


Abstract
Objectives Percutaneous pedicle instrumentation (PPI) has been used for the treatment of thoracic and thoracolumbar (TL) trauma. However, the ability of PPI to correct significant post-traumatic kyphosis requires further investigation. The objective of this study is to compare the amount of kyphosis correction achieved by PPI vs the traditional open posterior approach in patients presenting with significant kyphotic deformity following traumatic thoracic and TL spine injuries.
Methods Following Institutional Review Board approval, patients who underwent surgery for thoracic (T1-T9) or TL (T10-L2) fractures with at least 15° of focal kyphosis in a 5-year period were included in this study. Patients were separated into 2 cohorts based on surgical technique: traditional open posterior approach and minimally invasive PPI. Kyphosis correction was measured using Cobb angle 1 vertebrae above and 1 below the level of injury on sagittal preoperative computed tomography image, immediate and follow-up postoperative upright lateral radiographs. Initial degree of correction and loss of correction at the final follow-up were compared.
Results Of 91 patients included, 65 (71%) underwent open surgery and 26 (29%) underwent PPI. Open patients had 11° (95% CI, 9°–13°) of immediate correction compared with 11° (95% CI, 6°–15°) for PPI (P = 0.81). Follow-up data were available for 70 patients with a median of 105.5 days. Both groups had 1° (95% CI, 0°–2°) of loss of correction at follow-up (P = 0.82). Regardless of surgical technique, obesity (>30 kg/m2) and AO type-A compression fractures had significantly less correction. For each unit of body mass index, there was a 0.75° decrease in correction achieved (P < 0.0001). Other factors did not influence the degree of correction.
Conclusions PPI techniques provide equivalent postoperative angular correction and maintenance of correction compared with open surgery in thoracic and TL trauma patients.
Clinical Relevance This study provides evidence for spine surgeons to utilize either technique for treating significant traumatic kyphotic deformity.
Level of Evidence Therapeutic 3.
- spine trauma
- thoracolumbar
- open spine surgery
- percutaneous pedicle instrumentation
- kyphosis correction
- post-traumatic deformity
Introduction
Injuries to the thoracic and thoracolumbar (TL) spine comprise the majority of spinal fractures following high-energy trauma. The most common causes of these injuries are high-energy falls and motor vehicle accidents.1 However, the operative indications of these injuries continue to be a source of great debate and contention.
Surgical treatment may be indicated for patients with significant kyphosis due to sagittal imbalance and the risk of post-traumatic kyphotic deformity.2 Operative management provides immediate stability, reduction of the deformity, restoration of spinal alignment, and earlier patient mobilization.3 The traditional open approach involves a posterior reduction, instrumentation, and fusion in cases where direct spinal decompression or anterior column reconstruction is not needed. A minimally invasive approach with percutaneous pedicle screw instrumentation (PPI) has also emerged as a technique for fracture stabilization. Compared with the traditional open posterior approach, PPI has been shown to be associated with less soft-tissue trauma, lower blood loss, lower infection rate, faster short-term recovery, and shorter hospital length of stay.4,5 While several prior studies have evaluated sagittal balance with PPI, the effectiveness of PPI to correct traumatic kyphosis or angular deformity, however, has not been previously studied.5–10
The primary objective of this study was to compare the amount of kyphosis correction achieved by PPI vs the traditional open posterior approach in patients presenting with significant kyphotic deformity following traumatic thoracic and TL spine injuries.
Methods
Study Population
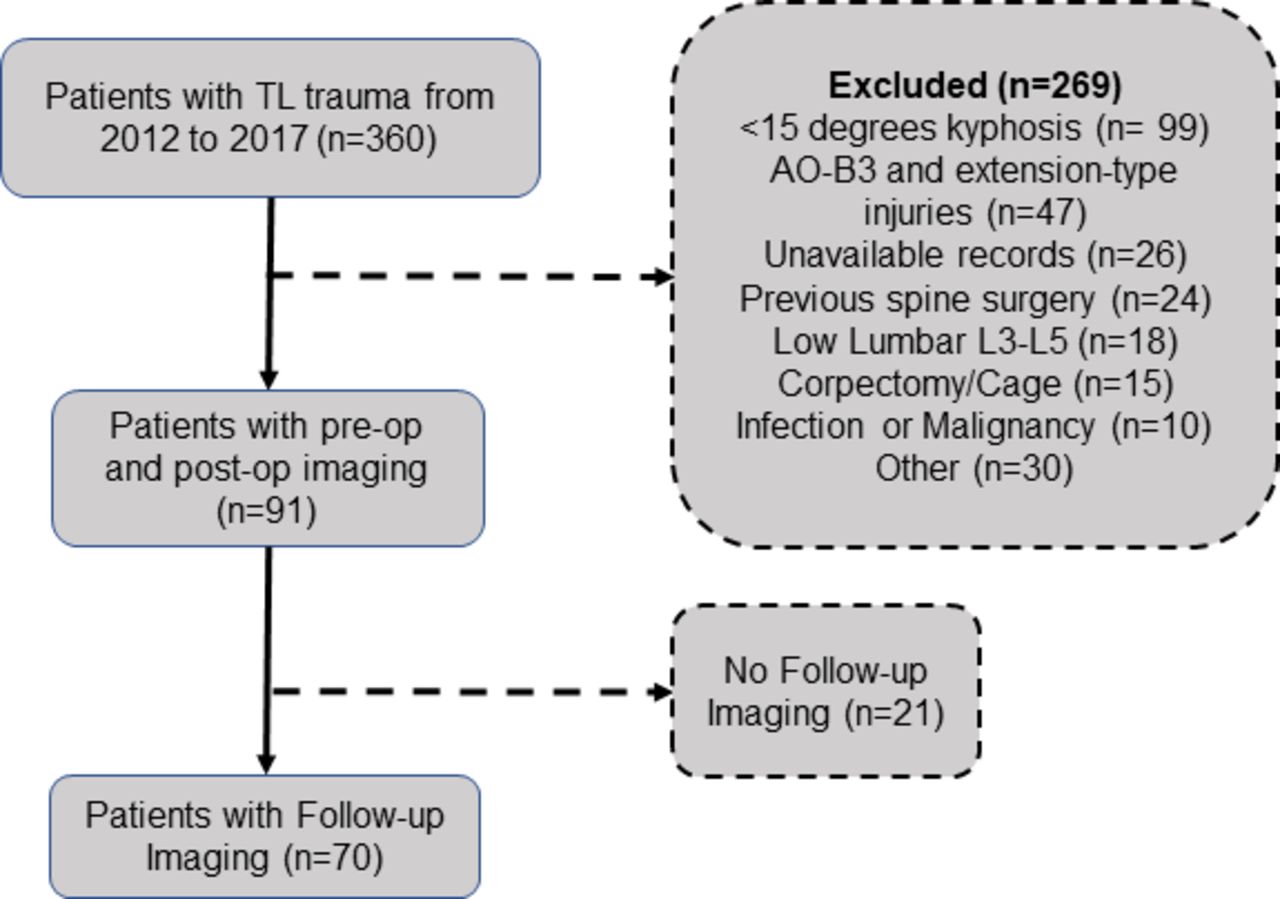
Following Institutional Review Board approval (HP-00082698), patients who underwent operative management at a large tertiary level 1 trauma center for thoracic and TL spine fractures from January 2012 to December 2017 were identified using current procedural terminology codes. As per standard of care, all patients received preoperative computed tomography image of their spine with fracture classification according to the AO spine fracture classification system.11,12 Patients were included in the study if they presented with thoracic (T1-T9) or TL (T10-L2) fractures with at least 15° of focal kyphosis to identify patients with significant kyphosis and unstable fractures. Patients with incomplete records, pathologic fractures, infection, AO type B3 (hyperextension) fractures, or prior TL spine surgery were excluded. Patients who received anterior column reconstruction were excluded as well. From the initial query of 360 patients, 91 patients were included in this study after inclusion and exclusion criteria. The final cohorts consisted of 65 patients in the open cohort and 26 patients in the PPI cohort. Of those, 21 patients (23.1%) were lost to follow-up and excluded from the study (Figure 1).

Study population selection criteria demonstrating included and excluded patients. A total of 360 patients were reviewed, and 91 were included in the study with 70 follow-up imaging. TL, thoracolumbar.
Operative Procedure and Postoperative Care
Selection of instrumentation technique (open vs PPI), fusion, and construct length was chosen at the discretion of the surgeon. Polyaxial pedicle screws with locking mechanism to act as monoaxial screws and titanium rods were used for each construct. Lateral-to-medial technique using C-arm fluoroscopy was utilized for the percutaneous instrumentation group. Details of the technique can be found elsewhere.13 After surgery, patients were allowed to ambulate as tolerated with lifting and heavy activity restrictions for 3 months.
Radiographic Measurements
All radiographic measurements were done with a digital computerized measuring tool. Radiographic analysis included measurement of the lateral bisegmental Cobb angle on the admission spine computed tomography image as well as AO fracture classification. The Cobb angle was measured from the superior endplate 1 vertebra above the fracture to the inferior endplate of the vertebra 1 level below the fracture. All patients obtained standing radiographs prior to discharge and during the follow-up period. Kyphosis on the postoperative and follow-up films were also measured using the Cobb angle. A negative angle measurement would indicate lordosis.
Outcomes Measure
The primary outcomes were angular correction immediately after surgery and loss of correction at follow-up appointment. Angular correction was defined as the difference between the preoperative and immediate postoperative Cobb angle. Similarly, loss of correction was the difference between immediate postoperative and follow-up measurements. Results were reported with mean, SD, and 95% CI. The average correction and loss of correction between open surgery and PPI for all patients were compared. We also compared open and PPI radiographic outcomes in several patient subgroups. Ultimately, we evaluated how body mass index (BMI), spine level, and AO fracture classification had an effect on outcomes regardless of surgical technique used.
Statistical Analysis
Data were managed using Microsoft Excel (Microsoft, Redmond, WA, USA). Mean, SD, median, and 95% CI were calculated for continuous variables. The Shapiro-Wilk test was used to assess for normality of continuous variables. Student’s t test was used to evaluate continuous variables with normal distribution, and Wilcoxon’s rank-sum test was used as the nonparametric alternative for continuous variables. Frequencies were calculated for categorical variables. Fisher’s exact test and χ 2 analysis were used to evaluate relationships between categorical variables. An a priori α was set at 0.05 for significance. Multivariate logistic regression was performed to evaluate factors influencing angular correction. All analyses were performed using SAS v9.4 statistical software (SAS Institute, Cary, NC).
Results
A total of 91 patients were included in the study, 65 patients (71%) underwent open surgery and 26 were operated with PPI techniques. There were 61 men (67%) and 30 women, with a mean age of 38.9 ± 15.5 years (range 17–82 years ) and BMI of 26.0 ± 5 kg/m2. Both groups were comparable in terms of age, sex, and BMI (Table 1). Patient groups were comparable in terms of Charlson Comorbidity Index, neurological status, American Society of Anesthesiologists score, and polytraumatic status. The most common mechanism of injury was motor vehicle accidents (n = 45, 49%), followed by fall from height (n = 37, 40%).
Comparison of patient characteristics between open and PPI cohorts.
Upon fracture evaluation, there were significantly more thoracic (T1-T9) fractures that underwent open surgical approach when compared with PPI, 34 (52%) vs 6 (23%) (P = 0.02) (Table 2). There were more AO type C (translational injuries) in the open surgery group and more AO type A (compression fractures) in the PPI group. Of the 30 AO type A fractures, there were: 25 AO type A4 complete burst fractures, 2 A3 incomplete burst fractures, and 3 A2 pincer-type fractures. All AO type B fractures were B2-flexion-distraction injuries. The open surgery group had significantly more instrumented segments.
Comparison of radiographic characteristics and surgical variables between open and PPI patients.
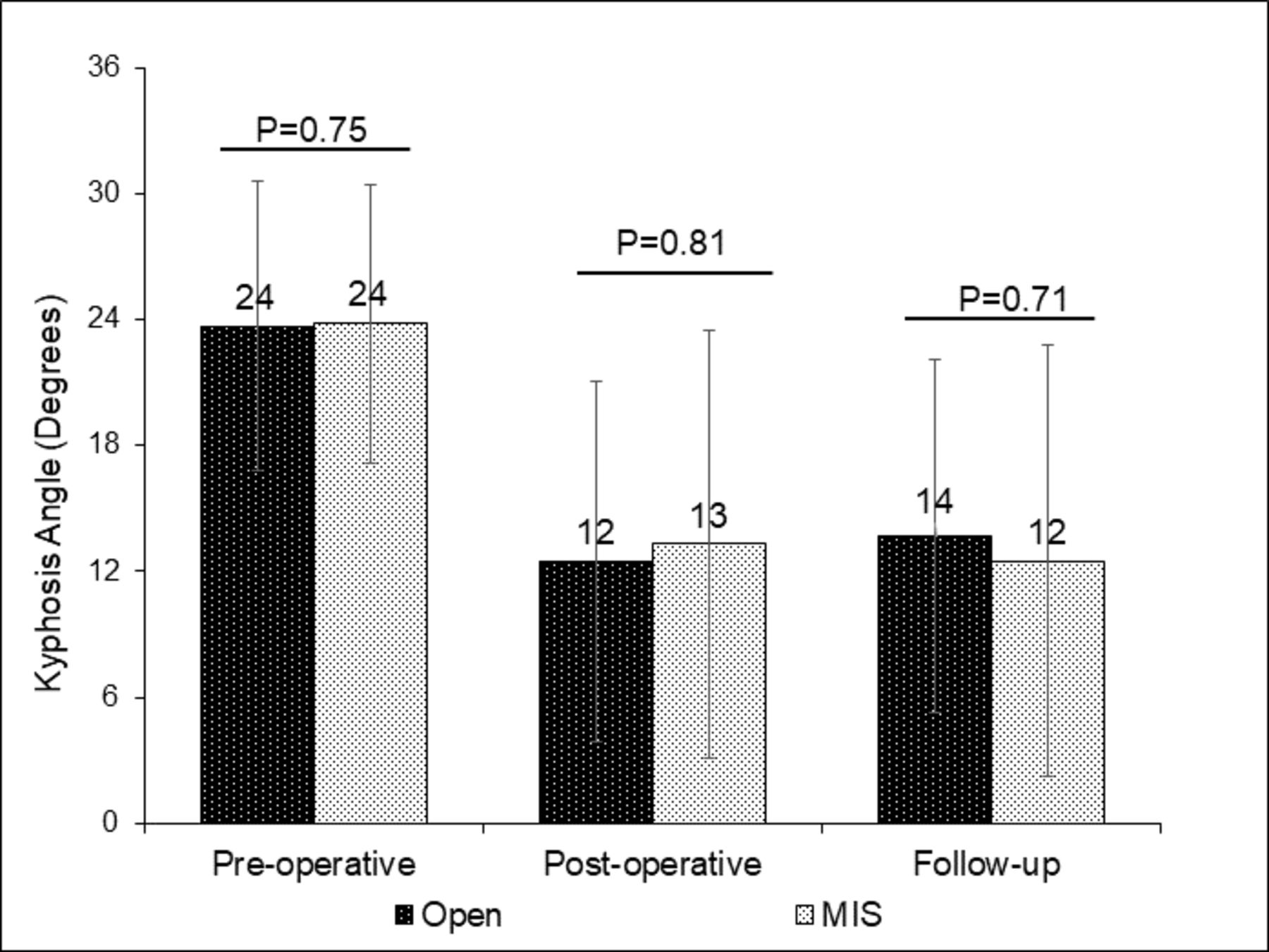
The mean angular measurements were comparable between groups at the preoperative, immediate postoperative, and follow-up period. The preoperative kyphosis was same for both open and PPI, with a mean and SD of 24° ± 7° (P = 0.75) (Figure 2). Postoperatively, the average angle for the open group was 12° ± 8° (95% CI: 10°–14°) and 13° ± 10° (95% CI: 9°–17°) for the PPI group (P = 0.71). The mean angle at follow-up for the open group was 14° ± 8° (95% CI: 11°–16°) compared with 13° ± 10° (95% CI: 8°–17°) for the PPI group (P = 0.67). Follow-up radiographs were available for 70 of the 91 patients included in study, with both groups having comparable length of follow-up (open, 127.2 ± 91.4 days vs PPI, 104.5 ± 53.3 days, P = 0.48). Of the 21 lost to follow-up, 15 were from open and 6 were from PPI group.

Comparison of mean kyphosis angle at preoperative, postoperative, and follow-up period between open and percutaneous pedicle instrumentation. MIS, minimally invasive surgery.
When evaluating our main outcomes, we observed that there was no significant difference detected in correction achieved postoperatively as well as loss of correction between surgical technique groups (Table 3). On average, the open group corrected 11° ± 9° (95% CI, 9°–13°) compared with the PPI group 11° ± 10° (95% CI, 6°–15°) (P = 0.81). Similarly, upon follow-up, open group lost an average of 1° ± 2° (95% CI, 1°–2°) and the PPI group lost 1° ± 3° (95% CI, 0°–2°) (P = 0.82). Additionally, we evaluated patient subgroups based on BMI, spinal level, and morphology of fracture, and found that these patient characteristics had no significant effect on outcomes achieved between the 2 surgical techniques.
Comparison of angular correction and loss of correction between open and PPI in all patients and selected patient subgroups.
A separate analysis was then performed to evaluate factors that influence angular correction and loss of correction for the entire cohort regardless of surgical technique. Obese patients (BMI >30 kg/m2) corrected 4° ± 10° (95% CI, −1° to 10°) on average and had significantly less postoperative correction when compared with other BMI classes (P = 0.0009) (Table 4). A simple linear regression demonstrated that for each increased unit of BMI, there was a 0.75° (95% CI, −1.1° to −0.4°) decrease in correction achieved (P < 0.0001, intercept = 30.4, R 2 = 0.18). TL fractures achieved greater angular correction when compared with thoracic spine fractures. Additionally, patients with AO type A compression fractures had significantly less correction than other AO classes regardless of surgical technique (P = 0.026).
Comparison of angular correction and loss of correction by patient subgroups regardless of surgical technique used.
Discussion
PPI has been shown to be associated with lower blood loss, shorter operative time, less postoperative pain scores, and decreased infection rates in patients with TL trauma. Previous studies have shown that PPI can achieve similar postoperative angular correction when compared with traditional open approach.14–16 However, these studies also included fractures without significant sagittal angular deformity. Therefore, the aim of this study is to compare the amount of correction achieved between PPI and open approaches for patients with more than 15° of post-traumatic angular deformity. In this retrospective study of 91 patients, there was no significant difference in the degree of postoperative correction or loss of correction at last follow-up (mean 121 days) between PPI and open surgery.
The ability of PPI to achieve similar correction to open surgery has been previously evaluated. Pooled data from multiple meta-analysis studies have failed to identify a significant difference between radiographic outcomes achieved with PPI compared with traditional open surgery.14–16 While these findings corroborate this study, previous studies are limited because of their heterogeneity and inability to measure angular correction as their primary outcome. Additionally, most studies evaluated single-level burst fractures treated with short-segment fixation without taking into consideration the magnitude of preoperative kyphotic deformity.5–10
While the degree of correction obtained immediately postoperative and at final follow-up were similar between the 2 groups, BMI negatively impacted correction. BMI may play a role in appropriate operating room positioning and affect the ability to achieve deformity correction. Furthermore, time to surgery may play a role. Most of the patients in this study received surgery within 24 to 48 hours of presentation, resulting in mobile fracture segments for easier reduction. The effect of surgical timing on kyphosis reduction requires further study.
Jiang et al performed a randomized control trial comparing radiographic outcomes for single-level TL burst fractures treated with short-segment fixation through percutaneous or open surgery techniques. They found paraspinal open surgery achieved better angular correction. On average, open surgery patients corrected almost 9° more than PPI group, and this difference was higher when postural reduction (defined by >90% of vertebral body height) was not successfully achieved. This difference may be attributable to the percutaneous instrumentation system used for the study, which uses a different technique for rod screw insertion that may limit its reduction capacity. However, similar to previous studies and our results, loss of correction at long-term follow-up in this study was comparable between groups.6–10
PPI is also an option for AO type B tension band injuries. The management of these types of injuries has historically necessitated the use of posterior instrumentation and fusion given the concern for slow ligamentous healing. Due to this concern, there has been a reluctance to use fixation techniques that do not include bone grafting and fusion. In 2013, Grossbach et al7 identified 38 patients who suffered flexion-distraction injuries and were treated with open posterior instrumentation and fusion (n = 27) and PPI with percutaneous screw fixation (n = 11). The PPI group had larger preoperative kyphosis angle (6.45° vs 9.85°, P = 0.23) and postoperative kyphosis angle (1.45° vs 6.26°, P = 0.10) than the open group, but there was no difference in correction achieved. The radiographic outcomes did not differ between groups at a mean follow-up of 18.5 months. Similarly, our study demonstrates that PPI is an option for posterior ligamentous injuries in patients with AO type B injuries.
Fracture morphology has an effect on correction achieved. Our results show that AO type A injuries have significantly less correction when compared with other AO classes. This may be due to intact posterior column structures limiting correction and/or the difficulty to reduce anterior vertebral body height through a posterior approach. When we compared AO type A injuries between open and PPI, no difference was observed. Similar results were seen when evaluating AO type B individually between both surgical groups and also combined with type A fractures. However, the true effect of fracture morphology on radiographic outcomes still needs further investigation.
The overall reoperation rate for this study was 4.4%. The PPI cohort had 1 reoperation (3.8%) for removal of symptomatic hardware at 1 year following the index procedure. The open cohort had 3 cases (4.6%) that required reoperation: 1 removal of symptomatic hardware approximately 1.5 years after the index procedure and 2 revisions for mechanical hardware failure. In the first revision case, the patient developed a fracture of the lowest instrumented level (L4) with retropulsion of the intervertebral body cage approximately 1 month postoperatively, requiring revision instrumentation. In the second revision case, the patient developed pullout of the distal pedicle screws with loss of reduction approximately 2 weeks following the index procedure, requiring revision instrumentation. Further studies are needed for sufficient power to compare reoperation rates between PPI and open treatment of TL fractures.
In this study, the surgical approach was determined by the surgeon. All surgeons routinely perform both open and PPI management of TL fractures. PPI is the default surgical approach with certain factors that encourage changing to an open approach. For example, obesity, osteopenia/osteoporosis, and rotational deformities are managed through an open surgical approach due to the fluoroscopic targeting difficulty. Furthermore, high-grade translational or rotational deformities and prior spine surgery are stabilized through a posterior open approach to achieve posterior fusion. Finally, severe kyphosis or chronic post-traumatic deformity is managed through an open surgical approach to achieve the appropriate correction in the sagittal plane.
This study has some limitations related to study design. The inclusion criteria of having at least 15° of kyphotic deformity are relatively strict, reducing the sample size. However, 15° was chosen to study patients with high risk for post-traumatic kyphosis and to better characterize kyphosis correction. Furthermore, the retrospective nature of this study and the surgeon’s choice for open vs PPI likely resulted in some of the imbalance between the 2 cohorts, representing a possible selection bias. However, we believe that the cohorts remain sufficiently homogenous for evaluating short-term kyphotic correction. Future studies can incorporate our data for subgroup analysis to investigate if factors such as BMI, spine level, and AO fracture classification may play a role in the degree of correction achieved, independent of surgical technique. Further prospective analysis, with random allocation to PPI technique, would be needed to help understand the relationship between these variables and radiographical outcomes.
Despite its growing prevalence, the literature regarding the use of PPI stabilization techniques lacks high-level evidence and exists mainly in the form of retrospective case series. Longer-term follow-up studies will be necessary to determine if these newer modalities can withstand the tests of time. This study contributes to the literature by providing valuable, rare data for further comparison of operative traumatic thoracic and TL fractures.
Conclusion
PPI techniques provide equivalent postoperative angular correction and maintenance of correction compared with open surgery in thoracic and TL trauma patients. While further studies are needed to assess the long-term outcomes of patients treated with percutaneous pedicle screw fixation, this study provides further evidence that PPI is a feasible option for kyphosis correction in TL trauma.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Daniel Cavanaugh reports consulting fees from AlphaTec. Eugene Koh reports consulting fees from Biomet. Dan Gelb reports royalties or licenses from DePuy Synthes; payment or honoraria from DePuy Synthes (lecturer/speaker) and AO Spine North America (course faculty/lecturer); and stock from the Advanced Spinal Intellectual Property. Steven Ludwig reports royalties or licenses from Theime and Quality Medical Publishers, DePuy Synthes Spine and K2M/Stryker; consulting fees from DePuy Synthes Spine and K2M/Stryker; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or education events from AO Spine North America; stock or stock options from Innovaite Surgical Designs and Advance Spinal Intellectual Property; and a leadership or fiduciary role in the following groups: Society for Minimally Invasive Spine Surgery, Cervical Spine Research Society, American Board of Orthopaedic Surgery, Maryland Development Corporation, Journal of Spinal Disorders and Techniques, The Spine Journal, Contemporary Spine Surgery, and Nuvasive. The remaining authors have no disclosures.
Ethics Approval Institutional Review Board approval was obtained for this study (HP-00082698).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.