


ABSTRACT
The sacroiliac joint is a complex, variable, and irregular structure, thought to be the source of 15% to 30% of low back, pelvic, and radicular pain. Several predisposing factors, including prior spinal surgery and particularly lumbar fusion, can contribute to joint inflammation and acceleration of joint degeneration. Evaluation of the sacroiliac joint as a pain generator using history and physical alone can prove difficult, because a number of other pathologies can have a similar presentation. Whereas a number of tests are used to examine the joint, no single test alone has proven validity. Imaging alone has also not been proven efficacious, particularly in nonspondyloarthropathy-mediated pain. Although no “gold standard” exists, diagnostic sacroiliac joint block has been shown to be a useful confirmatory tool in assessing sacroiliac (SI) joint–mediated pain. Sacroiliac joint injection with local anesthetic and steroids can be used as a possible therapeutic endeavor to manage pain and inflammation.
ANATOMY AND BIOMECHANICS
The SI joint is a C-shaped joint that connects the spine to the pelvis, aiding in transmission of forces to the lower extremities. It is a diarthrodial joint, considered to be synovial, although only the inferior third of the SI joint demonstrates characteristics similar to a traditional synovial joint, whereas the superior portion of the joint is closer to the cartilaginous articulation of a symphysis.1 Although its motion is complex, the 2 most common types of SI joint movement are nutation and counternutation: flexion or extension of the sacrum with counterrotation of the ilium. The degree of rotation is small,2 only up to 4°. Whereas the exact pattern of innervation of the joint is unclear, studies have shown the presence of both periarticular and intra-articular nociceptive elements, supporting the view that the central nervous system receives painful stimuli from the joint.3–5
PATHOPHYSIOLOGY
Low back pain is extremely common, affecting an estimated 70% of people during their lifetime.6 The estimated rates of low back pain attributable to the SI joint is between 15% and 30%.7,8 The proposed mechanism of injury to the SI joint is likely a combination of axial loading and rotation. The etiologies of SI joint–mediated pain include intra-articular pathology such as arthritis and spondyloarthropathy as well as extra-articular pathology such as ligamentous or muscular injury or enthesopathy. Factors predisposing patients to SI joint–mediated pain include leg-length discrepancy, transitional anatomy, scoliosis, persistent strain or low grade trauma, pregnancy, and spine surgery.9 Increased stress across the SI joint has been demonstrated by Ivanov et al10 using simulated surgical methods and is supported by computed tomography (CT) imaging evidence of accelerated SI joint degeneration in patients undergoing lumbosacral fusion when compared with matched controls.11
PHYSICAL EXAMINATION
Due to the overlapping pain patterns among the lumbar spine, SI, and hip joints, it is often difficult to clinically differentiate these pathologies. Fortin's mapping of SI joint pain pattern in asymptomatic individuals using diagnostic injection demonstrated an area within the buttock measuring 10 cm inferior and 3 cm lateral to the posterior superior iliac spine,12 but this area is also common to pain originating from the lumbar spine. No single physical exam technique or test has been shown to accurately identify SI joint pain. A thorough examination should include evaluation of the lumbar spine and hip as potential sources of pain. There are a number of maneuvers used to evaluate SI joint pain including the FABER (flexion, abduction, and external rotation), thigh thrust, pelvic distraction, pelvic compression, and pelvic torsion (Gaenslen) tests. Although no single test alone is specific for SI joint–mediated pain, if 3 of the 5 tests are positive, there is an 85% pretest probability of a positive diagnostic injection.13
IMAGING
In contrast to lumbar spine or hip imaging, specific imaging of the SI joint has not been shown to be efficacious in accurately correlating with SI joint–mediated pain. Computed tomography of the SI joint, often used to evaluate the degenerative changes, has been shown to have a sensitivity of 57.5% and specificity of 69% in patients with SI joint–mediated pain.14 Radionuclide imaging has higher specificity rates but low sensitivity.15,16 Magnetic resonance imaging (MRI), although 90% sensitive for evaluating sacroiliitis in spondyloarthropathies, is not as sensitive in evaluating the symptomatic nonspondyloarthritic SI joint.17 In addition, degenerative changes can often be seen in asymptomatic individuals, and SI joints proven to be inflamed and symptomatic with blockade often appear normal on imaging studies. Computed tomography and MRI are beneficial in excluding other causes, such as malignancy, infection, and fracture.
DIAGNOSTIC INJECTION
Whereas there is no true “gold standard” for SI joint–mediated pain, many clinicians use image-guided intra-articular blockade with local anesthetic to exclude or confirm clinically suspected SI joint symptomatology because it is target specific. The injections can be performed using fluoroscopy, CT, and even MRI or ultrasound. Sacroiliac joint injections without image guidance, also known as “blind” injections, are not recommended because studies demonstrated that intra-articular injection of the joint occurred in only 22% of these patients, with epidural or dorsal sacral foraminal flow demonstrated 24% and 44% of the time, respectively.18
The technique for injection with fluoroscopic guidance is as follows:
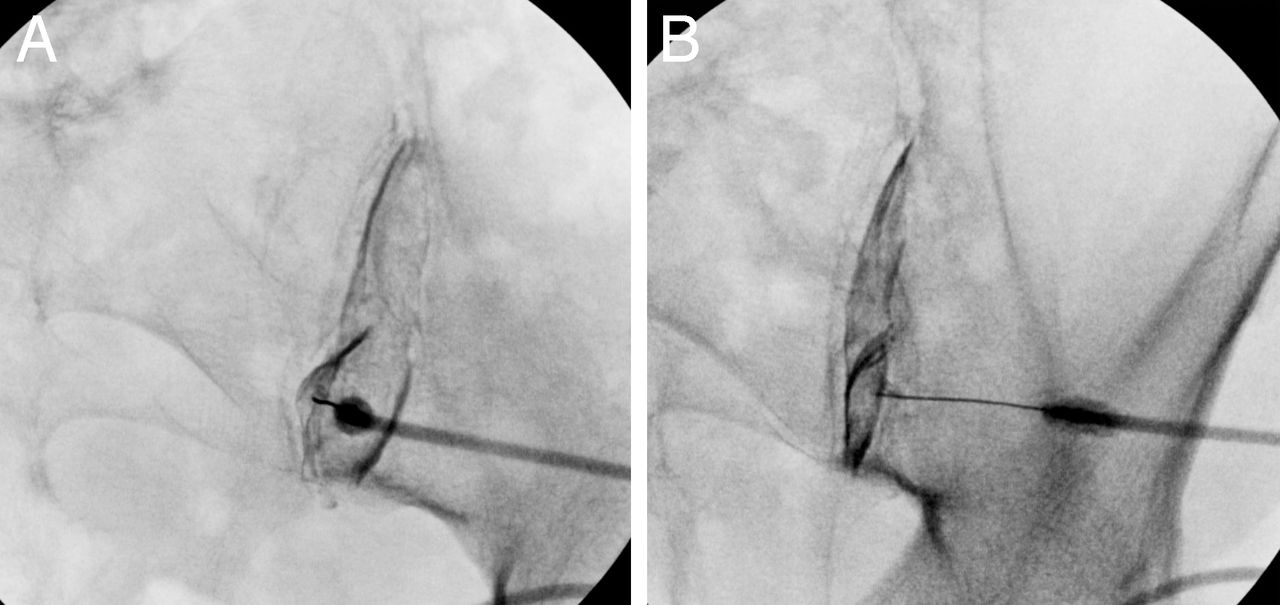
After informed consent, the patient is placed in the prone position. Using fluoroscopic guidance the SI joint is identified and the inferior corner of the joint, where we have found the joint to be most accessible to needle placement, is marked under the fluoroscopy. The area is sterilely prepped and draped. The skin may or may not be anesthetized with local anesthetic. The inferior third of the joint is accessed using a small-gauge (22- or 25-gauge) spinal needle. Intra-articular confirmation is performed via injection of a small amount of iodinated contrast under direct live fluoroscopy (Figure 1). Local anesthetic, with or without anti-inflammatory steroid, is then injected into the joint. The SI joint, though having a surface area of 17.5 cm2, has a small capacity ranging from 0.8 to 2.5 mL in asymptomatic individuals and 1.0 to 2.7 mL in symptomatic individuals.19,20 It is generally advised21 not to inject a total volume greater than 2.5 mL, because extravasation from the joint can leak onto nearby neural structures and compromise the target specificity of the injection. It is common to provoke a mild pain sensation during the therapeutic injection. This can be assessed regarding concordant or nonconcordant relation to the clinical pain being investigated. Fluoroscopy is most commonly used due to availability and cost, but the same procedure can be performed under CT (Figure 2), particularly if one is unable to access the joint via fluoroscopy due to the presence of dorsal marginal osteophytes (Figure 3). Injection under MRI or ultrasound could be considered, particularly if the injection must be performed in a pregnant individual. Regardless of imaging modality, there should be documentation that the injection is intra-articular.
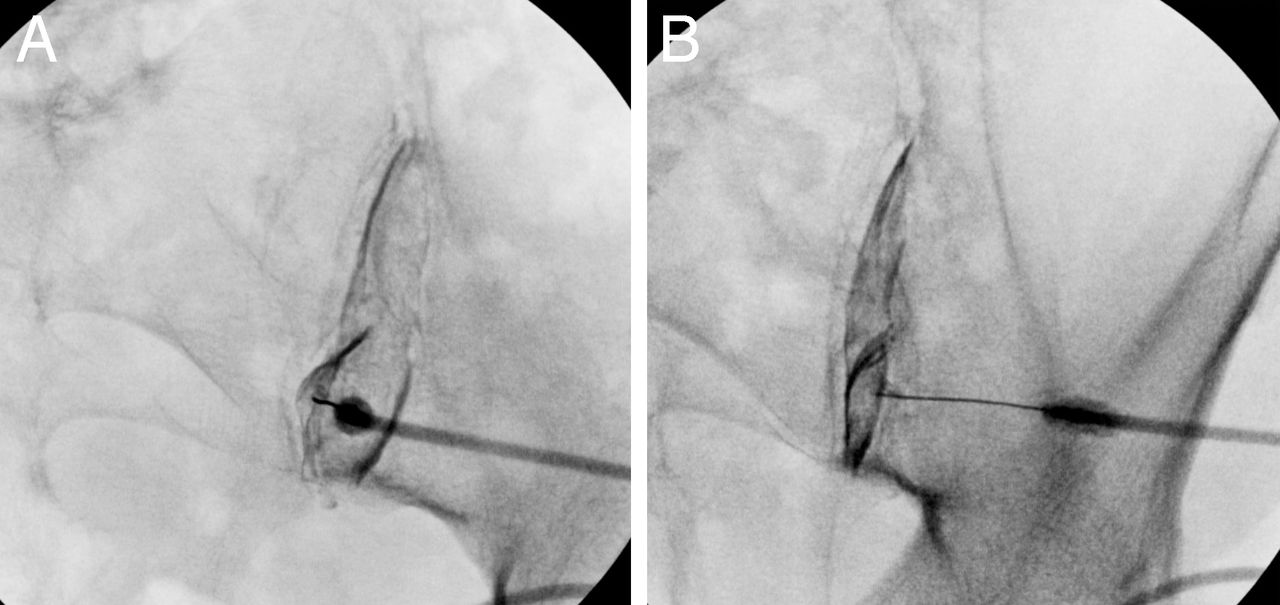
Sacroiliac joint arthrography. Two fluoroscopic views following the injection of 0.6 mL iohexol 240 mg/mL into the right sacroiliac joint clearly outlining the joint space.
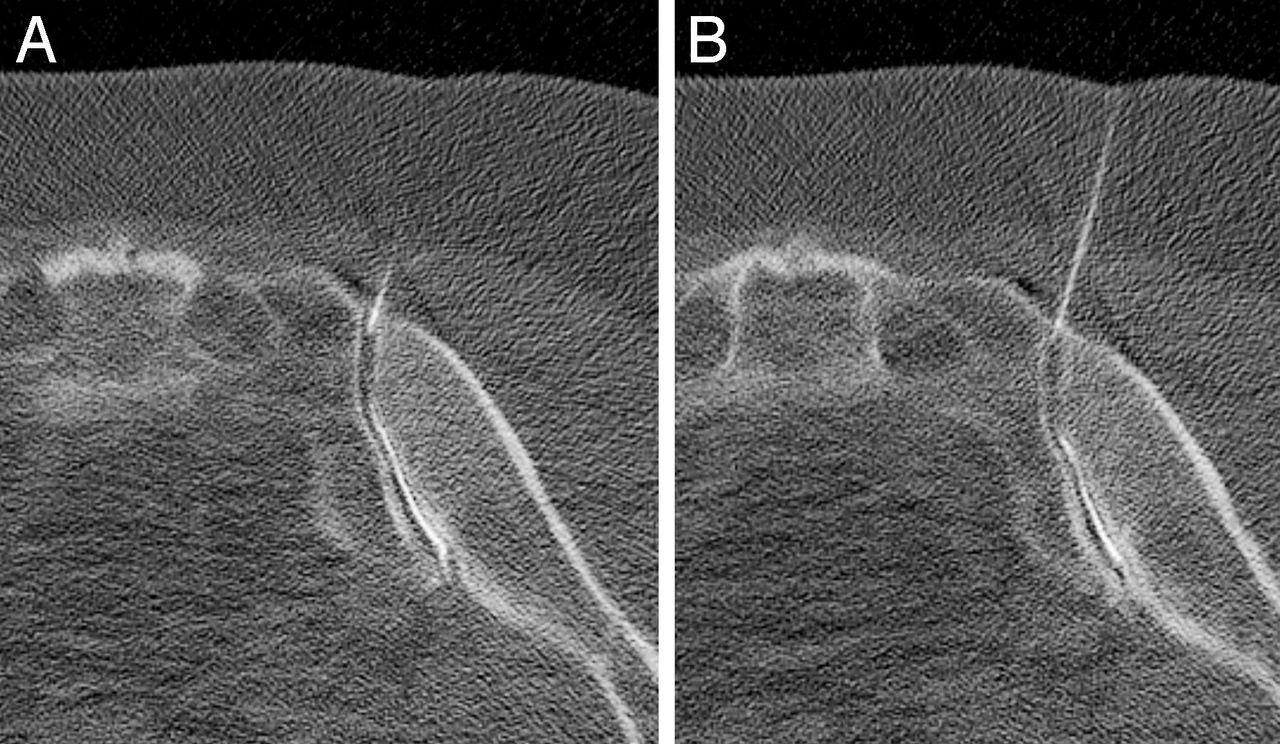
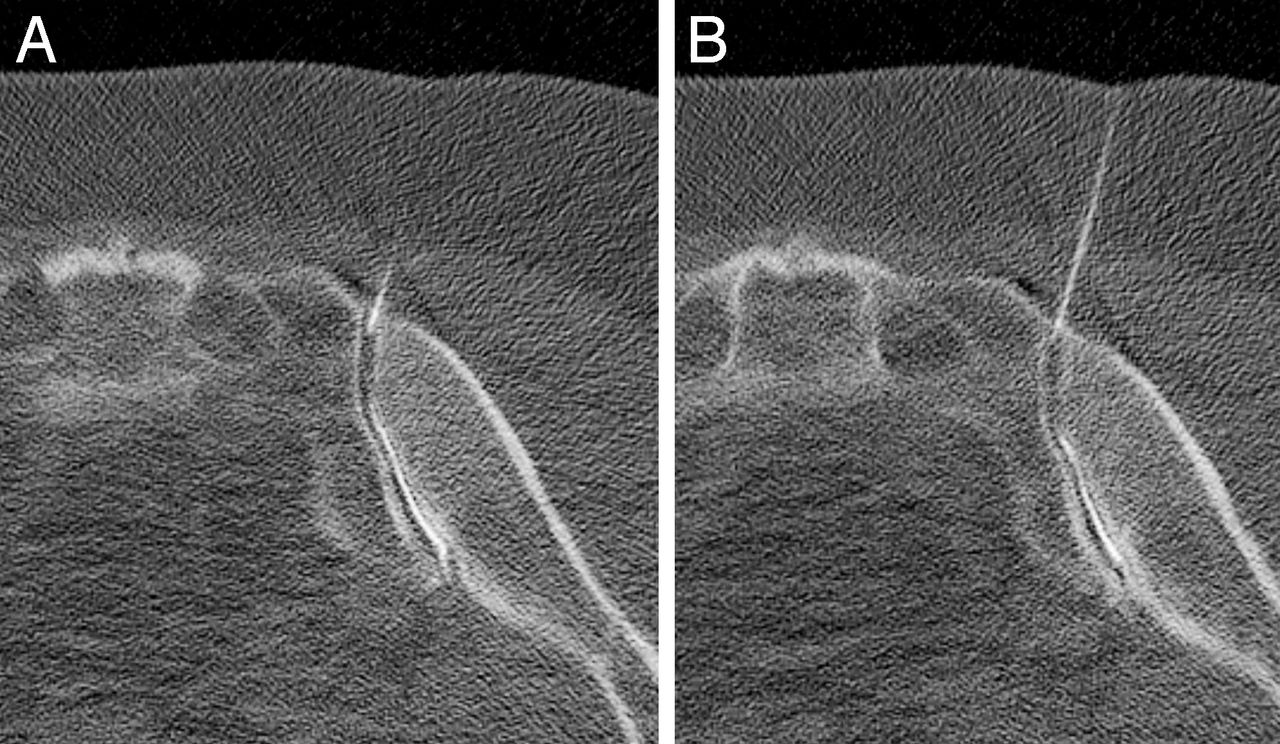
Computed tomography–guided sacroiliac joint arthrography. Sequential axial images of the right sacroiliac joint, following injection of 0.5 mL iohexol 240 mg/mL, demonstrating the needle tip within the joint and clear intra-articular opacification.
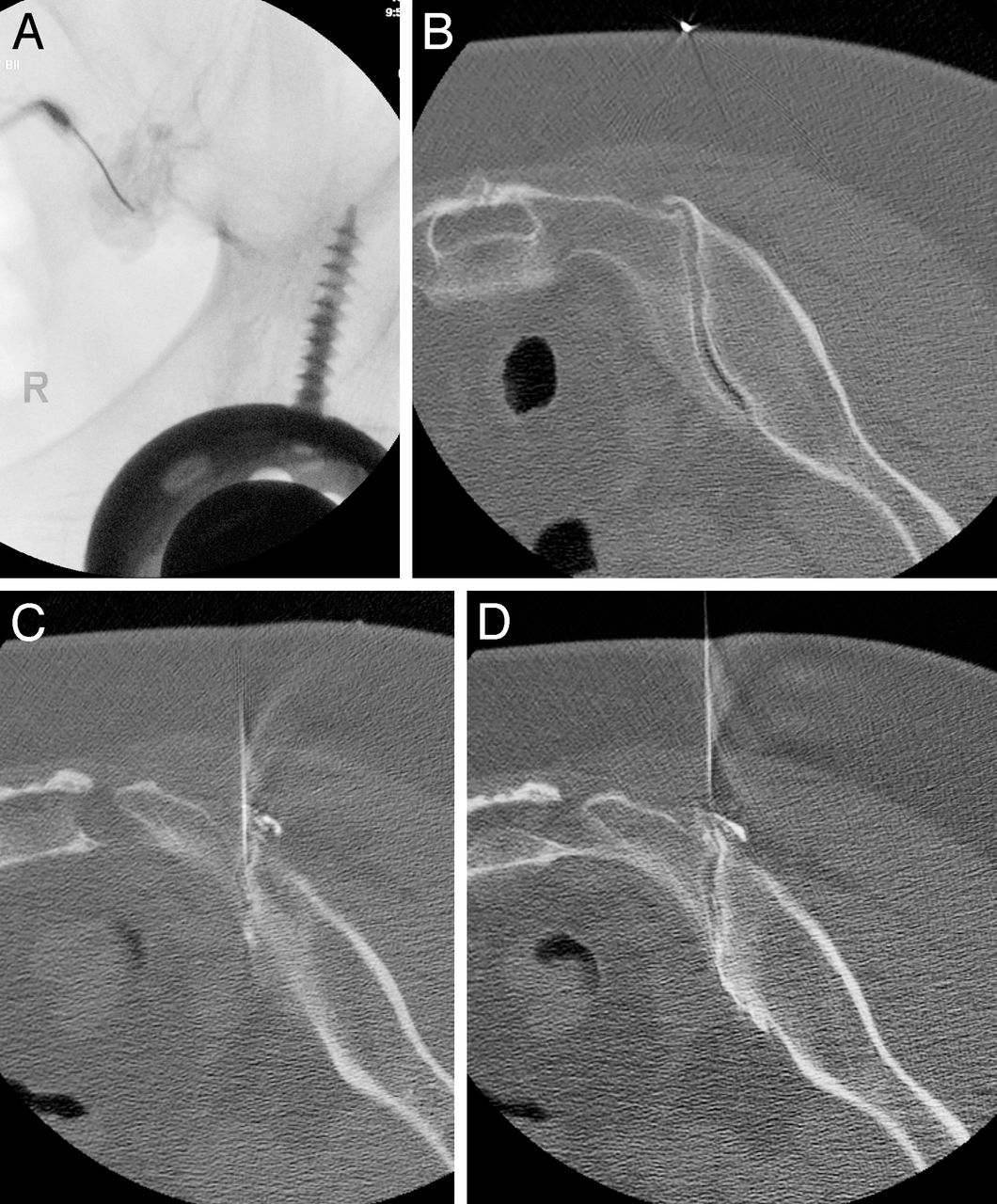
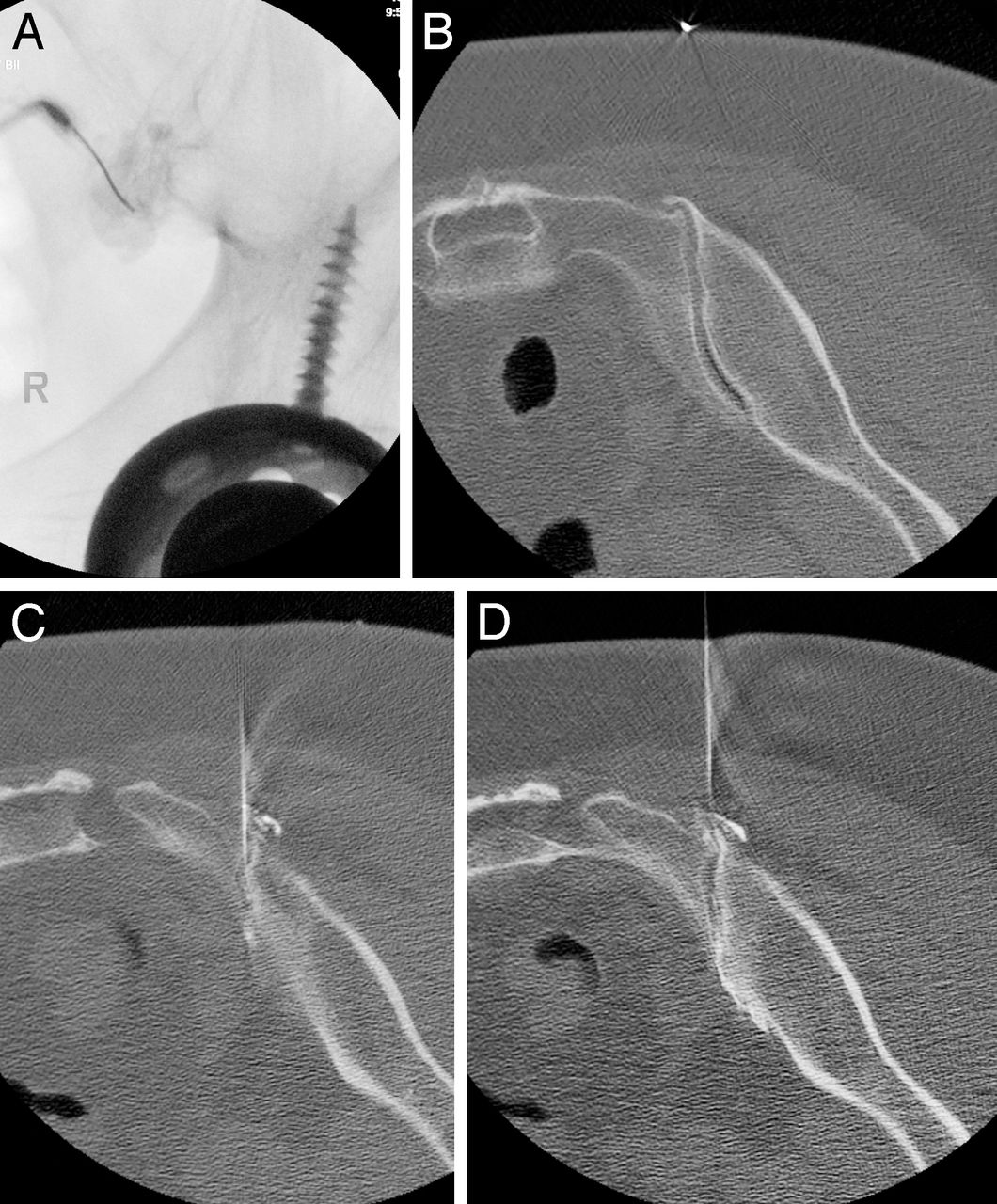
Fluoroscopic versus computed tomography (CT)–guided sacroiliac (SI) joint injection. (A) Fluoroscopic attempt at right SI joint injection, demonstrating predominantly periarticular contrast opacification. The same patient (B) demonstrating a medially oriented osteophyte on preinjection CT images and (C–D) postinjection images demonstrating intra-articular opacification of the joint.
It is recommended that patients refrain from taking pain medication the day of the injection to aid in accuracy of diagnostic response to injection. A preinjection level of pain should be obtained to accurately determine patient response. Postinjection, if there are provocative activities associated with the patient's pain, having the individual engage in such activities prior to and after the injection can also aid in diagnosis.
Local anesthetic works by blocking sodium channels, and the length of relief should correlate with the duration of anesthetic activity. In an ideal situation, the patient would undergo injection of a control agent, such as saline, to mitigate for false positives. However, this would require informed consent, and many patients may object to undergoing a sham procedure. An alternative to placebo control is use of a confirmatory or double block, where the patient undergoes 2 diagnostic injections using 2 different local anesthetic agents. Generally, the first block is performed with a shorter-acting anesthetic, such as lidocaine, whereas a longer-acting anesthetic, bupivacaine, is used for the confirmatory block. The duration of effect for lidocaine is about 0.5 to 3 hours versus bupivacaine, which is 2 to 5 hours.22 A pain diary may also be helpful in recording the patient's response and in correlating to the particular anesthetic.
The degree of pain relief required for a confirmatory response and to predict clinical outcome is unclear. Most studies and pain management societies have used a criterion of at least 75% relief from local anesthetic, as diagnostic.23–25 However, a recent study demonstrated good response to SI joint fusion in patients with 50% relief from diagnostic SI joint block, suggesting that those patients with a 50% to 74% response to diagnostic block may still benefit from certain treatments.26 One of the reasons suggested for this is that SI joint fusion acts as a mechanical stabilizer, possibly affecting both the intra-articular and extra-articular structures, whereas the anesthetic works biochemically, blocking the nerves innervating the articular surface. This may also explain why some studies suggest potential benefit with both intra-articular and periarticular injection of corticosteroid.27,28 Injection of corticosteroid can have both a diagnostic and potential therapeutic benefit. Patients who undergo SI joint injections of both local anesthetic and corticosteroid should have a biphasic response: immediate from the anesthetic and delayed from the steroid. If steroid is administered, patients should be asked to keep a pain diary and monitor their pain level on a daily basis for at least 1 week.
SUMMARY
The SI joint is a complex and important biomechanical structure that is richly innervated and can serve as a pain generator. Whereas acceptance of the SI joint as a potential source of low back pain has grown, confirming that it is the cause of a patient's pain remains a diagnostic challenge. This reflects a combination of factors including the inherent anatomical and biomechanical complexity of the joint, as well as its overlapping clinical presentation with adjacent structures. Although a thorough and complete physical examination is essential in evaluation of the sacroiliac joint, no noninvasive pathognomonic test exists to reliably differentiate it from other potential pain generators. Fluoroscopic or CT-guided blockade can serve as a reliable and confirmatory diagnostic tool to aid in the evaluation of SI joint–mediated pain.
Footnotes
Disclosures and COI: The authors received no funding for the study and report no conflicts of interest.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.