


Article Figures & Data
Figures
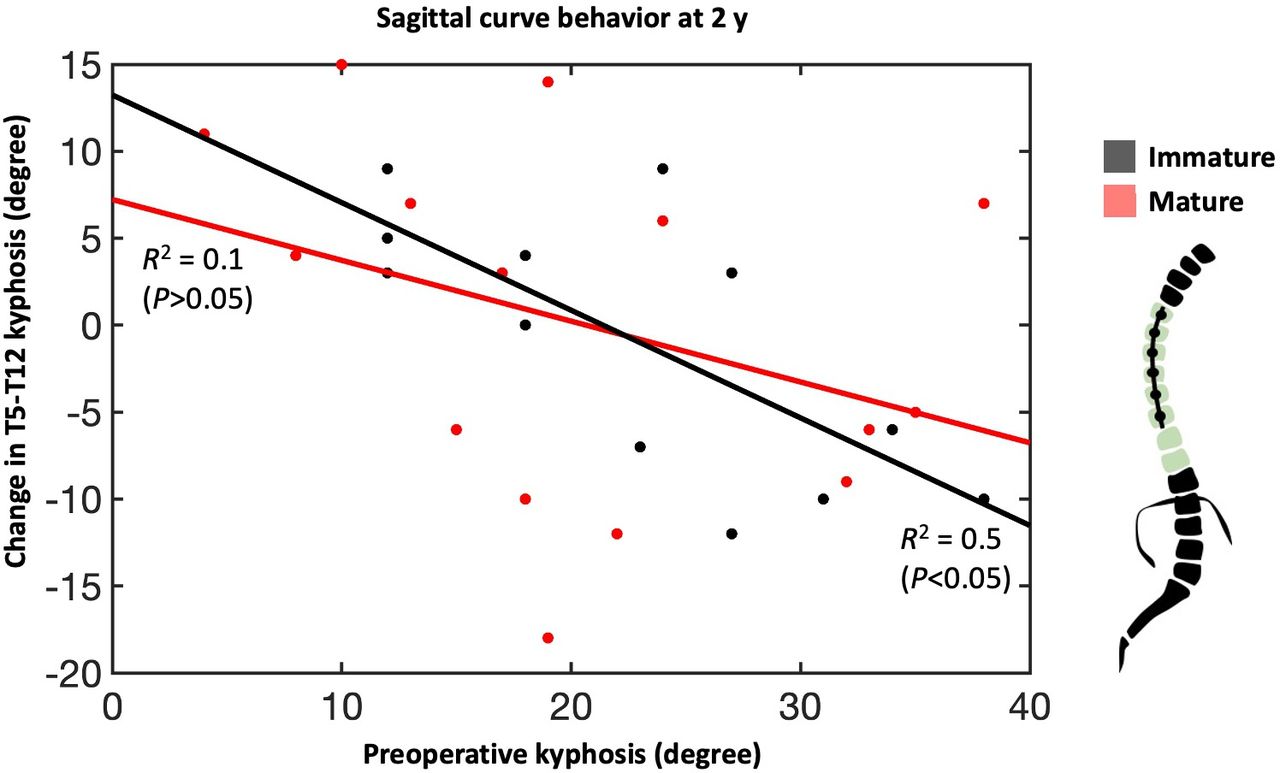
- Figure 1
Sagittal curve behavior, characterized as T5-T12 kyphosis, shows an inverse relationship between preoperative kyphosis and the change in curvature over 2 y. This relationship was statistically significant for immature patients whose spines are more amenable to growth modulation from anterolateral compression.
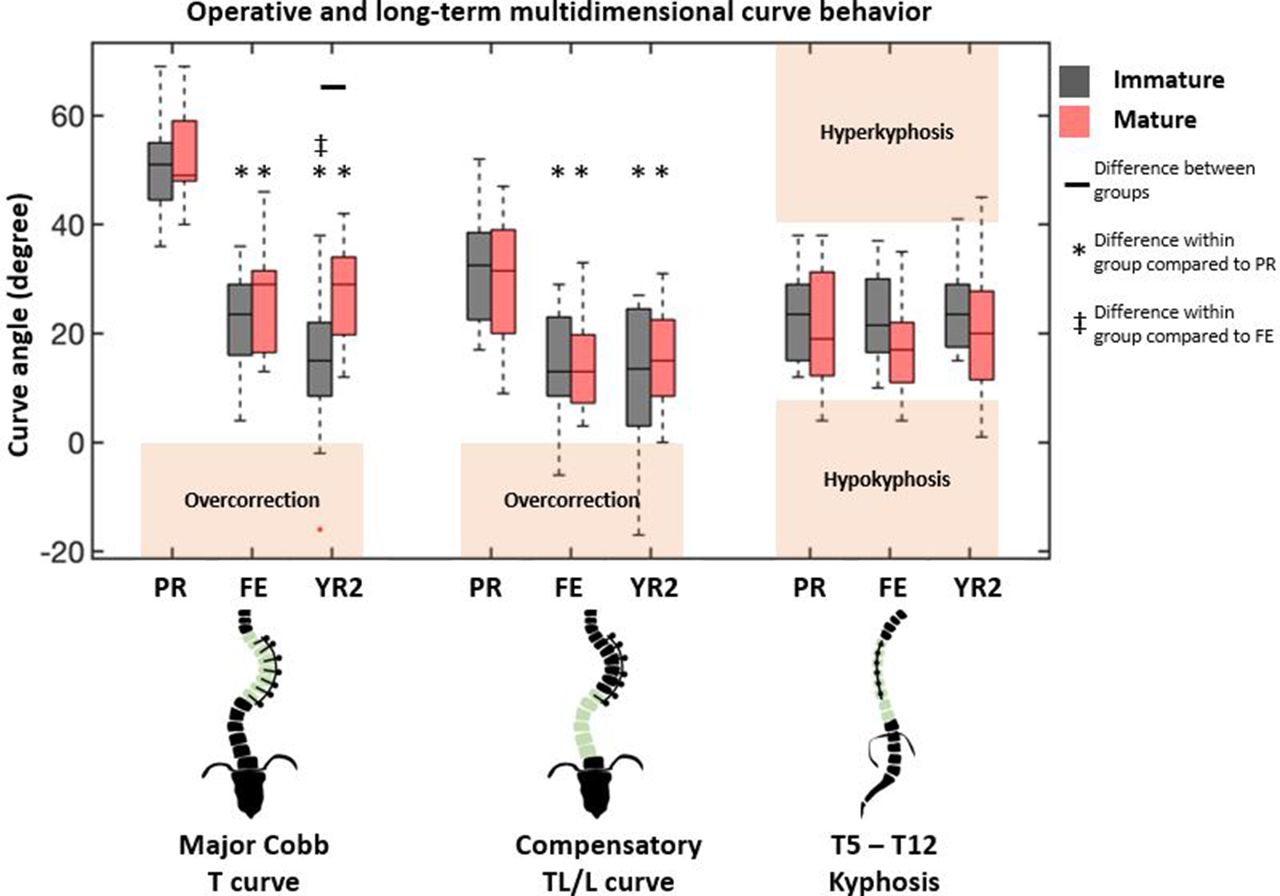
- Figure 2
Coronal and sagittal radiographic measurements at 3 timepoints show differences due to skeletal maturity only at 2-y follow-up in the instrumented thoracic curve. Differences between groups are designated by black bar. Differences within a group with reference to preoperative and first erect values are denoted by asterisk (*) and cross (‡), respectively. Boxplot interquartile range shows 25% to 75% with black bar indicating median. Outliers are designated by red plus sign (1.5 times interquartile range). Between- and within-group comparisons were done using a Mann-Whitney U test with Bonferroni correction (P < 0.05). PR, preoperative; FE, first erect; YR2, 2 y; T, thoracic; TL/L, thoracolumbar/lumbar.
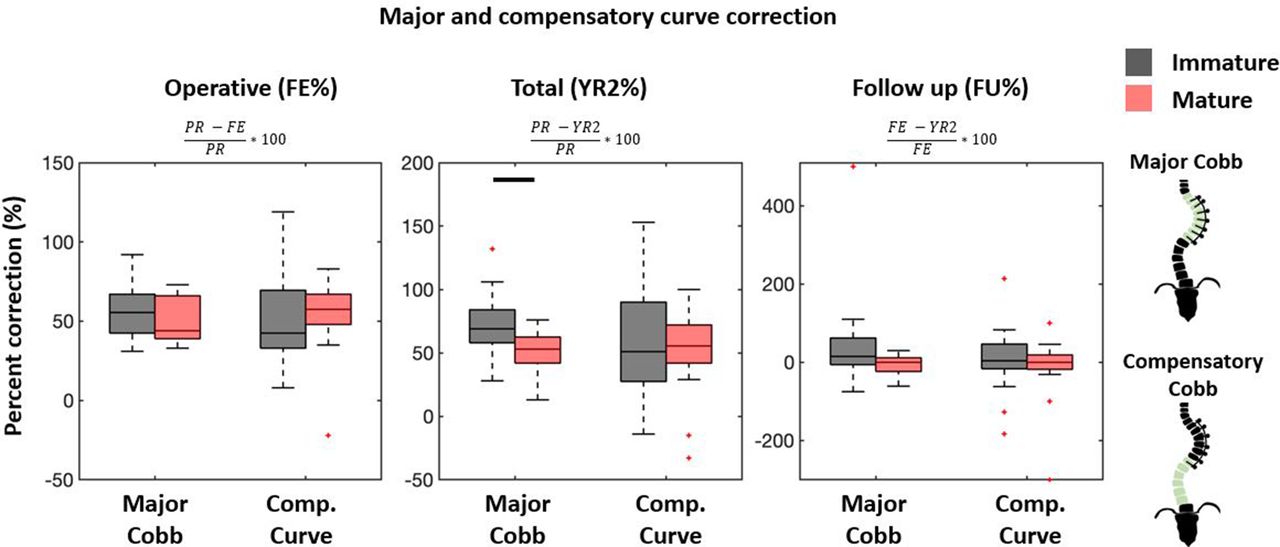
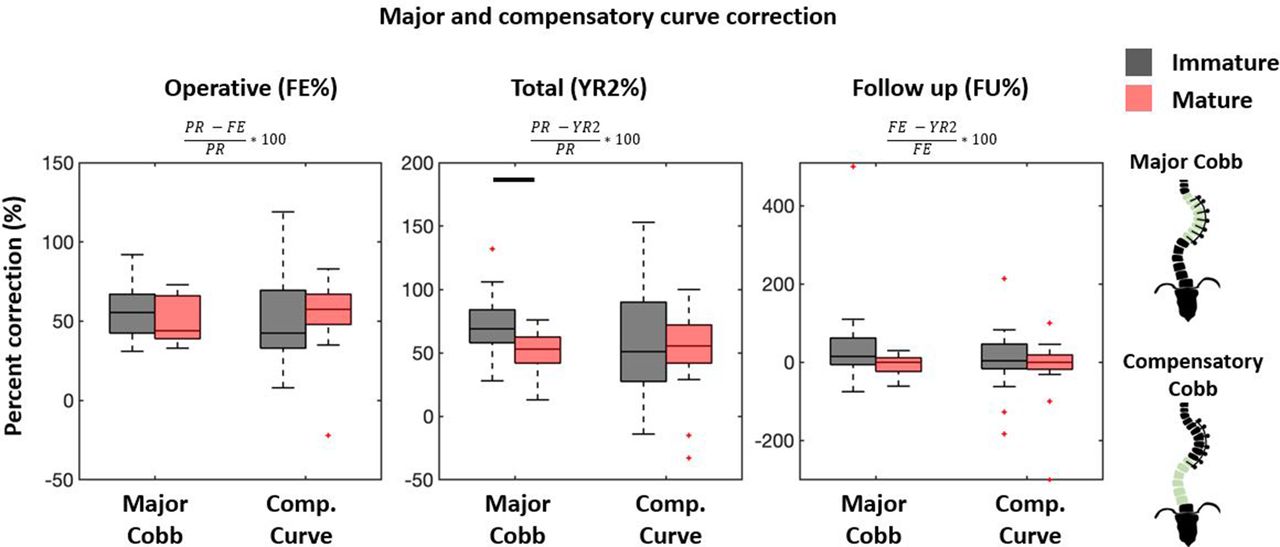
- Figure 3
Major and compensatory curve first erect and total percent correction (FE% and YR2%) are referenced to preoperative (PR) curve, whereas follow-up percent correction (FU%) compares FE with YR2. Percent correction beyond 100% defines overcorrection, and negative values define loss of correction. Large variations seen in FU% occurs with near-zero FE curves. Boxplots follow formatting described in Figure 2. Between-group comparisons were done using a Mann-Whitney U test with Bonferroni correction (P < 0.05).
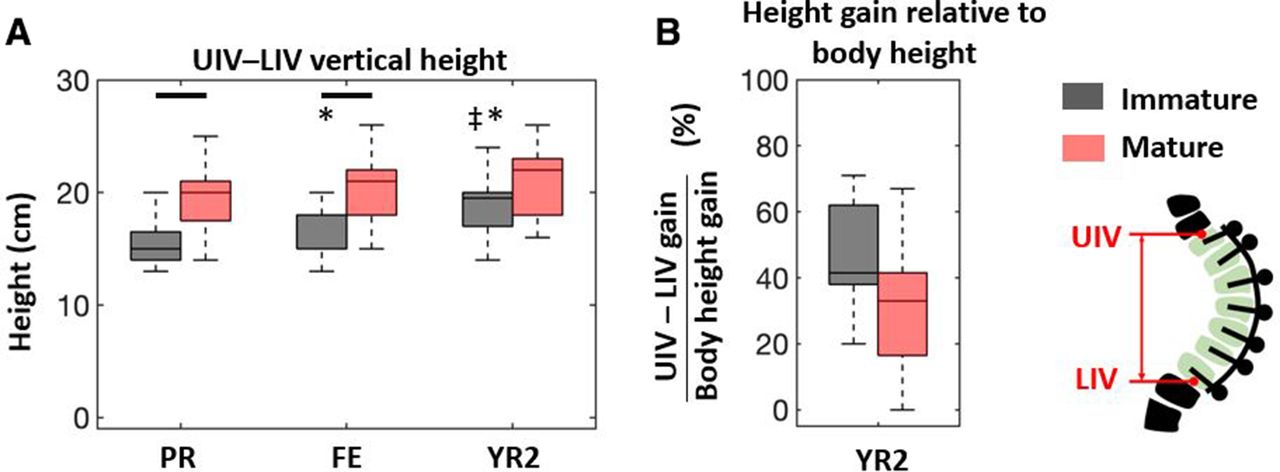
- Figure 4
(A) Vertical height changes of the instrumented segment show significant differences between groups at preoperative (PR) and first erect (FE) that disappear at 2 y (YR2). (B) The immature group had greater height gain at YR2, but this difference disappeared when normalizing by total body height gain. Between- and within-group comparisons were done using a Mann-Whitney U test with Bonferroni correction (P < 0.05). UIV-LIV, upper and lower instrumented levels.
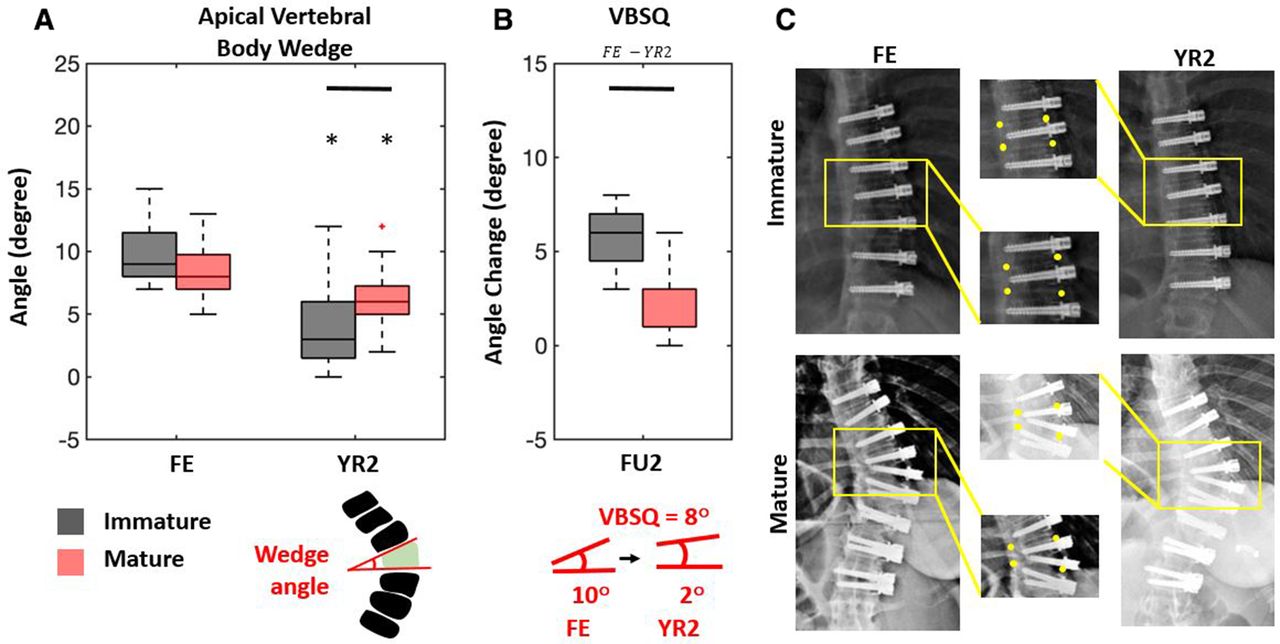
- Figure 5
(A) The degree of apical vertebral body wedging was assessed at first erect (FE) and compared with the 2-y (YR2) wedge. (B) Vertebral body squaring (VBSQ) quantifies the difference in wedging from FE to YR2, where more positive values indicate greater squaring. Immature patients showed significantly more squaring. (c) Representative immature and mature patients highlight changes in wedging. Between-group comparisons were done using a Mann-Whitney U test with Bonferroni correction (P < 0.05).
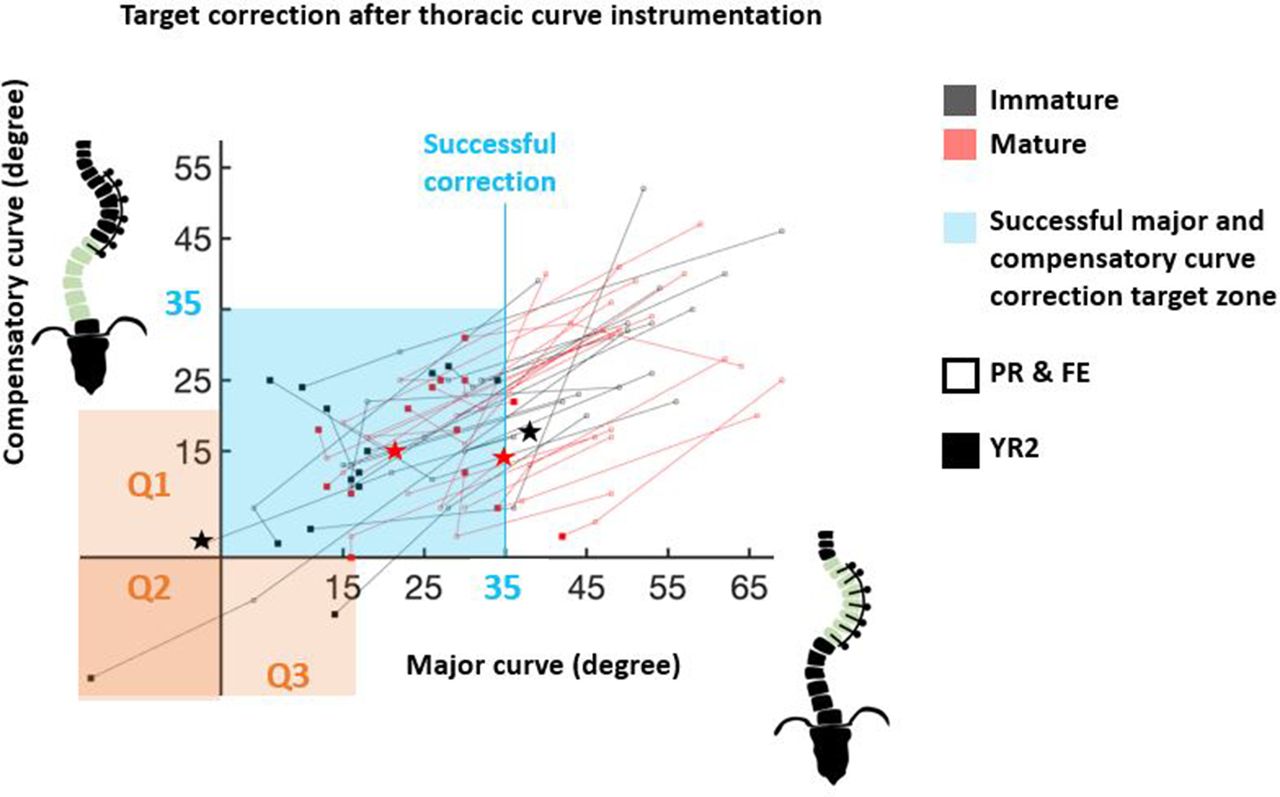
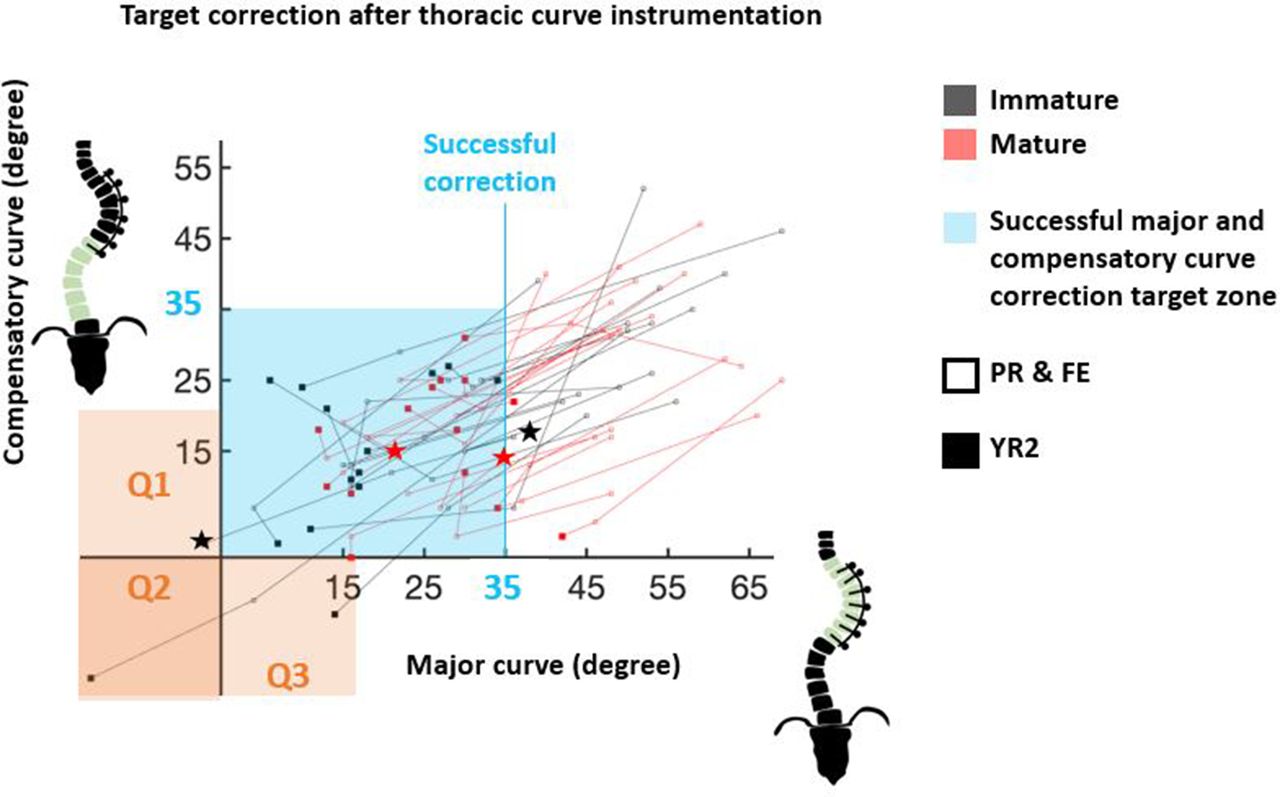
- Figure 6
Correction of major thoracic (instrumented) and compensatory thoracolumnbar/lumbar (noninstrumented) curves toward target region (light blue, <35°) is captured from preoperative (PR) (unfilled) and first erect (FE) (unfilled) to 2-y (YR2) follow-up (filled). Overcorrection of major (Q1), compensatory (Q3), or both curves (Q2) is highlighted in orange. Suspected breakage is indicated by star.
- Figure 7
Preoperative posteroanterior scoliosis radiograph of an immature group patient (Risser 2, proximal humerus ossification system 1 [PHOS 1]) with a 50° thoracic curve and 32° thoracolumbar curve. First erect (FE) radiograph shows correction of major and compensatory curves. FE% correction was 92%. The patient was Risser 4 (PHOS 5) at 24 mo, and posteroanterior radiograph shows major curve overcorrection (2-y percent correction [YR2%] = 132%), corresponding to a 500% follow-up percent change (from FE to YR2). Apical wedge angle was 8° at FE and 0° at YR2, generating a vertebral body squaring of 8°. Follow-up angles were measured between vertebra contained by the black bars, where white bars indicate preoperative angles. Yellow arrow indicates the apical vertebra, and yellow dots mark the vertebral body margins.
- Figure 8
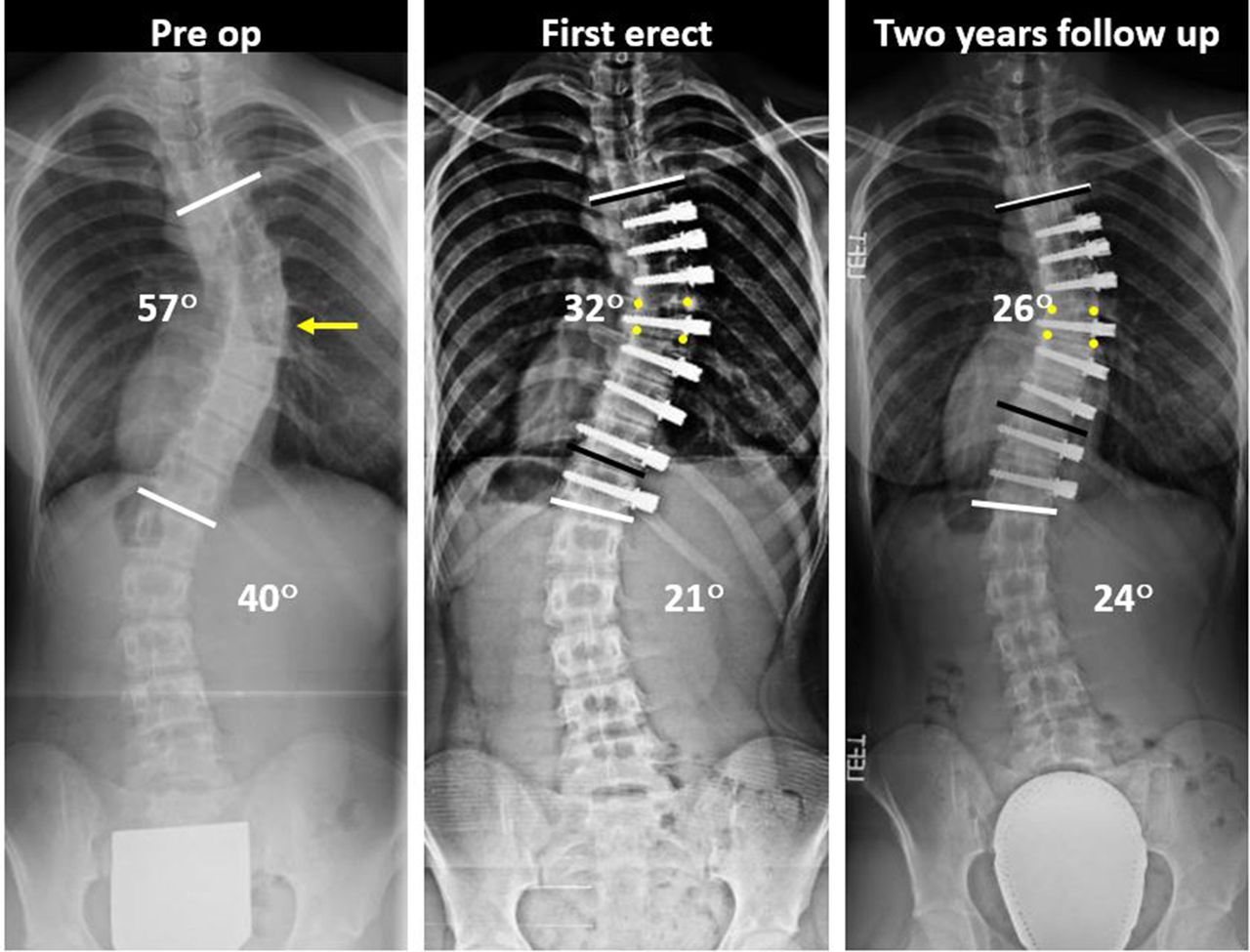
Preoperative posteroanterior scoliosis radiograph of a mature group patient (Risser 4, proximal humerus ossification system 4 [PHOS 4]) with a 57° thoracic curve and 40° lumbar curve. First erect radiograph shows correction of major and compensatory curves. At 24 mo, the patient was Risser 5 (PHOS 5), and posteroanterior radiograph shows maintenance of clinically successful correction. Apical wedge angle was 12° at first erect and 8° at 2-y follow-up, calculating a VBSQ of 4°. Follow-up Cobb angles were measured between vertebra contained by the black bars, where white bars indicate preoperative angles. The yellow arrow indicates the apical vertebra, and yellow dots mark the vertebral body margins.






Tables
Variable Skeletally Immature (Risser 0 to 2) Skeletally Mature (Risser 3 to 5) P Value Descriptives Number of patients 16 19 Follow-up, mo, median (range) 24 (24–39) 25 (24–32) 0.47 Female sex, n (%) 12 (75%) 6 (32%) 0.01 Age, y, median (range) 12.5 (9–16) 15 (12–18) <0.001 Height, cm, median (range) 156 (138–177) 169 (159–180) <0.001 Lenke classification 1 | 2 | 3 15 | 1 | 0 14 | 4 | 1 Preoperative Radiographic Major Cobb, degree, median (range) 51 (36–69) 49 (40–69) 0.77 Developmental Stage Risser, median (range) 1.5 (0–2) 4 (3–5) <0.001 Risser 0 | 1 | 2 | 3 | 4 | 5 6 | 2 | 8 | 0 | 0 | 0 0 | 0 | 0 | 6 | 12 | 1 PHOS, median (range) 2.5 (1–3) 4 (2–5) 0.02 PHOS 1 | 2 | 3 | 4 | 5 2 | 6 | 8 | 0 | 0 0 | 1 | 7 | 6 | 5 Triradiate cartilage closed, n (%) 11 (69%) 19 (100%) 0.49 Operative Data Levels tethered, median (range) 8 (6–9) 8 (6–9) 0.36 Upper instrumented level, most frequent level, n (%) T5, 9 (56%) T5, 9 (47%) 0.79 Lower instrumented level, most frequent level, n (%) T12, 9 (56%) T12, 8 (42%) 0.19 Cords used, 1 cord | 2 cords, n (%) 16 (100%) | 0 (6%) 16 (84%) | 3 (16%) 0.09 Thoracoplasty, n (%) 1 (6%) 2 (11%) 0.65 Estimated blood loss/estimated blood volume, %, median (range) 3.4 (0.8–7.1) 2.4 (0.9–12.4) 0.56 Operative time, h, median (range) 150 (105–210) 165 (105–240) 0.16 Length of stay, d, median (range) 5 (4–7) 5 (3–8) 0.29 Abbreviation: PHOS, proximal humerus ossification system.
- Table 2
Preoperative and follow-up radiographic curve behavior of instrumented major curve, noninstrumented compensatory curve, and T5-T12 kyphosis.
Variable Skeletally Immature
(Risser 0 to 2)Skeletally Mature
(Risser 3 to 5)P Value Skeletal maturity at final follow-up Risser, median (range) 4 (1–5) 5 (4–5) <0.001 Risser 0 | 1 | 2 | 3 | 4 | 5 0 | 1 | 1 | 2 | 11 | 1 0 | 0 | 0 | 0| 3 | 14 PHOS, median (range) 4 (2–5) 5 (4–5) 0.007 PHOS 1 | 2 | 3 | 4 | 5 0 | 1 | 1 | 8 | 3 0 | 0 | 0 | 1| 11 Instrumented major Cobb, degree, median (range) Preoperative 51 (36–69) 49 (40–69) 0.77 First erect 23.5 (4–36)a 29 (13–46)a 0.27 2-y follow-up 15 (−16 to 38)a,b 29 (12–42)a 0.008 Percent correction, % degree, median (range) First erect 55.5 (31–92) 44 (33–73) 0.37 Total 69 (28–132) 53 (13–76) 0.008 Follow-up 15 (−75 to 500) 0 (−61 to 30) 0.09 Successful correction (residual curve degree <35), n (%) First erect 16 (100%) 15 (79%) 0.21 Final follow-up 15 (94%) 15 (79%) 0.58 Noninstrumented thoracolumbar/lumbar curve, degree, median (range) Preoperative 32.5 (17–52) 31.5 (9–47) 0.77 First erect 13 (−6 to 29)a 13 (3–33)a 0.72 2-y follow-up 13.5 (−17 to 27)a 15 (0–31)a 0.77 Percent correction, % degree, median (range) First erect 42.5 (8–119) 57.5 (−22 to 83) 0.18 Total 51 (−14 to 153) 55.5 (−33 to 100) 0.85 Follow-up 4 (−183 to 214) 0 (−300 to 100) 0.64 T5-T12 kyphosis, degree, median (range) Preoperative 23.5 (12–38) 19 (4–38) 0.51 First erect 21.5 (10–37) 17 (4–35) 0.10 2-y follow-up 23.5 (15–41) 20 (1–45) 0.14 Change in T5-T12 kyphosis, degree, median (range) First erect −5 (−12 to 9) −5 (−13 to 16) 0.82 Total 1.5 (−12 to 9) 3 (−18 to 15) 0.61 Follow-up 4 (−7 to 10) 2.5 (−20 to 19) 0.94 - Table 3
Preoperative and follow-up body height, instrumented segment vertical height measurements, and apical vertebral body squaring.
Variable Skeletally Immature
(Risser 0 to 2)Skeletally Mature
(Risser 3 to 5)P Value Body height, cm, median (range) Preoperative 156 (138–177) 169 (159–180) <0.001 2-y follow-up 162 (153–178) 175 (162–184) 0.04 Height gain 8 (2–15) 3.5 (0–15) 0.04 Upper and lower instrumented levels vertical height, cm, median (range) Preoperative 15 (13–20) 20 (14–25) <0.001 First erect 18 (13–20)a 21 (15–26) <0.001 2-y follow-up 19.5 (14–24)a,b 22 (16–26) 0.12 First erect gain 1.5 (0–4) 1 (0–3) 0.15 Total gain 3.5 (1–8) 1.5 (0–4) <0.001 Proportional height gain, % 41.5 (20–71) 33 (0–67) 0.15 Apical vertebral body squaring, degree, median (range) First erect wedge 9 (7–15) 8 (5–13) 0.13 2-y follow-up wedge 3 (0–12)a 6 (2–12)a 0.02 Follow-up squaring 6 (3–8) 1 (0–6) <0.001 Variable Skeletally Immature
(Risser 0 to 2)Skeletally Mature
(Risser 3 to 5)P Value Revisions, n (%) 0 (0%) 0 (0%) Screw plowing, n (%) 1 (6%) 0 (0%) 0.27 Screw loosening, n (%) 0 (%) 0 (%) Cord breakage Number of breakages, n (%) 2 (13%) 2 (12%) 0.94 Survival time of breakages, mo, events (24, 39) (12, 42) Survival time all, mo, median (range) 24 (24–39) 25 (12–42) 0.32 Correction complications Overcorrection, n (%) 2 (13%) 0 (0%) 0.13 Overcorrection degree, median (range) 9 (2–16) 0 Loss of correction, n (%) 1 (6%) 4 (23%) 0.17 Loss of correction degree, median (range) 8 (8) 7.5 (6–11) 0.12 2-y follow-up Scoliosis Research Society Questionnaire Scores, median (range) Activity 4.1 (3.6–4.4) 4.4 (3–5) 0.24 Pain 4.5 (3.7–5) 4.7 (3.3–5) 0.26 Image 4.3 (3.4–4.9) 4.4 (3.1–5) 0.44 Mental 4.4 (3.2–5) 4.7 (3.4–5) 0.46 Satisfaction 4.5 (3–5) 4.7 (3–5) 0.57 Average 4.3 (3.6–4.8) 4.5 (3.3–5) 0.30
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.