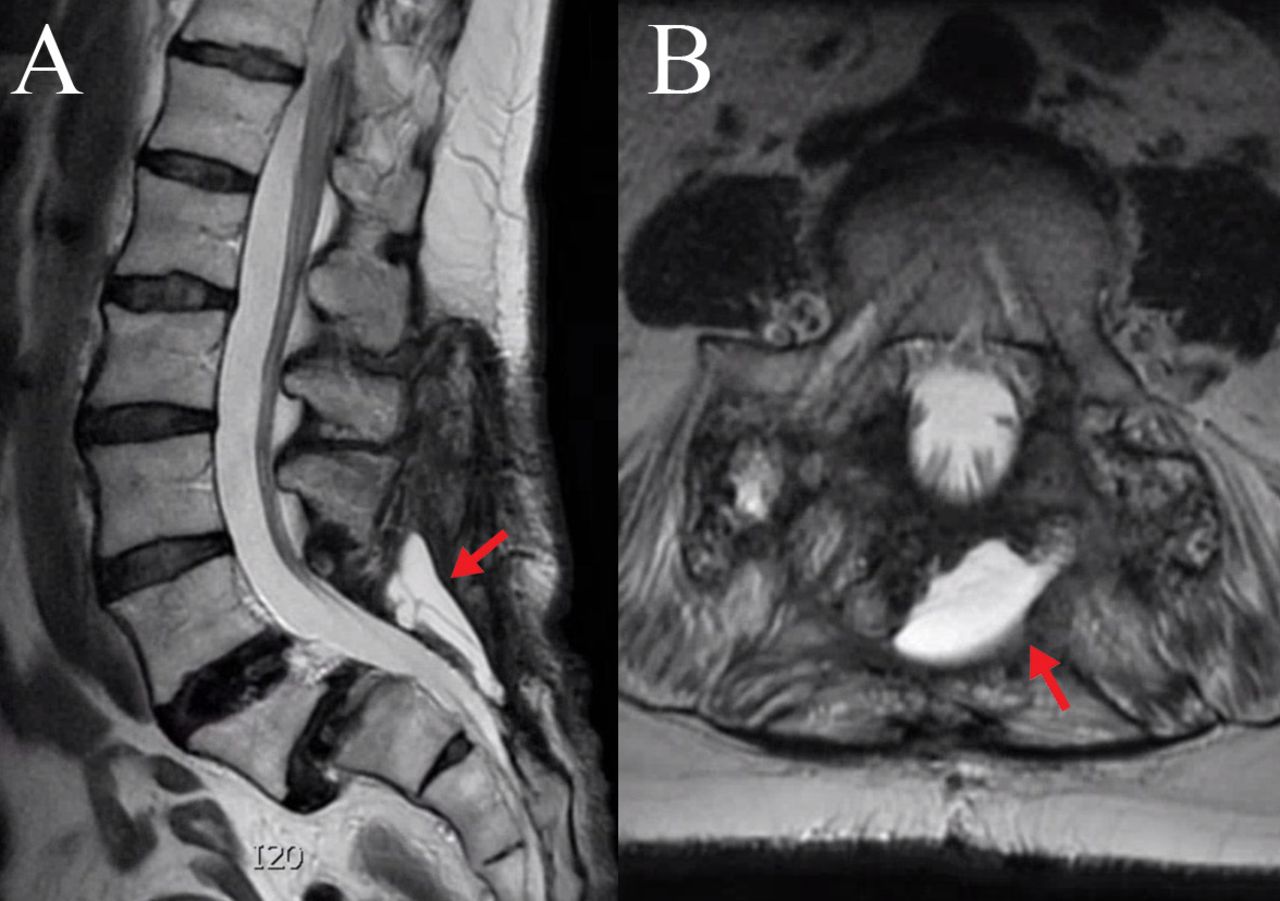
Magnetic resonance imaging showing (A) sagittal and (B) axial views of a small pseudomeningocele associated with the patient's initial surgeries.
Intraoperatively, on exposure of the dorsal sacrum, the fluid collection was identified and qualitatively appeared to be CSF. A suture line was seen at the dorsal sacral dura, indicative of a prior durotomy repair, and a small persistent pinhole leak was noted at the distal suture line at the S2 dura. This was repaired primarily with a 6-0 prolene suture in a cruciate stitch, and a Valsalva to 40 mm Hg confirmed no further leak. An additional onlay of a dural matrix substitute, surgical soaked in blood as a blood patch, and a dural sealant were applied. After instrumentation and bone grafting, multilevel closure proceeded in usual fashion. Due to her prior spine surgeries, it was noted that her paraspinal musculofascial soft tissue was stiff. Although the fascia was reapproximated well, the underlying muscle could not be brought together, leaving known dead space above the bony spine.
Within several days postoperatively, she complained of severe positional headaches that she had never experienced before. Due to a high suspicion of a persistent CSF leak, she was brought back to the operating room for repair. CSF was visualized within the wound emanating from the same dural defect. This was repaired again with a dural substitute inlay, 7-0 prolene suture, Surgicel soaked in blood as a blood patch, a muscle graft onlay, and a dural sealant. The wound was again closed at the level of the fascia, and the patient was kept flat in bed for 2 days. Her headaches improved, and she was discharged.
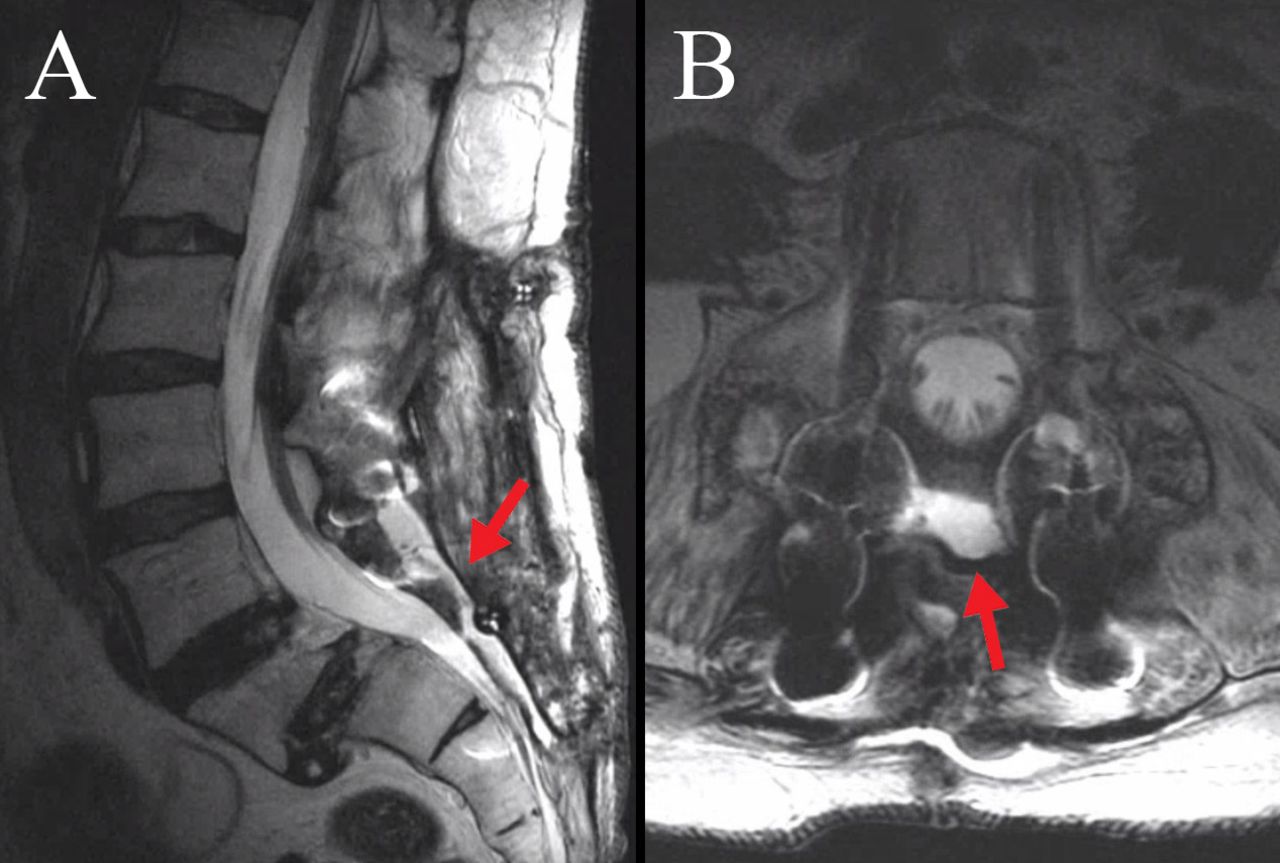
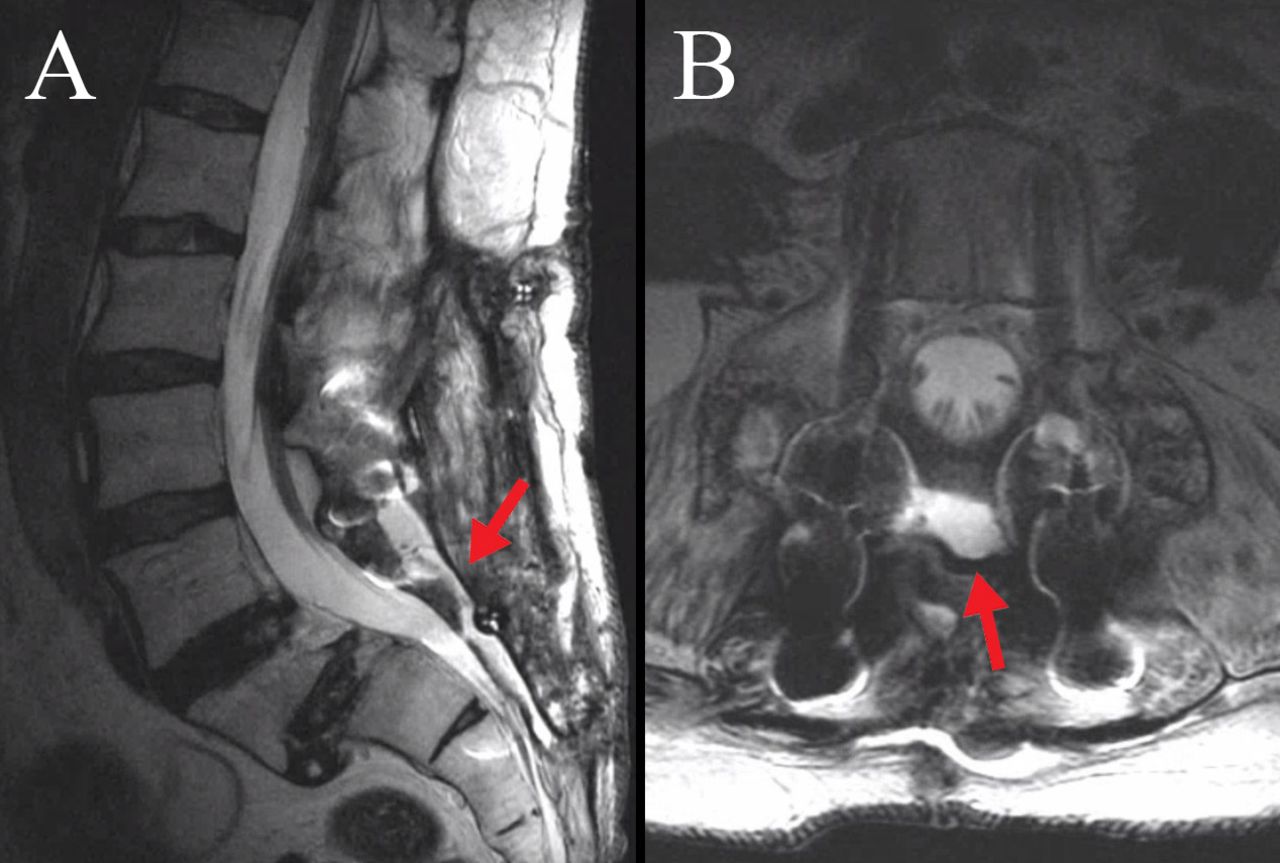
She returned to the emergency room due to debilitating positional headaches. Magnetic resonance imaging (MRI) demonstrated a giant sacral pseudomeningocele measuring 10.5 × 7.8 × 3.5 cm (Figure 3). She was again brought back to the operating room for placement of a lumbar drain and another attempted direct repair of the S2 dura with a dural substitute inlay, 7-0 prolene suture, dural substitute onlay, Surgicel soaked in blood as a blood patch, and a dural sealant. She was kept flat in bed for 5 days total, and 10 cc of CSF was removed from the lumbar drain every hour for the entirety of those 5 days. On release of her bed rest, she continued to complain of positional headaches, and a repeat MRI demonstrated recurrence of her giant sacral pseudomeningocele. It was determined at this point that her soft tissue dead space was accumulating from the slow CSF leak and that plastic surgery was required to elevate and mobilize the muscle soft tissue to extirpate this dead space and reduce its volume.

Magnetic resonance imaging showing (A) sagittal and (B) axial views of a giant sacral pseudomeningocele originating from a failure primary repair of the sacral durotomy.
Surgical Technique
The patient was brought back to the operating room. A new lumbar drain was placed, and the dura was repaired with a bovine pericardial patch inlay sutured with 7-0 prolene, Surgicel soaked in blood as a blood patch, and a dural sealant. A Valsalva to 40 mm Hg confirmed no leak and no other site of CSF leakage.
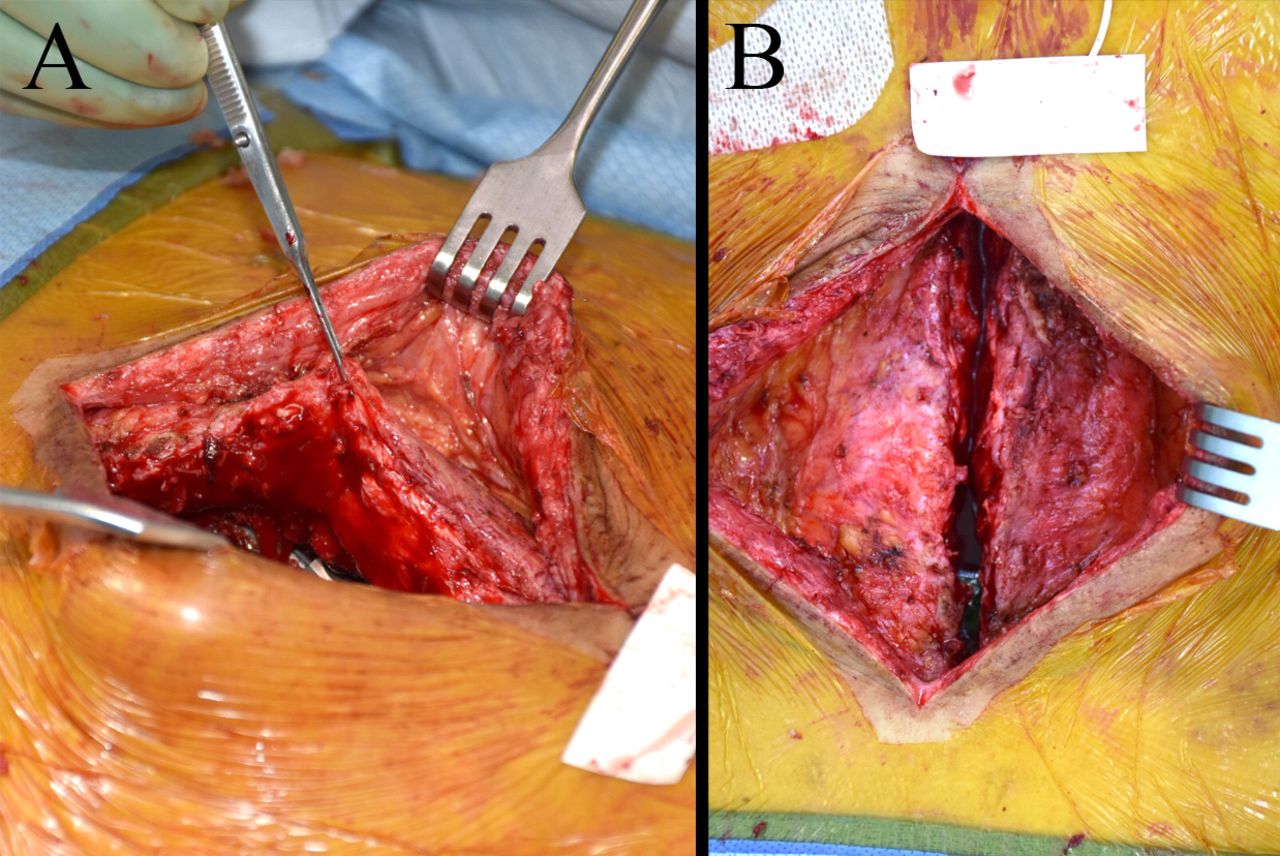
Plastic surgery then elevated paraspinous flaps by elevating the fasciocutaneous flaps superficially, divided the thoracolumbar fascia, and then elevated the paraspinous muscles off the transverse processes of the spine. This allowed for their advancement and preparation for subsequent layered closure (Figure 4). An acellular dermal matrix was then laid over the dural closure to cover the exposed bony spine and instrumentation. The bilateral paraspinal flaps were then advanced medially to cover the entirety of the acellular dermal matrix, and the fasciocutaneous flaps were then advanced to the midline for a watertight closure. The rest of the wound was closed in usual fashion.
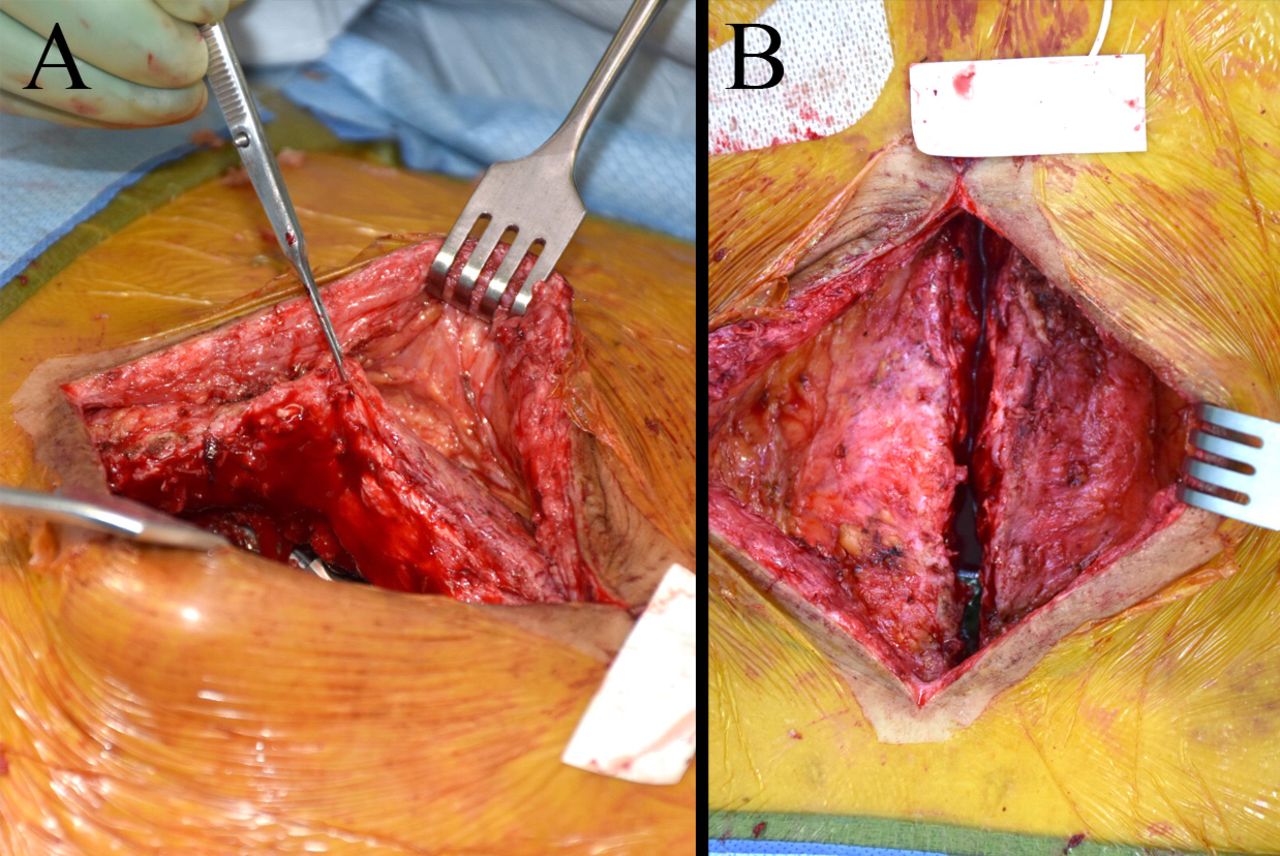
(A) Elevation of the fasciocutaneous flaps by plastic surgery. (B) Extirpation of the deep dead space and advancement of soft tissue for watertight closure.
Postoperative Course
She was kept flat in bed again for 5 days total, and 12 cc of CSF was removed from the lumbar drain every hour. On liberalization of her activity, she had no further return of her positional headaches. A repeat MRI showed significant resolution of the pseudomeningocele filling a small sheet of potential space, which now only measured 5.8 × 1.3 × 0.6 cm (Figure 5). She was subsequently discharged. At 3-month follow-up from this giant pseudomeningocele repair, she continues to be headache free and has returned to her usual activities of daily living.
Magnetic resonance imaging showing (A) sagittal and (B) axial views showing resolution of the giant sacral pseudomeningocele after primary repair, temporary cerebrospinal fluid diversion, and soft tissue mobilization and dead space extirpation by plastic surgery.
DISCUSSION
Pseudomeningoceles greater than 5 cm have been characterized as “large,” while those greater than 8 cm are characterized as “giant.”20,21 There are few reports and no definitive recommendations on management of giant pseudomeningoceles, particularly in patients who undergo revision operations.4,18–20,22 Some have reported spontaneous resolution of giant pseudomeningoceles, potentially through slow healing of the dural tear and gradual reabsorption of extradural CSF.18 Solomon et al18 report on 2 patients with giant pseudomeningocele who achieved resolution with no surgical intervention ranging in follow-up time from 3 months to 3 years and thus recommend conservative management with observation for infection and recurrence or worsening of symptoms.
Others advocate immediate surgical intervention to extirpate the pseudomeningocele and close the abnormal dural openings.3,19,20 Multiple successful interventions for dural tears have been described, including the use of blood patches,23 watertight sutures,18,20 fibrin glue,3,24,25 and fascial grafts.3,18,19 Misra et al21 demonstrated success with myofascial advancement of lumbar paravertebral muscles in 12 patients with large pseudomeningoceles. Furthermore, a Valsalva maneuver can be used to assess the success of an intervention or the presence of an abnormal opening in the dura.3,20,26 The best method for CSF drainage accompanying surgical management of iatrogenic pseudomeningoceles remains unclear; some have reported resolution with continuous drainage through placement of lumboperitoneal shunts.27,28
Weng et al20 report using a subarachnoid catheter following extirpation and closure of dural tear with a watertight suture or fascial graft. They report complete success in 11 symptomatic patients with a giant pseudomeningocele, 9 of which were in the lumbosacral region. The most common symptoms reported where neck and back pain (64%), headaches (55%), and nausea and vomiting (36%).20 All patients had an initial operation for disc herniation or spinal stenosis and thus had an associated risk of incidental durotomy between 5% and17%.13–16 The average time of follow-up was 50.6 days.20 Sirlomask et al19 suggest nonsurgical treatment in asymptomatic patients and use of subarachnoid catheter in mildly symptomatic patients; they conclude that extirpation and dural repair should be reserved for patients with severe symptoms or those with persisting symptoms beyond several weeks postoperation.
We present this unique case to highlight the difficulty of sacral dural repair despite multiple technical maneuvers. Although there have been many technical reports on the correction of giant pseudomeningoceles, the difficulty with its resolution in this case proved to be a combination of frail sacral dura in the context of prior revision surgery. Extirpation and obliteration of the dead space by plastic surgery in addition to the aggressive dural repair and CSF diversion during recovery was the lasting and durable solution. Although some have advocated for lumboperitoneal shunts, we did not believe that a lumboperitoneal shunt would be successful in our case, as the dead space in the patient's wound was increasing her total CSF volume, and diversion away from that stiff dead space would not have resolved the wound. In addition, her primary complaint of debilitating low-pressure headache affecting all aspects of her quality of life would have likely persisted and worsened.
We present here a case of a persistent giant sacral pseudomeingocele in the setting of prior revision spine surgery, treated with primary repair, aggressive temporary CSF diversion, and soft tissue extirpation by plastic surgery. We recommend early consultation with plastic surgery if there is a concern for sacral durotomy in the setting of avascular soft tissue that is difficult to mobilize to help prevent complications associated with persistent CSF leakage, pseudomeingocele, and return to the operating room for revision surgery.
Footnotes
Disclosures and COI: There were no conflicts of interest or sources of funding for this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.