


Abstract
Background Length of stay (LOS) is a meaningful outcome measure for more efficient and effective quality of care. However, algorithms to predict LOS have yet to be created for patients who undergo surgical management for traumatic spinal fractures.
Objectives The objectives of this study were to (1) identify preoperative, perioperative, and postoperative factors associated with increased LOS and (2) create predictive formulas to estimate LOS in thoracolumbar trauma patients who undergo surgical correction.
Methods This is a retrospective case series of 196 patients operated for thoracolumbar spine trauma from January 2012 to December 2017 at a level 1 trauma and academic institution. Bivariate analysis between LOS and various preoperative, perioperative, and postoperative factors was conducted to identify significant associations. Multivariate analysis was conducted to create models capable of predicting LOS.
Results LOS was significantly associated with various preoperative (eg, Charlson Comorbidity Index, Glasgow Coma Scale [GCS], injury severity score), operative (eg, length of surgery, number of instrumented segments, surgical technique), and postoperative variables (eg, complications, discharge location). Multivariate analysis of preoperative variables identified 5 significant independent predictors that could predict LOS with strong correlation with observed LOS (ρ = 0.63). With all variables considered, multivariate analysis identified 8 variables (GCS, American Society of Anesthesiologists score, neurological status, polytrauma, packed red blood cell transfusion, number of unique postoperative complications, skin complications, and discharge facility) that could predict LOS with strong correlation (ρ = 0.80).
Conclusions Various preoperative, perioperative, and postoperative factors are significantly associated with LOS in traumatic thoracolumbar spine patients. We developed models with good predictive capacity for LOS. If validated, these models should help in risk stratifying patients for increased LOS and consequently improve perioperative patient counseling.
Clinical Relevance This article contributes to identifying and predicting patients who are high risk for extended LOS after traumatic thoracolumbar injuries.
Level of Evidence 4.
Introduction
In an attempt to curb the increase in healthcare costs, the Centers for Medicare and Medicaid Services have employed cost containment and quality improvement measures, such as bundled payments and pay for performance.1 These reimbursement programs strategically incentivize hospitals and providers to reduce excessive resource use, such as extended length of stay (LOS) after surgery.2 Extended LOS has been shown to be correlated with increased risks of readmission and of developing healthcare-acquired infections, both frequent targets of hospitals for cost reduction.3–5 Understanding risk factors associated with extended LOS may help inform preventative measures to avoid unnecessary additional costs. Furthermore, knowing the predicted LOS of trauma patients can help guide patient and family counseling during their stay.
In patients who undergo surgical correction for thoracolumbar (TL) trauma, many factors may influence hospital LOS. Hospital-specific factors, such as hospital volume and doctors-to-patient ratio, have been shown to be associated with LOS.6 However, preoperative, perioperative, and postoperative patient-specific factors may perhaps play a larger role in LOS. Factors such as age, sex, American Society of Anesthesiologists (ASA) physical classification score, comorbidities, operative duration, number of levels fused, blood loss during surgery, and postoperative complications have been shown to be associated with LOS in elective spine surgery.6–17 Furthermore, it has been suggested that for elective lumbar spine surgeries, postoperative variables account for more of the variance in LOS compared to preoperative or perioperative variables, but whether this holds true for nonelective spine surgeries has yet to be determined.11
Despite the numerous studies investigating LOS for patients undergoing elective spine surgeries, there is a lack of studies exploring LOS for patients who undergo semielective surgery for TL trauma. The objectives of this study are to (1) identify preoperative, perioperative, and postoperative factors associated with increased LOS and (2) create predictive formulas to estimate LOS in TL trauma patients undergoing spine surgery.
Methods
Study Design and Patient Selection
This study was designed and conducted using the format recommended by Strengthening the Reporting of Observational Studies in Epidemiology guidelines.18 Following approval from institutional review board, a surgical billings database was queried using current procedural terminology codes for spine surgery and filtering for thoracic and lumbar spine trauma cases from January 2012 to December 2017. Informed consent was not obtained. All surgeries were performed by 1 of 4 fellowship trained orthopedic spine surgeons at an urban level 1 trauma and academic institution. All adult patients were included. Patients who underwent additional nonspine surgery during their admission were excluded. Patient with nontraumatic fractures, previous spine surgery, mortality, or unavailable records were also excluded. A total of 360 patients were originally queried, and after applying eligibility criteria, 196 patients were included in the study.
Data Collection
Retrospective chart review to collect patient-specific factors was performed by researchers blinded to outcome results. Patient demographic information (age, sex, body mass index [BMI], and Charlson Comorbidity Index [CCI]) and trauma-related variables (Glasgow Coma Scale [GCS], ASA score, neurological status at admission, loss of consciousness, fracture spine level, fracture morphology, and polytraumatic status) were gathered from history and physical examination notes and radiology notes in the electronic patient chart. Polytrauma was defined as having traumatic injury to at least 2 of the following: head, face, neck, chest, extremity, or abdomen. Injury severity score (ISS) was obtained from the institution’s trauma database. Perioperative variables, such as surgical approach, number of instrumented levels, estimated blood loss, packed red blood cell (PRBC) transfusions, and surgery duration, were gathered from anesthesia reports and operative notes. Postoperative variables, such as complications and discharge location, were primarily collected from discharge notes as well as the trauma database. Complications were divided into systems: cardiac, pulmonary, gastrointestinal, renal/genitourinary, skin, neurologic, and hematologic/infectious. A total of 61 different postoperative complications were tracked, and the number of unique complications without duplicates was recorded for each patient. Complications were recorded from chart review and coded complications from the institution’s trauma database. A full list of the postoperative complications can be found in Appendix A. Insurance payor information and in-patient LOS were recorded from the trauma database and double checked with the billings database.
Statistical Analysis
Data were collected in Microsoft Excel (Microsoft Office Professional Plus, Microsoft Corporation, Redmond, WA). JMP Pro (Version 13.0.0, SAS Institute Inc., Cary, NC, 1987–2007) was used for descriptive statistics and statistical tests. LOS was tested for normality with the Shapiro-Wilk test, and as a result, nonparametric statistical tests were used for bivariate analysis. For categorical variables, Wilcoxon/Mann-Whitney U test was used to compare LOS between 2 groups, and Kruskal-Wallis test was used to compare among more than 2 groups. For continuous variables, correlation with LOS was assessed using Spearman correlation coefficient (ρ) where ρ < 0.1 was interpreted as no correlation, 0.1 < ρ < 0.3 was considered weak, 0.3 < ρ < 0.6 was considered moderate, and ρ > 0.6 was considered a strong correlation. After natural log (ln) transformation of LOS to achieve a more normal distribution, we applied backward stepwise linear regression to create 2 multivariable linear regression models. The first multivariate model initially considered all preoperative variables that had a significant association with LOS in bivariate analysis, and then the least significant variables were removed one after the other until remaining variables were all significant independent predictors. In the second model, all variables with significant associations with LOS in bivariate analysis were initially included, and then stepwise removal was similarly performed. To evaluate the models, predicted LOS from the models was compared with actual LOS. P < 0.05 was considered statistically significant.
Results
There were 196 patients included in our analysis from a total of 360 patients who were operated for thoracic or lumbar spine trauma (Figure 1). Average patient age was 45.7 (range 16–91) and 139 (71%) were men. The median and mean of LOS were 6.7 and 10.7 days. LOS did not fit a normal distribution, and thus nonparametric alternatives were used for statistical tests (P < 0.0001). Bivariate analysis of demographic variables indicated that CCI had a significant weak positive correlation with LOS (ρ = 0.20, P = 0.005), whereas age and BMI had weak positive correlations that did not reach statistical significance (Table 1). As for categorical demographics, sex and insurance did not show statistically significant differences in LOS (P = 0.23 and P = 0.71, respectively).
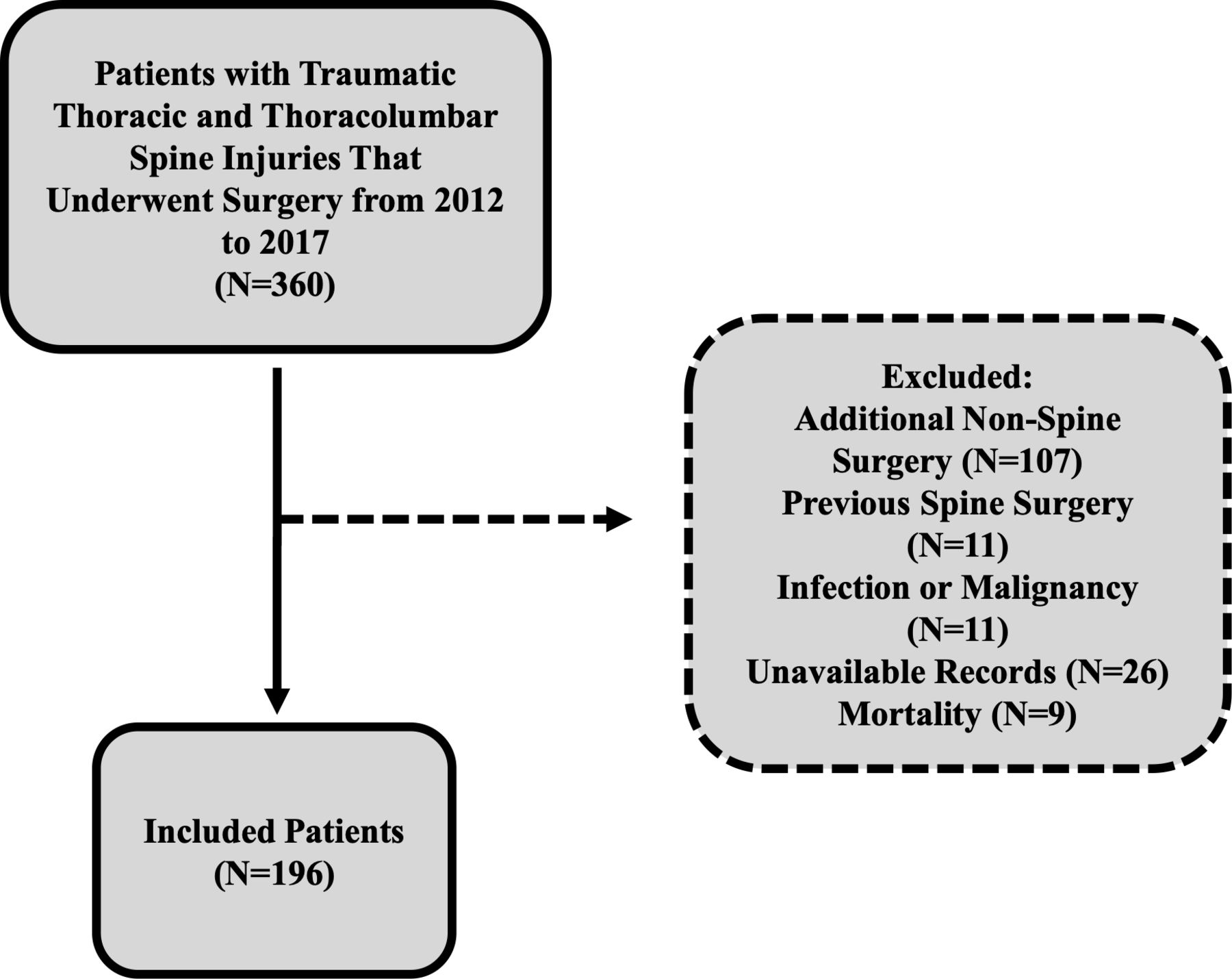
Flowchart of patients included in the study.
Bivariate analysis of demographic variables and LOS.
Bivariate analysis of trauma variables showed that GCS, ISS, fracture level, fracture morphology, ASA, loss of consciousness, neurological status, pulmonary injury, assisted ventilation, and polytrauma were significantly associated with LOS (Table 2). Pairwise analysis for fracture level revealed T1-T9 fracture group had longer LOS compared to both T10-L2 (P < 0.0001) and L3-L5 (P = 0.003) groups. Pairwise analysis for fracture morphology revealed that fracture-dislocation is associated with an increased LOS compared to burst/compression (P = 0.0005), extension-distraction (P = .05), and flexion-distraction (P = .003). For neurological status, patients with complete injury had significantly higher LOS compared to patients with incomplete or intact neurological status (P < 0.0001). Pairwise analysis for assisted ventilation revealed mechanical ventilation >96 hours being associated with longer LOS compared to mechanical ventilation <96 hours (P = 0.02), and mechanical ventilation <96 hours having longer LOS compared to no assisted ventilation (P = 0.003).
Bivariate analysis of trauma variables and LOS.
Bivariate analysis of perioperative variables showed that length of surgery, number of instrumented segments, and estimated blood loss were all moderately positively correlated with LOS (Table 3). Open surgery was associated with a higher LOS compared to minimally invasive surgery. Furthermore, having received PRBC transfusion during surgery was also associated with statistically significant longer LOS.
Bivariate analysis of perioperative variables and LOS.
Bivariate analysis of postoperative complications revealed that the number of unique complications had a strong positive correlation with LOS (ρ = 0.67, P < 0.0001). Specifically, cardiac, pulmonary, gastrointestinal, renal/genitourinary, skin, neurologic, and hematologic/infectious complications were all associated with higher LOS (Table 4). LOS was found to be significantly associated with discharge to a rehabilitation facility but showed no statistically significant difference for 30-day readmission or reoperation.
Bivariate analysis of postoperative and postdischarge variables and LOS.
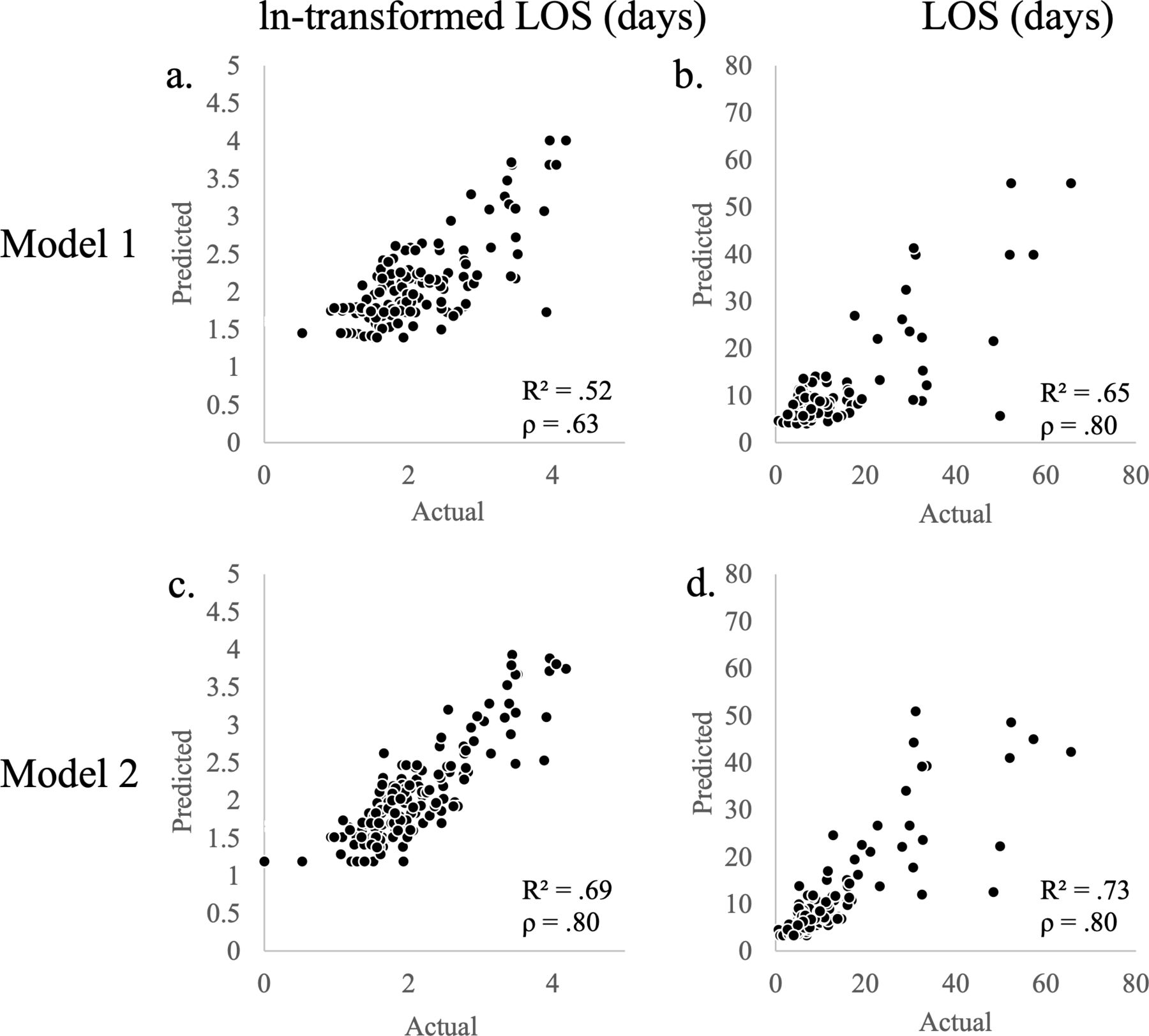
Multivariate analysis of only preoperative variables (model 1) identified GCS, ASA, neurological status, polytrauma, and ISS as independent predictors that could account for 52% of the variance in ln-transformed LOS, which equated to 65% of the variance in LOS (Table 5) (Figure 2a and b). Using the equation produced by model 1, LOS = exp (2.30 + 0.52 × GCS + 0.17 × ASA + 0.14 × Neurological Status + 0.12 × Polytrauma + 0.012 × ISS), there was a strong correlation between predicted LOS and observed LOS (ρ = 0.63, P < 0.0001). When all variables were considered (model 2), GCS, ASA, neurological status, polytrauma, PRBC transfusion, number of unique complications, skin complication, and discharge facility were able to account for 69% of the variance in ln-transformed LOS, which translated to 73% of the variance in LOS (Figure 2c and d). In model 2, number of unique complications accounted for 52% of the variance in ln-transformed LOS alone. Using the equation produced by model 2, LOS = exp (2.27 + 0.31 × GCS + 0.096 × ASA + 0.12 × Neurological Status + 0.16 × Polytrauma + 0.085 × PRBC Transfusion + 0.093 × Number of Unique Complications + 0.20 × Skin Complication + 0.11 × Discharge Facility), there was a strong correlation between LOS predicted by model 2 and observed LOS (ρ = 0.80, P < 0.0001).
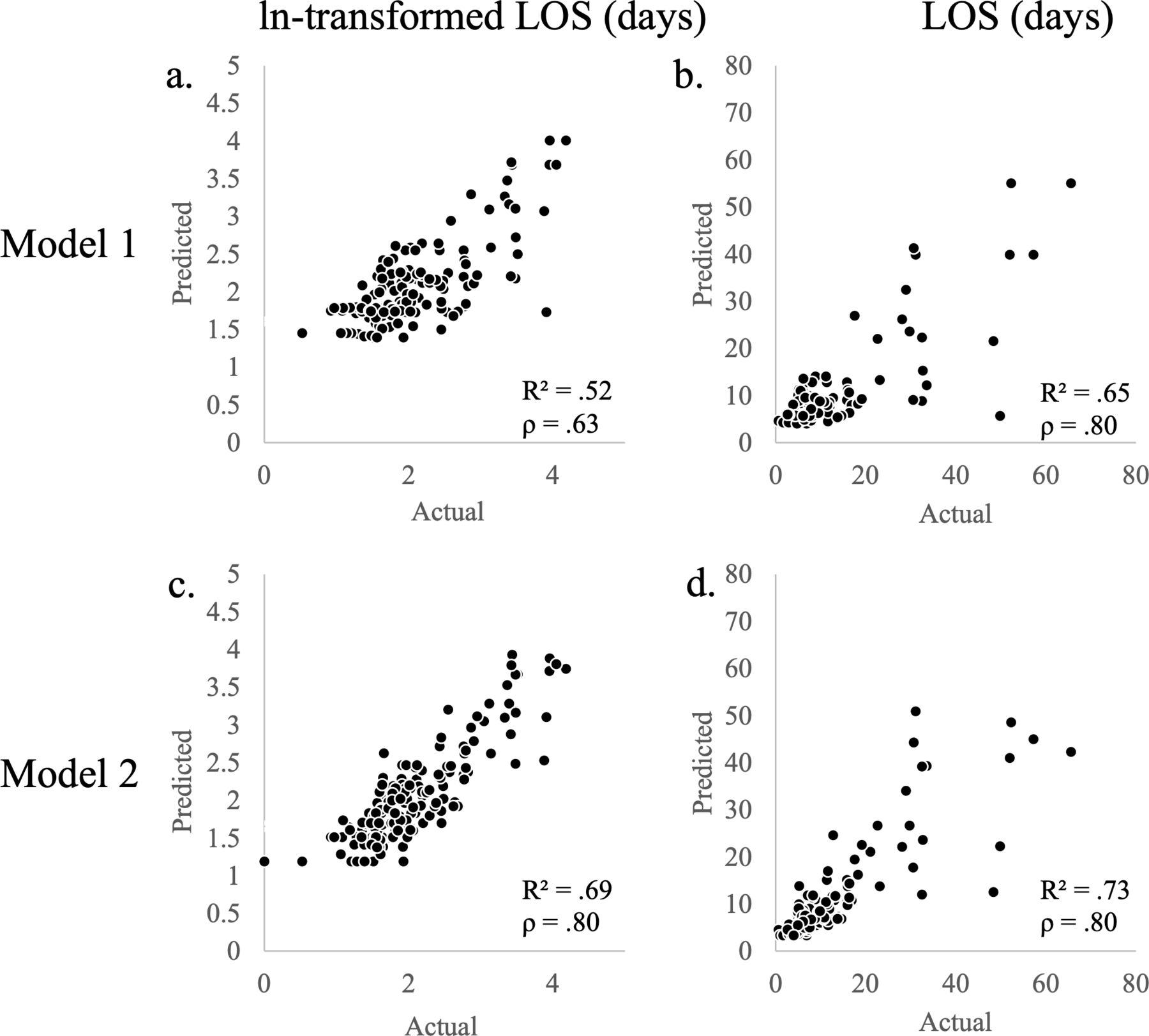
Scatter plots of natural log (ln)-transformed length of stay (LOS) and LOS predicted by model 1 and 2 vs actual ln-transformed LOS and LOS. (a) Model 1 vs actual: ln-transformed LOS; (b) model 1 vs actual: LOS; (c) model 2 vs actual: ln-transformed LOS; (d) model 2 vs actual: LOS.
Multivariate analysis of ln-transformed LOS.
Discussion
With policy initiatives aimed to reduce excessive resource use, LOS has been suggested to be a meaningful outcome measure for efficient quality of care. Patients with longer LOS are at increased risk for developing healthcare-acquired infections and also increase overall costs to hospitals. Factors associated with LOS have been studied for elective spine surgeries and also in orthopedic trauma. However, we were interested in investigating predictors of LOS specifically in patients with TL spine trauma.7,8,19 In this study, many preoperative, perioperative, and postoperative variables were associated with LOS; however, multivariate analysis revealed that 5 preoperative variables alone could account for 65% of the variance in LOS, and that 8 variables could account for 73% of the variance in LOS.
The risk factors identified in model 1 (preoperative variables only) is consistent with those previously reported in the literature. In general, GCS, neurological status, polytrauma, and ISS largely reflect the extent of injuries, whereas ASA is commonly used to describe preoperative global health and comorbidity status. GCS and ASA have been shown in multiple elective spine and trauma cohorts to be associated with LOS,9,10,12,17,20–24 and Chabok et al. identified ISS as being the best predictor for hospital LOS in pediatric trauma patients.25 Multiple studies have demonstrated certain demographics, such as age, sex, BMI, and insurance, to be associated with LOS for the elective spine surgery cohort and general trauma cohort;11,26–30 however, these demographics did not show significance with LOS in the TL trauma cohort. As similarly noted by Chona et al. in the general orthopedic trauma population, perhaps demographics have relatively less impact on LOS compared to variables assessing the extent of injury in orthopedic trauma.19 Nonetheless, the preoperative variables in model 1 are largely accessible and thus provide a convenient initial assessment for anticipated LOS. If validated, this model may be used for patient and family consulting specifically regarding potential LOS.
In addition to preoperative variables, model 2 also includes perioperative and postoperative variables and thus was better able to predict LOS. Specifically, the number of unique postoperative complications accounted for most of the variance in ln-transformed LOS (r 2 = .52), emphasizing the role of the postsurgical hospital course in LOS. This supports Chona et al. who found that 10 of the 12 most impactful predictors of LOS in the general orthopedic trauma population were postoperative in-hospital complications.19 Furthermore, their most impactful variable was surgical site infections, which were also included in model 2 as skin complications. Although skin complications were rare (3.6%) in our cohort, those who experienced it had a median ± IQR LOS of 23.6 ± 37.3 days compared to 6.7 ± 4.2 days those who did not. However, infection complications were not significant predictors of LOS in model 2, a difference likely attributed to the high risk of infection from open fractures in the population studied in Chona et al. Model 2 is also similar to the LOS model developed by Kanaan et al. for elective lumbar spine surgery that incorporated preoperative, perioperative, and postoperative variables. Their model, which included age, preoperative hemoglobin, illness severity, and postoperative complications, could explain 47% of the variation in LOS.12 Model 2 also indicates that discharge to a rehabilitation center results in a longer LOS. The effect may be 2-fold, as patients requiring rehabilitation are in more critical conditions, but it may also reflect the delay associated with discharge or transfer to rehabilitation centers.29 Linzey et al. observed that 30.7% of neurosurgical patients discharged to skilled nursing facilities or a rehabilitation center experienced stay beyond being medically ready compared to 7.7% of patients who were discharged home.31 With 68% of our TL trauma cohort being discharged to rehabilitation centers, this phenomenon may have a sizeable effect. Its inclusion in model 2 may allude to the larger issue of nonclinical delays in excessively long hospital stays. Hwabejire et al. noted that 47% of excessively long hospital stays were due to difficulties in transferring to a rehabilitation center, 26% were due to in-hospital operational delays, 7% were payer related, and only 20% were due to clinical deterioration.32
We went through the exercise of evaluating our models with case scenarios to demonstrate the effects of the variables captured in our model. For a 40-year-old patient with a TL burst fracture who (1) is completely alert, awake, and oriented (GCS of 15), (2) has no comorbidities (ASA of 1), (3) is neurologically intact, (4) has minor injuries (ISS = 6), and (5) no other trauma, model 1 predicts a LOS of 4.1 days. If the same patient instead comes in with a GCS of 5 and a complete spinal cord injury, model 1 predicts a LOS of 15.5 days. With the addition of perioperative and postoperative variables, model 2 is able to account for complications. If this patient subsequently develops a urinary tract infection and surgical site infection, model 2 predicts an increase of LOS of 6.2 days compared to an uneventful postoperative course. In this case, model 1 contains unmodifiable preoperative factors that can help providers stratify high-risk patients for higher acuity of care. Model 2 includes modifiable postoperative variables that can be targeted to reduce LOS, such as number of complications and skin complications. For example, the hospital may implement more frequent wound checks and bed-positioning changes for the patient with GCS 5 and complete spinal cord injury to reduce LOS through reducing skin complications.
There were several limitations to this study. First, there are countless variables that contribute to LOS, and although a wide array of variables was used in this study, there were still variables not considered that may improve the accuracy of the models. Until a model can account for all of the variance in LOS, there will always be more variables to consider; however, the goal of this study was to establish models without using an abundance of variables in order to increase the ease of use of the models created. To develop a model that accounts for 73% of the variance in LOS based on 8 variables means that, out of the nearly infinite variables associated with LOS, only 8 are needed to predict LOS to a strong degree. As for the investigated variables, most of our postsurgical variables dealt with complications, but variables such as physical therapy assessment, pain, and mental health were not represented in the models. In a model predicting LOS following lumbar spine surgery, Kanaan et al. showed that postsurgical physical therapy assessment, such as walking distance, level of assistance during walking, and balance scores, had the highest contribution.11 Although we wanted to include these variables in this study, these variables were not consistently available upon chart review. Another limitation includes model 2’s most impactful variable, number of unique complications, being unstandardized. Due to a lack of a comprehensive score assessing the postoperative hospital course, we created this variable. Although it tracks many complications, it doesn’t consider the severities of each complication or whether they reoccur. However, its inclusion and weight in the model provide insight into the importance of the postsurgical hospital course. Finally, there were also multiple factors limiting the generalizability of our models: (1) data were collected retrospectively from a single level 1 trauma center; (2) certain variables, such as GCS, ASA, and ISS, require assessment from healthcare professionals, who may not be consistent; (3) the study’s cohort was specific for TL trauma patients who only underwent spinal surgery during their stay. It is unknown how these models would perform prospectively in other institutions or cohorts.
Conclusion
With the increasing efforts to provide more efficient care and reduce excessive resource use, LOS has emerged as an important outcome to investigate. However, LOS has a multitude of drivers and may be difficult to predict. Our study demonstrates that CCI, GCS, ISS, fracture level, fracture morphology, ASA, loss of consciousness, neurological status, assisted ventilation, polytrauma, length of surgery, number of instrumented segments, estimated blood loss, surgical technique, PRBC transfusion, and postoperative complications are significantly associated with LOS. Additionally, LOS predicted from a preoperative-only model as well as a preoperative, perioperative, and postoperative model had strong correlations with observed LOS. Future prospective studies are needed to validate the generalizability of these models, and perhaps determine whether guidance from predictive models can safely decrease LOS.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Eugene Y. Koh reports consulting for Biomet and grants from the National Institutes of Health. Daniel E. Gelb reports royalties from DePuy Synthes and Globus Medical; stock ownership from Advanced Spinal Intellectual Property; speaking and/or teaching arrangements and Board of Directors for AO Spine North America. Charles Sansur reports consulting for DePuy Synthes, Medtronic, and Stryker, and speaker and/or teaching arrangements with DePuy Synthes and Gobus Medical. Steven C. Ludwig reports royaltoes from DePuy Synthes, Globus Medical, Theime, and Quality Medical Publishers; stock ownership in Innovaive Surgical Designs and the American Society for Investigative Pathology; consulting for DePuy Synthes, K2M, and Globus Medical; speaking and/or teaching arrangements with DePuy Synthes and K2M; Board or committee member for Globus Medical, the American Board of Orthopaedic Surgery, the American Orthopaedic Association, the Cervical Spine Research Society, and the Society for Minimally Invasive Surgery; research support from Pacira Pharmaceutical, AOA Omega Grant, and Nuvasive; and Fellowship support from AO Spine North America Spine Fellowship Support; Pacira Pharmaceutical; AOA Omega Grant, and Nuvasive. The remaining authors have no disclosures.
Ethics Approval Institutional review board approval was obtained before conducting this research.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.