


Abstract
Background Lumbar spinal stenosis (LSS) is a common disorder in older people. Inactivity secondary to the disease state can further increase LSS symptoms. Initial care includes physiotherapy to relieve symptoms and optimize patient function and quality of life. It is currently unclear whether inactivity before surgery for LSS is associated with postoperative outcomes. Our aim was to investigate associations between self-reported exercise before LSS surgery and self-reported outcomes at 1-year follow-up.
Methods Using a retrospective cohort study design, prospective data were collected from the National Swedish Register for Spine Surgery (Swespine) between September 2006 and December 2012: 11,956 patients diagnosed with LSS completed the 1-year follow-up. The primary outcome measure was the Oswestry Disability Index (ODI). Secondary outcome measures were back and leg pain reported on a visual analog scale (VAS). The independent variable was dichotomized into no regular exercise (NRE) and regular exercise (RE). Adjusted analysis of covariance models were used to analyze differences in outcome improvement between the NRE and RE groups.
Results The mean improvement in the ODI was 15.9 (95% CI, 15.5–16.3) in the NRE group and 19.2 (95% CI, 18.5–19.8) in the RE group (P < 0.001). Improvement in back pain (P < 0.001) and leg pain (P < 0.001) were also inferior in the NRE group compared to the RE group. The NRE group improved 21.8 (95% CI, 21.2–22.5) units in back pain and 28.8 (95% CI, 28.1–29.5) in leg pain on the VAS compared to 25.2 (95% CI, 24.2–26.3) units in back pain and 32.5 (95% CI, 31.3–33.6) in leg pain in the RE group.
Conclusions Inactivity defined as self-reported NRE before surgery for LSS is associated with worse outcomes 1-year postsurgery compared to patients reporting RE.
Clinical Relevance This study is relevant to currently practicing spinal surgeons and spine physiotherapists.
Level of Evidence 3.
- lumbar spinal stenosis
- inactivity
- low back pain
- leg pain
- physical function
- physical activity
- spinal surgery
INTRODUCTION
Lumbar spinal stenosis (LSS) is highly prevalent in the elderly population, and surgery for LSS constitutes the most common indication for spine surgery in many countries.1–3 Typical symptoms include leg pain, especially during walking and standing, numbness or paresthesia, and sometimes loss of motor control and bladder disturbances.4 The symptoms can be attributed to isolation and inactivity, and the impairment in quality of life is comparable to stroke, heart disease, and diabetes.5,6
Inactivity can further increase LSS symptoms as well as the risk for medical comorbidities such as heart disease, stroke, cancer, depression, and diabetes. We now know that inactivity is a major health problem analogous to smoking and obesity.7,8
Therefore, initial care should include physiotherapy, including aerobic and strength exercises to relieve symptoms, reduce the risk of inactivity’s medical complications, and optimize patient function, mobility, and well-being.9,10 In selected cases, surgical treatment for LSS is considered the best choice. To achieve further benefits from LSS surgery, a Cochrane review recommended structured training after surgery.11,12 However, several reviews found no benefits of orthopedic surgery prehabilitation (physiotherapy before surgery).9,13 Notwithstanding, a recent randomized controlled trial included 40 patients surgically treated for LSS. The authors found preoperative and perioperative benefits in patients treated with prehabilitation but no differences in outcomes 6 months after surgery.10 There are several methodological problems to measure the level of physical activity in large epidemiological studies, which may be one explanation for the conflicting results.14,15 Conversely, self-reported inactivity using a single question can reliably measure it.16,17 Furthermore, inactivity is a major health problem regarding overall health and outcomes after LSS, perhaps even greater than the level of physical activity.
We conducted a large register-based study because inactivity can be reliably addressed through a single-item question. We hypothesized that inactivity is a possible negative predictor for outcomes after surgery for LSS. We aimed to investigate associations between self-reported inactivity before LSS surgery and self-reported outcomes at 1-year follow-up. Our primary outcome was the Oswestry Disability Index (ODI). The ODI is a patient-reported outcome measure used to assess functional status in patients with pain. Secondary outcome measures were back and leg pain as measured by a visual analog scale (VAS).
METHODS
Study Design
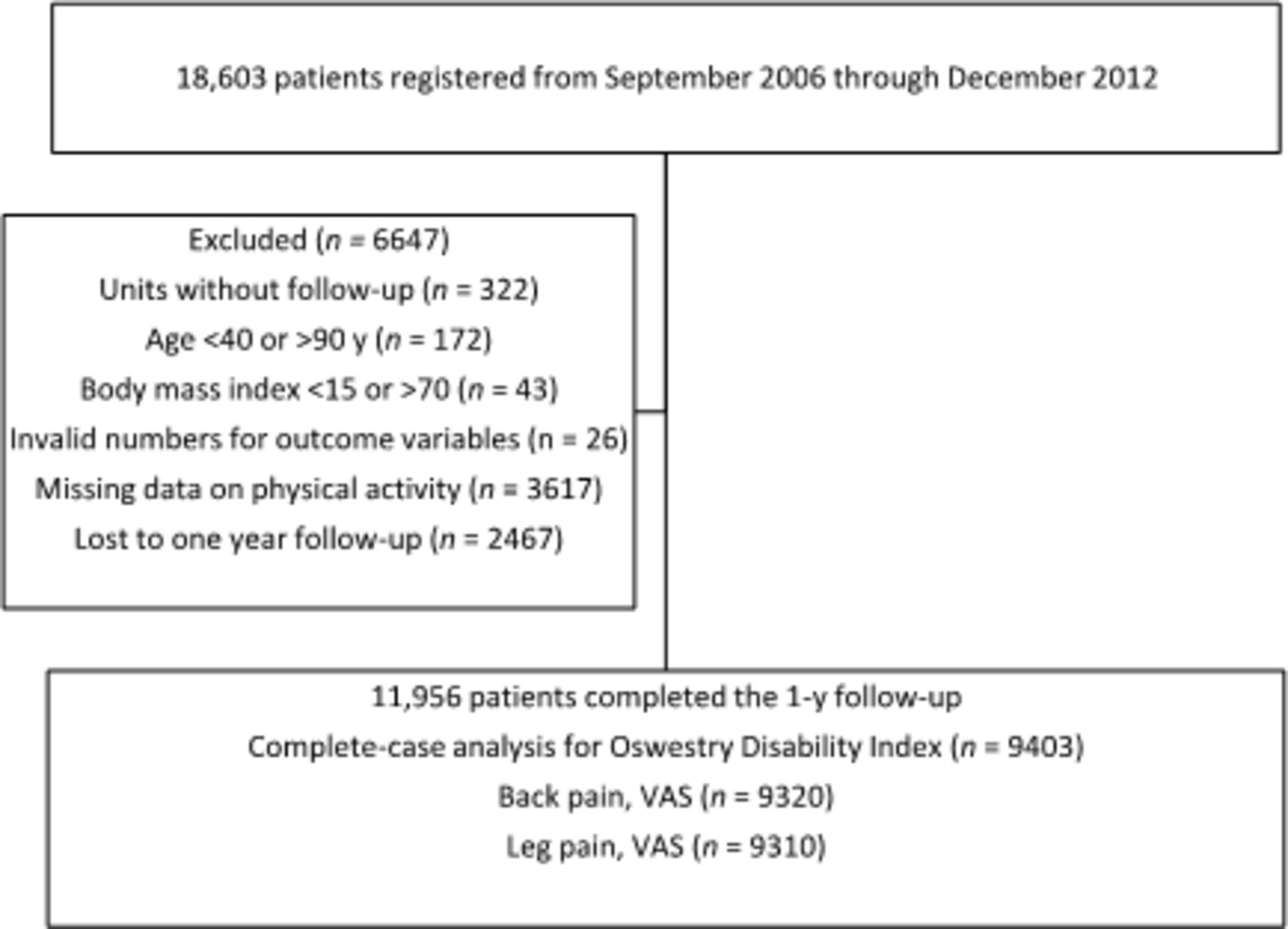
This study retrospectively reviewed large, prospectively collected data from the National Swedish Register for Spine Surgery (Swespine). The register contains patients who have undergone surgery for spinal disorders, including LSS. More than 80% of the total number of surgical procedures for degenerative lumbar spine disorders in Sweden are included in the register. The patients complete a preoperative questionnaire and postal follow-up questionnaires at 1, 2, 5, and 10 years after surgery. The surgeon records surgical data, including diagnosis, without having access to the patient’s questionnaires. Patients’ preoperative data include age, sex, smoking habits, weight, height, back pain (VAS), leg pain (VAS), and the ODI. Physical workload is recorded in 4 categories: I am not employed, low workload, medium workload, or heavy workload. Exercise is recorded in 3 categories: elite, regular exercise (RE), and no regular exercise (NRE). Finally, the independent variable exercise was dichotomized into the categories: RE, which comprised elite and RE responses, and NRE. We included patients registered with a diagnosis of LSS with or without spondylolisthesis from September 2006 to December 2012. Our inclusion criteria were age between 40 and 90 years and body mass index of 15 to 70. Patients missing data on physical activity or lost to 1-year follow-up were excluded. The Figure presents a flowchart for the study.
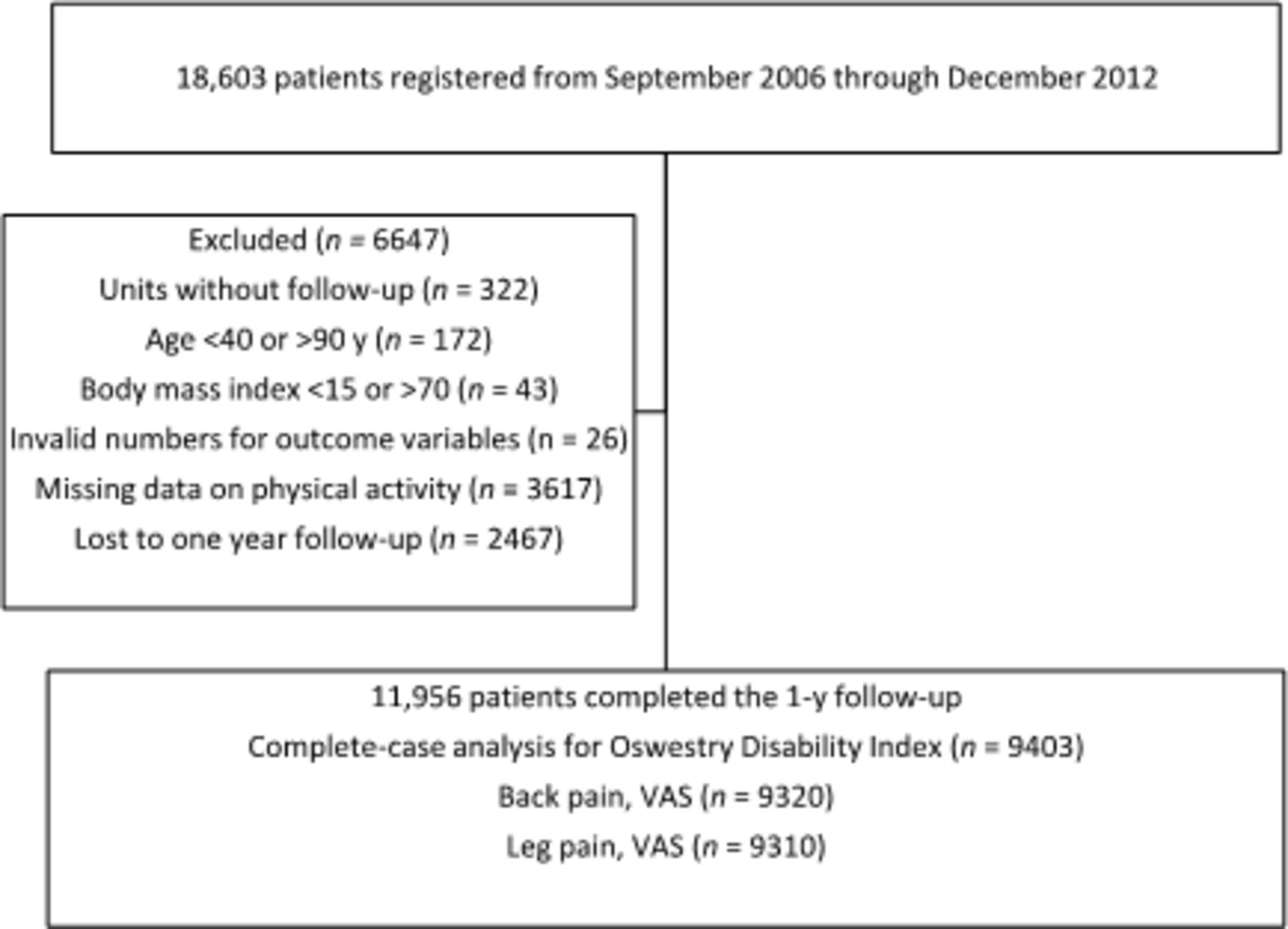
Flowchart for inclusion of patients in the study.
Sensitivity Analysis
Because of the large population included in this study, significant differences can be achieved without a clinically important difference (CID) for the patients. Accordingly, we conducted a sensitivity analysis to analyze the proportion of patients who achieved a CID of 12.8 points on the ODI and 18 units on the VAS.18,19
Statistical Analysis
For continuous outcome variables, adjusted means for the categories NRE and RE were calculated using adjusted analysis of covariance models. We applied multivariable logistic regression to assess ORs with 95% CIs for the dichotomous dependent variables used in the sensitivity analysis. The models were adjusted for age, sex, smoking, body mass index, earlier back surgery, physical workload, and the baseline values of the outcome measures.
RESULTS
Of 18,603 patients reported from 44 orthopedic or neurosurgical clinics, 14,664 (79%) had data about preoperative exercise, and of these, 11,956 (82%) completed the 1-year follow-up. The most common diagnosis was central spinal stenosis without olisthesis (72%, n = 8596). The remaining patients had central spinal stenosis with olisthesis (28%, n = 3360). Most of the patients reported NRE before surgery (75%, n = 8925), followed by 25% (n = 3031) who reported RE. Table 1 describes the baseline characteristics of the 11,956 patients. The final complete case analysis included 9403 patients for function (ODI), 9320 for back pain (VAS), and 9310 for leg pain (VAS). The results from the analysis are described below and in Table 2.
Characteristics of the study group at baseline.
Improvements in ODI and back and leg pain in VAS scores between inclusion and the 1-year follow-up.
Mean improvement in ODI was 15.9 (95% CI: 15.5–16.3) in the NRE group and 19.2 (95% CI: 18.5–19.8) in the RE group (P < 0.001). Improvements in back pain (P < 0.001) and leg pain (P < 0.001) were also inferior in the NRE group compared to the RE group: the NRE group improved 21.8 (95% CI: 21.2–22.5) units in back pain and 28.8 (95% CI: 28.1–29.5) in leg pain vs 25.2 (95% CI: 24.2–26.3) units in back pain and 32.5 (95% CI: 31.3–33.6) in leg pain in RE patients.
Fifty-four percent of NRE patients reported a CID in ODI compared to 61% in the RE group. Compared to the RE patients, the average adjusted OR (aOR) for a CID in the NRE group was 0.75 (95% CI: 0.68–0.83; P < 0.001).
The difference in CID for back pain was smaller: 52% in the NRE group vs 55% in the RE group. The aOR with the RE group as the comparative reference group was 0.81 (95% CI: 0.73–0.91; P < 0.001). Finally, with the RE group as reference, 58% of the patients in the NRE and 65% in the RE group reported a CID for leg pain: aOR for CID in leg pain was 0.81 (95% CI: 0.73–0.81; P < 0.001).
DISCUSSION
To our knowledge, this is the first large multicenter study on inactivity in LSS. The main finding of this study is that self-reported lack of RE is associated with inferior improvement in ODI and back and leg pain 1 year after LSS surgery. Most orthopedic and spine surgery studies have focused on training or specific prehabilitation programs, including exercise and special diets. Few studies have used inactivity as an independent variable. Although our study design prevents us from drawing valid conclusions about causality, several peripheral and central potential pathways can be discussed. Degenerative disc disease, including annulus fibrosus and degeneration of the facet joints, can be a stimulus source for nociceptive pain.20 In addition, spinal stenosis can cause neurogenic pain due to a combination of direct pressure on neural elements and vascular structures. Moreover, the increased pressure inside the dural sac can disturb the nutrition of the neural elements.4 Local nociceptive and neurogenic pain can contract the musculature, further increasing local pain. Chronic low back pain is associated with paraspinal muscle atrophy.21 Inactivity, especially in older adults, can quickly increase the atrophy of muscles and even lead to sarcopenia, which can further increase pain and reduce function.22,23 Moreover, inactivity is considered a risk factor for chronic pain due to the decreased activity of opioid receptors within the central neurons, mediated through N-methyl-D-aspartate receptors in the rostral ventromedial medulla.24
Inactivity can also increase kinesophobia and catastrophizing, conditions that can further reduce function and increase pain.25 Finally, inactivity can further amplify perceived pain through a physiological process, making the brain more sensitive to the peripheral pain stimulus, a phenomenon known as central sensitization.26
Strengths and Limitations
The main strength of the study is the large sample size and the data collection method. To the best of our knowledge, this is the largest study on inactivity in LSS. Our study also has several limitations worth noting. One is the single-item question for exercise, and self-reported data on physical activity have inherent recall bias. However, our data are prospectively collected, and in contrast to physical activity, inactivity can be measured with high specificity through 1-item questions.16,17 Another limitation is that 19% (n = 3617) had missing data on physical activity. Even if this could introduce a risk for selection bias, most of the patients included reported NRE. We therefore believe the responders are representative of physically inactive patients—that is, the missing data on physical activity do not affect the generalization of the results.
Most of the patients were older and retired, and only a minority had physically demanding jobs. Thus, we assume that any remaining confounding due to a high level of physical activity at work is of small importance. In addition, the regression models were adjusted for physical activity at work. Physically inactive individuals tend to overestimate their physical activity, leading to misclassifying physical activity status (especially for inactive people). Such nonstructural misclassification reduces differences between study groups and may slightly affect the estimates leading to a conservative bias. Furthermore, even if the regression models were adjusted for several important confounders, there is always a risk for residual confounding. Another limitation is the loss to follow-up: 70% of eligible patients completed the 1-year follow-up. Although loss to follow-up is a major potential cause of bias, 2 previous spine register studies found no differences in outcome assessment between responders and nonresponders.27,28 Based on these findings, we believe that our results can be generalized to other datasets.
CONCLUSION
Inactivity, defined as self-reported NRE before surgery, is associated with poorer outcomes as measured by the ODI and back and leg pain VAS compared to the patients reporting RE before surgery. Future studies should investigate whether the prevention of inactivity in this population can improve patient outcomes after surgery.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest related to this article.
Ethics Approval The study was approved by the National Ethical Review Board.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}