


Abstract
Background Lumbar spinal stenosis is a prevalent and increasingly important cause of low back pain, leg pain, and walking impairment. Minimally invasive decompressive techniques such as spinous process (SP) osteotomy have become more common in recent years. The main aim of this study was to investigate the proportion of complete SP union and whether complete radiological healing after the osteotomy is associated with superior clinical outcome after 2 years.
Methods In this retrospective cohort study, 149 patients were included from the Spinal Stenosis Trial, a part of the NORwegian Degenerative spondylolisthesis and spinal STENosis study. Computed tomography imaging was performed 2 years postoperatively. The number of osteotomies and the number of SP unions were recorded. Patients were divided into groups based on the degree of union: nonunion, partial union, and complete union. Rate of success (>30% improvement in Oswestry Disability Index [ODI]) and mean change in ODI were the primary outcome measures. We compared the differences between baseline and follow-up between the Degree of Union groups.
Results The study included 102 of 149 eligible patients. Ten patients (9.8%) were classified as having nonunion, 15 (14.7%) as having partial union, and 77 (75.5%) as having complete union. Of the 155 osteotomies, there were 122 classified as union (77%). The success rate was 74%, with no influence of SP union. The mean change in the ODI was −20.1 (95% CI −37.0, 14.2) with no influence of SP union.
Conclusions We found no influence of SP union, classified by computed tomography, on clinical outcome 2 years after SP osteotomy in patients with lumbar spinal stenosis.
Clinical Relevance Supplying useful information about SPO to assist surgeons in the choice of decompressive technique.
Level of Evidence 2.
Introduction
Degenerative lumbar spinal stenosis (LSS) is a clinical syndrome where degenerative changes in and around the spinal canal compress the neural and vascular contents of the spinal canal. This causes a pattern of pain and weakness in the lower extremities and possibly in the lower back, often accompanied by reduced walking distance. LSS is a prevalent and increasingly significant cause of low back pain and impaired walking among older adults. Among Americans older than 65 years, LSS is the most common indication for spine surgery.1 Two large substudies of the Wakayama Spine Study found that 9.8% of the general population had symptomatic LSS, and only 17.5% of those with severe radiological LSS had symptoms.2,3 The most recent Cochrane review concluded that despite many studies, the evidence in favor of decompressive surgery is sparse; however, the number of surgeries performed suggests that surgery is perceived as an effective treatment option.
Laminectomy was once considered the reference method of surgical treatment, but in recent decades, minimally invasive midline retaining procedures, such as bilateral laminotomy, unilateral laminotomy with crossover, and to a lesser extent spinous process osteotomy (SPO), have become more popular. These minimally invasive techniques have been shown to yield similar clinical results as total laminectomies and are considered less invasive.4
When performing multilevel decompression, it has been debated whether to perform lumbar fusion as well. Studies have suggested no added value of fusion in the clinical outcome of multi- and single-level decompression.5,6
The SPO procedure provides good visualization of the spinal canal and the lateral recesses.7 There are 2 main approaches to SPO for posterior decompression, one with the osteotomy being performed at the base of the spinous process (SP) and the other where the SP is split longitudinally from the dorsal surface. However, concern has been raised about whether nonunion of the osteotomy can cause pain.
Several studies have examined the union rates following SP osteotomies and their correlation to clinical outcomes. In a 2014 study involving 55 patients who underwent SP base osteotomy, a union rate of 44% was observed after 2 years. Patients with SP union in all levels showed significantly better scores on the Oswestry Disability Index (ODI) and EQ5D after 2 years; however, no significant difference was found in pain scores.8 In a 2019 study involving 73 patients who underwent SP splitting osteotomy, a union rate of 52% was observed between the SP and lamina after 6 to 18 months, with no impact on clinical outcome.9 In 2 other studies, one with 53 patients reported a union rate of 55% after 1 year, while the other with 50 patients reported a 100% union rate after 9 months.10,11
The main aim of the present study was to investigate the proportion of complete SP union and examine whether radiological healing of the SP after the osteotomy (osteotomy at the base of SP) is associated with superior clinical outcome after 2 years.
Materials and Methods
Study Population and Data Collection
The data for this retrospective cohort study was collected from the Spinal Stenosis Trial (SST), a randomized controlled trial part of the NORwegian Degenerative spondylolisthesis and spinal STENosis study (NORDSTEN-study).
The SST included 437 Norwegian patients aged 18 to 80 yearswho underwent surgery between April 2014 and October 2018, with claudication or radiating pain and radiological findings indicating LSS without spondylolisthesis.12 The patients were randomized into 3 surgical intervention groups, and the 149 patients allocated to the SPO arm were eligible for inclusion in this study. See Table 1 for inclusion and exclusion criteria.
Eligibility criteria for the Spinal Stenosis Trial of the NORDSTEN-study.
This study was approved by the Norwegian Committees for Medical and Health Research Ethics (2011/2034).
Surgical Intervention
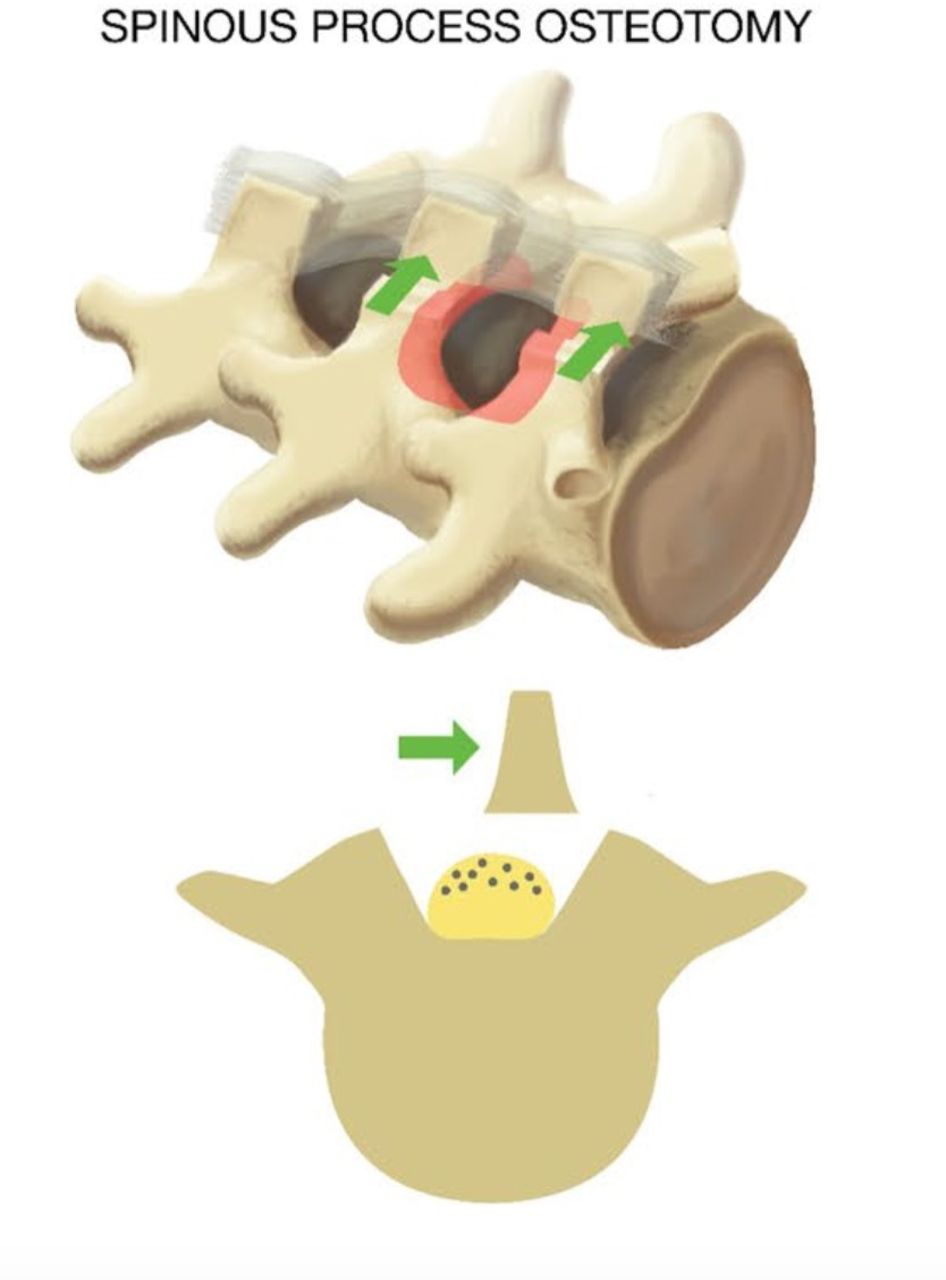
Access to the spinal canal was obtained by an osteotomy at the base of the SP above (and sometimes under) the affected level. The SP was then retracted to 1 side with intact supraspinous and intraspinous ligaments, giving midline access to the spinal canal (Figure 1). A laminotomy of the lower part of the superior lamina and the upper part of the inferior lamina was then performed, followed by a medial facetectomy. Both nerve roots were visualized, and the lateral recesses were decompressed. After the decompression was performed, the retractors were released, and the osteotomized SP fell back to its original position. Additional details have been published in the SST protocol.12

Illustration of a spinous process osteotomy. The red zone illustrates the focus of decompression.
Radiological Evaluation
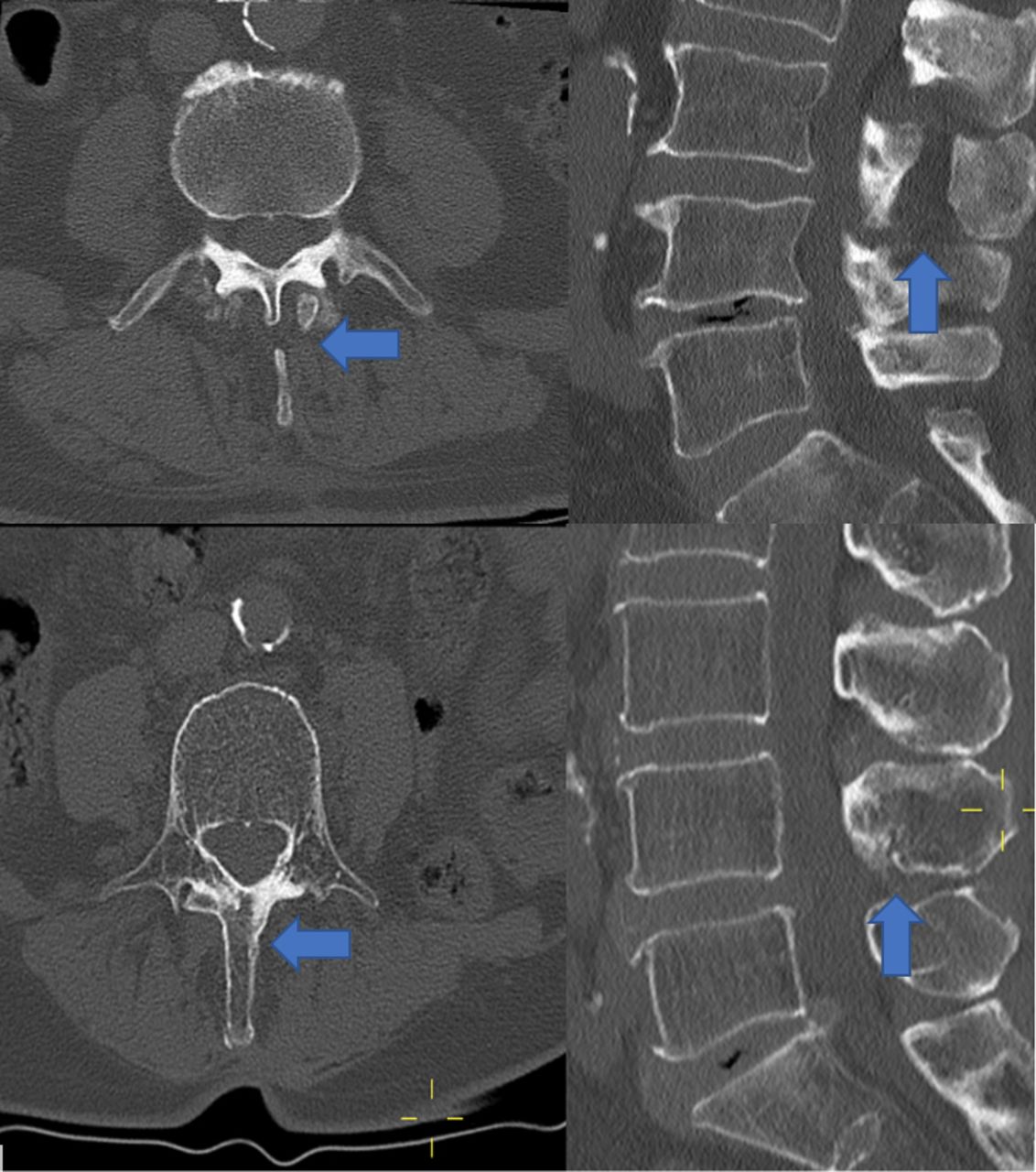
Computed tomography (CT) was performed 2 years postoperatively. The lumbar spine was visualized with 3-mm thick sagittal, coronal, and axial reformatted CT images. The CT examinations were evaluated by a board-certified radiologist (H.B.) and a junior physician (S.H.). The former instructed the latter in the methodology prior to the examination. To improve inter-rater agreement, both examinators performed 20 evaluations together as a pilot. Data from the pilot study were not used in the final analysis. Afterward, all patients were examined by the 2 examinators independently. Each SP was examined individually and classified as union if there was observable bridging callus formation between the distal and proximal fragment of the SP. If no bridging callus was present, the SP was defined as nonunion. Examples are shown in Figure 2.

Transverse and sagittal computed tomography images of the lumbar spine. A nonunion is shown in the top 2 images and a union in the bottom 2 images.
The patients were categorized into 3 groups, based on degree of union (DOU). If none of the patient’s osteotomized SPs were classified as union, the patient was placed in the nonunion group. If some but not all SPs were classified as union, the patient was placed in the partial union group, and if all SPs were classified as union, the patient was placed in the complete union group. Inconsistencies between the 2 examinors were reviewed independently by an orthopedic surgeon (E.H.) to obtain consensus.
Primary Outcome Measures
Mean change in ODI score from baseline to 2-year follow-up was chosen as the primary outcome. The ODI is the most used outcome measure in spinal surgery; we used the Norwegian version 2.0.12–14 The ODI is expressed as an index ranging from no disability (0) to the worst imaginable disability (100).
The proportion of patients classified as achieving successful outcomes was chosen as the second primary outcome. Success was defined as >30% improvement in ODI score from baseline to follow-up. This criterion has been used in the other publications from the NORDSTEN-study and is considered a relevant outcome measure.15
Secondary Outcome Measures
Mean change in patient-reported outcome measures (PROMs) comprised the secondary outcome measures. Mean change in symptom severity and functional outcome was measured by change scores on the Zürich claudication questionnaire, a standardized spinal stenosis-specific self-administered questionnaire consisting of a symptom severity part (ranging from 1–5), a daily function part (ranging from 1–4), and a surgery satisfaction part.16 Mean change in low back and leg pain was quantified using a numeric rating scale (NRS, ranging from 1−10). Mean change in health-related quality of life was measured by EQ-5D, a prominent health-related quality of life tool that evaluates health status across 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and a visual analog scale for self-rated health assessment (indexed scores ranging from −0.59 to 1).17 Radiological outcomes included the number of osteotomies defined as union and the number of patients in each DOU group.
Statistical Analysis
All analyses were performed using IBM SPSS statistics version 28.0.0.0 (190). The baseline data and the change from baseline to follow-up in PROMs were examined for DOU-group differences. For the continuous variables (age, body mass index, and PROMs), analysis of variance with Tukey’s honestly significant difference for post hoc testing to control for making type-I error was used. For the categorical variables (sex, smoking, and success), the χ2 test was used. In the cases with an expected count of less than 5, the Fisher’s exact test was used. Due to the skewed DOU-group sizes, another analysis was performed on the change from baseline PROM data, with the nonunion and partial union treated as 1 group and compared with the complete union group using an independent 2-sample t test. A weighted Cohen’s kappa analysis was performed to assess interrater agreement between the 2 examinors.
Results
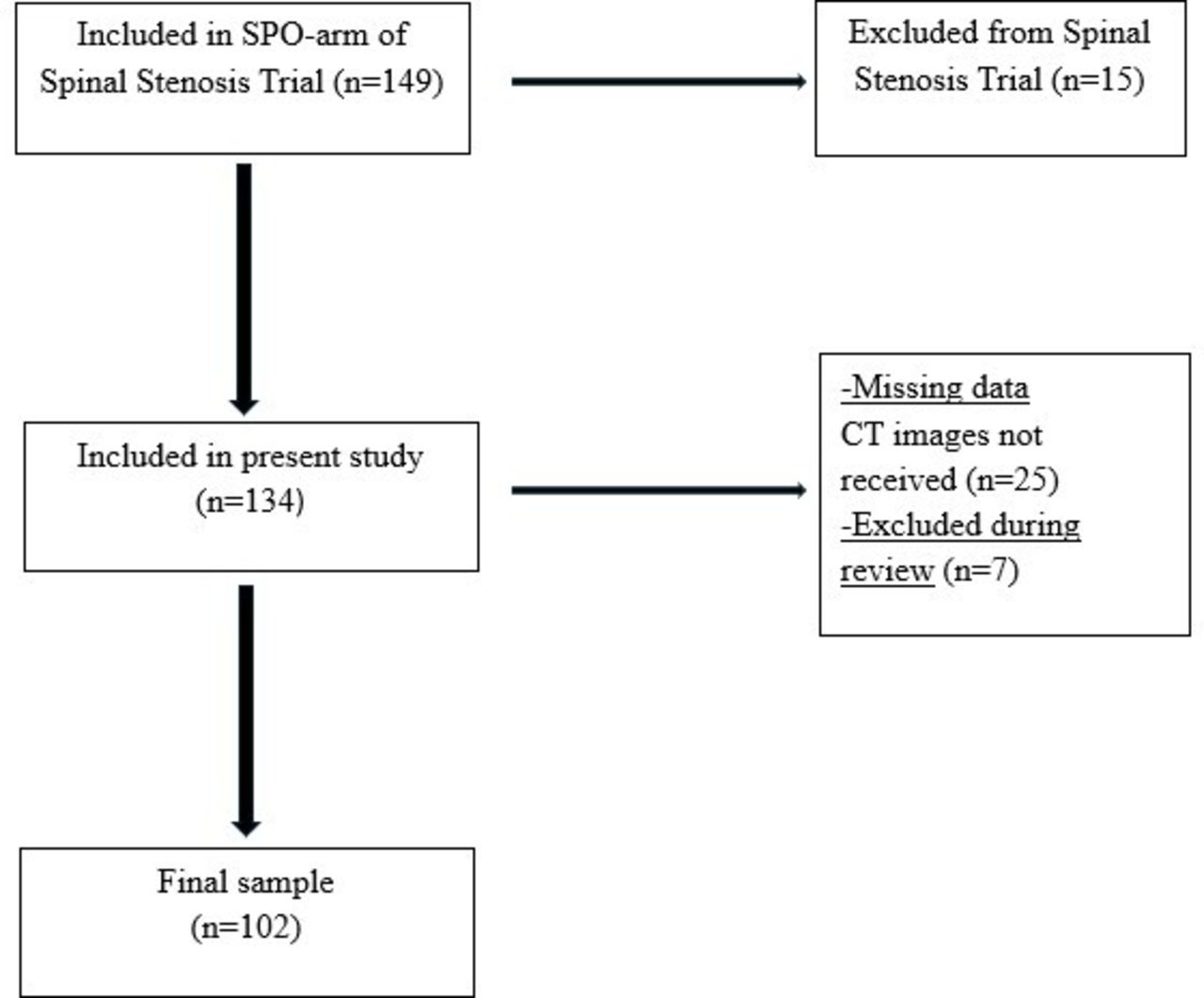
Of 149 patients eligible for inclusion, 102 were included in this study (Figure 3). Ten (9.8%) patients were classified as nonunion, 15 (14.7%) as a partial union, and 77 (75.5%) as a complete union. The number of patients in each DOU group who answered all follow-up PROMs varied (detailed with secondary outcomes later in this section). The total number of osteotomies, counting every cut SP on every patient, was 155, of which 122 (77.7%) were classified as union at 2-year follow-up. Two examinors agreed on all but 2 cases, resulting in an observed agreement rate of 98% and a weighted Cohen’s kappa of 0.95 (95% CI 0.87–1.03).

Flowchart of the patients in the current study.
Baseline Data
The baseline characteristics of the patients are shown in Table 2. There were no significant differences in the measured demographic data between the 3 DOU groups. The only baseline PROM with significant DOU-group differences was low back pain measured with NRS, with the nonunion group mean being 2.4 points higher than that of the partial union group (P = 0.04).
Demographics and baseline pain and function scores in the 3 degree of union groups.
Primary and Secondary Outcomes
The mean change in ODI was −20.1 (95% CI −37.0, –14.2) from baseline to follow-up in the total cohort. The mean change from baseline to follow-up was −25.6 (95% CI −14.2, –37.0) in the nonunion group and −19.9 (95% CI −16.7, –23.7) in the complete union group. The differences between the DOU groups were not statistically significant (P = 0.49; Table 3).
Primary outcome of change from baseline to follow-up in the 3 degree of union groups
There were no statistically significant differences in the mean change from baseline to follow-up between the union groups for any secondary outcome measures (Table 4). The number of patients in each DOU group who answered all follow-up PROMs varied, as noted throughout Table 4.
Secondary outcome measures change from baseline to follow-up, mean (SD).
When t tests were performed with nonunion and partial union patients combined into 1 group (mean ODI change −20.8) vs the complete union group (mean ODI change −19.9), no significant differences were found (P = 0.83; Table 5).
Primary and secondary outcome measures: change from baseline to follow-up, comparing the complete union group and not complete union group made from merging the nonunion group and partial union group.
Discussion
The main finding of this study is that there was no influence of SP union on 2-year patient-reported outcomes. There was a high proportion of patients classified as complete union (75.5%), a high success rate (74%), and a high number of osteotomies classified as union (77.7%).
The mean improvement in ODI is in line with results after other decompressive techniques and above current estimates of minimal clinically important difference.7,8,18–20 The clinical results after different minimal invasive decompression techniques are similar, as shown in a recent randomized controlled trial.21
The previously mentioned studies examining union between the SP and lamina found union rates between 44% and 100% after 6 to 24 months in groups of 50 to 73 patients. Hermansen et al8 found patients with union in all levels to have better clinical outcomes after 2 years, while Wi et al found no relationship between union and clinical outcome after 6 to 18 months. We found a high rate of union (77%) among our 102 patients, with no effect of union on clinical outcome. Two of the benefits of our study compared with the aforementioned studies are the larger sample size and the use of 2 independent examinators using CT imaging to evaluate union.
A limitation of this study is the unequal number of patients in the DOU groups, with only 10 patients classified as nonunion according to our classification. Another limitation is that the lack of an existing standardized method for evaluation of SP union makes our qualitative assessments harder to precisely reproduce. Our follow-up interval of 2 years may also be too short to determine the long-term effects of SP union. In a 2015 study investigating the effects of SP union following SP splitting osteotomy during open-door laminoplasty, the authors reported no significant impact of union on clinical outcome after 2 to 4 years. However, they observed that nonunion was associated with worse clinical outcomes after 10 to 12 years.22 Further studies with extended follow-up intervals of 5 and 10 years are required to observe the long-term effects of SP union on clinical outcomes after the SP base osteotomy procedure. Additional studies should also include magnetic resonance imaging scans to visualize potential noncalcified fibrotic tissue formation between the proximal and distal SP fragments. Another limitation is that we, in our analysis of the CT images, did not assess other readily available parameters relevant for LSS in general, such as changes in slip progression and facet joint degeneration in the index level and adjacent levels.
Further research is needed on the long term clinical importance of SP union and if one should try to facilitate SP union, for example, through osteosutures. Our findings suggest that nonunion does not worsen clinical outcomes and that trying to facilitate union thus seems unnecessary. SPO is a viable primary decompressive approach for LSS or as a rescue technique when performing unilateral laminotomy with crossover. The surgeon can thereby choose a technique according to his or her preference and experience. SPO is, by some surgeons, considered to be less technically demanding and offers good visualization, especially when decompressing the lateral recess.
Conclusion
Most of the SPOs (77%) were classified as union. The success rate was high in the total sample (74%). We found no influence of SP union, classified by CT, on clinical outcome 2 years after SPO in patients with LSS.
Footnotes
Funding This trial received funding from Central Norway Regional Health Authority (RHA) and Western Norway Regional Health Authority (RHA).
Disclosures The authors report no disclosures or conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.