


Article Figures & Data
Figures
- Fig. 1
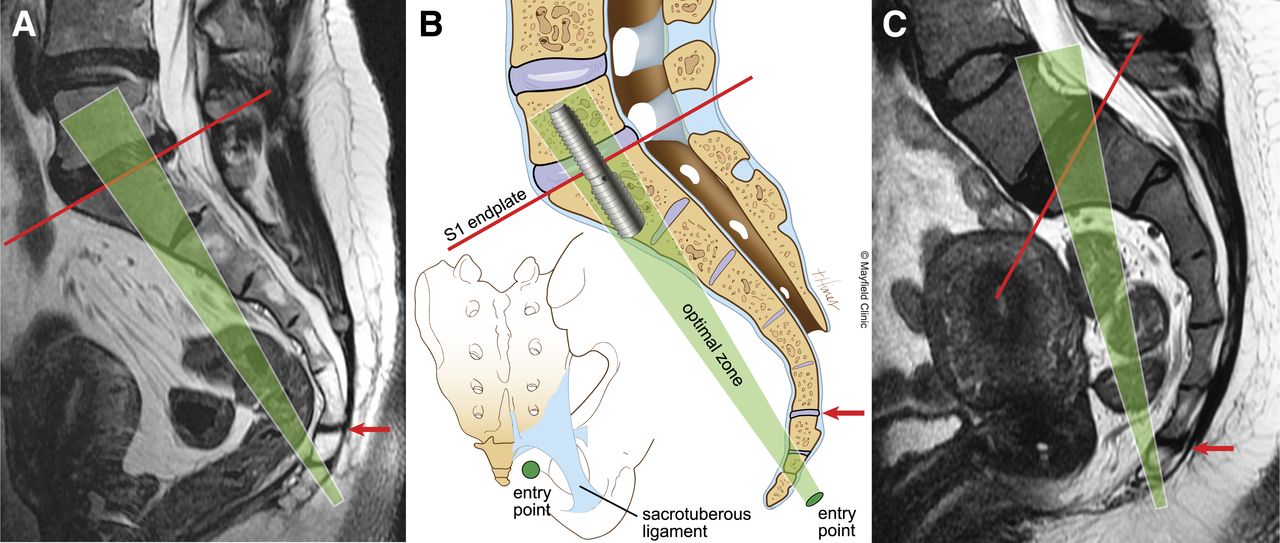
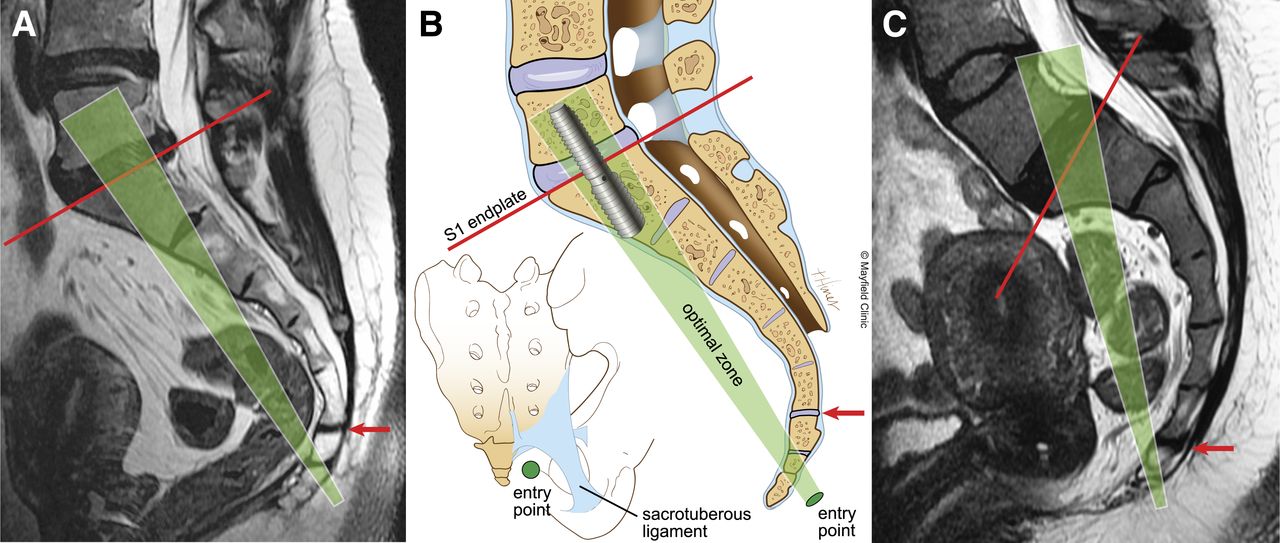
Preoperative evaluation of the sacrum and coccyx for the presacral ALIF procedure. To assess the feasibility of the approach, a line is drawn on the midsagittal MR scan from the probe entry point below the sacrococcygeal joint (red arrow) to the midpoint of the S1 endplate (red line). The optimal trajectory zone (green shaded area) for placement of the implant should be perpendicular to and centered at the midpoint of the superior endplate of S1. MR scan (A) and illustration (B) shows an ideal trajectory for insertion of the screw into the L5-S1 vertebrae. Illustration of the posterior view of the sacrum shows the probe entry point lateral to the coccyx and inferior to the attachments of the sacrospinous and sacrotuberous ligaments. MR scan (C) shows an excessive curvature of the sacrum and coccyx that would result in screw placement at an acute angle to the superior endplate of S1, which is biomechanically suboptimal, and in violation of the spinal canal. This procedure is contraindicated in these patients (with permission from Mayfield Clinic).
- Fig. 2
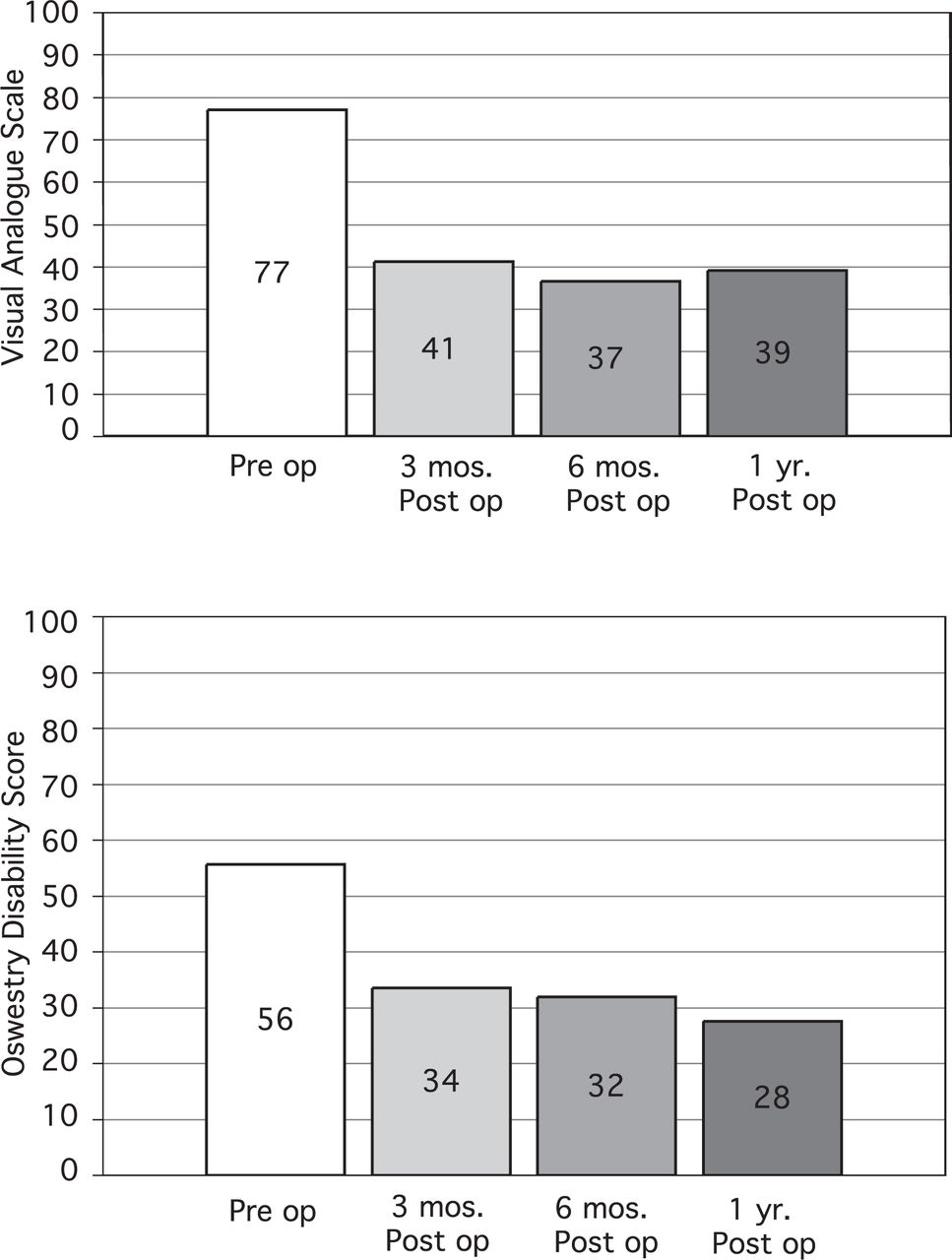
Bar graphs of the pre- and postoperative Visual Analog Scale (A) and Oswestry Disability Index (B) scores. At 1-year follow up, VAS improved 49% and ODI improved 50% (statistically significant P < .0001) (with permission from Mayfield Clinic).
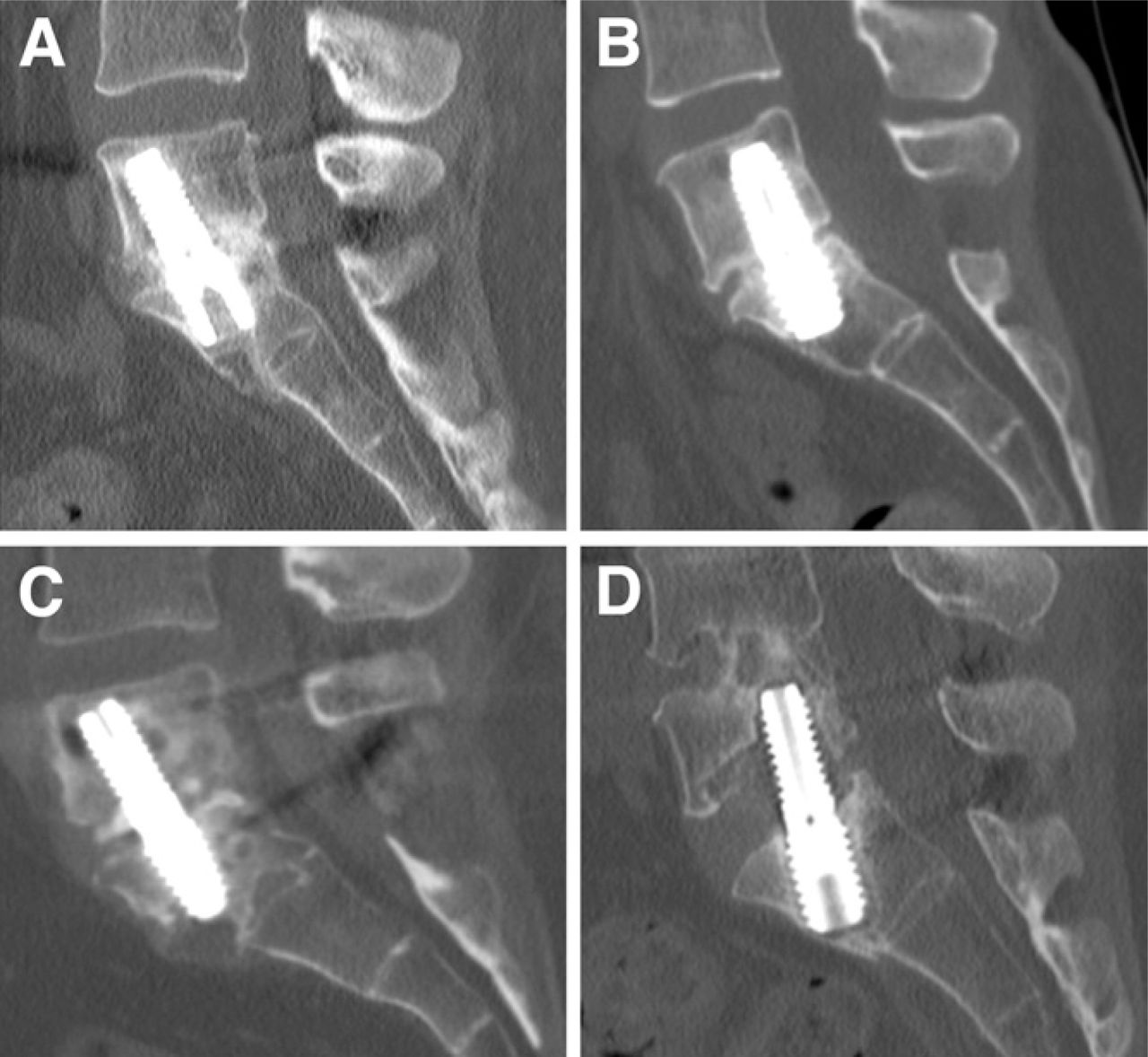
- Fig. 3
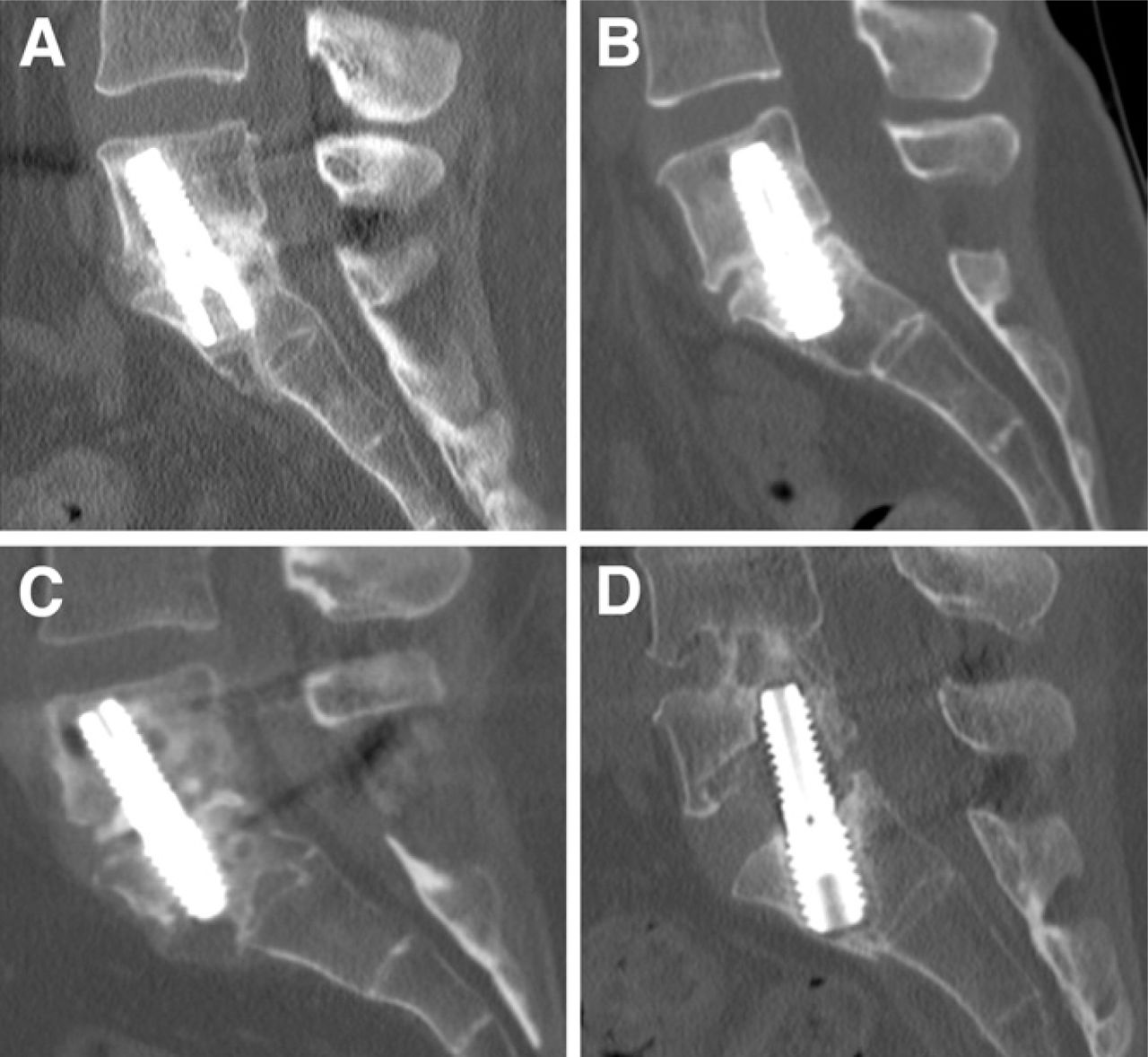
Postoperative fusion grades for the procedure depicted on 1-year postoperative CT scans. (A) Grade I shows continuous bridging bone extending from the L5 to the S1 endplate and occupying >50% of available space for fusion. (B) Grade II has bridging bone extending from the L5 to the S1 endplate and occupying < 50% of available space for fusion. (C) Grade III has developing bone with presence of bone connected to either L5 or S1 endplate without bridging. (D) Grade V is a pseudoarthrosis (with permission from Mayfield Clinic).

Tables
- Table 1
Fusion criteria on 3-mm high-resolution CT scan reconstructions in coronal and sagittal planes (with permission from Mayfield Clinic)
Grade Time period Definition I Applicable at any follow-up Bridging bone, advanced fusion. Presence of continuous bridging bone extending from the L5 to the S1 endplate on the reconstructed images, occupying >50% of available space for fusion. II Applicable at any follow-up Bridging bone, fusion. Bridging bone filling <50% of available space between vertebral bodies. III Early: 6 months Early: Presence of developing bone connected to either end plate without bridging. Late: 12,18, 24 months Late: Presence of developing bone connected to either endplate without bridging with fusion mass greater than previous scan. IV 6 months No bridging or developing bone connected to either endplate. V Applicable at 12, 18, 24 months No bridging or developing bone. Decrease or nonprogression of developing bone since previous visit. - Table 2
Mean intraoperative blood loss and operative times as noted from anesthetist's chart were significantly lower in stand-alone procedures when compared with procedures supplemented by either pedicle screw fixation or TLIF procedure at another level. Although few patients underwent the procedure alone, morbidity associated with this procedure was substantially lower
Total Stand-alone With posterior procedure Paired t test Criteria (N = 50) (n = 5) (n = 45) P value Estimated blood loss (ml) 218 29 234 .02 Operative time (minutes) 194 55 207 .0001
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.