


Article Figures & Data
Figures
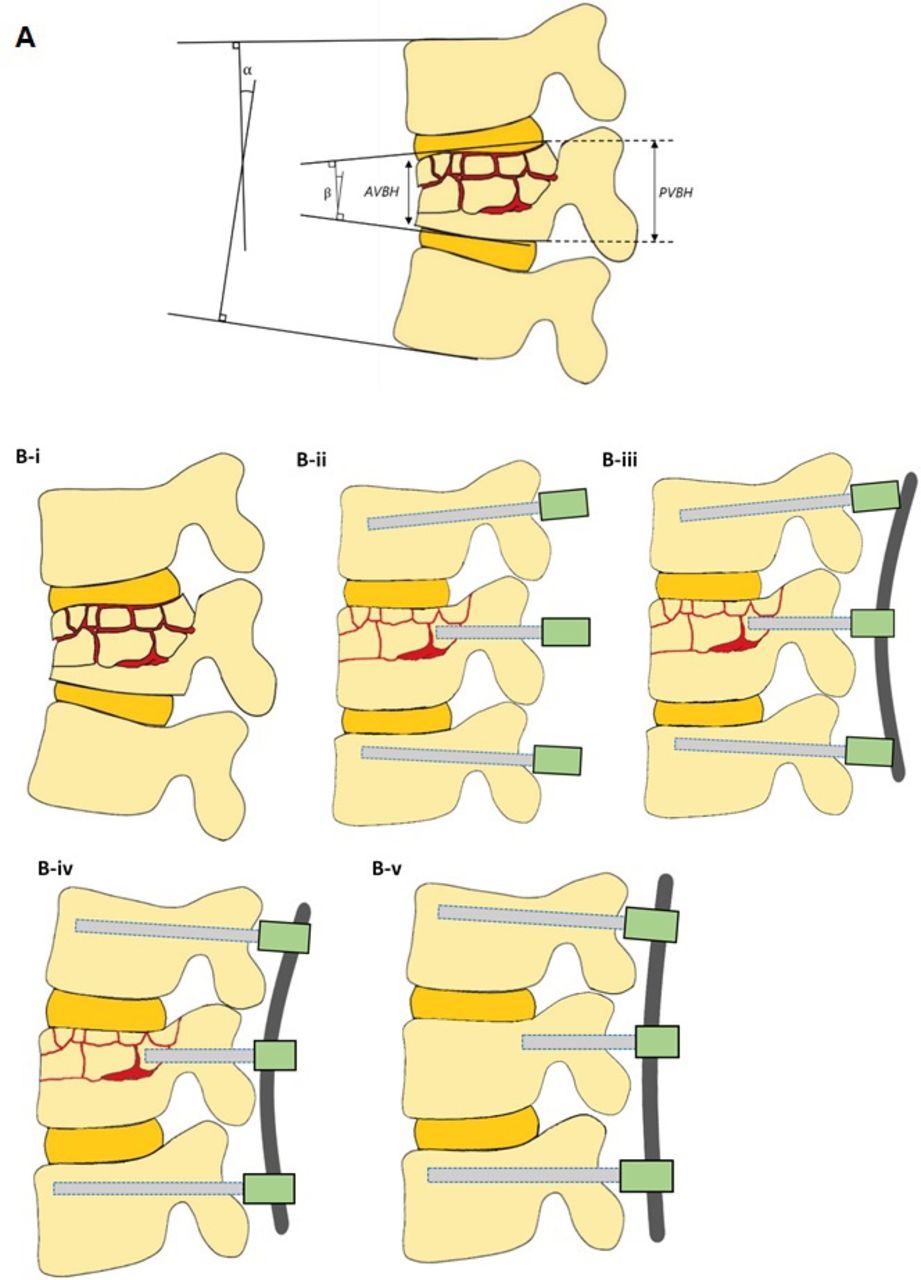
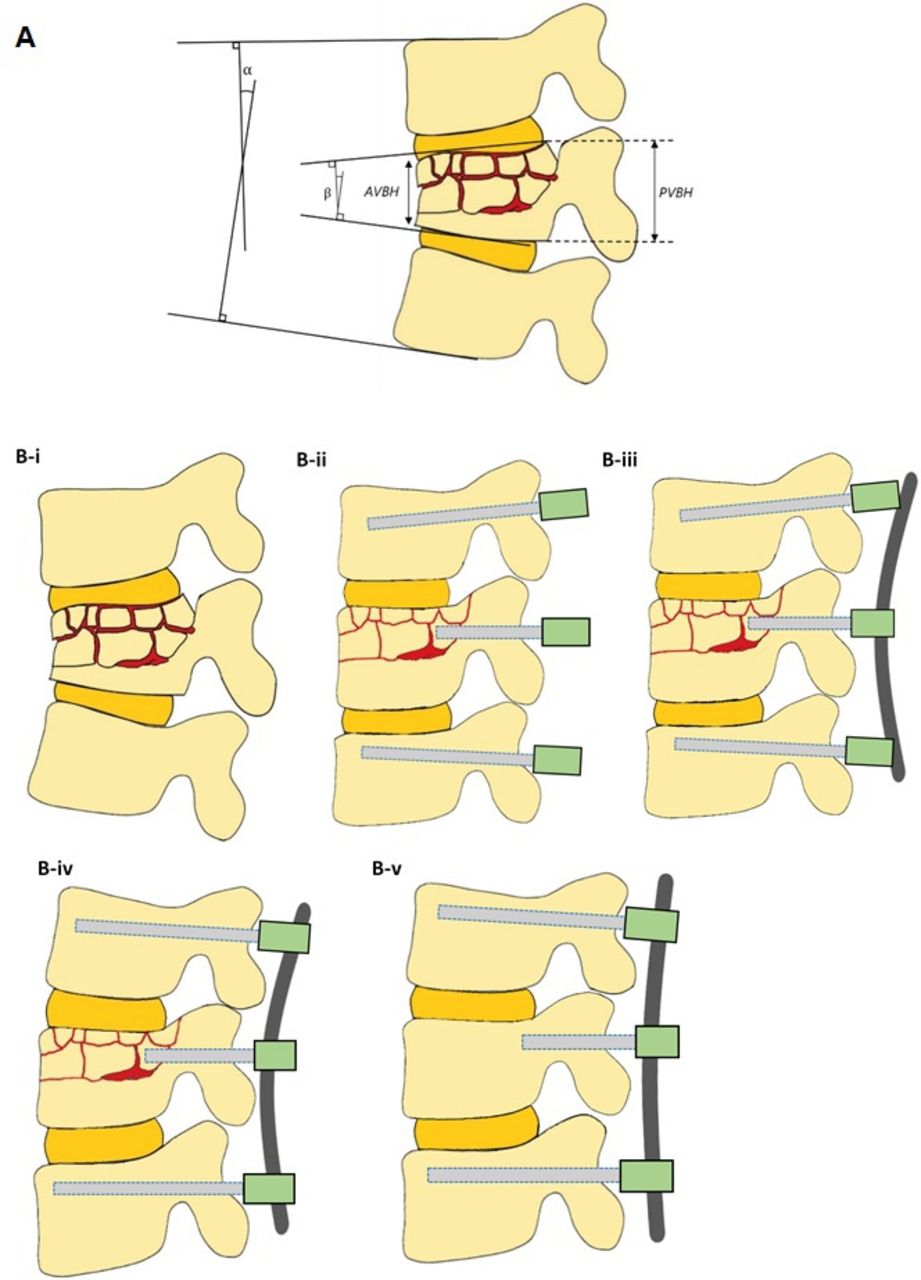
- Figure 1
(A) Pictorial representation of radiological parameters—vertebral wedge angle vs regional kyphosis angle. (B) Graphical representation of short-segment minimally invasive surgery fixation of thoracolumbar fractures with burst elements highlighting procedural nuances A: α, regional kyphosis angle; β, vertebral wedge angle; AVBH, anterior vertebral body height; and PVBH, posterior vertebral body height. B-i: Thoracolumbar fracture with burst elements. B-ii: Placement of bilateral pedicle screws into adjacent vertebrae, with one shorter pedicle screw inserted proud into fractured vertebra. B-iii: Fixation of contoured convex rod on intermediate short pedicle screw. B-iv: Fixation of contoured convex rod on screws in the adjacent vertebrae. B-v: Postoperative healed fracture maintaining correction.
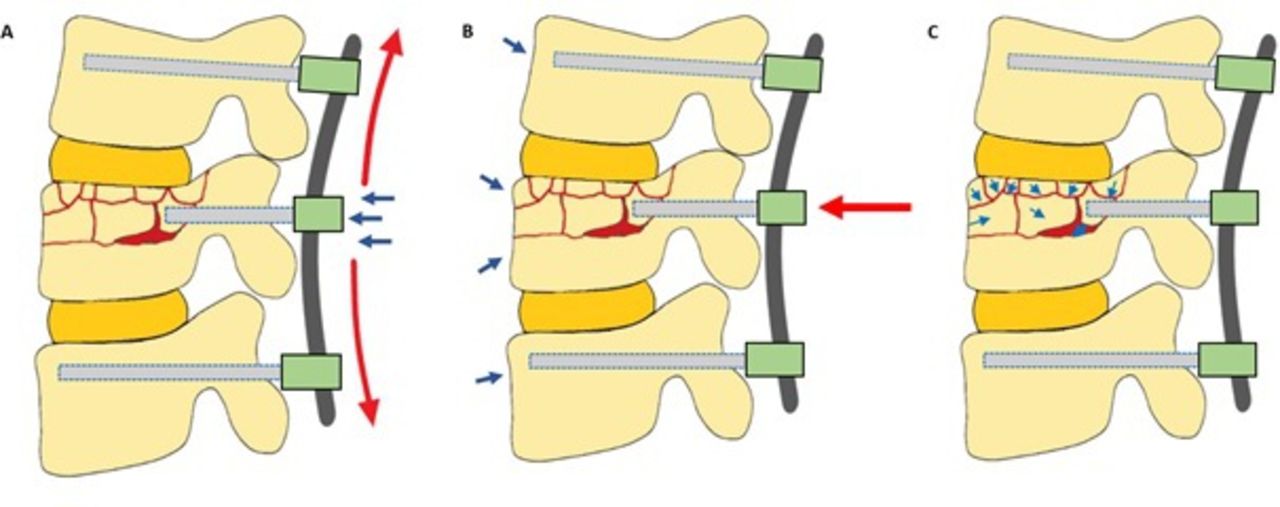
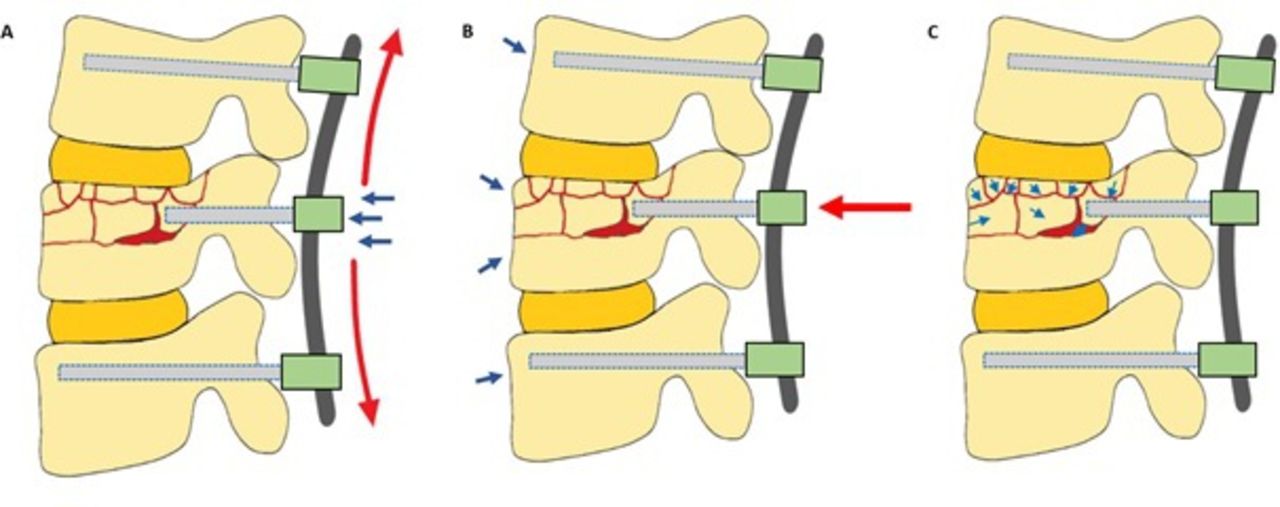
- Figure 2
Force diagram of pedicle screw-rod construct implanted with our technique. (A) Increased sagittal and anterior directed forces as a result of concave rod with shorter, proud intermediate pedicle screw placement. (B) Anterior directed forces from screw-rod construct with reactive posterior directed forces from anterior ligamentous complex and periosteal sleeve, reducing the burst fragments and intact bone close. (C) Interfragmentary motions of burst fragments.
- Figure 3
Pre-, intra-, and post-operative radiographs of a patient with flexion distraction injury with burst elements. (A) Preoperative computed tomography (CT), sagittal view. (B) Intraoperative correction sagittal radiograph. (C) Immediate postoperative CT sagittal and coronal views. (D) 6-month follow-up anteroposterior and lateral views. (E) 2-year follow-up anteroposterior and lateral views.

Tables
Inclusion Criteria Exclusion Criteria Rationale Age 17–74 y Age <16 or >75 y Minimum age of 16 yto reflect age of consent; maximum age of 75 y to exclude senile burst fractures. Thoracolumbar burst fracture T8-L4 Multiple burst fractures Short-segment fixation technique is aimed at single burst fractures. Fractured vertebral wedge angle ≤25° Fractured vertebral wedge angle >25° A significant wedge kyphosis indicates that severe loss of anterior vertebral body height may warrant direct decompression and/or corpectomy for vertebral reconstruction and sagittal correction. TLICS ≥4 – TLICS ≥4 is the minimum score warranting surgery. No, milda to moderateb neurological deficit Severe neurological deficitc Severe neurological deficit may have significant burst fragment retropulsion causing canal compromise that is likely to require direct decompression and fixation. Mild to moderate neurological deficit may have burst fragments retropulsion causing canal compromise that is amenable to indirect reduction. Abbreviations: MRC, Medical Research Council Scale for Muscle Strength; TLICS, Thoracolumbar Injury Classification and Severity Score.
↵a Dermatomal or nondermatomal sensory deficits in the lower limbs involving 1 nerve root and/or motor deficit involving 1 nerve root (2 ≤ MRC Grade ≤ 4).
↵b Dermatomal or nondermatomal sensory deficits in the lower limbs involving 1 to 3 nerve roots and/or motor deficit involving1 to 3 nerve roots (2 ≤ MRC Grade ≤ 4).
↵c Motor deficit involves >3 nerve roots with MRC Grade <2 or paraplegia/paraparesis.
Case
No.Age, y Sex Burst Fracture Level Preoperative ASIA Score Radiographic Results Individual Operative Details TLIC Score Denis
ClassificationAO Spine
ClassificationPLC Destruction ASA Score Instrumented Levels Intraoperative Complications Postoperative Complications 1 21 M L3 E 7 B B1 Y 1 L2, L3, and L4 N N 2 47 M L2 E 4 A B2 N 2 L1, L2, and L3 N N 3 22 M T12 E 7 B B1 Y 2 T11, T12, and L1 N N 4 21 F L3 E 4 A A3 N 2 L2, L3, and L4 N N 5 60 F L1 D 7 A B1 Y 3 T12, L1, and L2 N Yb 6 27 M L3 E 7 A B1 Y 2 L2, L3, and L4 N N 7 19 F L1 E 5 A A3 Y 2 T12, L1, and L2 N N 8 30 M L4 E 4 A B2 Y 1 L3, L4, and L5 N N 9 37 M L2 E 4 B B2 Y 2 L1, L2, and L3 N N 10 43 M T12 E 4 B B2 Y 3 T11, T12, and L1 N N 11 24 M L1 NAa 7 A A2 Y 3 T12, L1, and L2 N N 12 73 M L3 E 5 A B2 Y 2 L2, L3, and L4 N N 13 38 M L2 E 4 A A3 N 2 L1, L2, and L3 N N 14 38 M L4 E 4 A A3 N 2 L3, L4, and L5 N N 15 21 F L1 E 7 A B1 Y 2 T12 and L2 N N 16 18 F L4 E 4 B B2 Y 3 L3, L4, and L5 N N 17 64 M L1 E 2 B A3 N 3 T12, L1, and L2 N N 18 43 F L1 E 5 A B2 Y 2 T12, L1, and L2 N N 19 19 M L2 E 7 A B1 Y 2 L1, L2, and L3 N N 20 24 M L4 E 2 B A3 N 2 L3, L4, and L5 N N Abbreviations: ASA, American Society of Anesthesiologists; F, female; M, male; N, no; NA, not available; PLC, posterior ligamentous complex; TLIC, Thoracolumbar Injury Classification and Severity Score; Y, yes.
↵a Uncommunicative at the time of preoperative assessment.
↵b Developed postoperative ileus, which was subsequently resolved.
Characteristics N = 20 Patient characteristics Age, y 34.5 ± 16.4 Sex, men, n (%) 14 (73.6) Admission and operative details Time to admission, h 4.7 ± 2.4 Time to operating room, h 69.5 ± 44.4 Operative duration, min 108.6 ± 48 Intraoperative blood loss, mL 55 (10–1300) Total volume of blood transfused, mL 500 (250–750) Postoperative Course Length of hospital stay, d 11.5 (6–162) Outcomes Preoperative Intraoperative (After Positioning) Postoperative
(2 d)Follow-up 3 m 6 m 1 y 2-y Radiologic Vertebral wedge angle (°) 16.8
(−12.2 to 30.0)5.0
(−3.2 to 18.0)1.8
(−7.4 to 17.9)5.4
(−5.9 to 14)5.9
(−4.4 to 16.9)4.5
(−5.4 to 15.3)5.2
(−5.1 to 16.0)Regional kyphosis angle (°) 10.2
(−27.9 to 28.6)−4.0
(−29.0 to 19.2)−7.5
(−31.0 to 11.1)−6.3
(−25.5 to 18.4)−6.0
(−22.9 to 14.9)0.2
(−16.8 to 15.6)0.5
(−16 to 15.2)Coronal Cobb angle (°) 2.8
(−5.0 to 13.7)1.9
(−1.0 to 5.0)1.1
(0.0–5.0)1.0
(0.0–6.1)1.4
(0.4–5.6)1.7
(0.3–5.5)1.0
(0.3–5.8)AVBH, mm 20.3
(1.4–29.1)N/A 26.8
(15.6–39.1)25.5
(13.1–31.4)23.1
(12.6–31.2)23.1
(12.0–31.9)19.3
(12.2–29.1)PVBH, mm 28.4
(1.7–34.1)N/A 31.8
(18.2–35.9)31.4
(16.7–34.6)29.3
(16.5–35.1)27.7
(15.9–36.1)25.1
(16.0–35.0)Evidence of fracture healing, n (%) - - 0 (0) 12 (63) 15 (100) 15 (100) 15 (100) Implant Failure, n (%) - - 0 (0) 1 (5.9) 1 (5.9) 1 (5.9) 1 (5.9) Clinical Visual analog score 76 (4.8) - 48.5 (3.4) 31.2 (4.6) 25 (4.4) 20.3 (4.5) 11.5 (4.8) Oswestry Disability Index 84.5 (3.4) - 78.4 (3.3) 44.7 (5.5) 23.8 (4.0) 17.7 (5.1) 9.9 (4.5) Abbreviations: AVBH, anterior vertebral body height; PVBH, posterior vertebral body height.
Outcome Intraoperative (After Positioning) Postoperative Follow-up 3 m 6 m 1 y 2 y Vertebral wedge angle (°) 0.006 a
(−2.736)0.001 a
(−3.461)0.002 a
(−3.125)0.004 a
(−2.864)0.011 a
(−2.556)0.016 a
(−2.413)Regional kyphosis angle (°) 0.000a
(−3.823)0.000a
(−3.582)0.031a
(−2.154)0.039 a
(−2.059)0.191
(−1.306)0.208
(−1.258)Coronal Cobb angle (°) 0.124
(−1.538)0.050
(−1.960)0.088 (−1.705) 0.093
(−1.681)0.140
(−1.477)0.196
(−1.294)AVBH, mm N/A 0.001 a
(−3.375)0.010 a
(−2.586)0.020 a
(−2.328)0.158
(−1.413)0.937
(−0.078)PVBH, mm N/A 0.112
(−1.590)0.171
(−1.371)0.569
(−0.569)0.875
(−0.157)0.556
(−0.589)Visual Analog Score - 0.000 a
(−3.742)0.000 a
(−3.635)0.000 a
(−3.631)0.001 a
(−3.412)0.001 a
(−3.190)Oswestry Disability Index - 0.000 a
(−3.736)0.000 a
(−3.624)0.000 a
(−3.627)0.001 a
(−3.411)0.001 a
(−3.184)
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.