


Abstract
Background The literature reports that index level (IL) revision spine surgery (RSS) and adjacent level (AL) RSS are diminished in lumbar TDR compared with fusion procedures. There is a paucity of PROMs reported after RSS.
Objective To present the incidence of RSS at the IL and AL following single-level lumbar total disc replacement (TDR) and to document patient-related outcome measures (PROMs) associated with RSS.
Methods PROMs and timelines were analyzed for 32 RSS patients from a prospective cohort study of 401 patients treated with TDR for single-level degenerative disc disease. The data collected prospectively are analyzed from baseline (prior to index surgery) to latest follow-up following RSS. PROMs, including visual analog scales for back and leg, Oswestry Disability Index, and Roland-Morris Disability Questionnaire, were collected preoperatively; postoperatively at 3, 6, and 12 months; and annually thereafter until RSS. The time to RSS was recorded, and PROMs for RSS (IL, AL, or both) were documented, analyzed, and compared.
Results The median time to RSS in the IL cohort was 35 months (interquartile range [IQR] = 9–51 months). The median time to RSS cohort was 70 months (IQR = 41.3–105.3 months). Timepoints facilitate PROM discussion for RSS. Patients in both groups achieved thresholds for the minimum clinically important difference for pain and disability scores. The small sample size in each group contributed to the variability demonstrated by the 95% CIs, thereby cautioning definitive conclusions.
Conclusions This study reveals that statistically significant and modest clinical improvements in PROMs can be achieved in RSS for lumbar TDR at IL and AL. The surgical approach and technique are reflective of the pathology and suggest that anterior RSS for AL degeneration and posterior RSS for IL pathology yield similar results.
Clinical Relevance Statistical and clinical improvements can be achieved in IL-RSS and AL-RSS following single level TDR. It is essential for clinicians to understand and verify the underlying IL and/or AL pathology to select an appropriate management strategy and to facilitate balanced informed discussions with patients.
Level of Evidence 4.
- artificial disc
- back pain
- degenerative disc disease
- motion preservation
- total disc replacement
- arthroplasty
- long-term results
- lumbar spine
- revision
- index level
- adjacent segment
INTRODUCTION
Surgical treatment for recalcitrant symptomatic lumbar degenerative disc disease (DDD), involving either axial discogenic pain and/or radiculopathy, has become increasingly prevalent worldwide.1,2 This has arisen, in part, due to the failure of conservative alternatives to resolve the severely disabling effects of this pathology,3 in spite of the proliferation of multidisciplinary pain clinics.4 Patient expectations regarding quality of life and the impact of successful technological innovations have fueled this momentum.5 The surgical techniques developed to ameliorate the symptoms related to DDD mostly involve fusion of the motion segment. Spine surgery has established its role in the management of the pain and disability arising from lumbar DDD.6,7
Nevertheless, the failure rate is reported to be as high as 37% after lumbar fusion8 and as high as 30% after lumbar surgery without fusion.9 An alternative solution was developed to solve some complications associated with fusion: motion preservation through total disc replacement (TDR).10–12 After TDR, the reported rates of revision spine surgery (RSS) vary from 0% to 28.6%.13–17 The literature reports that index level (IL) revision and adjacent level (AL) disease encompassing clinical and radiographic adjacent segment pathology (CASP/RASP) are diminished after TDR in comparison to after fusion procedures.18–21
The need for RSS can often be reduced through maximization of nonoperative treatment,22 careful patient selection,23 fastidiously obtaining a precision diagnosis,6 and meticulous surgical technique.24 Despite precautions, it is inevitable that the need for RSS will continue to arise.25 The reasons are complex and often include a failure of indication or technique.26 Patient-related factors, such as comorbidities, psychological profile, as well as compensation and litigation, need to be considered before RSS for single-level lumbar TDR.27
Generally, patient satisfaction following RSS is less than that after IL surgery. However, patient expectations28 may have changed significantly following IL surgery and should be considered. The influence of preoperative expectations on patient-reported outcome measures (PROMs) following surgery has not been systematically reviewed.29 However, the surgeon–patient discussion regarding the role of RSS is critical. Various authors contend that there is the potential for surgeon bias in educating expectations from surgery. Consequently, a balanced discussion regarding potential risks vs benefits, and evidence-based outcomes following RSS, is essential. Highlighting with the patient the impact of their expectations30 on their outcome is an essential part of the open and frank discussions about what to expect following RSS.
This article aims to present the incidence of RSS at the IL and AL following single-level lumbar TDR.31,32 An additional aim is to explore the PROMs associated with RSS, with a view to adding to the informed discussions between surgeons and patients when RSS is one of the options being considered.33,34
MATERIALS AND METHODS
Data Collection
This study involves a prospective cohort of 401 patients with single-level symptomatic lumbar DDD who underwent one-level TDR by 2 surgeons at a single center between 1996 and 2015. Data were analyzed from 32 RSS patients from baseline (prior to IL) to latest follow-up after RSS.
PROMs including visual analog scores for back and leg (VAS-B and VAS-L),35 Oswestry Disability Index (ODI),36 and Roland-Morris Disability Questionnaire (RMDQ)37,38 were collected preoperatively; postoperatively at 3, 6, and 12 months; and annually thereafter until RSS. Following RSS, the time to RSS was recorded and PROMs were collected. The RSS at the IL, AL, or both were documented, and PROMs were analyzed. The results for the IL, AL, and general TDR groups were collated and compared.
Patients underwent both index surgery and RSS at the study clinic, except 1 patient who underwent their RSS at another clinic. Two patients had IL and AL revised during the same revision.
Statistical Methods
Descriptive statistics were reported as mean (SD) or median (interquartile range) depending on the distribution of continuous variables. Categorical variables were summarized as counts and percentages. The analyses used PROMs at the following timepoints:
T1 first year after index procedure
T2 final follow-up timepoint before RSS
T3 first year after RSS
T4 final follow-up timepoint after RSS
The mean differences between baseline and follow-up scores were tested using paired t tests and compared against a Bonferroni-adjusted P value of 0.013 to account for multiple comparisons within an outcome. Graphical representations of the mean change scores were plotted along with 95% CIs and the corresponding minimum clinically important difference (MCID)39–41 for each main outcome. Earlier research has found the MCID to be 12 points for VAS-B, 16 for VAS-L, 10 for ODI, and 5 for RMDQ. Statistical analyses were carried out using R statistical software, version 3.5.3.
RESULTS
Thirty-two patients underwent RSS: 14 patients at IL, 16 patients at AL, and 2 patients at both IL and AL. The baseline characteristics of the patients are presented in Table 1. The average follow-up duration was 120 months for IL-RSS and 168 months for AL-RSS. All primary surgeries were performed via left and right retroperitoneal approaches. All anterior RSS was performed by index surgeons without the assistance of an access surgeon. All patients undergoing anterior RSS had angiography studies performed and, if access was suitable, a ureteric stent was inserted at the time of surgery by a urologist and removed 6 weeks later. Table 2 details the types of RSS performed.
Baseline characteristics of surgery patients (n = 32).
Types of RSS performed for IL-RSS and AL-RSS.
The indications for IL-RSS include facet arthropathy (FA) (n = 7), migration (n = 2), FA and migration (n = 3), endplate subsidence (n = 3), and removal of interspinous dynamic stabilization device IDSD (n = 1). The average range of motion of the IL TDRs that were revised was 5 degrees. Two of the patients had undergone a prior discectomy, one an IDSD insertion.
Seven patients with verified painful FA were treated with instrumented posterior spinal fusion (PSF). All cases had a Charité Artificial Disc (DePuy Spine, Raynham, MA, USA) TDR inserted. One patient had a PSF of the L4-5 TDR with extension to the pelvis (IL and AL). The 3 patients with subsidence were also treated with PSF. Two were Charité and one was a Prodisc L Total Disc Replacement (Synthes Spine, West Chester, PA, USA). The subsidence occurred at the junction of the upper prosthesis endplate and the posterior-inferior border of the L5 vertebral body. Three patients with severe FA developed superior endplate migration over the inferior endplate, creating a spondylolisthesis, and were treated with a PSF. Two of these patients had removal of the prosthesis and anterior lumbar interbody fusion (ALIF) via a right retroperitoneal approach (1 with prior hemifacetectomy and discectomy; Figure 1). One was fused in situ. The 2 Charité prostheses that migrated anteriorly more than 5 mm had a PSF performed. One patient had undergone a prior discectomy at L5-S1 with insertion of an IDSD. The disc degenerated over time and was treated with a TDR. Postoperatively, the patient complained of ongoing localized tenderness and investigations revealed an eroded spinous process of L5 that necessitated removal of the IDSD. The 2 patients who had anterior procedures were operated on through a right retroperitoneal approach (the index surgery was performed through a left retroperitoneal approach).

(A) Preoperative magnetic resonance images, (B) preoperative postdiscography computed tomographic image, (C) postoperative radiograph, (D) 6-mo postoperative radiograph with spondylolisthesis, and (E) postoperative radiograph of index level revision, circumferential fusion.
Regarding AL-RSS, 7 patients had a Charité prosthesis inserted at L4-L5 and 10 patients at L5-S1. The average range of motion of the IL TDR before AL-RSS was 8 degrees. None of the patients had undergone prior surgery. At L4-L5, 1 patient suffered a herniation at L5-S1, and a discectomy was performed. Four patients developed discogenic symptoms at L5-S1 and had an ALIF performed via a right retroperitoneal approach. One patient developed symptoms at L3-L4 and underwent a L3-L4 TDR via a revision left retroperitoneal. One patient had a PSF performed at L5-S1 (complex vascular anatomy). At L5-S1, 1 patient had an ALIF performed at S1-S2. Eight patients had a TDR inserted at L4-L5 (Figure 2). All cases utilized a revision left retroperitoneal approach. One patient had an L5-S1 FlexiCore (Stryker Spine, Kalamazoo, MI, USA) prosthesis removed, followed by a PSF of L3-S1 (IL and AL).

(A) Postoperative radiograph of index level L5-S1 total disc replacement (TDR) and (B) revision at adjacent level, L4-L5, with insertion of a TDR.
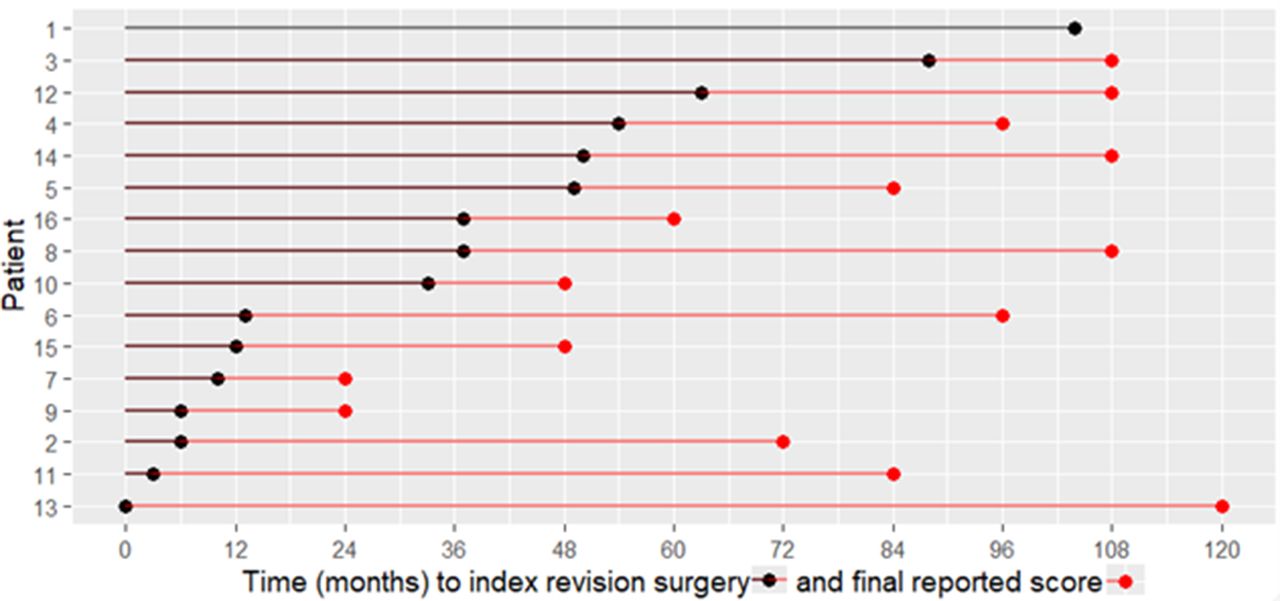
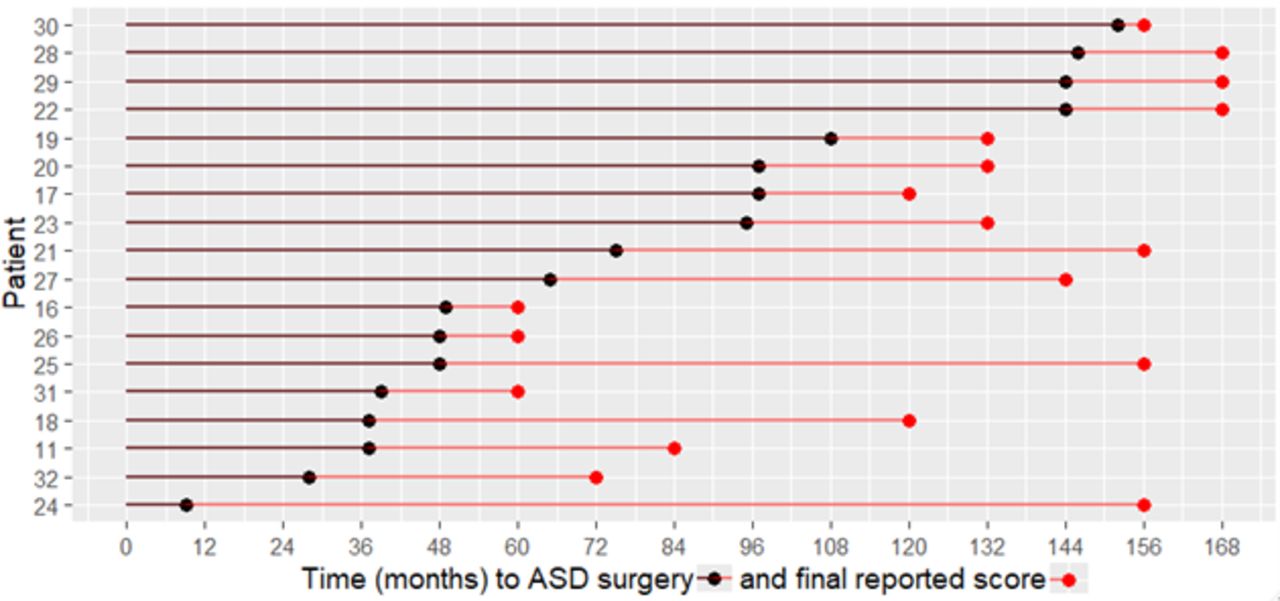
The timeline for IL-RSS and AL-RSS patients is shown in Figures 3 and 4. The black portion of the timeline is the period from index surgery until RSS, while the red portion is the period following the RSS until the latest follow-up. Generally, IL-RSS (Figure 3) occurred in the short- to midterm postoperative period; the median time to revision was 35 months (IQR = 9–51 months). The time to RSS in the AL-RSS cohort (Figure 4) tended to occur in the mid- to long-term postoperative period (median = 70 months, IQR = 41.3–105.3 months).
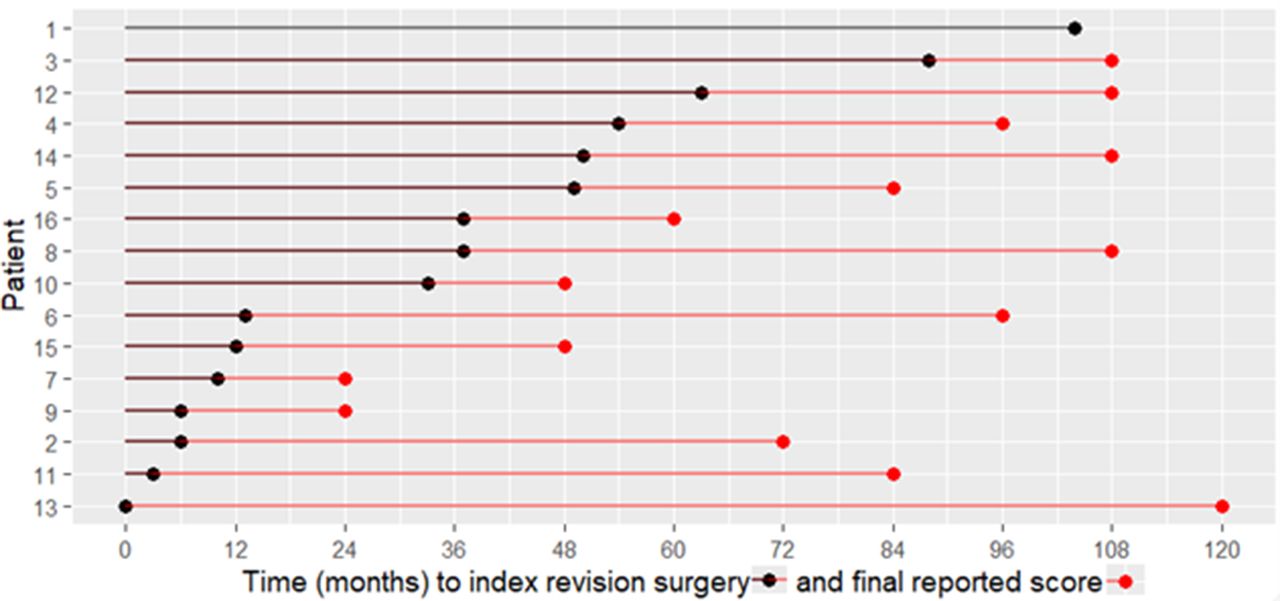
Time to index level revision spine surgery and final reported outcome score for each patient (n = 16). Patients 11 and 16 also had adjacent-level revision spine surgery. Patient 13 underwent revision surgery at another clinic.

Time to adjacent level revision spine surgery for clinical adjacent segment pathology, and final reported outcome score for each patient (n = 18). Patients 11 and 16 also had index-level revision spine surgery.
Table 3 summarizes the PROMs following the RSS. The 2 IL-RSS and 3 AL-RSS patients who had partially completed or missing baseline PROMs were not included in this table.
Change from baseline test results for VAS pain and ODI/RMDQ disability scores.
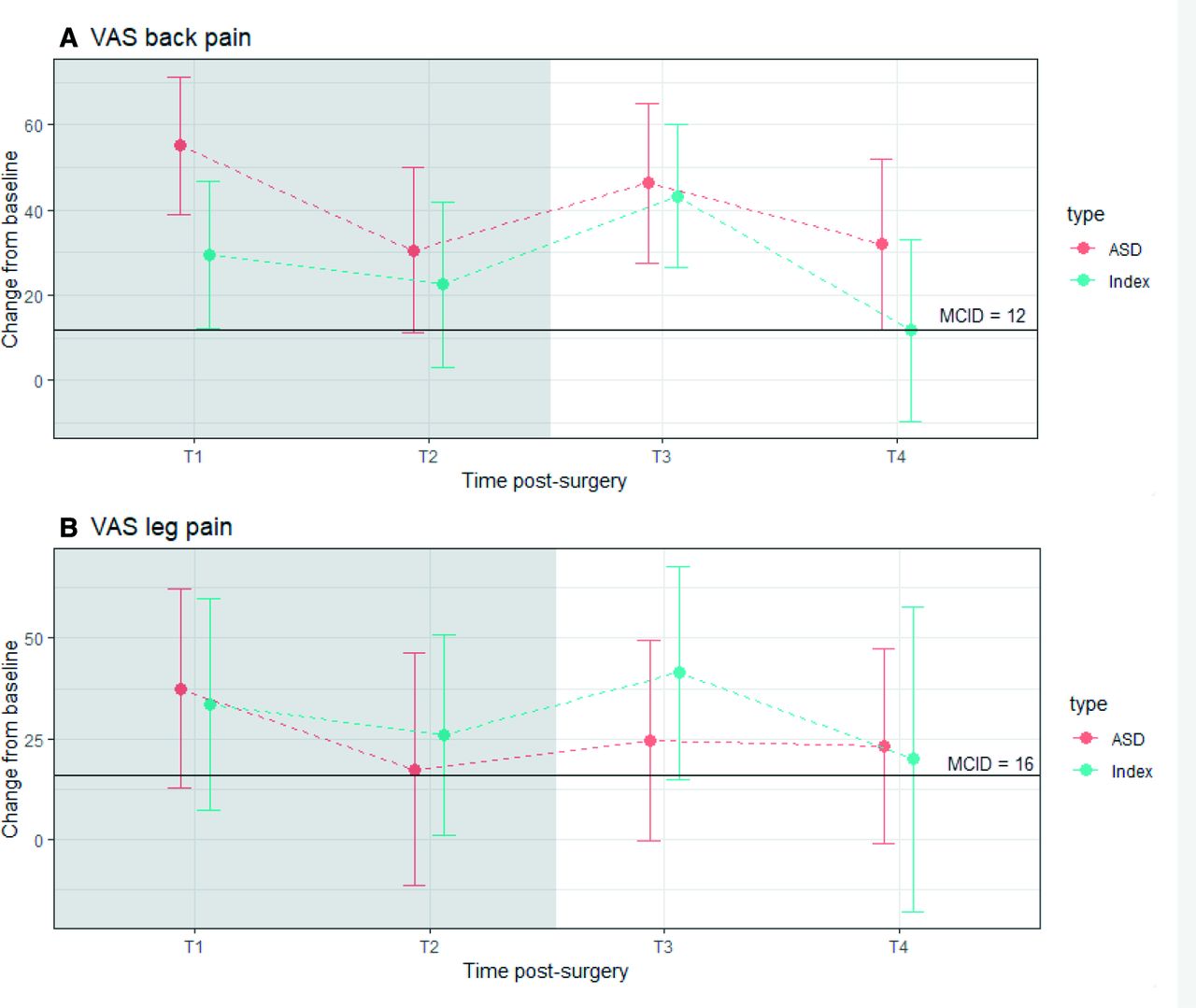
The timepoints T1 and T2 comprise the period following the original surgery, which in turn correlates with the black plot in Figures 3 and 4 and the gray-shaded area in Figures 5 and 6. The timepoints T3 and T4 comprise the period following the RSS, which in turn correlates with the red plot in Figures 3 and 4 and the white-shaded area in Figures 5 and 6. Patients in both groups achieved thresholds for MCID for pain and disability scores. However, the small sample size in each group contributed to the variability demonstrated by the 95% CI error bars, making it difficult to draw definitive conclusions.

Mean change from baseline and 95% CI for visual analog scale (VAS) (0 = no pain to 100 = worst pain) back and leg pain scores at follow-up times after surgery. ASD = adjacent segment disease; T1 = first year after primary surgery; T2 = final year after primary surgery; T3 = first year after revision surgery; T4 = final year after revision surgery with reported outcome. Most mean scores were above the minimum clinically important difference (MCID).
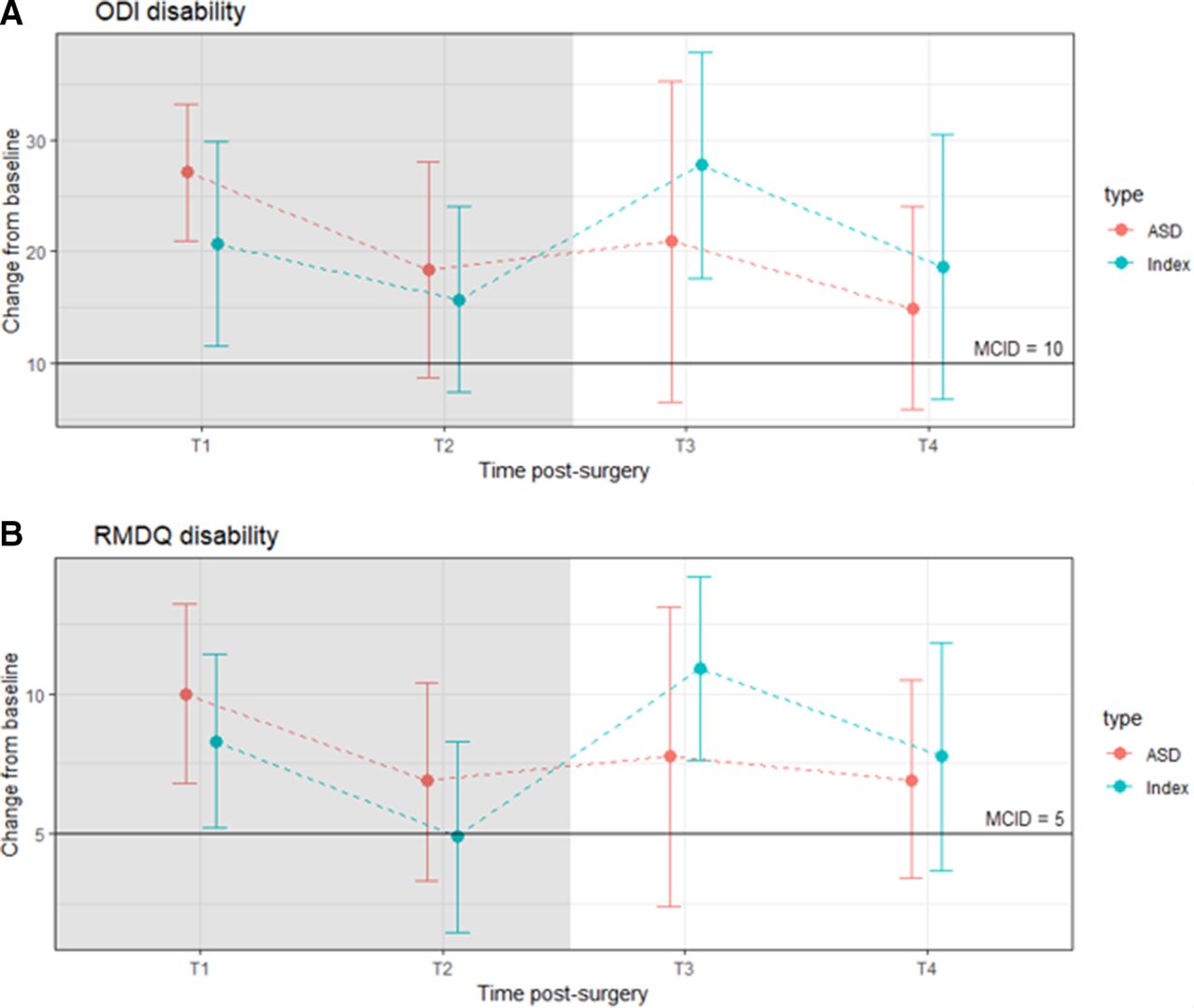
Mean change from baseline and 95% CI for Oswestry Disability Index (ODI) (0 = no disability to = 100 worst disability) and Roland-Morris Disability Questionnaire (RMDQ) (0 = no disability to 24 = worst disability) at follow-up times after surgery. ASD = adjacent segment disease; T1 = first year after primary surgery; T2 = final year after primary surgery; T3 = first year after revision surgery; T4 = final year after revision surgery with reported outcome. Most mean scores were above the minimum clinically important difference (MCID).
DISCUSSION
This study reports on 32 patients who underwent RSS, following 401 consecutive single-level lumbar TDR, with IL revision performed on 16 patients (4%) and AL revision performed on 18 patients (4.4%), 2 of whom underwent IL and AL revision simultaneously (Tables 1 and 2).
Interpretation of Data
This study was conducted independently by the clinicians’ clinic in partnership with Bond University, without any external funding. The study has Bond University’s Human Research Ethics Committee (BUHREC) approval (0000015881). There is potential for bias from industry-funded studies with greater likelihood to report positive results than for studies with other funding sources.42
For simplicity and comparability, we have defined key timepoints as T1 (first year after index surgery), T2 (last follow-up timepoint before RSS), T3 (first year after RSS), and T4 (latest follow-up after RSS).
Figures 3 and 4 show the actual timeline to RSS, in order of longest to shortest, as well as the time to final reported score after RSS.
Table 3 shows the results of the analyses of the difference between baseline and timepoints T1-T4. Compared to the unrevised cohort, the revision cohort showed lower improvements. In the unrevised cohort, the range of mean differences over 13 years were 49.9 to 60.9 for VAS-B, 39.9 to 55.5 for VAS-L, 32.9 to 42.2 for ODI, and 12.0 to 15.0 for RMDQ.
Although statistical significance was achieved, it is important not to overemphasize this, as statistical significance depends heavily on sample size and effect size. However, there is value in considering the results in context of the reported values for MCID (Figures 5 and 6). Most score changes were on or above the MCID, achieving a clinically significant improvement in pain or disability. For each outcome, the pattern of mean improvement was similar, with substantial improvement observed at T1, followed by a drop at T2, before marked increase in improvement at T3 after RSS, and a decrease at T4.
With respect to variability, error bars (Figures 5 and 6) reflect the 95% CI, which tries to generalize to the population of similar patients. In some cases, the error bars are below the MCID. We hypothesize that this is accounted for, in part, by the small sample size. With larger sample sizes, the CIs are always narrower and the mean itself can potentially improve. In summary, our sample means achieved MCID at T4, but due to small sample sizes and the inherent cohort variability, it is harder to draw definite generalizable conclusions.
Some PROMs produced noticeably wider CIs, hence more variability (eg, leg pain at T4 for index patients in Figure 4; and T3 for adjacent segment disease patients on disability scores in Figure 5). These may provide more insight compared to the more consistent and precise results for other results with smaller CIs that lie entirely above the MCID.
Context of RSS
There are considerable publications on PROMs in relation to index surgeries in the US Food and Drug Adminstration investigational device exemption studies42–44 and others.45,46 There is, however, a paucity of published revision data such as incidence,47 time to failure, mode of failure,48,49 method of reconstruction, and PROMs data.48 The term “failed back syndrome”50–52 implies that patients have undergone surgery without improvement. This implies the presence of symptoms that are derived from surgery, rather than despite surgery. The assumption is that the surgeon performed the operation incorrectly or inadequately. Most surgeries are performed adequately on reasonable clinical candidates by experienced surgeons.53 Despite technological advances, our ability to fully diagnose all pain generators for a specific patient is not complete. Similar to primary surgery, RSS should have informed consent detailing risks, benefits, and reasonable expectations regarding PROMs .54 RSS encompasses reoperations, revisions and removals at the IL, and surgery for CASP/RASP at the AL.55
Revision Data
Zeegers et al reported on the first 50 of 350 patients receiving TDR, with a 2-year follow-up.56 In 70%, a satisfactory clinical result was achieved. Around 4 patients were lost to follow-up and 12 patients underwent 24 reoperations. Of these, 7 were related to complications, 11 had AL-RSS, and 6 had IL-RSS. Reoperation was beneficial in only 3 patients and PROMs were not reported.
Van Ooij et al reported on 27 TDR patients seen from another institution.17 The authors stated that they “lack information concerning the pain level and functional status prior to the disc replacement”. The group later published 2 further studies on revision arthroplasty. These studies reported that VAS and ODI scores show similar variability in outcome as in this study. The clinical results of 2 revision strategies for failed TDRs were studied after a mean follow-up of 3.7 and 4.4 years in the removal and fusion groups. A clinical improvement (≥25%) in VAS was found in 47% in the removal group and 22% in the fusion group. For ODI, 21% and 27% in the removal and fusion groups, respectively, showed a clinical successful improvement.32,57
Siepe et al reported an overall reoperation rate of 11.6% for IL and 2.2% for AL for RASP. The combined data of RSS for both surgical approach and device-related complications revealed a mean interval of 9.3 months following the index procedure. Revision surgeries for persisting pain were performed after a mean follow-up of 43.2 months (range 10.8–98 months). RSS-AL were performed late postoperatively after 72.3 months. PROMs for RSS were not reported.
Guyer et el compared 2 TDR prostheses with 5-year follow-up.58 They reported that the percentages of patients undergoing RSS surgery at the IL were 11.8% and 11.6% in the 2 TDR groups. Compared with the number of patients with reoperations at 2-year follow-up, 3 (1.5%) additional patients in the investigational group and 6 (3.2%) in the control group underwent surgery at the index level by 5-year follow-up. PROMs for patients with RSS were not reported.
Laugesen et al reported on 57 TDR patients for postoperative follow-up at a mean of 10.6 years (range 8.1–12.6 years).31 About 19 Nineteen patients (33%) underwent IL-RSS with fusion at an average of 42 months postoperatively. RSS patients had statistically significant worse outcome scores at last follow-up than patients who had no revision. The outcomes of RSS were presented, with VAS-B improving 40% and VAS-L improving 24% from baseline. In the IL-RSS group, 14 (85.6%) of the 16 patients underwent RSS by a PSF/decompression for FA and/or neural compression. The median time to revision was 35 months (IQR 9–51), suggesting an element of kinematic mismatch resulting in facet degeneration and time for the pathology to develop and become symptomatic. Despite RSS, outcomes from baseline were statistically significant and achieved thresholds for MCID.
Kalichman et al noted a significant increase in FA with age, reporting the prevalence as 24% in patients aged under 40 years and 44.7% in patients aged 40 to 49 years.59 It is difficult to differentiate FA due to aging, from FA secondary to unconstrained design in certain lumbar TDR prostheses. A variety of factors likely contribute to biomechanical changes that may result in the development and progression of FA following TDR. Siepe et al revealed that the incidence of FA was significantly higher at IL in comparison to AL following TDR at the lumbosacral junction (P < 0.001). In our study, the incidence of FA was also higher at L5-S1 and had a higher incidence of RSS. We agree with Siepe et al that a cohort of patients may have a kinematic mismatch between the biomechanical properties of the prosthesis vs the physiologic motion of the index segment. Future studies should investigate the relative effects of a constrained prosthesis and analyze spinopelvic parameters with respect to FA and surgical outcomes.60–62
In our AL-RSS group, 14 (82.4%) of the 18 patients underwent RSS for CASP, using anterior reconstructive techniques (anterior lumbar interbody fusion/TDR). The median time to revision was 70 months (IQR 41.3–105.3 months), suggesting genetic or constitutional influences as the underlying cause rather than TDR kinematic effects. The precise mechanism following TDR of reduced RASP/CASP remains elusive. Some studies have suggested that range of motion (ROM) may have a protective effect.63 However, it is more likely that the quality of movement rather than the numeric range of movement is more important. The presence and significance of altered AL intradiscal pressures have been debated, with authors arguing that AL disc pressures are reduced following TDR, while other biomechanical studies report there is no difference in disc pressures.64 Nevertheless, the exact quality and quantity of ROM required for preservation of the adjacent segments remain unknown. The advantage of anterior reconstructive techniques is that they allow superior restoration of disc height and lordosis, improved sagittal balance,65 and preserve the posterior dynamic stabilizers.
This study shows that statistical and modest clinical improvements in PROMs are achievable in RSS for TDR. The surgical approach and technique reflect the pathology and suggest anterior RSS for CASP/RASP results in better clinical outcomes. The IL-RSS, generally performed posteriorly, had improvements from baseline that are statistical but less clinically relevant.
Strengths and Limitations
The data were acquired within the framework of a prospective case series before and after the study. Limitations include a relatively small sample size when considering the statistical significance of PROMs and its effect on the CIs. The strengths of this study include a prospectively followed cohort and financial independence.
CONCLUSION
An evidence-based discussion between the surgeon and patient around risk/benefit considerations and patient expectations and goals regarding RSS is essential. An appropriate course of conservative therapy should be trialed before considering RSS. A second opinion and a multidisciplinary team approach are recommended. This study can assist clinicians in their discussions with patients about the outcomes of RSS following TDR to enable the patient to make an informed decision about whether to undergo RSS.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Matthew Scott-Young previously received royalties and had a consulting agreement with DePuy Spine. The remaining authors report no disclosures.
Ethics Approval Bond University’s Human Research Ethics Committee (BUHREC) approval number: 0000015881
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}