


ABSTRACT
Background: Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is a surgical technique frequently used to treat symptomatic lumbar spondylolisthesis. We aim to investigate the safety and efficacy of using a biplanar expandable cage in the treatment of symptomatic lumbar spondylolisthesis using a MIS TLIF approach.
Methods: A retrospective review of patient records was performed on patients who underwent MIS TLIF for symptomatic lumbar spondylolisthesis using the FlareHawk cage over a 12-month period. Patient demographics, as well as preoperative and postoperative clinical and radiographic outcome measures were recorded and analyzed.
Results: A total of 13 consecutive patients underwent MIS TLIF for symptomatic spondylolisthesis during the study period. The mean age was 60.2 ± 13.9 years, and 61.5% were female. The mean preoperative and postoperative slippage was 7.0 ± 3.0 mm and 1.0 ± 1.9 mm, respectively. The preoperative mean segmental lordosis was 5.1° ± 6.0°, mean anterior, posterior disc, and foraminal height were 9.1 ± 3.9 mm, 5.7 ± 1.5 mm, and 11.0 ± 2.0 mm, respectively. The postoperative mean segmental lordosis was 6.8° ± 4.7°, and mean anterior, posterior disc, and foraminal height were 11.4 ± 2.2 mm, 7.8 ± 1.0 mm, and 12.3 ± 1.3 mm. There was improvement in all radiographic parameters postoperatively. The mean Visual Analog Scale (VAS) back pain, VAS leg pain improved from 7.0 ± 2.9 and 5.1 ± 3.0 preoperatively to 3.1 ± 2.9 and 1.1 ± 1.7 at the latest clinic follow-up visit, respectively (P = .0081). The mean EuroQol-Five Dimensions (EQ5D) score improved from 0.37 ± 1.7 to 0.66 ± 0.23 after surgery. There was no subsidence, endplate violation, cage migration, or other implant-related complications. No patient required reoperation.
Conclusions: The biplanar expandable cage is both safe and efficacious in treating symptomatic lumbar spondylolisthesis using the MIS TLIF approach. Spine surgeons should be familiar with the biplanar expandable cage technology and keep it in their armamentarium in surgical treatment of lumbar spondylolisthesis.
Level of Evidence: 4.
INTRODUCTION
Lumbar spondylolisthesis is a common pathology that affects many patients. Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is a commonly used surgical technique to treat symptomatic lumbar spondylolisthesis. One challenging aspect of MIS TLIF is the cage insertion through a relatively small surgical corridor between the thecal sac and the exiting nerve root. Furthermore, in a lordotic disc space, the posterior disc height is typically shorter than the anterior disc height, thus limiting the size the cage can be inserted posteriorly and potentially limiting the amount of lordosis restoration. Due to these reasons, many spine surgeons consider MIS TLIF a kyphogenic procedure that decreases segmental lumbar lordosis,1 especially in patients with baseline medium to high segmental lordosis preoperatively.2
To circumvent some of these aforementioned drawbacks of the static TLIF cages, various expandable cages have been developed. The first-generation expandable cages are typically uniplanar in design which expand in craniocaudal dimension. Uniplanar expandable cages offered better restoration of disc height and segmental lordosis compared to static cages.2 However, a disadvantage of uniplanar expandable cages is that the increased distraction force during cage expansion places increased stress over a relatively small area on the endplate, thus potentially increasing the incidence of endplate violation and cage subsidence.3 Biplanar expandable cages can expand in both height and width, thus not only allowing for improved restoration of segmental lordosis and disc height, but also increasing the total implant-endplate contact surface area which theoretically decreases the likelihood of cage subsidence and maximizes fusion potential.
In this study, we aim to investigate the safety and efficacy of using a biplanar expandable cage (FlareHawk, Integrity Implants Inc., Palm Beach Gardens, FL) in the setting of treating symptomatic lumbar spondylolisthesis using a MIS TLIF approach.
METHODS
Patient Population
A retrospective review was conducted using an electronic database after approval by our Institutional Review Board (IRB# 16-20085). Patients with symptomatic lumbar spondylolisthesis who underwent MIS TLIF using the FlareHawk cage over a 12-months period (March 31, 2019 to February 29, 2020) were identified.
Radiographic and Clinical Assessment
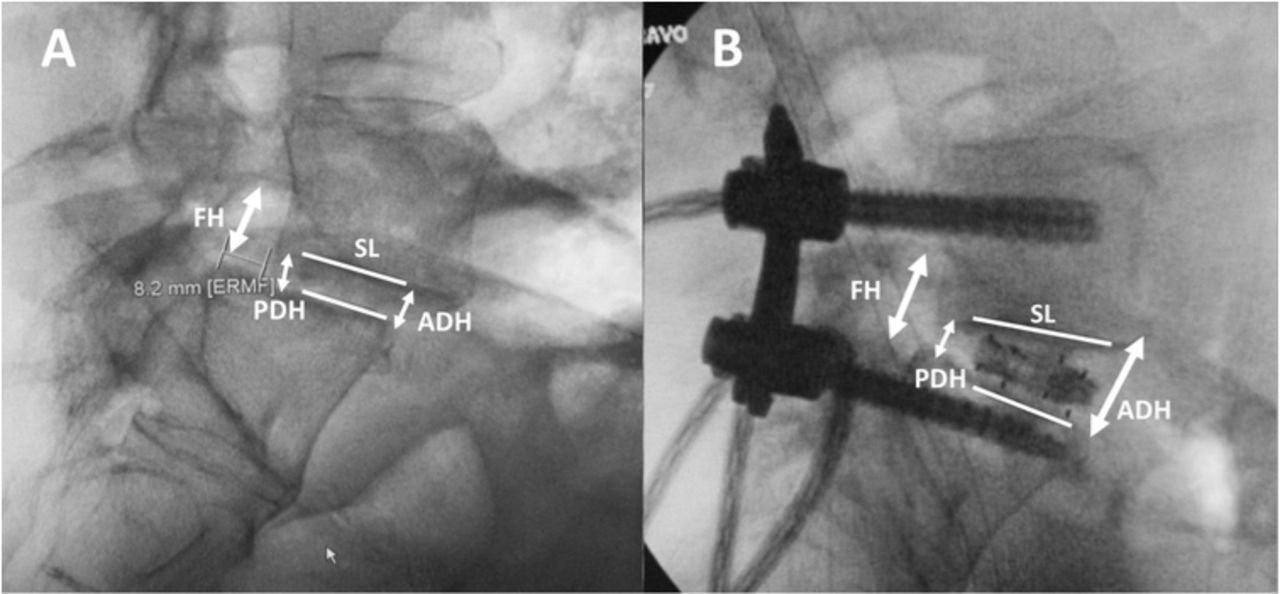
Patient demographics including age, sex, and body mass index were recorded. Radiographic parameters such as preoperative and postoperative anterior, posterior disc, and foraminal height; segmental lordosis; Meyerding grade; amount of slippage reduction; as well as endplate violation and cage subsidence were measured and recorded from preoperative and postoperative upright lumbar radiographs as demonstrated in Figure 1. The measurements were performed by 2 independent film reviewers using standard imaging software. Clinical outcome scores including Visual Analog Scale (VAS) back, VAS leg, EQ5D, and any surgical complications were also recorded and analyzed.
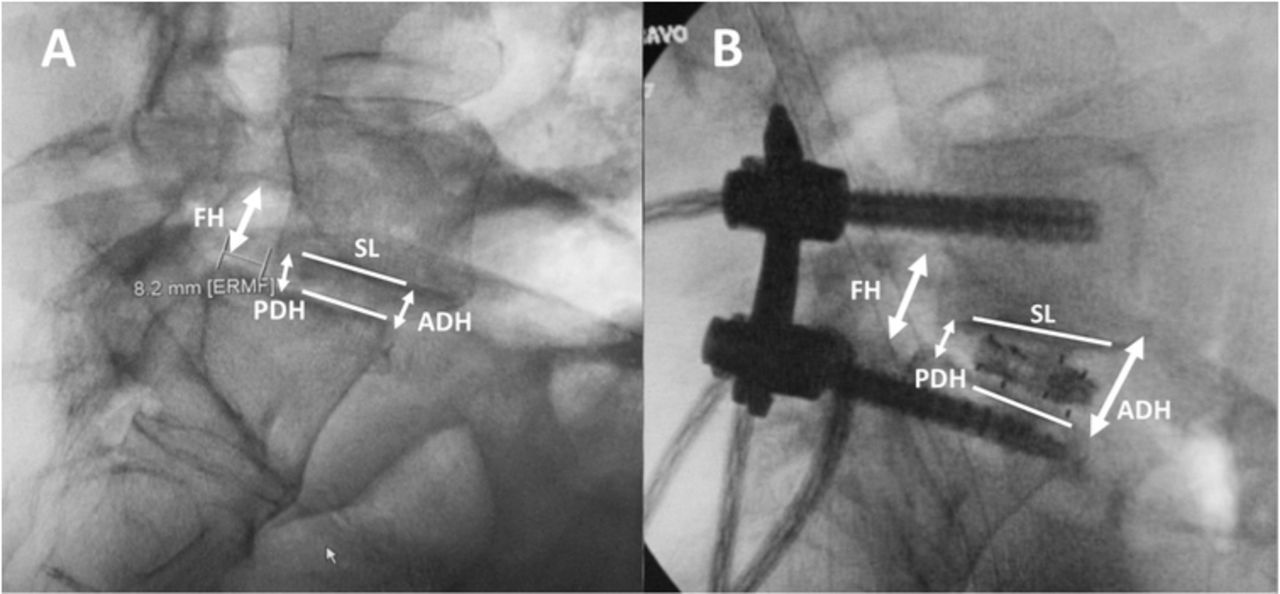
(A) Preoperative and (B) postoperative lateral lumbar x-rays demonstrating the measurement of segmental lordosis, anterior and posterior disc height, as well as foraminal height.
FlareHawk Cage Description
FlareHawk is a low profile, biplanar expandable cage designed to minimize the surgical corridor required for cage insertion, while allowing radial expansion of the cage after insertion with a shim-in-shell type of design. After expansion, the cage allows for postinsertion filling of the cage and prepped disc space with additional allograft to optimize fusion potential.
Surgical Technique and Workflow
The patient is brought into the operating room and undergoes general endotracheal anesthesia. The patient is then positioned prone onto a Jackson table. The lumbosacral area is prepped and draped in the standard fashion. A percutaneous pin is then placed in the region of PSIS (we typically prefer using the opposite side of cage insertion) for attachment of the navigation reference array. An intraoperative computed tomography (CT; O-arm) is then obtained for navigation purpose. Two paramedian incisions are then marked with navigation guidance at the index level. The incisions are planned such that there are optimal trajectories for the pedicle screws and the interbody cage insertion.
The skin incisions are then opened using 10 blade, and small fascial opening are made using monopolar cautery. A navigated drill-guide is then inserted through the fascia opening and docked at the pedicle screw entry point and adjusted for optimal pedicle screw trajectory. The screw pilot holes are then made sequentially, and K-wires are inserted into the pilot holes, then retracted out of the way. Then tubular dilators are docked at the index level over the facet joint with a 26-mm METRx tube. A unilateral facetectomy is performed by removing the inferior and superior articular processes using the high-speed burr and Kerrison rongeurs. The Kambin's triangle is then completely visualized with removal of ligamentum flavum. The traversing root and thecal sac are then gently retracted medially, and an annulotomy is made with a 15 blade. The disc space is then thoroughly prepared by removing all the disc material using disc shavers, curettes, rasps, and pituitary rongeurs. Care is taken to not violate the endplates.
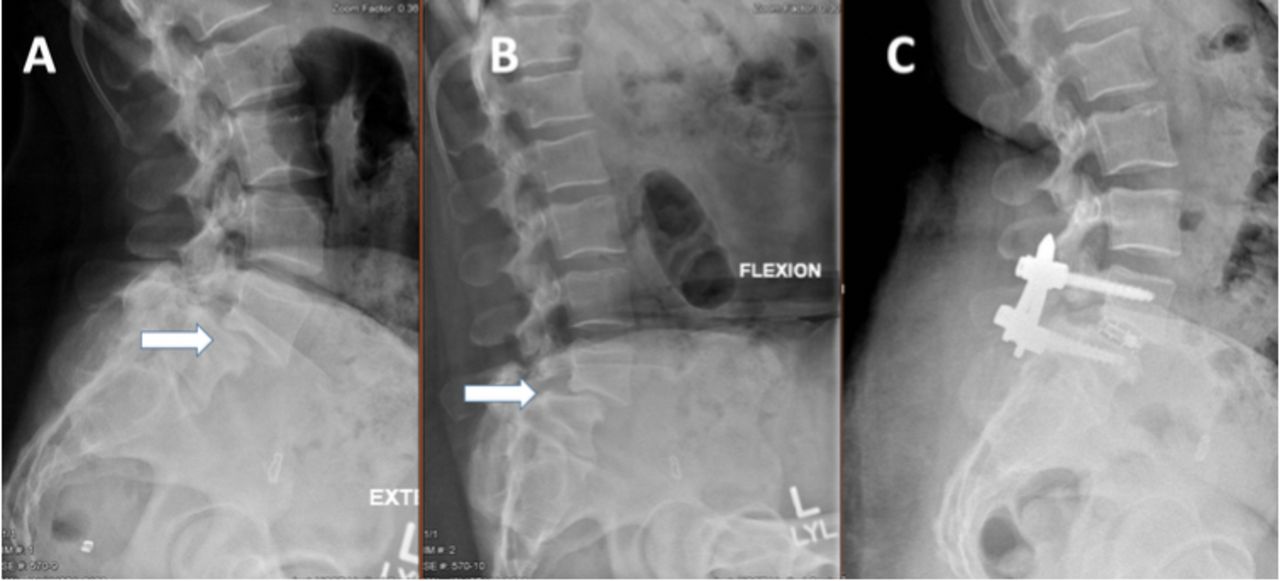
After adequate disc space preparation, an implant trial is used to determine the optimal implant height. The appropriately sized cage is then inserted into the disc space and expanded with fluoroscopic confirmation of cage position. A bone graft funnel is attached to the dorsal cage opening, and allograft bone is used to fill the cage and disc space. The METRx tube is then removed. Percutaneous pedicle screws are then inserted over the K-wire and under navigation guidance. It should be noted that there is often translation of the vertebral body in relationship to the navigation reference frame after TLIF cage insertion, thus making the navigation not completely accurate. The “dancing K-wire” technique can be used to make sure that each pedicle screw is inserted in a trajectory concentric to the K-wire and true to the previously planned screw trajectory. Fluoroscopy is used to confirm screw position. Percutaneous rods are then inserted with the caudal set screws tightened first. The spondylolisthesis is reduced by slowly tightening bilateral cranial set screws. After final x-rays showing good cage position and adequate spondylolisthesis reduction (Figure 2), all set screws are then finally tightened. The wound is then closed in multiple layers in the standard fashion.

Preoperative (A) extension and (B) flexion films demonstrating a Grade 2 spondylolisthesis; (C) postoperative lateral radiograph showing good reduction of a Grade 2 lumbar spondylolisthesis using the FlareHawk cage.
Statistical Analysis
Descriptive statistics were reported as means and standard deviations. Continuous variables were compared using paired Student's t tests using Microsoft Excel. A P value < .05 was considered statistically significant.
RESULTS
A total of 13 patients underwent MIS TLIF for symptomatic spondylolisthesis during the study period. The mean age was 60.2 ± 13.9 years, and 61.5% were female. The median follow-up period was 6 months. There were 7 cases at L5–S1, 5 cases at L4–5, and 1 case at L3–4; 85.6% of the cases were Grade 1, and 14.4% were Grade 2 according to Meyerding classification. The mean preoperative and postoperative slippage was 7.0 ± 3.0 mm and 1.0 ± 1.9 mm, respectively, with mean spondylolisthesis reduction of 6.0 ± 3.0 mm (Table 1).
Patient demographics, surgery levels, and Meyerding grades.
The preoperative mean segmental lordosis was 5.1° ± 6.0°, mean anterior, posterior disc, and foraminal height were 9.1 ± 3.9 mm, 5.7 ± 1.5 mm, and 11.0 ± 2.0 mm, respectively; the postoperative mean segmental lordosis was 6.8° ± 4.7°, and mean anterior, posterior disc, and foraminal height were 11.4 ± 2.2 mm, 7.8 ± 1.0 mm, and 12.3 ± 1.3mm, respectively. There was improvement in all radiographic parameters postoperatively, with mean change in segmental lordosis, anterior, posterior disc, and foraminal height being 1.7°, 2.3 mm, 2.1 mm, and 1.3 mm (P = .0036), respectively (Table 2).
Radiographic and clinical outcomes.
The mean VAS back pain and VAS leg pain improved from 7.0 ± 2.9 and 5.1 ± 3.0 preoperatively to 3.1 ± 2.9 and 1.1 ± 1.7 at the latest clinic follow-up visit, respectively. These changes were statistically significant (P = .0081). The mean EQ5D score improved from 0.37 ± 1.7 to 0.66 ± 0.23 after surgery. There was no subsidence, endplate violation, cage migration, or other implant-related complications. There was no patient that required reoperation.
DISCUSSION
Minimally invasive TLIF is one of the workhorse procedures for treating symptomatic lumbar spondylolisthesis. Various TLIF designs currently exist on the market and can be generally divided into 3 groups including static, uniplanar expandable, and biplanar expandable cages. Several studies have investigated the biomechanical characteristics of uniplanar expandable TLIF cages. Cannestra et al4 also performed a biomechanical study and found expandable cages with unilateral fixation equivalent to static cages with bilateral pedicle screw fixation. In addition, the expandable cage also provided the strongest resistance to lateral bending compared with ALIF or static cage. Mica et al5 performed a biomechanical study of the Luna cage, which is expandable in the horizontal plane, and showed similar reduction in range of motion compared to an ALIF cage.
There are also several numerous studies comparing the clinical and radiographic outcomes between static and uniplanar expandable cages. Hawasli et al6 also reported their experience of MIS TLIF in 48 patients and found that expandable cages provided greater increase in disc height, foraminal height, and segmental lordosis and more improvement in Oswestry Disability Index (ODI) scores. They also demonstrated that disc height and segmental lordosis were correlated with improved clinical outcome. Godzik et al7 advocated by tailored selection of cages as they showed similar results for segmental lordosis correction but more improvement in disc and foraminal height for the expandable group in biomechanical testing with cadavers. Kim et al8 reported 50 patients who underwent MIS TLIF and found significant improvement in both clinical and radiographic outcomes at 2 years postoperative posterior disc height increase from 8.3 mm to 11.3 mm. Boktor et al9 reported their series of 54 patients who underwent TLIF using expandable cage with 2-year follow up and found there were significant improvement in ODI, VAS leg, VAS back, as well as radiographic improvement in disc height, foraminal height, and segmental lordosis. Interestingly, Yee et al10 reported a retrospective comparison study and showed no statistically significant difference in segmental lordosis between expandable and nonexpandable cages. This may be because their cohort had both open and MIS cases and were nonhomogenous in distribution. Open TLIF affords more ability to distract the disc space precage insertion and more compression postcage insertion, thus may confound their results. Vaishnav et al2 reported a series of 171 patients undergoing MIS TLIF. They found that patients with baseline low segmental lordosis (<15°) had increase in segmental lordosis with either static or expandable cages. In patients with baseline medium to high lordosis, expandable cages maintained the lordosis, while static cages caused loss in segmental lordosis postoperatively. Alvi et al11 performed a meta-analysis on 12 existing studies and found that there was improved segmental lordosis restoration in the expandable group compared to the nonexpandable group (5° versus 2°, P < .001). Other studies have compared crescent versus straight uniplanar expandable cages. Tassemeier et al12 found that disc height increased more with the crescent cage but no statistically significant difference in segmental lordosis restoration. In addition, they found less subsidence with the crescent cage (6.6%) than the straight cage (14.8%).
Massie et al13 reported outcomes on 44 patients undergoing MIS TLIF using a crescent uniplanar expandable cage in patients with lumbar spondylolisthesis and showed that there was improved disc height and segmental lordosis, with 6% subsidence rate. There was also significant improvement in ODI and back pain. They were able to achieve an average reduction of 4.3 mm (6.7 mm preoperatively to 2.4 mm postoperatively). They also demonstrated that the large reduction in spondylolisthesis was associated with greater improvement in ODI and back pain scores. They found an average improvement of segmental lordosis of 3.1° (5.6°–8.7°) and average disc height increase of 3.1 mm (5.1–8.2 mm).
There is limited literature on the clinical and radiographic outcomes with biplanar expandable TLIF cages. In our series, we used the FlareHawk biplanar expandable cage to treat 13 consecutive patients with symptomatic lumbar spondylolisthesis via the MIS TLIF approach.
We achieved good spondylolisthesis reduction in all patients, with slippage improving from 7 mm preoperatively to 1 mm slippage postoperatively. The segmental lordosis also improved 1.7° (5.1°–6.8°), posterior disc height increased from 5.71 to 7.77 mm, and foraminal height increased from 11.0 mm to 12.3 mm. Clinical outcomes measured by VAS back, VAS leg, and EQ5D scores also improved across the board. These findings echo the previous reports on uniplanar expandable cage.
Remarkably, we had no case of endplate violation or cage subsidence in the current series. This is significantly lower than the rates reported in the current literature, which ranges from 6% up to 33%.13,14 One possible explanation is that the increased surface area from expansion in the horizontal plane helps to distribute the stress over a large area on the endplate, thus decreasing the chance for subsidence. In addition, the shim-in-shell FlareHawk cage design consists of a PEEK shell surrounding a titanium shim. The PEEK shell can confirm to the contour of the endplate, thus avoiding endplate violation.
One limitation of the current study is its relatively small sample size and short follow up. However, our early experience with the FlareHawk biplanar expandable cage demonstrated favorable results, with improvement in both radiographic and clinical outcomes in all patients. Future studies with larger sample size and longer follow-up periods are needed to validate our findings.
We treated 13 consecutive patients with symptomatic lumbar spondylolisthesis using the FlareHawk biplanar expandable cage via the MIS TLIF approach. Our early experience showed that there were good short-term radiographic and clinical outcomes. There was almost complete reduction of spondylolisthesis postoperatively in all cases, and there was zero cage subsidence with no other implant-related complications. The patients' EQ5D quality-of-life and pain scores also improved across the board during the follow-up period. The absence of nerve root injury is suggestive that biplanar expandable cage is safe and obviates the need for excessive nerve root retraction during cage insertion.
CONCLUSIONS
Our early experiences indicate that the FlareHawk biplanar expandable cage is both safe and efficacious in treating symptomatic lumbar spondylolisthesis via a MIS TLIF approach. Spine surgeons should be familiar with the potential advantages of biplanar expandable cage technology and keep it in their armamentarium. Larger studies with longer follow-up periods are needed to validate our early experience and to elucidate the long-term clinical and radiographic outcomes.
Footnotes
Disclosures and COI: Dr. Tan is a consultant for Medtronic, Stryker/K2M, Depuy, and Integrity Implants. Mr. Rivera, Ms. Tan, and Ms. Le have no conflict of interest to declare. Dr. Berven is a consultant for Medtronic, Stryker/K2M, Innovasis, Globus Medical, and Integrity Implants; he also receives royalties from Medtronic and Stryker/K2M and has direct stock ownership in Green Sun Medical and Providence. Dr. Khoo is a consultant for Integrity Implants and a clinical collaborator of Burst Biologics.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Biplanar Expandable Cages for Transforaminal Lumbar Interbody Fusion Are Safe and Achieve Good 1-Year Clinical and Radiological Outcomes in an Asian Population
- Biplanar Expandable Cages for Transforaminal Lumbar Interbody Fusion Are Safe and Achieve Good 1-Year Clinical and Radiological Outcomes in an Asian Population