


Abstract
Background The kidneys, ribs, liver, spleen, and iliac crests can pose access-related issues to the disc space during both anterior-to-psoas (ATP) and transpsoas (TP) surgical approaches. The aim of this study was to identify and compare the presence and degree of obstruction caused by these structures for the ATP and TP approaches bilaterally from L1 to S1 using abdominal computed tomography.
Methods Presence of obstruction by a given structure was recorded if the structure was within ATP or TP borders. Degree of obstruction was calculated as the quotient of the structure measurement within the ATP or TP approach divided by the entire corridor length at the point of obstruction.
Results The percentage of time the left kidney was present during the ATP vs TP approaches at L1 to L2 was 44% vs 89% (P < 0.001), at L2 to L3 was 26% vs 75% (P < 0.001), and at L3 to L4 was 5% vs 19% (P < 0.001). For the right kidney, these values were 37% vs 78% (P < 0.001), 43% vs 71% (P < 0.001), and 11% vs 18% (P < 0.001). The percentage of time the left rib was present during ATP vs TP approaches was 41% vs 81% (P < 0.001) at L1 to L2 and 11% vs 26% (P = 0.413) at L2 to L3. With respect to the liver, the ATP approach was obstructed 56%, 30%, and 9% of the time at the levels of L1 to L2, L2 to L3, and L3 to L4; the liver was not present in L1 to L4 TP approach.
Conclusions This study is the first to both characterize and compare nonneurological structures at risk during ATP and TP fusion approaches bilaterally from L1 to S1 using abdominal computed tomography. Findings suggest the ATP approach poses less structures at risk relative to the TP approach with respect to the kidneys, ribs, and iliac crests bilaterally. The TP approach offers advantages compared with ATP approach with respect to the liver and spleen.
Clinical Relevance Findings from this study are clinically relevant for ATP and TP surgical approach planning.
Level of Evidence 3.
INTRODUCTION
Nonneurological anatomic structures such as the kidneys, ribs, liver, spleen, and iliac crests can pose access-related issues to the intervertebral disc space during both anterior-to-psoas (ATP) and transpsoas (TP) surgical approaches.1–4 Understanding and comparing the rates of access obstruction for ATP and TP may assist surgeons with approach-related decision-making and reduce intraoperative iatrogenic complications. Computed tomography (CT) of the abdomen offers distinct advantages compared with magnetic resonance imaging (MRI) of the lumbar spine with respect to visualization of organs within the ATP and TP approaches. Whereas CT of the abdomen allows for full visualization of abdominal contents in relation to both the spine and skin surface, MRI of the lumbar spine is limited to only spine anatomy. The aim of this study was to identify and compare the presence and degree of obstruction of the kidneys, ribs, liver, spleen, and iliac crests for the ATP and TP approaches bilaterally from the L1 to S1 disc levels using abdominal CT.
METHODS
Following IRB approval (#5220184), we performed a radiographic analysis of 100 patients who received abdominal CT imaging (GE Discovery 750 HD 64 slice CT Scanner) between December 2021 and April 2022. Patient consent was not required due to the nature of this retrospective radiographic study. All patients demonstrated clear axial and sagittal CT images and were aged between 18 and 80 years. Patients with history of spinal surgery, infection, or malignancy were excluded from review. Radiographic, demographic, and anthropometric data were retrieved using IMPAX6 (Agfa-Gavaert, Mortsel, Belgium) picture archiving and communication system. Radiographic measurements were conducted by 3 independent reviewers (J.R., S.M., and G.H.). To perform each measurement, a midsagittal view was first used to identify the disc space center. An axial slice of the disc space was then viewed, with the axial cut extracted from the mid cut of the disc space at each level. To ensure standardized measurements, this axial cut was utilized to measure both the ATP approach and TP approach as well as the percentage of obstruction caused by nonneurological structures within both approaches. The TP approach was characterized as the plane of the psoas muscle between the anterior and posterior margins divided into four equally sized zones based on the method described by Moro et al (Figure 1).5 Measured on the same slide, the ATP approach was defined bilaterally as the distance between the anteromedial aspect of the psoas major and the posterolateral aspect of the aorta, inferior vena cava, or common iliac vessels, depending on disc level and side ( Figure 2).1,6–8 The presence and degree of obstruction by each anatomical structure within the ATP and TP approaches were then calculated using the methods described in Figure 3. The percentage of time, or frequency, a given anatomical structure obstructed the surgical approach (ATP or TP) was calculated as the quotient of the number of times the structure was observed within the ATP or TP approach within the cohort, divided by 100 (the total number of patients included in this study).
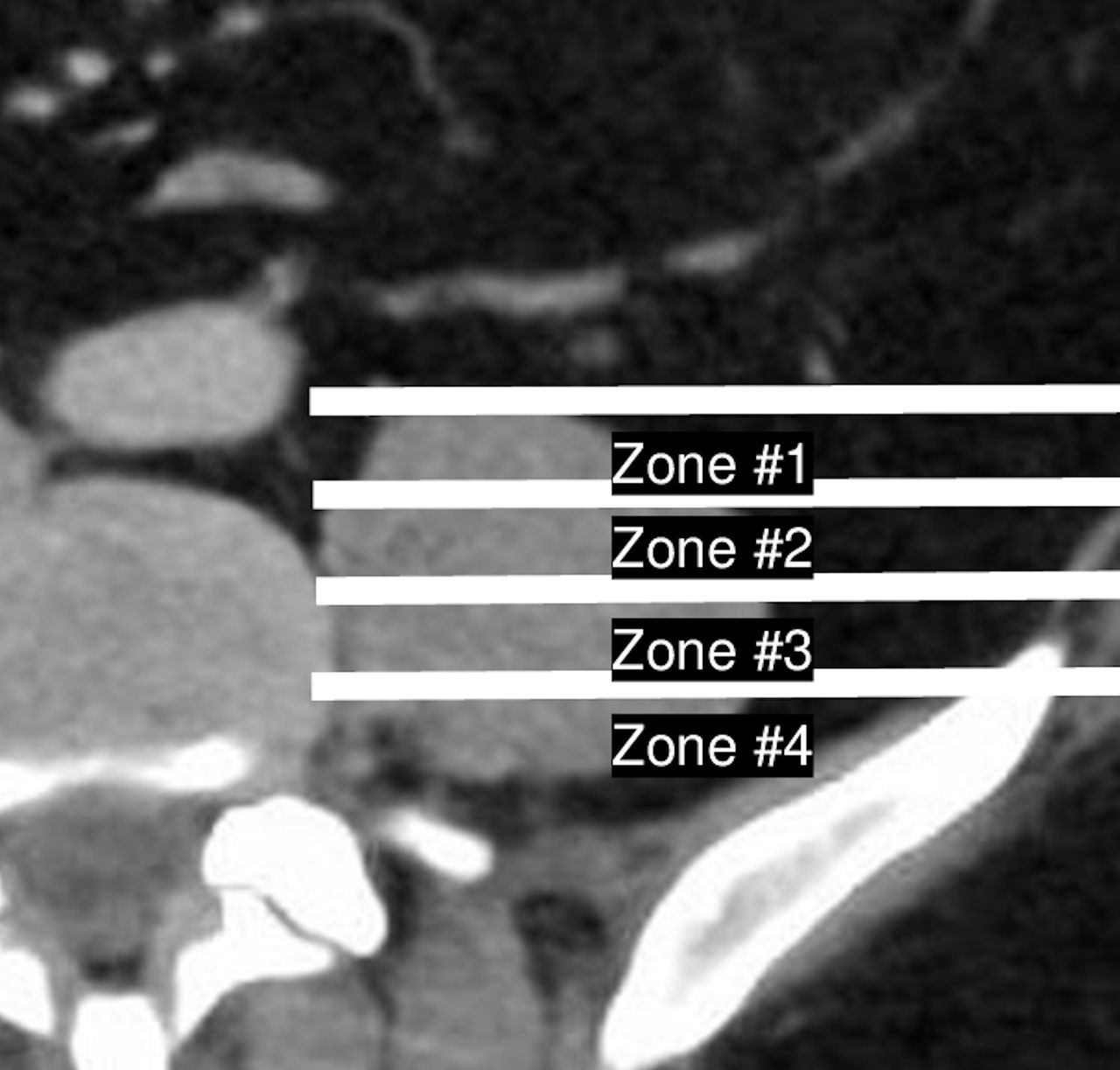
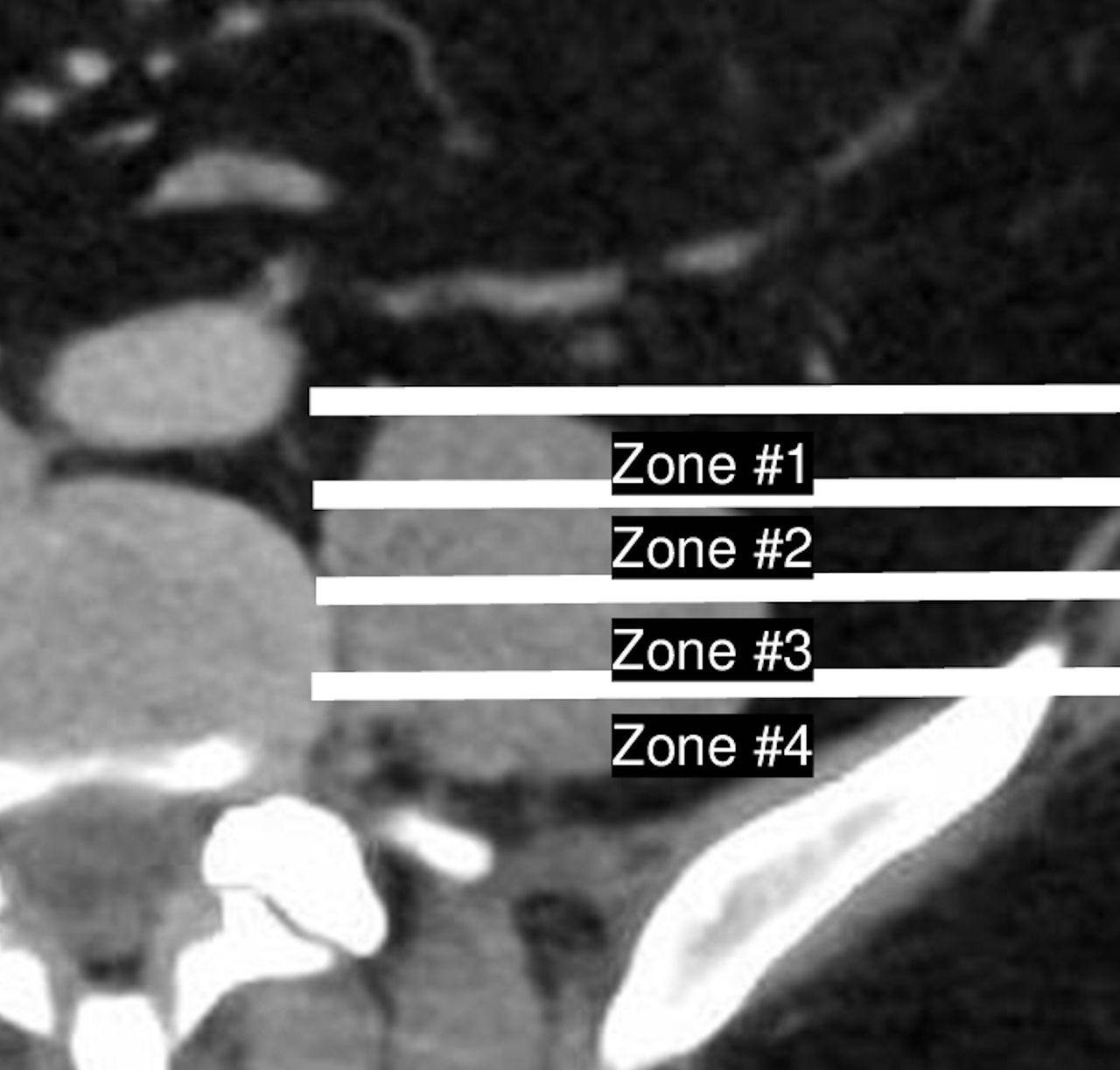
Transpsoas approach characterization by division of the psoas major into four zones. The psoas major was divided anterior-to-posterior into four equally sized zones using IMPAX6 measurement software.
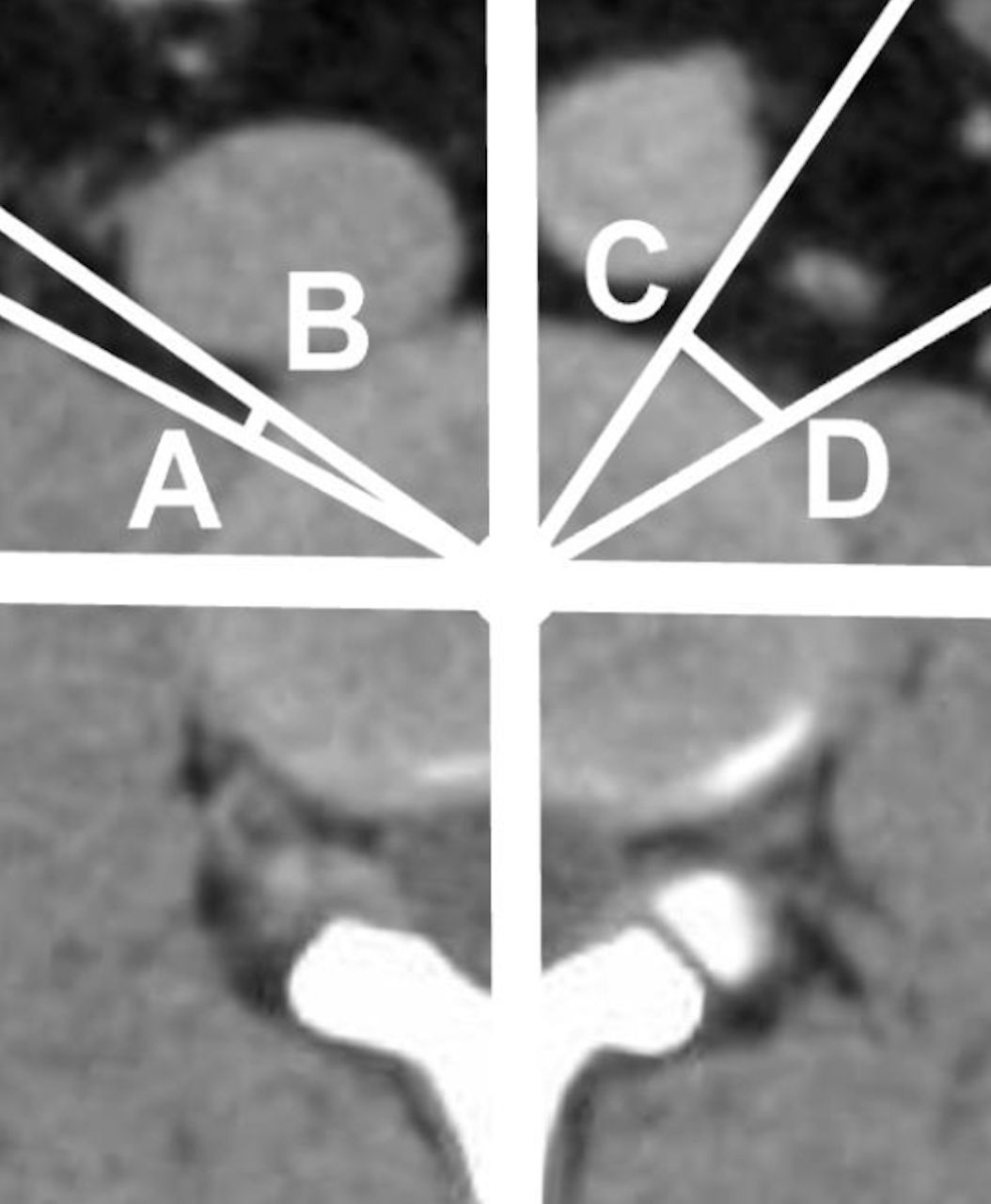
Anterior-to-psoas (ATP) approach characterization. The ATP approach was measured as the distance between the anteromedial aspect of the psoas major and the posterolateral aspect of the vasculature (line segments AB and CD).
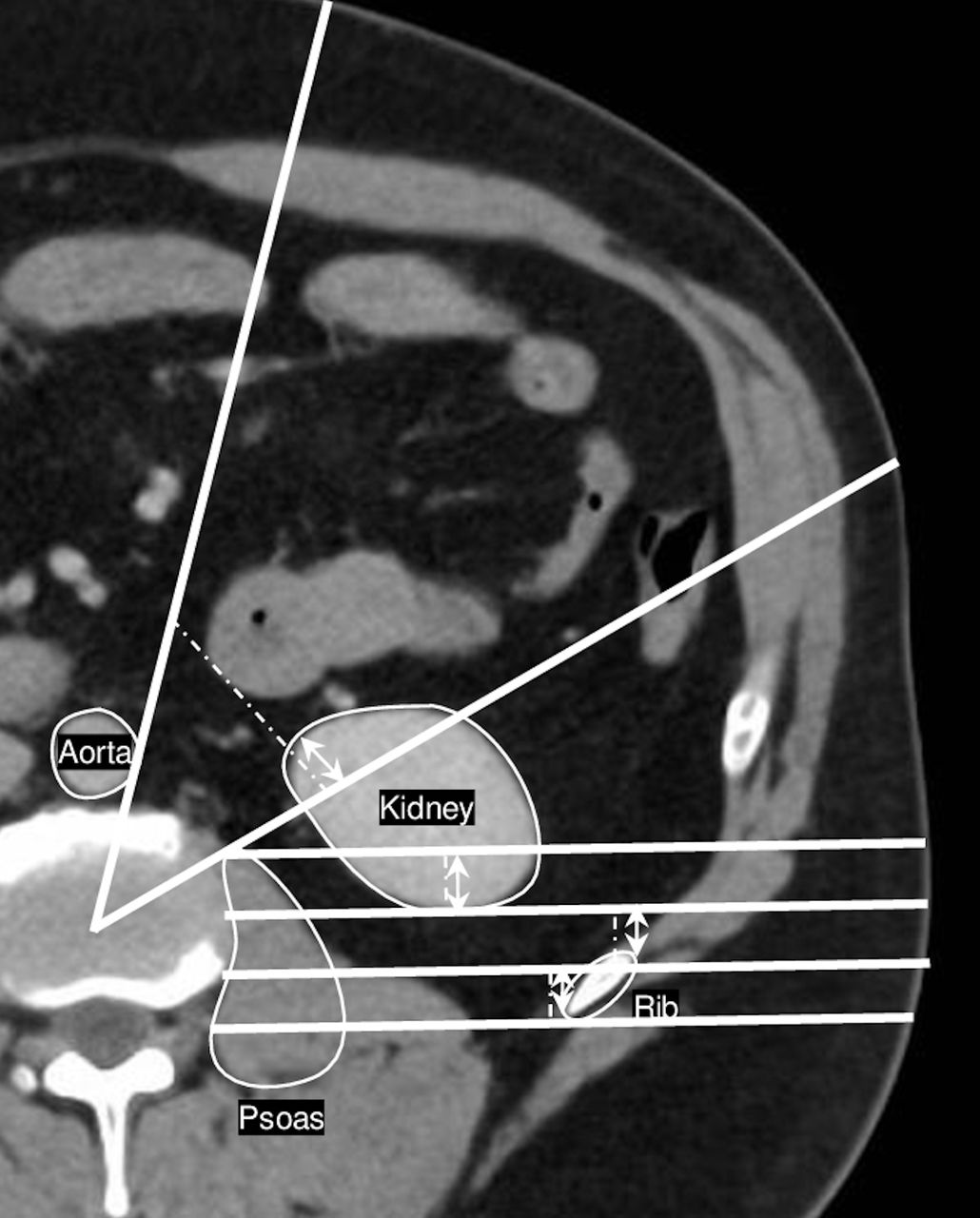
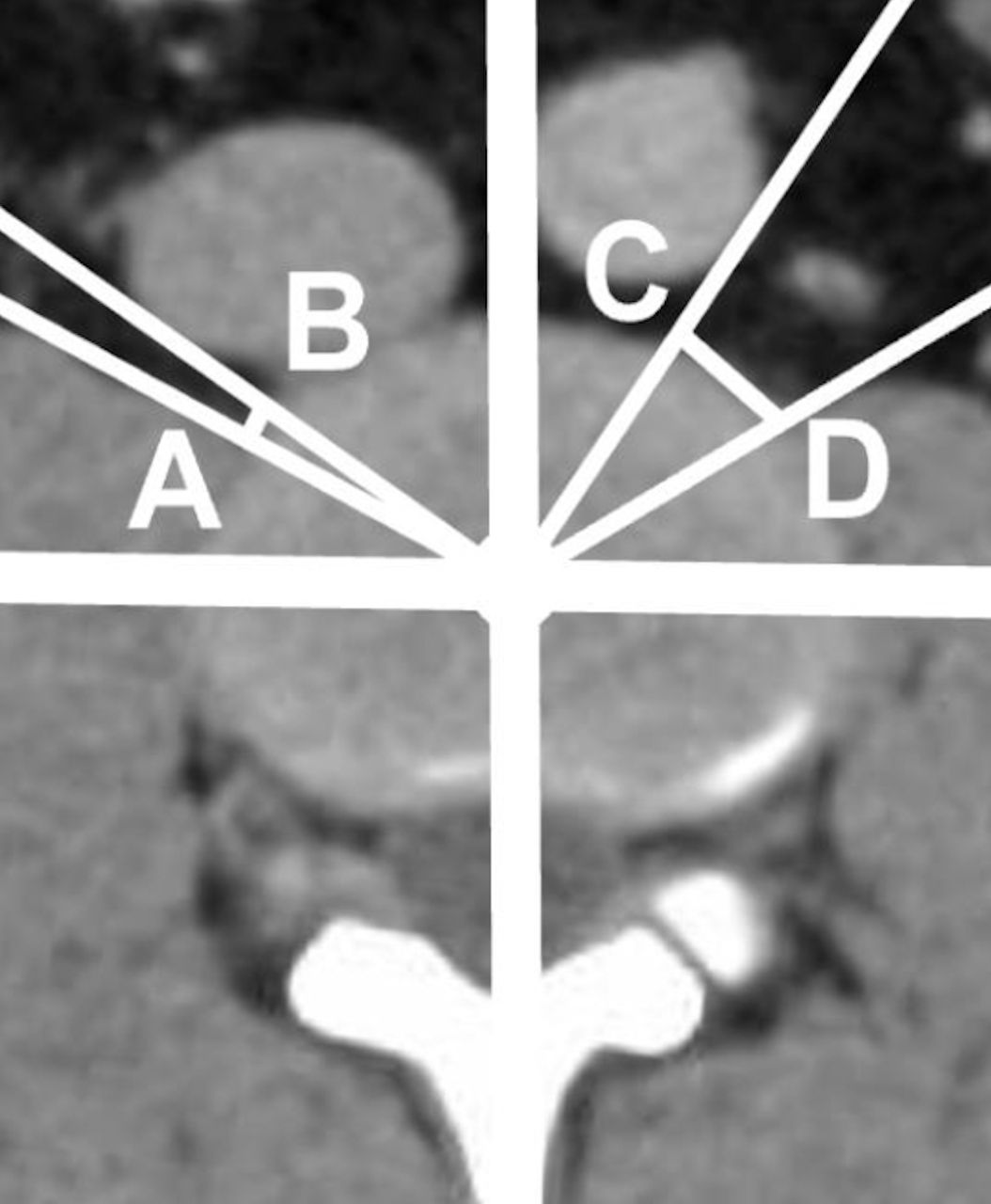
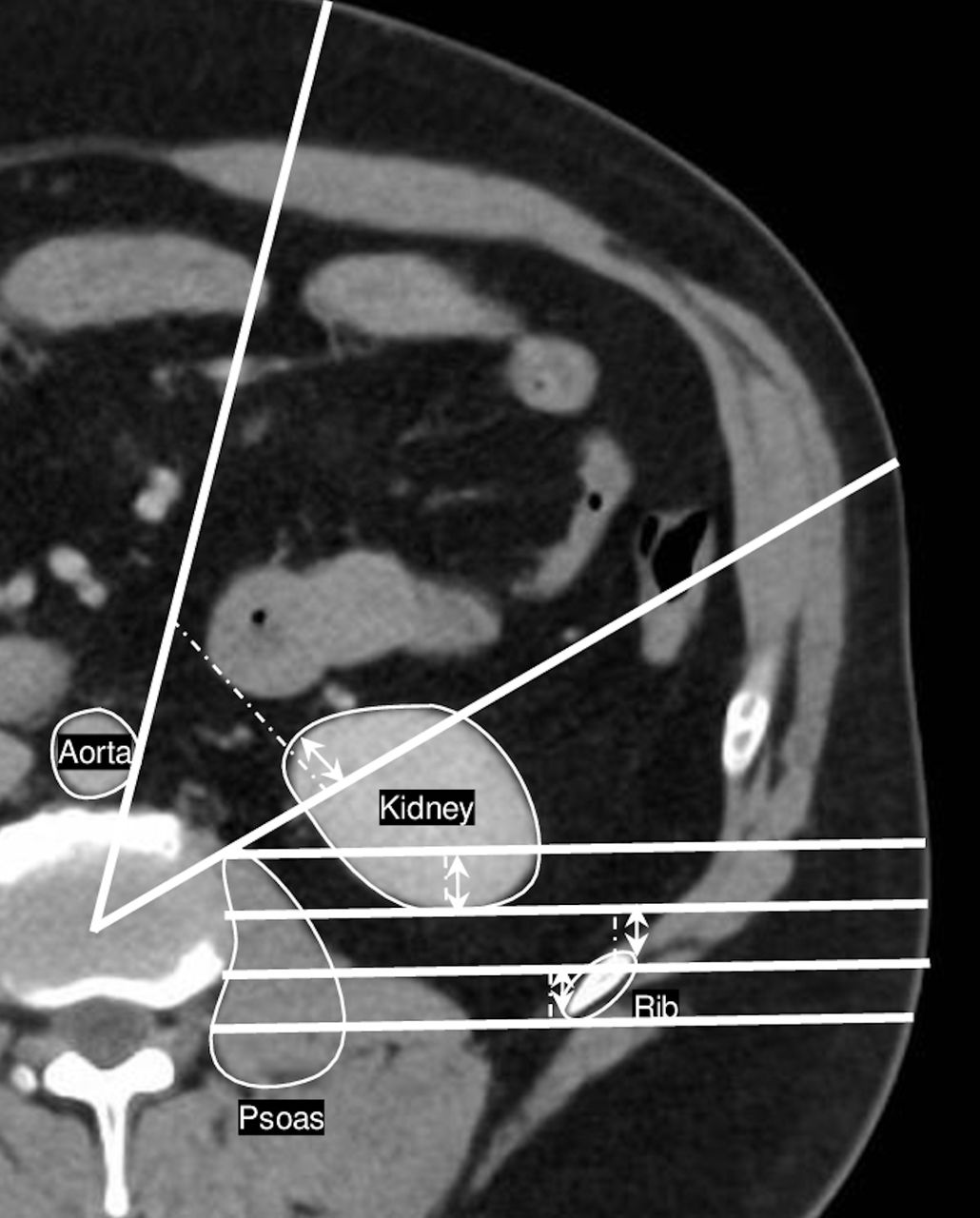
Measuring technique for structures at risk within anterior-to-psoas (ATP) and transpsoas (TP) approaches. The presence of obstruction by a given anatomical structure was recorded if the structure was within ATP and TP borders. Degree of obstruction was calculated as the quotient of the structure measurement within the ATP or TP approach (solid arrows) divided by the entire corridor length at the point of obstruction (hatched lines). If a structure occupied an entire zone (eg, kidney in TP zone #1 as shown above), this was recorded as 100% obstruction.
Statistical Analysis
Data collection was performed using Microsoft Excel version 16.58 (Microsoft Corporation, Redmond, WA, USA). SPSS version 28 (IBM Corporation, Armonk, NY, USA) was utilized for all subsequent statistical analyses with statistical significance defined as P < 0.05. The intraclass correlation coefficient (ICC) 2-way mixed model on absolute agreement was used to analyze interrater reliability.9 ICC was characterized as either poor, fair, good, or excellent corresponding to values of <0.40, 0.40 to 0.59, 0.60 to 0.74, and >0.75, respectively.10,11 Descriptive statistics utilized percentages, means, 95% confidence intervals (CIs), and SDs for radiographic, demographic, and anthropometric data. Homoscedasticity was assessed using homogeneity of variance tests and regression residual plots.12 Q-Q plots and Kolmogorov-Smirnov tests were used to assess for normality of data.13,14 To assess correlations among radiographic, demographic, and anthropometric data, Pearson’s correlation tests and multivariate linear regression models were constructed. Correlation coefficients were classified as weak, moderate, and strong corresponding to value ranges of 0 to 0.3, 0.3 to 0.7, and 0.7 to 1, respectively.15 Defferences in sex were analyzed using independent sample t tests. Measurement differences between disc levels were analyzed using 1-way analysis of variance with post-hoc Bonferroni and Tukey corrections. Differences between left- and right-sided measurements were evaluated using paired sample t tests.
RESULTS
We evaluated 50 female and 50 male subjects in our study. Demographic and anthropometric characteristics are detailed in Table 1. Calculated ICC was excellent with a value of 0.942 and a 95% CI of 0.937 to 0.955, remaining excellent at the lowest end of the CI. For all bilateral measurements and levels, no differences based on sex were observed. Additionally, no statistically significant associations between radiographic observations and age, height, weight, or body mass index were observed. Table 2 details the percentage of time the kidney, ribs, spleen, and liver were present within the ATP approach and the percentage of obstruction caused by each structure when present.
Patient characteristics, mean (SD).
Presence of kidneys, spleen, liver, and ribs in ATP approach.
Kidney
The percentage of time the left kidney was present during ATP vs TP approach at L1 to L2 was 44% vs 89% (P < 0.001), at L2 to L3 was 26% vs 75% (P < 0.001), and at L3 to L4 was 5% vs 19% (P < 0.001). For the right kidney, these values were 37% vs 78% (P < 0.001), 43% vs 71% (P < 0.001), and 11% vs 18% (P < 0.001), respectively. The frequency of presence and obstruction by the kidneys within the TP approach is presented in Table 3.
Kidney presence and obstruction of TP approach per side and zone.
Ribs
The percentage of time the rib was present during left-sided ATP vs TP approach—analyzing per the aggregate rib presence across all four zones—was 41% vs 81% (P < 0.001) at L1 to L2 and 11% vs 26% (P = 0.413) at L2 to L3. For the right-sided ribs, these values were 33% vs 67% (P < 0.001) at L1 to L2 and 10% vs 56% (P = 0.072) at L2 to L3. The frequency of presence and obstruction by the ribs within the TP approach per zone is displayed in Table 4.
Rib presence and obstruction of TP approach per side and zone.
Liver, Spleen, and Iliac Crest
With respect to the liver, the ATP approach was obstructed 56%, 30%, and 9% of the time at the respective levels of L1 to L2, L2 to L3, and L3 to L4, though the liver was not present in the L1 to L4 TP approach. Regarding the spleen, the ATP approach was obstructed 22%, 10%, and 3% of the time at the respective levels of L1 to L2, L2 to L3, and L3 to L4, though the spleen was not present in the L1 to L4 TP approach. Relative to the iliac crests, the TP approach was obstructed at the levels of L4 to L5 and L5 to S1, though the L4 to S1 ATP approach was not obstructed by the iliac crests. The frequency of presence and obstruction by the iliac crests within the TP is detailed in Table 5.
Iliac crest presence and obstruction of TP approach per side and zone.
DISCUSSION
This study offers novel findings to the literature by way of both characterizing and comparing nonneurological structures at risk during ATP and TP fusion approaches bilaterally from L1 to S1 using abdominal CT images. Previous research has evaluated the presence of single anatomic structures within the ATP or TP approaches such as vascular, neurological, or renal structures.1,4,16 This study, however, is the first to use abdominal CT to simultaneously compare the ATP to TP approaches with respect to several at-risk nonneurological structures. Comparing the rates of access obstruction for ATP and TP approaches may provide insight for preoperative decision-making as well as reduce intraoperative iatrogenic complications associated with these structures.
Kidney
Comparing the ATP and TP approaches, we found the kidneys obstructed the TP approach more frequently than the ATP approach across all levels (P < 0.001). Our study found the left-sided kidneys presented less obstruction compared with the right across all levels (P < 0.001). In an MRI-based study by Julian Li et al,1 obstruction of the left-sided ATP approach by the kidney was observed 22.5% and 1% of the time at the L1 to L2 and L2 to L3 levels, while no obstruction was observed from L3 to L5. On the right side, Julian Li et al found obstruction by the kidney was present 91.5%, 42%, and 4.5% of the time at L1 to 2, L2 to L3, and L3 to L4, respectively. Though our measurement technique is similar to Julian Li et al, our findings differ as we observed obstruction by the left-sided kidney 44% and 26% of the time at L1 to L2 and L2 to 3, and 5% of the time at L3 to L4. On the right side, we found obstruction present 37%, 43%, and 11% of the time from L1 to L4. While Julian Li et al did not investigate the percentage of obstruction caused by the kidneys, this discrepancy in findings highlights the need for further understanding of the ATP approach using several imaging modalities. While our measurements techniques were similar, the observed measurement differences may be explained by our study’s use of CT vs Julian Li et al’s use of lumbar spine MRI.
Ribs
Ribs were observed within the ATP approach at L1 to L2 and L2 to L3, though ribs were more frequently observed within the TP approach (P =). At level L1 to L2, the ATP approach poses less risk to the ribs compared with the TP approach. At L2 to L3, however, there was not a statistically significant difference on either side (P =). However, it should be noted that methodology to visualize the ribs using CT imaging is likely to underestimate the actual presence of rib at a given side and level due to the presence of obscuring soft tissue and angulation of the rib that can prevent it from being visualized on imaging for both ATP and TP approaches. Therefore, this study likely provides more conservative estimates regarding the presence of ribs within the ATP and TP approaches.
Liver, Spleen, and Iliac Crests
We found the spleen to be present 22%, 10%, and 3% of the time from L1 to L4 within the ATP approach, though the spleen was not observed within the TP approach. Similarly, we observed the liver 56%, 30%, and 9% of the time during ATP approach, though the liver was never observed during TP approach. Julian Li et al1 observed obstruction by the liver 38%, 15%, and 1.5% of the time from L1 to L4. Similarly, these discrepancies are likely explained by the enhanced visualization capability provided by abdominal CT as compared with lumbar MRI with respect to organs within the ATP and TP approaches.
The iliac crest, however, was not observed within the ATP approach at the lower lumbar levels and appears to pose limited concern for the ATP approach. This is in contrast with the TP approach, which is well-documented to pose access-related issues with respect to the iliac crests.17 Likewise, our study found obstruction by the iliac crests to be 46% on the left side and 43% on the right side at L4 to L5. At L5 to S1, the iliac crest was observed 88% on the left side and 89% on the right side, and when present, created total obstruction of the TP approach almost 100% of the time. As such, the TP approach appears to offer an advantage compared with the ATP approach with respect to the liver and spleen, while the ATP approach poses significantly less risk with respect to the iliac crests.
Limitations
Imaging-based studies such as our own are not without several limitations. Subjectivity in the radiographic measurements performed poses limitations to our methodology, though we sought to minimize this error with multiple reviewers and obtained a high ICC of 0.942. The imaging-based nature inherent to our study design also limits the external validity of our findings: intraoperative ATP and TP measures are likely larger than the windows measured in this study as additional area is gained intraoperatively with tissue retraction.18 As such, the values reported in this study are likely more conservative than what would be found intraoperatively with larger approach windows. It is also important to keep in mind that although preoperative imaging is performed supine, intraoperatively patients are placed in the lateral decubitus or prone position. Deukmedjian et al found shifting patients from the supine to right lateral decubitus position shifted the left kidney 22 mm anteriorly and 15 mm caudally, while the right kidney moved 9 mm rostrally.19 For the left lateral decubitus position, Deukmedjian et al also found the left kidney moved 3 mm anteriorly and 1 mm caudally, while the right kidney moved 20 mm anteriorly and 5 mm caudally. With respect to the psoas muscle, Gandhi et al found positional changes from supine to the left lateral decubitus position can result in 0.21 to 5.8 mm anterior shifts of the psoas.20
Nonetheless, as Julian Li et al clarify, there is still a role for imaging studies based on standard supine imaging as retraction of the psoas muscle intraoperatively is going to occur and variable alteration of psoas positioning is a constant.1 Furthermore, even with anatomical shifts from the supine position, retraction in the decubitus position back to as if the patient were supine is unlikely to inflict injury as the psoas is not retracted beyond its natural state. If anything, measuring from the supine position ensures more conservative estimates are taken and would only ensure stricter parameters of the actual ATP approach. Therefore, we agree with Julian Li et al that imaging in the supine position is a valuable approach-related assessment tool for surgeons.
A final limitation of our study is its lack of specificity toward patients with pathologic anatomy, though these patients are a reality of clinical practice. Our study sought to analyze a cross section of heterogeneous patients, which may limit its applicability for patients with outlier anatomic variations. This emphasizes the importance of personalized patient care—utilizing routine imaging to assess patient-specific anatomic features and to inform surgical decision-making. There is wide consensus that careful review of preoperative imaging is necessary for ATP and TP approaches.6,21–27 Our beliefs are similarly aligned. Certainly, while this study seeks to standardize and identify anatomical considerations for ATP and TP approaches, this is by no means a substitute for careful radiographic assessment of patient anatomy preoperatively. For instance, there are numerous clinical reports of performing an ATP approach on patients with situs inversus totalis or a left-sided inferior vena cava.28–31 Understanding the anatomical landscape of each patient prior to surgery is crucial to mitigate iatrogenic injury.
CONCLUSION
This study is the first to both characterize and compare nonneurological structures at risk during ATP and transpsoas fusion approaches bilaterally from L1 to S1 using abdominal CT imaging. Findings suggest the ATP approach poses less structures at risk relative to the transpsoas approach with respect to the kidneys, ribs, and iliac crests bilaterally. The transpsoas approach offers advantages compared with ATP approach with respect to the liver and spleen. Understanding structures at risk during both the ATP and transpsoas approaches may inform preoperative decision-making and mitigate intraoperative iatrogenic complications.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors have no disclosures relevant to the content of this study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.