


Abstract
Background Postoperative spinal epidural hematomas (pSEHs) are a rare complication of microdiscectomy surgery. The hematoma may be unnoticed intraoperatively, but timely treatment may prevent permanent neurologic impairment. Airway management in patients with a full stomach is generally performed with rapid sequence intubation and general anesthesia. Awake spine surgery without intravenous analgesia or sedation may be beneficial in patients with a full stomach who are at higher risk for pulmonary aspiration with general anesthesia due to a loss of non-per-oral (NPO) status. The authors propose that it can also be performed in cases of urgent/emergent postsurgical epidural hematoma evacuation.
Methods We present the airway management of a 41-year-old man who underwent a minimally invasive microdiscectomy with normal strength immediately after surgery but developed progressive weakness with right foot dorsiflexion, right extensor hallucis longus muscle weakness, and progressive right lower extremity ascending numbness over the course of the first 2 hours after surgery due to an epidural hematoma.
Results The patient underwent urgent awake epidural hematoma evacuation with a spinal anesthetic. Afterward, the patient recovered neurological function and was discharged the following morning.
Clinical Relevance pSEHs are a rare complication of microdiscectomy surgery. The purpose of this article is to describe the novel use of awake spine surgery in emergent epidural hematoma evacuation and demonstrate its feasibility.
Conclusions In emergencies, when a patient is not NPO, awake spine surgery can safely be performed with no sedation, ensuring the patient can protect their airway and avoid the risk of aspiration.
Level of Evidence 3.
Introduction
Postoperative spinal epidural hematomas (pSEHs) are a rare complication of microdiscectomy surgery.1 The severity of neurologic deficit and time spent experiencing hematoma-related paraplegia have been found to be correlated with prognosis in surgical patients.2 The hematoma may present early, and timely evacuation may prevent severe neurologic impairment.3–6 However, in a patient with a full stomach, general anesthesia (GA) could increase the risk of perioperative pulmonary aspiration.5 Awake spine surgery is a novel technique that involves the use of local or regional anesthetics. This technique has been conducted safely in various spine surgeries.7 Although spinal anesthesia has been used on a full stomach during obstetric surgery (expecting mothers are usually not non-per-oral [NPO] prior to delivery), no identifiable research articles assess emergency hematoma evacuation by awake spine surgery.8 However, in cases where a patient is not a good candidate for GA due to loss of NPO status, awake spine surgery can be beneficial.7
Case Presentation
History
A pleasant 41-year-old man presented to the clinic for evaluation of approximately 6 weeks of right lower extremity radicular pain and paresthesia symptoms in the posterolateral leg consistent with a right L5 and S1 radiculopathy. The patient also noted right lower extremity weakness with toe walking. The patient did try conservative treatment for this problem including a right L5-S1 transforaminal epidural steroid injection, lifestyle modifications, and medication management using nonsteroidal anti-inflammatory drugs and gabapentin without durable relief.
Physical Examination
Physical examination findings were significant for a dropped right Achilles reflex, inability to perform a single-leg calf raise on the right lower extremity, abnormal gait due to right lower extremity weakness, 4 out of 5 right gastrocnemius strength, and a positive right-sided straight leg raise test.
Imaging
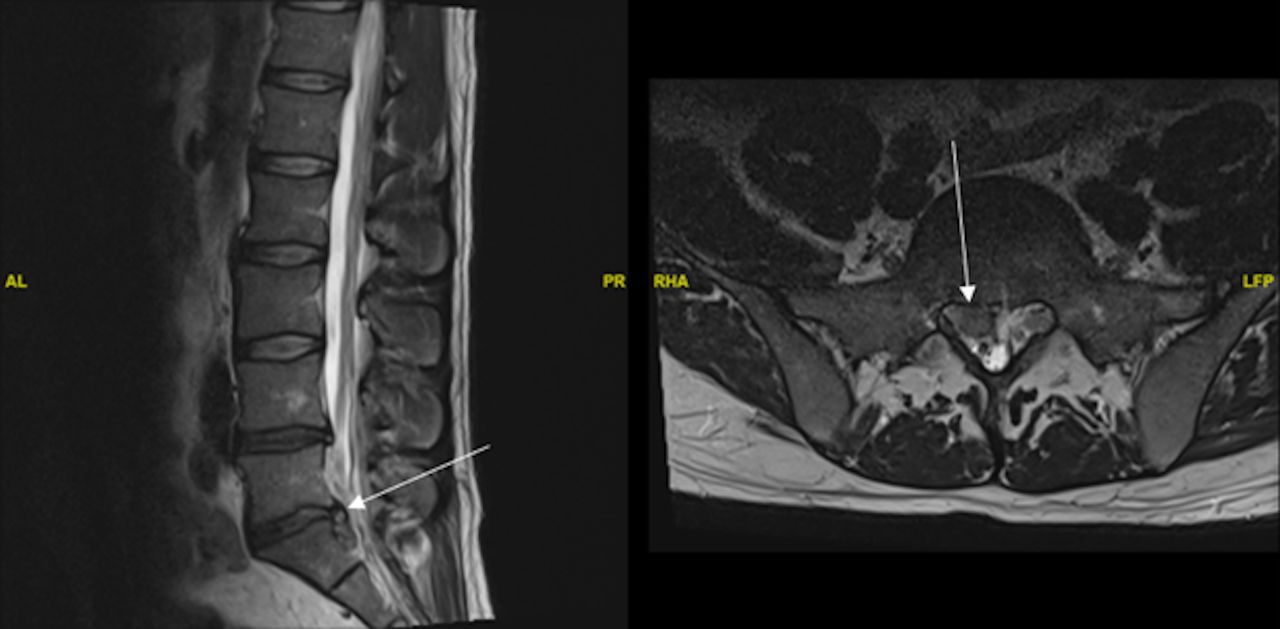
The patient underwent magentic resonance imaging of the lumbar spine without contrast, the results of which showed a large right L5-S1 paracentral disc extrusion with associated right L5-S1 lateral recess stenosis and contact of the traversing right S1 nerve root (Figure ).

Preoperative sagittal T2-weighted (left) and axial T2-weighted (right) magnetic resonance image revealed a right, paracentral disc extrusion at the L5-S1 level (indicated by the white arrow). The disc is contacting the traversing S1 nerve with associated lateral recess stenosis.
Surgical Procedure
The patient underwent an uneventful awake right L5-S1 microdiscectomy with epidural block and sedation. Afterward, the patient was transferred to the postanesthesia care unit in stable neurologic condition. In the immediate postoperative period, the patient was neurologically intact to the bilateral lower extremities with intact bilateral foot plantar and dorsiflexion and extensor hallucis longus (EHL). The epidural block was confirmed to have completely worn off. Over the course of the first 2 hours of the patient’s postanesthesia care unit stay, he developed progressive weakness with right foot dorsiflexion and EHL, as well as progressive right lower extremity ascending numbness. Our institution’s Enhanced Recovery After Surgery protocol dictates that the patient’s diet is advanced as soon as they can eat, so he had a full stomach at the time of his neurological decline.
Postsurgical Hematoma Evacuation Procedure
The patient was taken back to the operating room on an urgent basis, 71 minutes after symptom onset, for re-exploration and evacuation of a right L5-S1 epidural hematoma that lasted for 1 hour and 11 minutes. During this procedure, a spinal block was performed intraoperatively for pain control. Awake spine surgery was performed without the use of intravenous sedation or systemic analgesia because the patient had a full stomach. Wound exploration began with local anesthesia. Next, 0.5 mL of 1.5% mepivacaine was injected intrathecally with a 27-gauge needle when the dura was visualized, and the hematoma was evacuated. Mepivacaine is a short-acting local anesthetic with a half-life of between 90 and 240 minutes, depending on dosing. The medication and dosage were chosen to ensure an early postoperative neurologic examination. Spinal anesthetic, as opposed to local alone, is necessary for awake surgery without systemic anesthesia due to the pain associated with mobilizing neural elements. We also wanted to be prepared to enlarge surgical exposure by increasing the size of the laminotomy. The patient tolerated the procedure well and was fully conscious. As a result, the patient was able to protect his airway in the prone position.
Immediate Postoperative Course
Postoperatively, additional neurologic checks were performed after the spinal anesthetic had worn off. The patient was found to be neurologically intact with intact right foot plantar and dorsiflexion, EHL strength, and improved right lower extremity sensation to light touch.
Postoperative Follow-Up
The patient was discharged from the surgery center upon meeting unit criteria. He followed up in clinic approximately 4 weeks postoperatively for further evaluation and was found to have interval relief of his initial radicular symptoms as well as intermittent positional headaches. The patient was referred to the anesthesia acute pain service and underwent a blood patch. He had complete resolution of his positional headache following the blood patch.
Discussion
pSEHs that are associated with neurological deficit should undergo timely evacuation.2–4 The literature has identified various risk factors for hematoma, but there is some consensus on its link to advanced age, perioperative coagulopathy, and multilevel spinal decompression. Some symptomatic cases are unnoticed intraoperatively; however, some may present as late as postoperative day 2 after surgery.4,6 Spinal anesthesia has been utilized on pregnant patients during delivery even on a full stomach.8 In the current article, we present a novel implementation of awake spine surgery in an emergent case of postoperative pSEH.
Awake spine surgery has already been shown to be safe and beneficial in eliminating risks associated with GA.9,10 Compared to GA, awake surgery tends to allow patients a faster time to ambulation, decreased postoperative opioid use, and decreased cost of treatment.11 Awake spine surgery is also being increasingly implemented in models of surgical care.11 Regardless of the induction techniques for GA, sedatives blunt the patient’s airway protective reflexes and increase the risk of aspiration. Awake patients that are fully conscious can protect their airway because they can maintain protective airway reflexes.
Surgical timing of hematoma evacuation and the degree of neurological improvement after epidural hematoma evacuation are the most important prognostic factors.12 Current literature also shows a correlation between time to evacuation and neurologic recovery post-evacuation.13 Although there is no set rule for when to undergo surgical evacuation, it is imperative that an epidural hematoma diagnosis is made as soon as possible (ideally within 6 to 12 hours).6 This case demonstrates the feasibility of awake spine surgery in emergent situations when the patient has already eaten postoperatively.
The recommendations for preoperative fasting are that patients abstain from solid foods for at least 8 hours and clear fluids for at least 2 hours before procedures requiring GA. Nonadherence to these guidelines has been associated with an increased risk of pulmonary aspiration.14 In this case, the patient ate solid food postoperatively according to our Enhanced Recovery After Surgery protocol but before hematoma evacuation, making him a poor candidate for GA.
Based on the use of this technique, the authors believe that awake spine surgery is feasible for epidural spinal hematoma evacuation without the need for an intravenous analgesic or sedatives that may blunt protected airway reflexes. GA is associated with a risk of pulmonary aspiration, especially in the setting of a full stomach. These risks may be as high as 1 in every 2000 to 3000 surgeries, making aspiration one of the most frequent causes of anesthesia airway-related mortality.5,14 Additionally, spinal anesthesia with mepivacaine is known to be reliable for up to 2 hours.15 Therefore, a postoperative neurologic examination cannot be performed while the spinal anesthetic is still active. Hence, the choice of intrathecal anesthetic is imperative in allowing for early identification of a postoperative neurologic deficit. This, combined with the patient’s development of a postdural puncture headache, may raise concerns of perioperative complications, delayed identification of those complications, and subsequent treatment. Although delayed identification of postoperative complications may be possible due to the duration of spinal anesthesia, research shows that there is no significant difference in complication development in routine surgeries when compared to GA.16 For postdural puncture headache specifically, there is a low risk (2%), which is mitigated by the use of less traumatic needles.17
Conclusion
In the case described here, the patient underwent a routine microdiscectomy and ate a meal shortly after surgery. However, the patient began presenting with symptoms of epidural hematoma within a few hours and needed to return to the operating room. The loss of good NPO status increased the patient’s risk of pulmonary aspiration with intubation and GA. Consequently, the surgeons elected for awake spine surgery. We propose that awake spine surgery can allow surgeons to act swiftly in urgent or emergent cases of suspected hematoma, initiating evacuation as soon as possible. In such emergent cases, surgeons can perform timely intervention without needing to wait for gastric emptying and preoperative fasting guidelines for GA. However, this case only demonstrates the feasibility of awake spine surgery in the setting of simple epidural hematoma. We are not advocating for its implementation as a new standard of care but rather highlighting novel use of spinal anesthesia for awake spine surgery. More research needs to be done to access widespread safety and reproducibility.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosures Ernest Braxton reports consulting fees from Accelus, Aesculap, Boston Scientific, Spinal Elements, GE Healthcare, and Medtronic. Muhammad Abd-El-Barr reports grants/contracts from NREF; consulting fees from TrackX, Spinal Elements, and Globus, and stock/stock options with TrackX. The remaining authors have nothing to disclose.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.