


Article Figures & Data
Figures
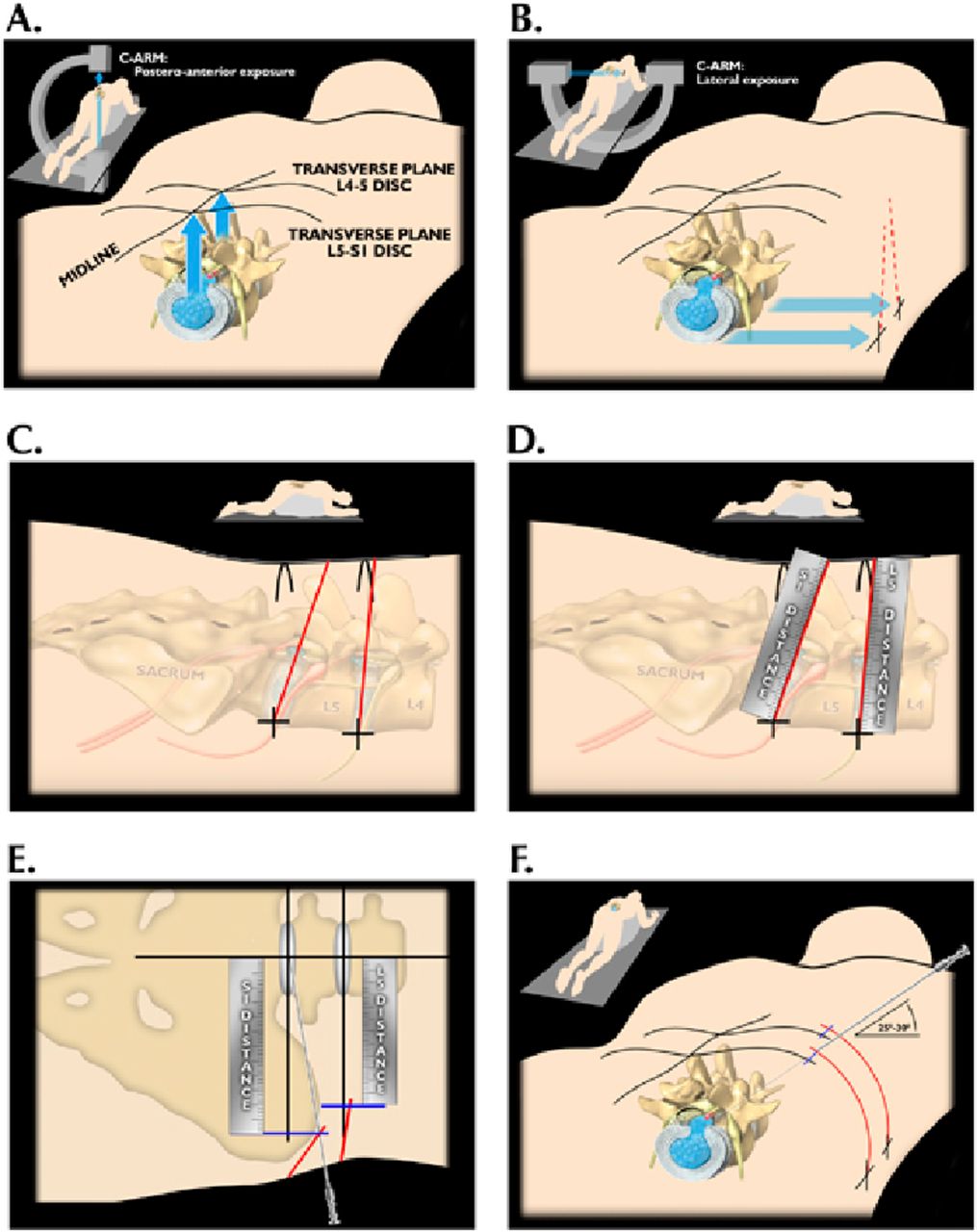
- Fig. 2
Changed trajectory to 20-30 degrees.
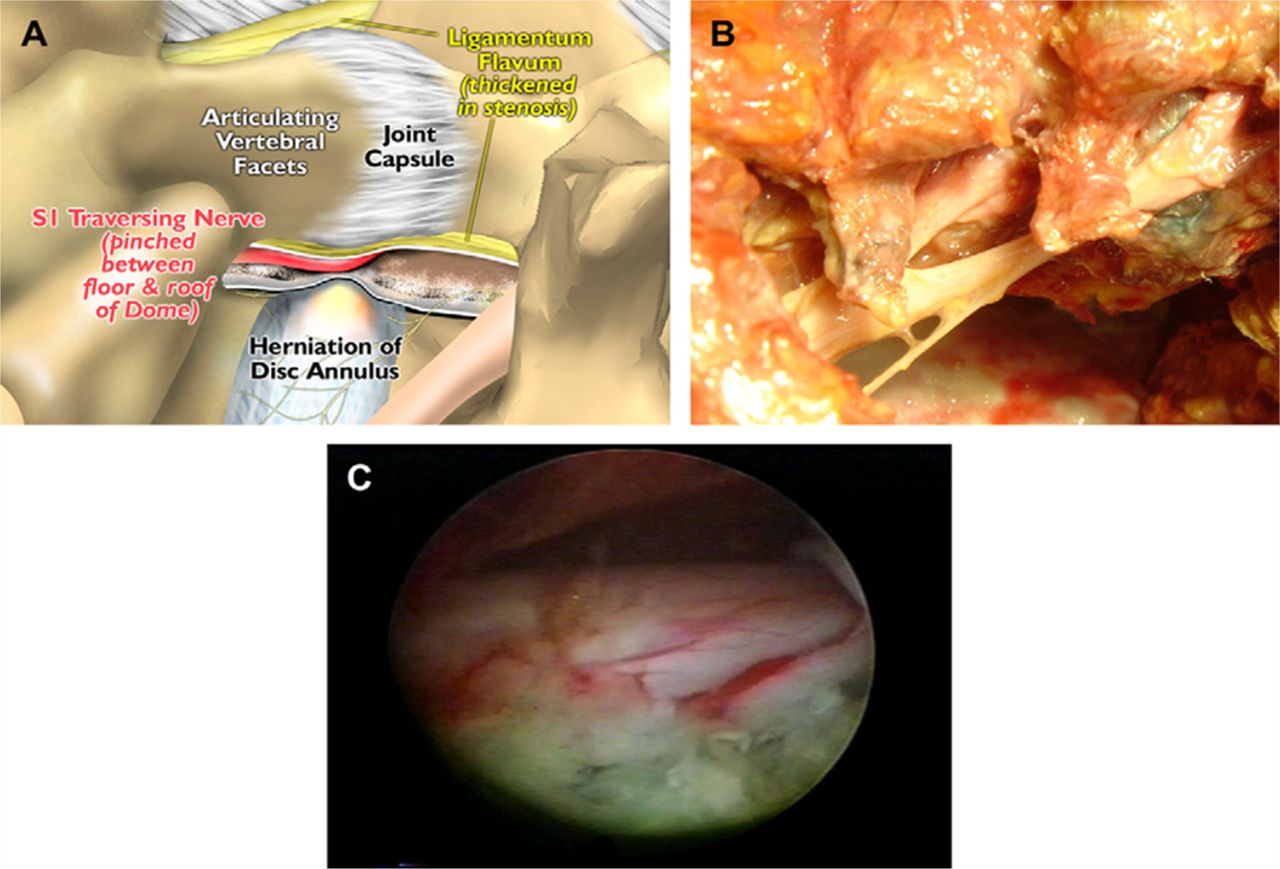
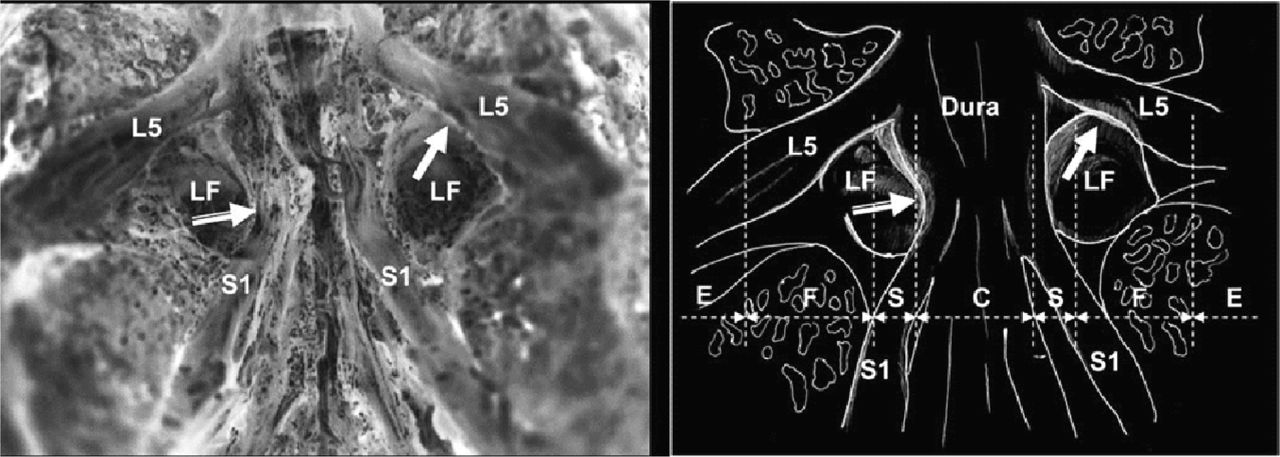
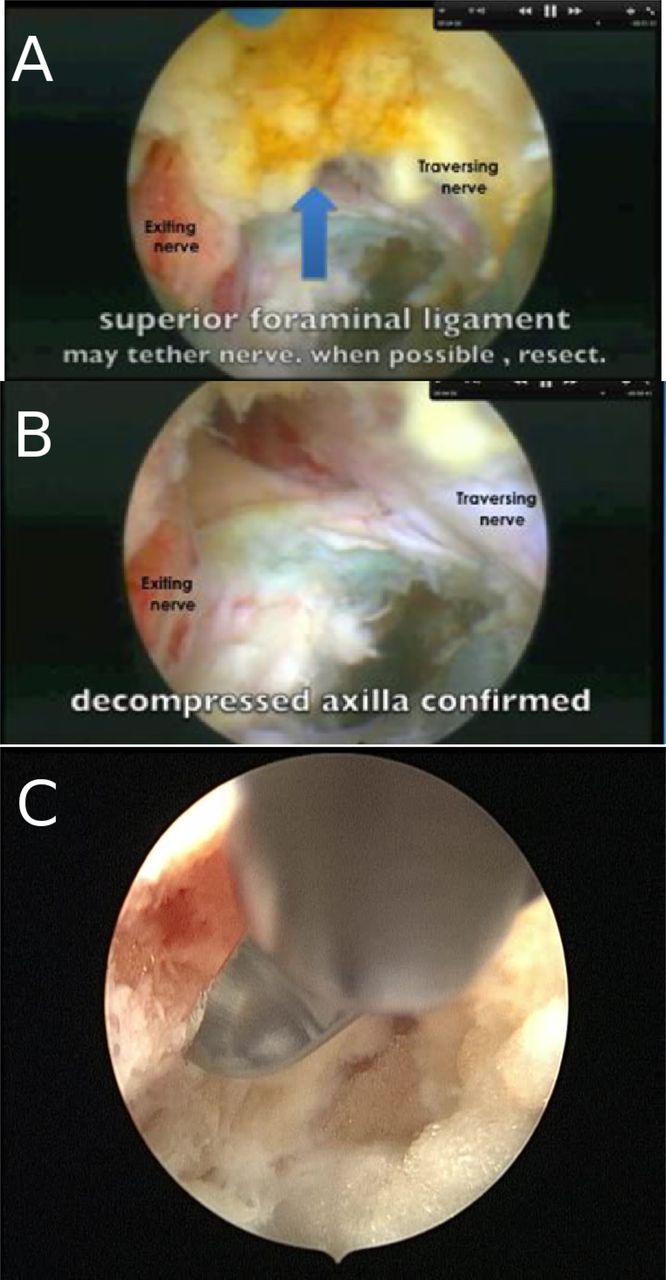
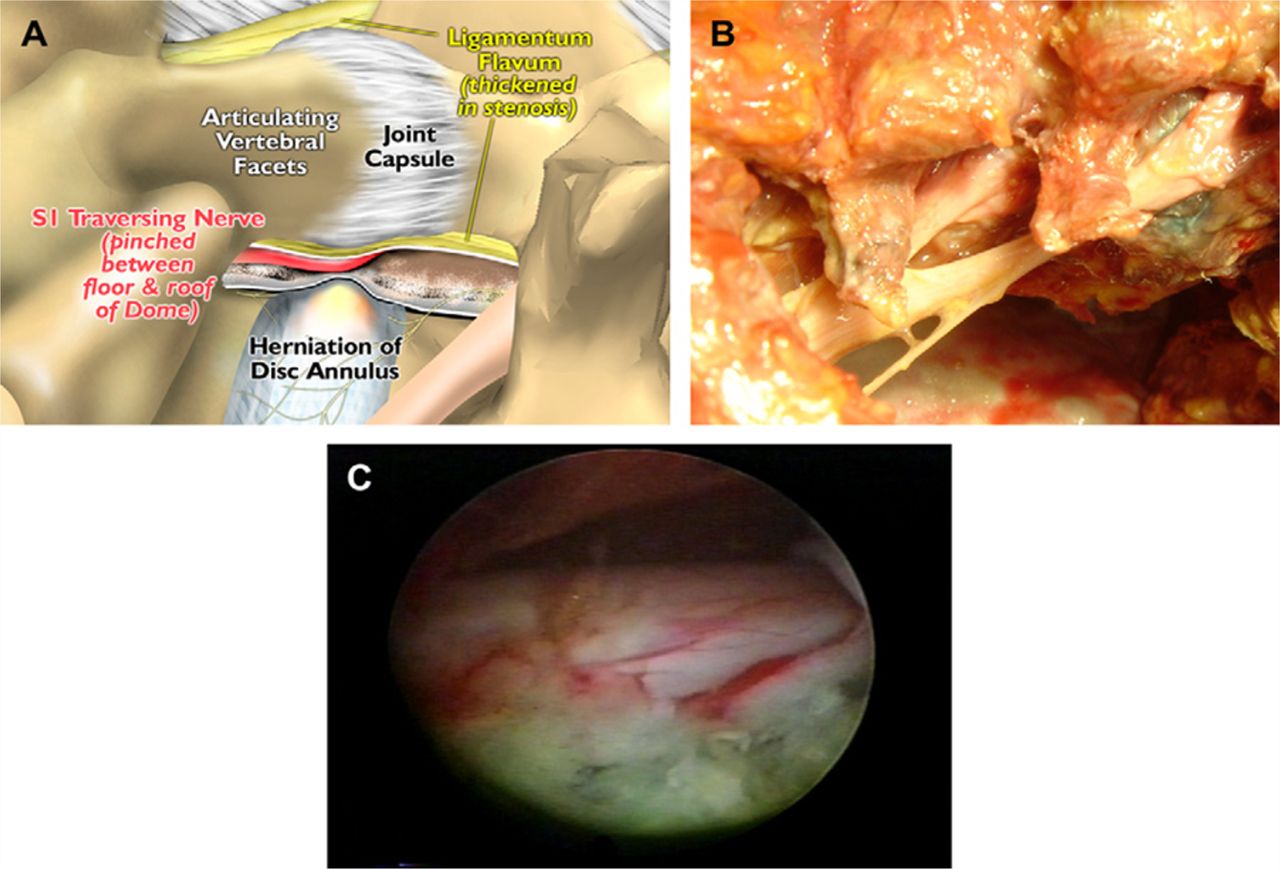
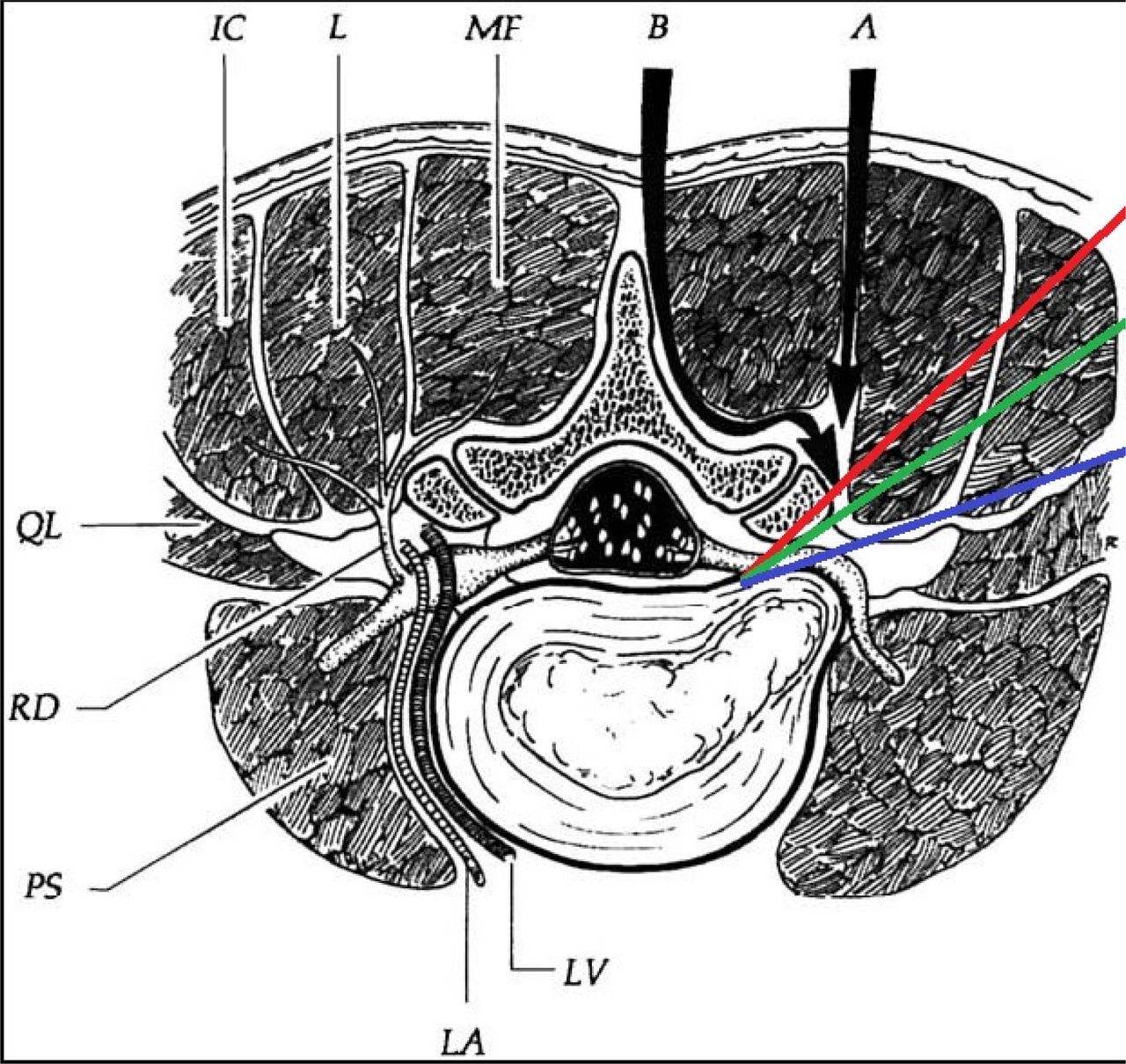
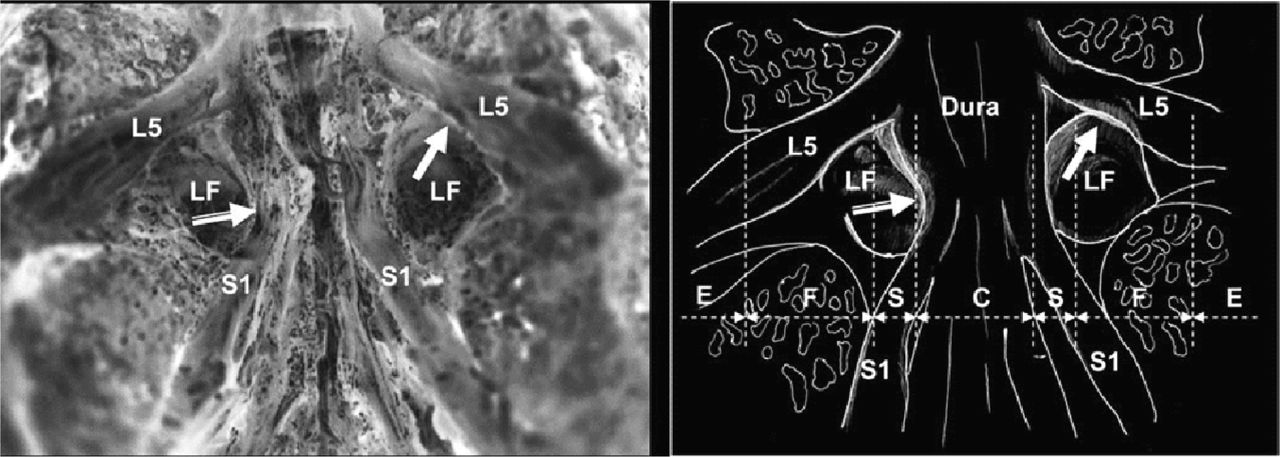
- Fig. 3
Shows structures in foramen which we come across when targeting the disc. Note facet forms roof of the lower foramen
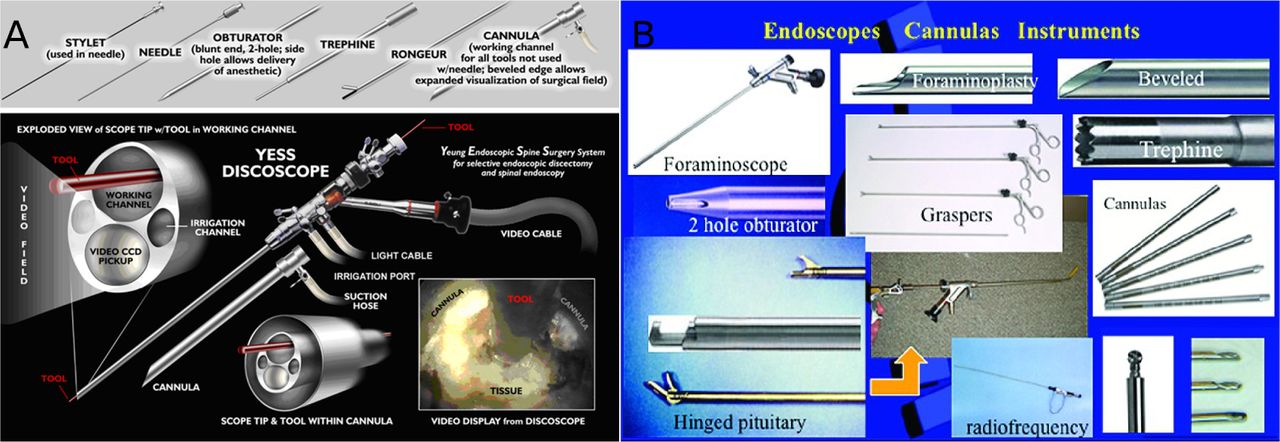
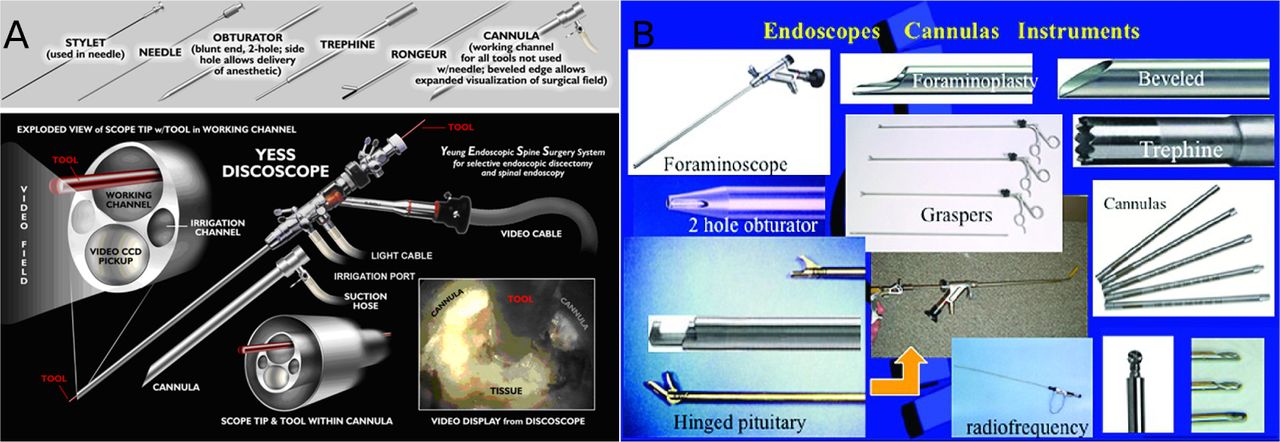
- Fig. 8
A. The Richard Wolf YESS endoscope facilitates endoscopic documentation of pathoanatomy. The uniqueness of the YESS scope is the 2.8mm working channel with integrated distal irrigation ports that keep the lens clear of blood that may otherwise obscure Intradiscal and epidural visualization.
B. In addition to custom instruments used by the senior author (ATY), Wolf has a full complement scopes and instrumentation designed for disc inspection, disc excision, foraminal decompression, and ablation. An additional complement of scopes with working channels and instruments offer operating ports of 2.2, 2.8, 3.1, and 4.2mm are used for discectomy, rhizotomy, foraminoplasty and for the trans foraminal and translaminar approach to the lumbar spine.
- Fig. 10
Extraforaminal herniation.
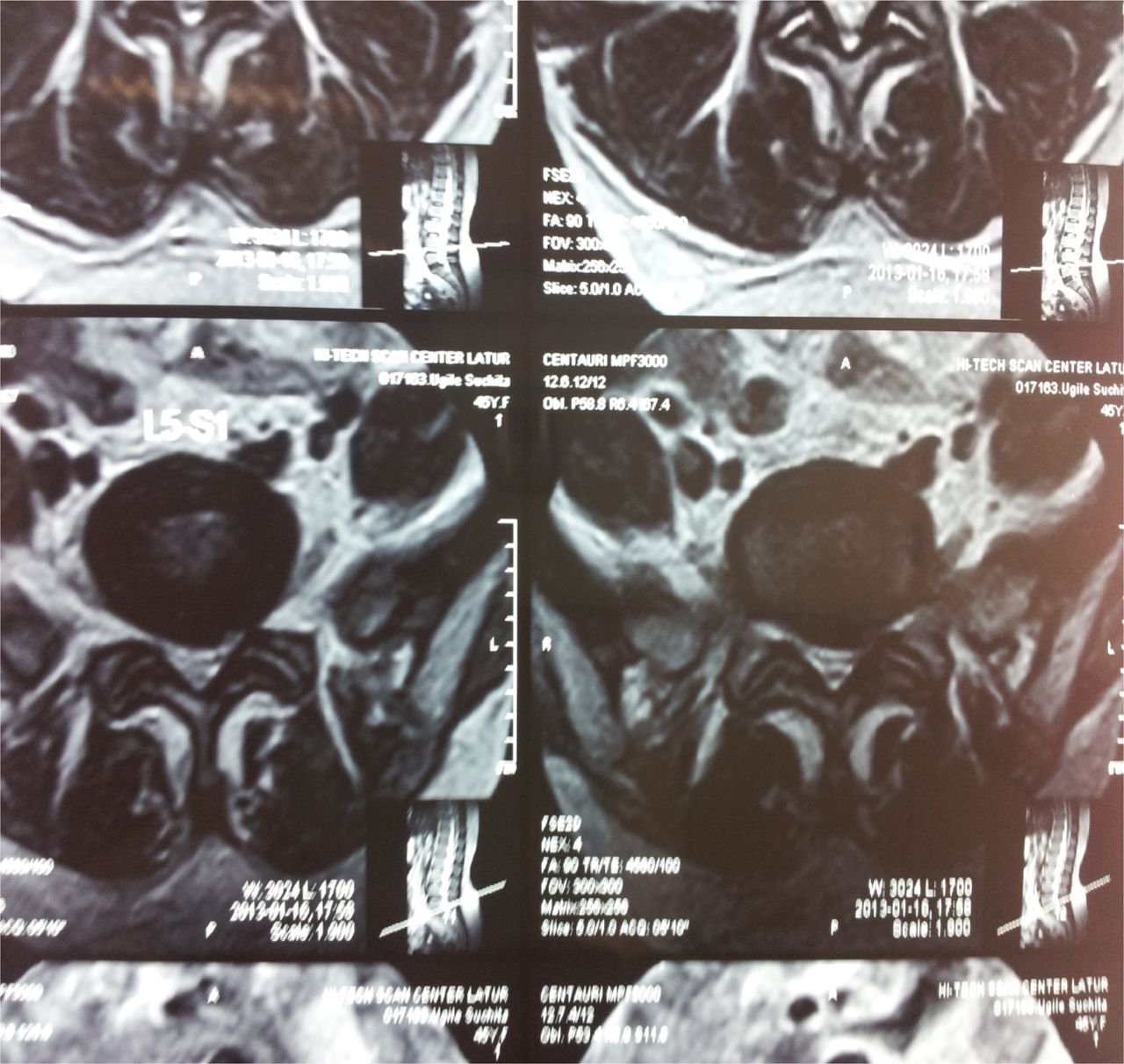
- Fig. 11
Paracentral herniation.
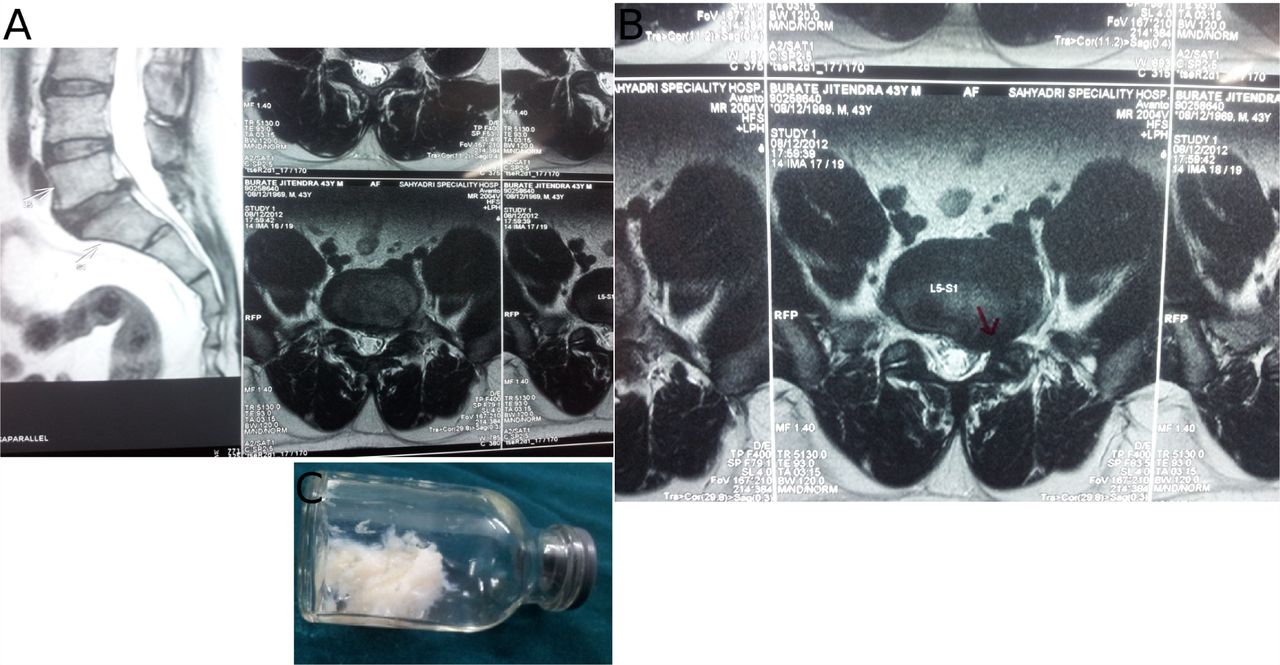
- Fig. 12
Central herniation.
- Fig. 13
Paracentral and foraminal left annular tear, which was treated successfully.
- Fig. 15
Karl Storz Gore System of instruments for lumbar spine endoscopy and surgery. This set includes bipolar cautery probe, kerrison style roungeurs, angled articulated instruments, and trephines. In addition it has a drill, burr, and shaver set. The set has a 3.625 mm working channel, and instruments are specially configured for shorter Asian morphometry. It has a hook, which helps with probing, nerve mobilization and manipulation of annular tears. The basic set has 9 instruments needed for simplicity, but adequate for routine surgery.
- Fig. 16
Endoscopic instruments shown Illustrations show a 1 hook, 2 articulated graspers for targeting migrated fragments and 3 a back biter amongst others.
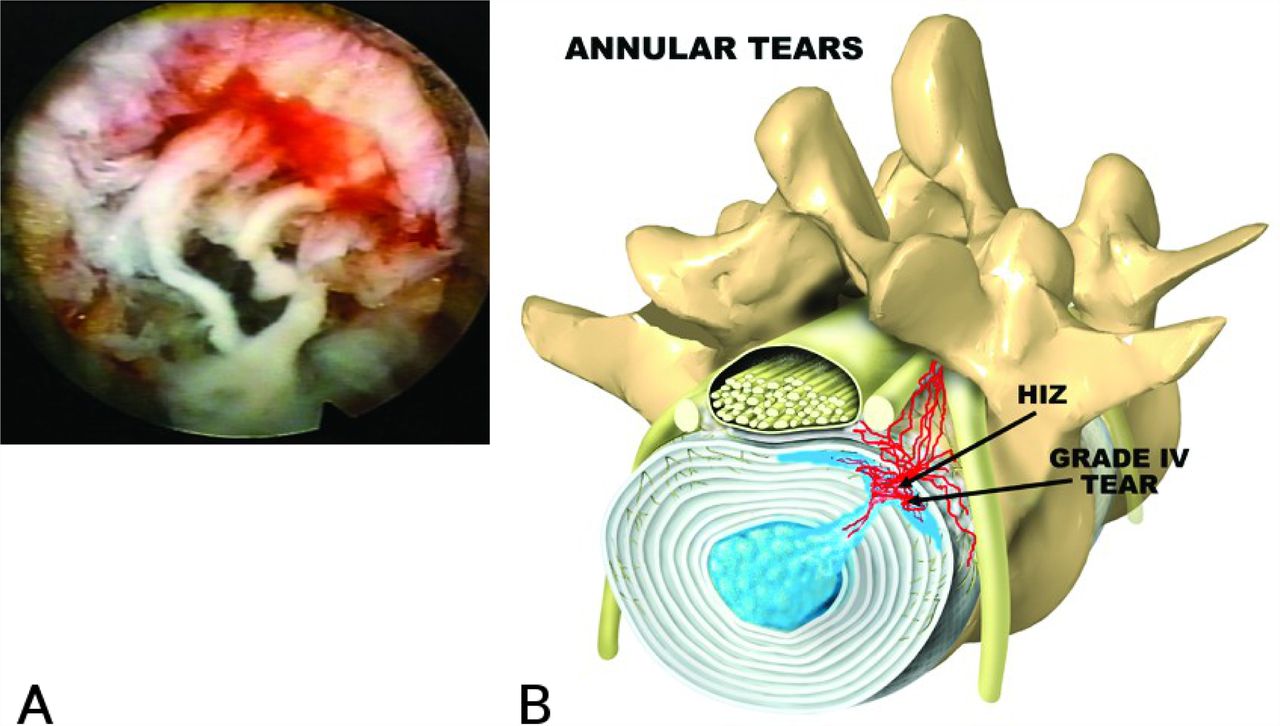
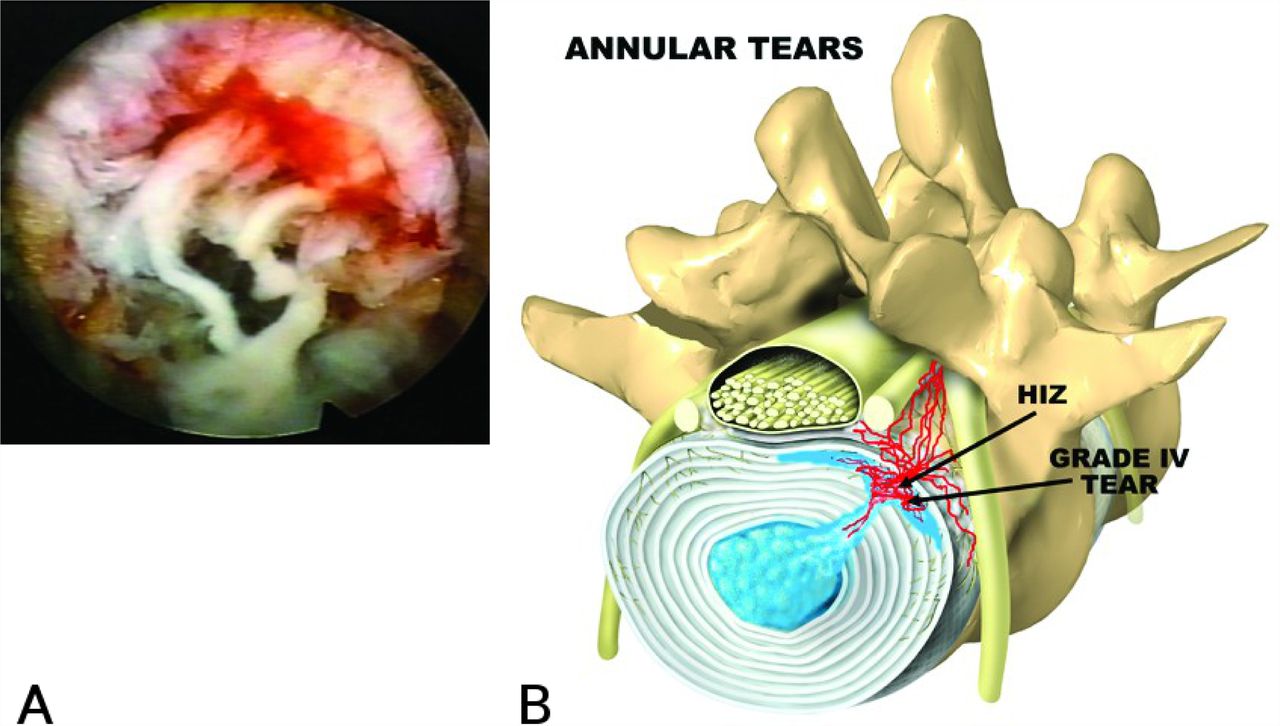
- Fig. 17
Annular tears.
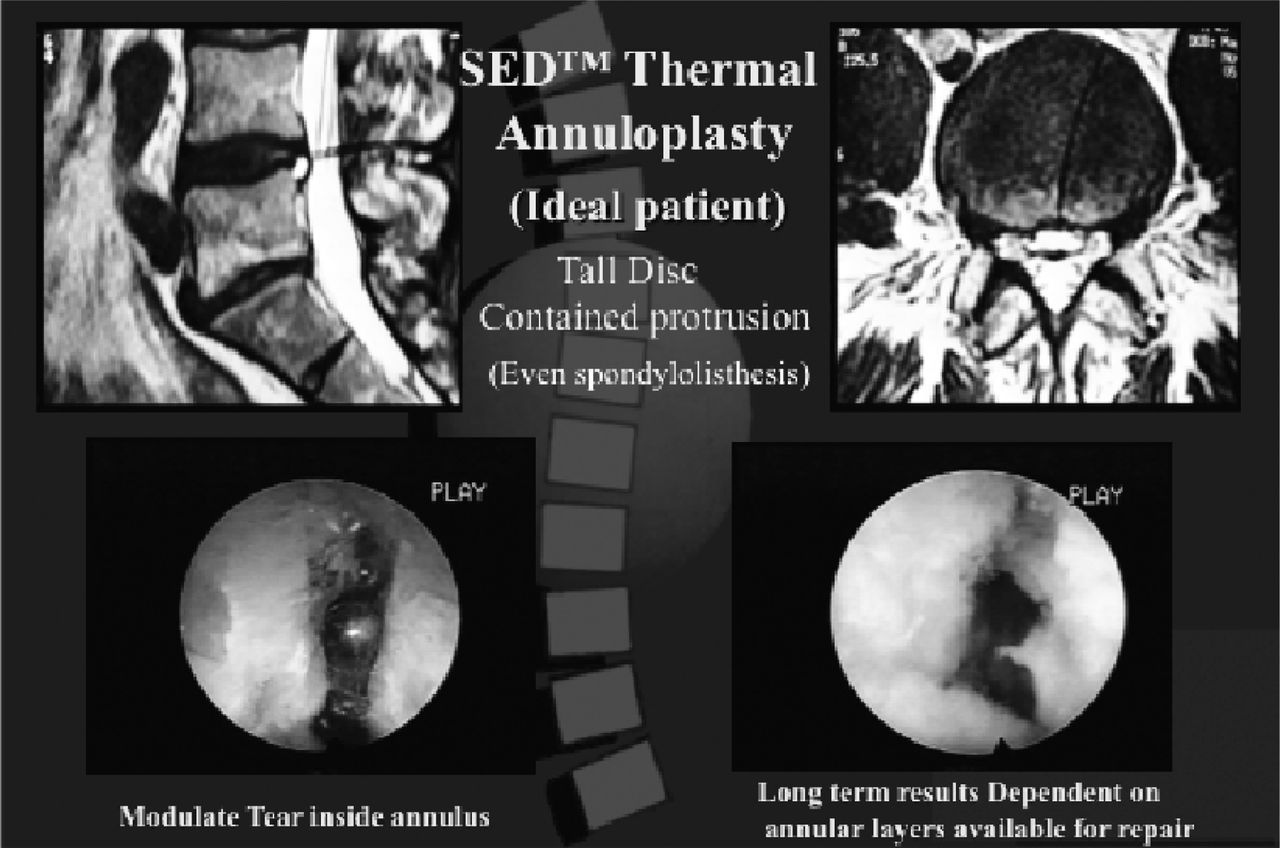
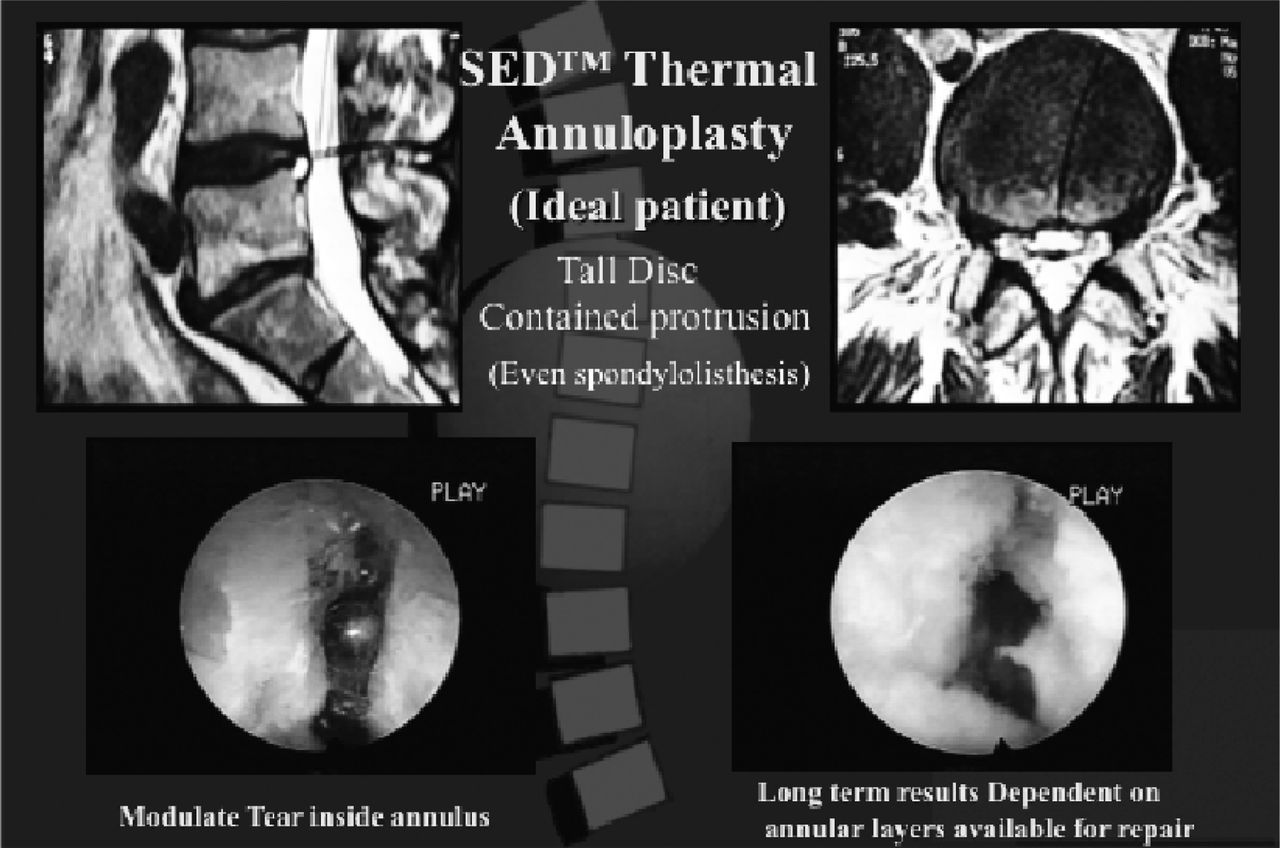
- Fig. 18
Radiofrequency Thermal Modulation of a Grade IV annular tear in a tall disc.
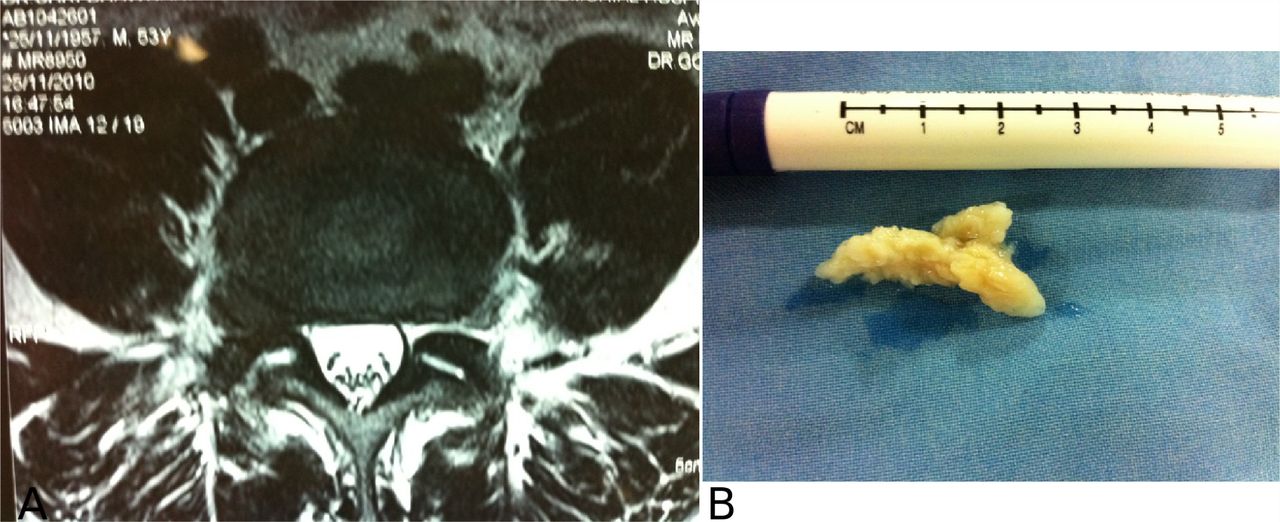
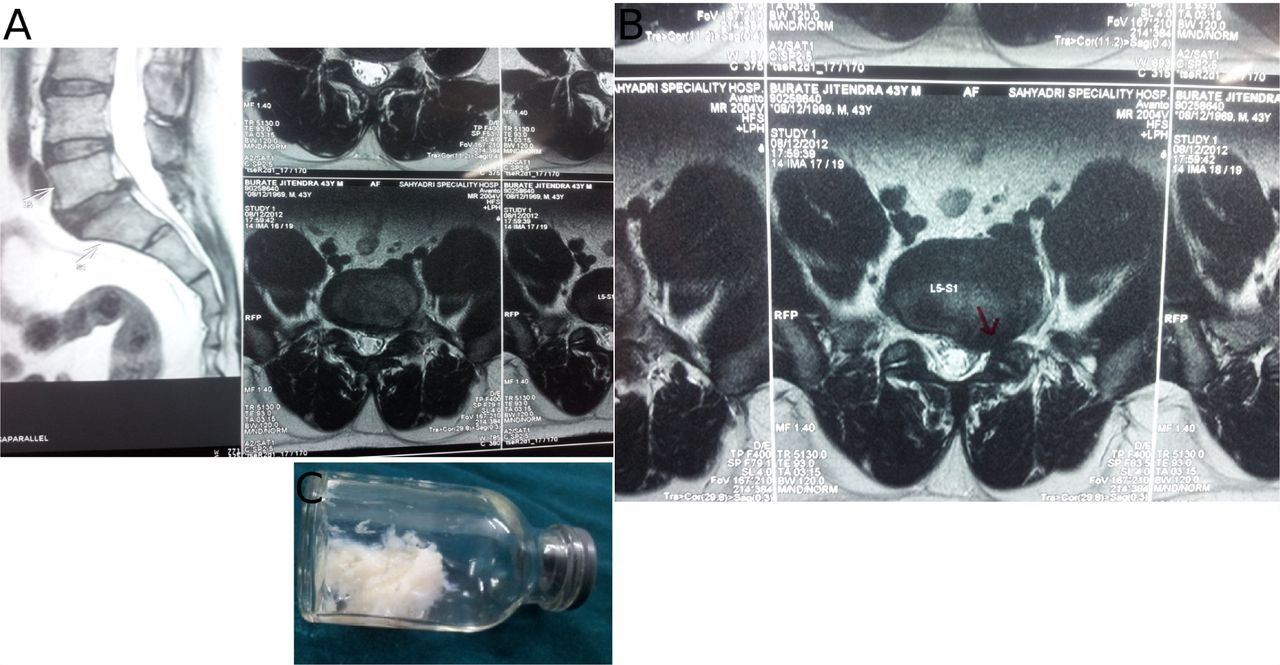
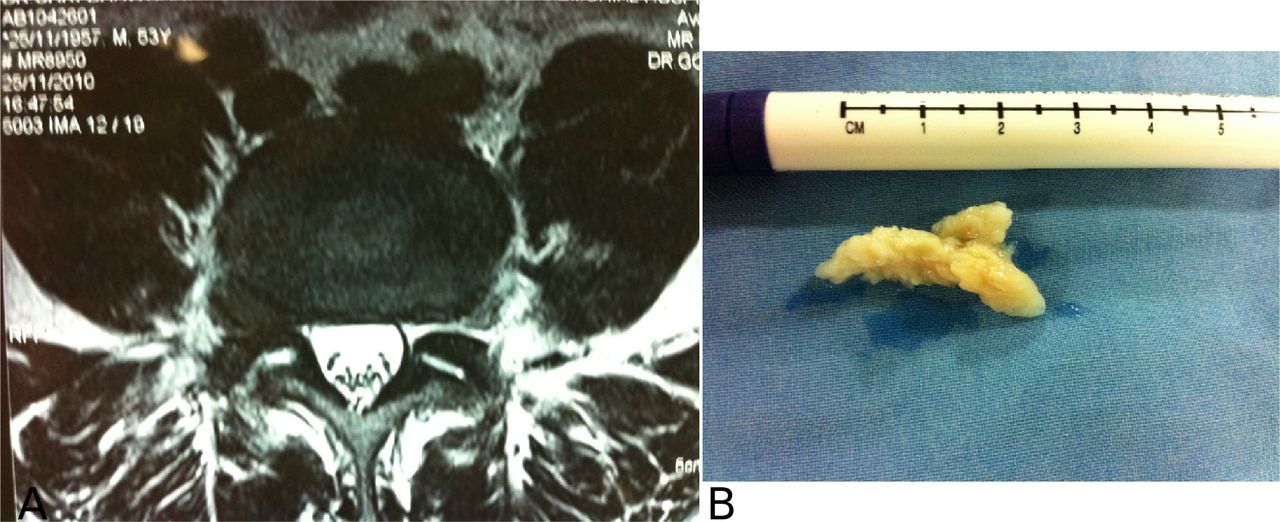
- Fig. 20
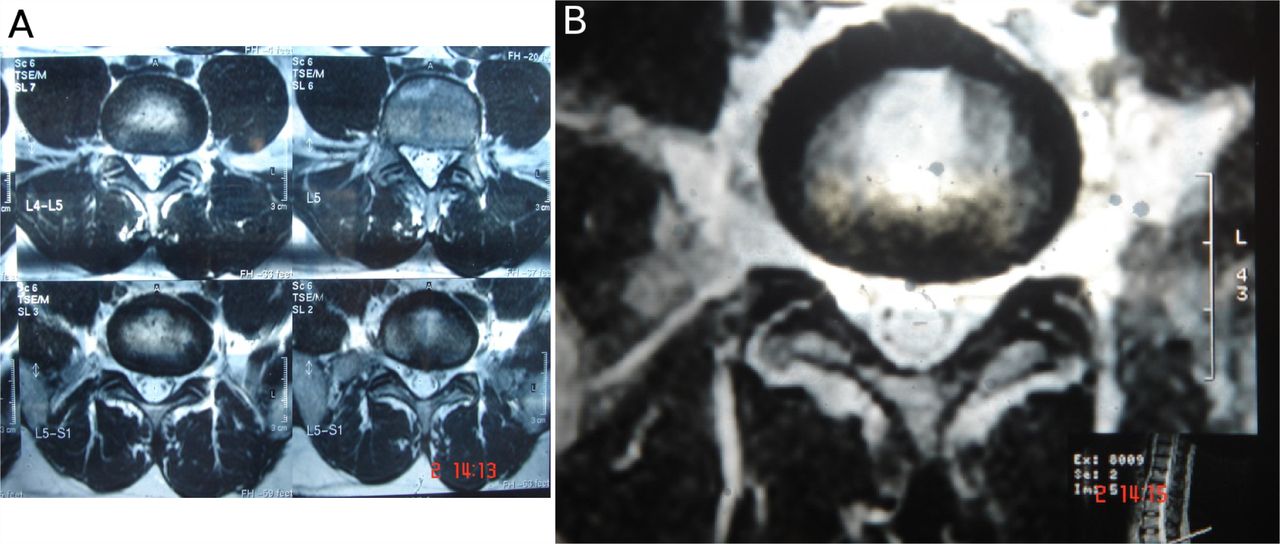
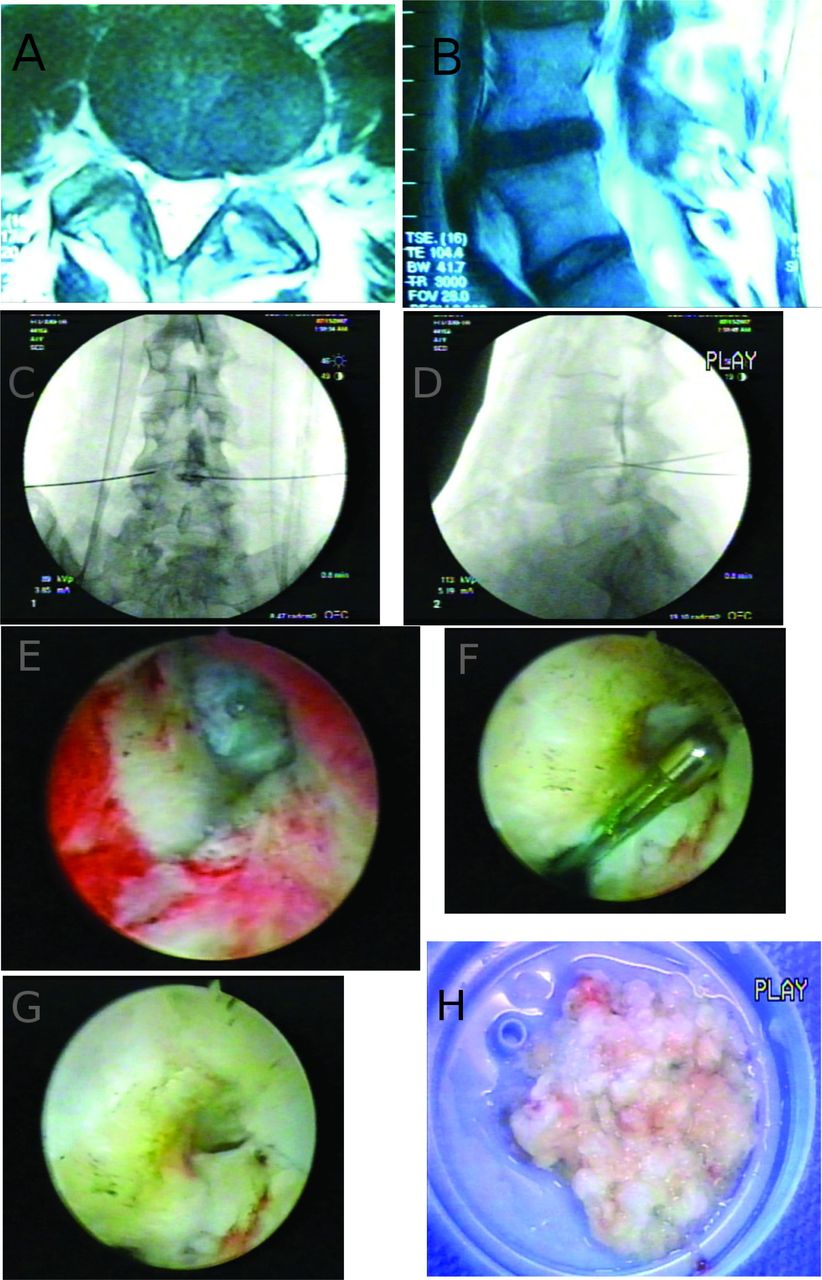
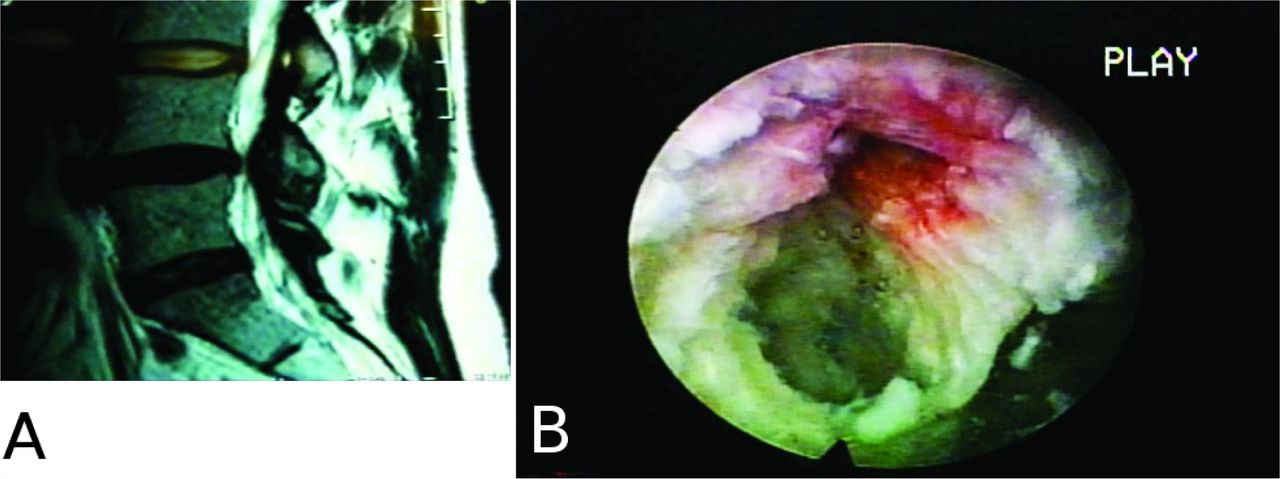
A: This saggital MRI demonstrates two dark discs on T2 imaging, but does not show significant disc protrusion or the presence of an HIZ. It could be interpreted as “normal.” Positive evocative discography identified a painful grade IV annular tear. B: The annular tear is identified endoscopically and successfully treated with foraminal discectomy and thermal annuloplasty.
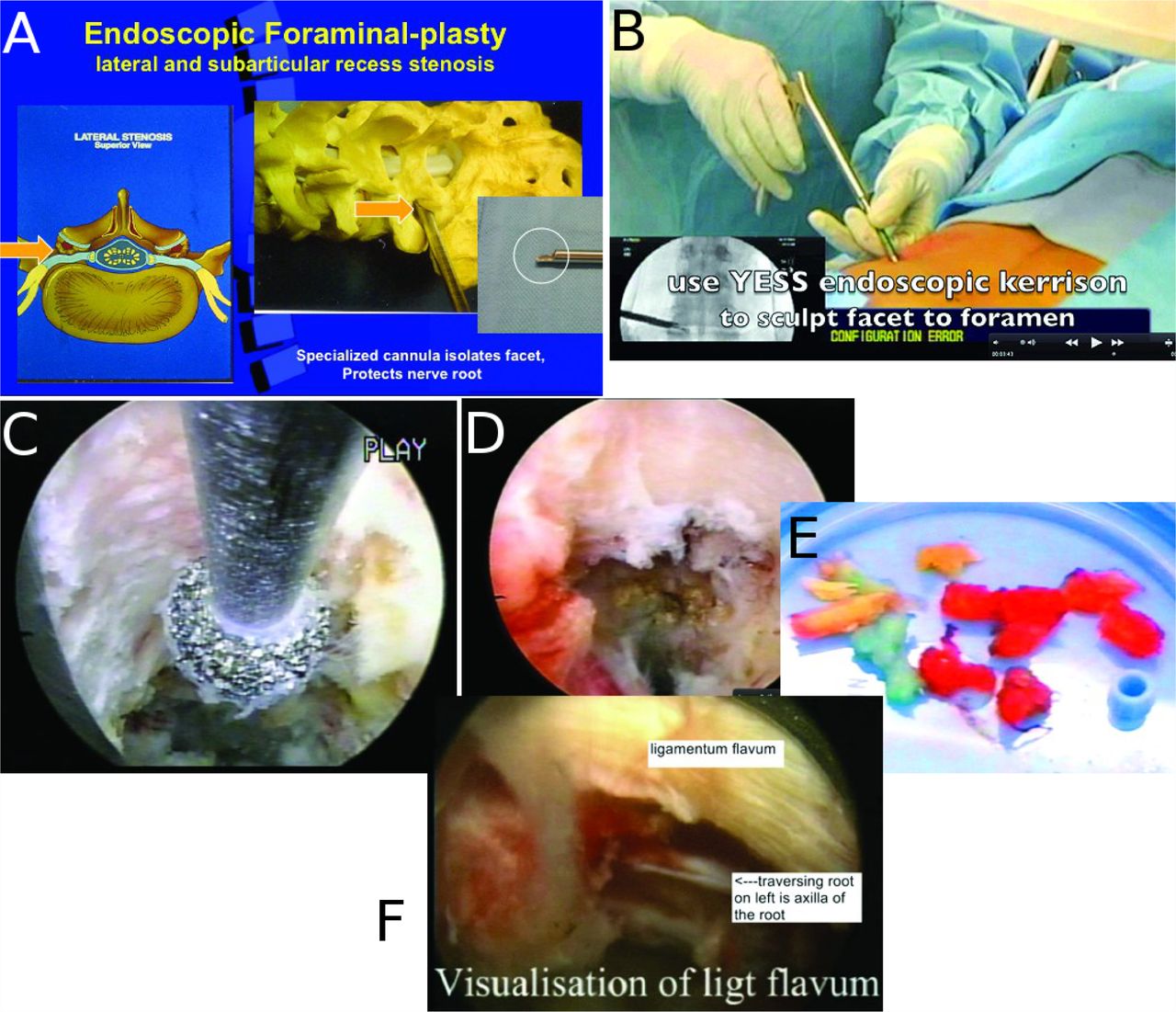
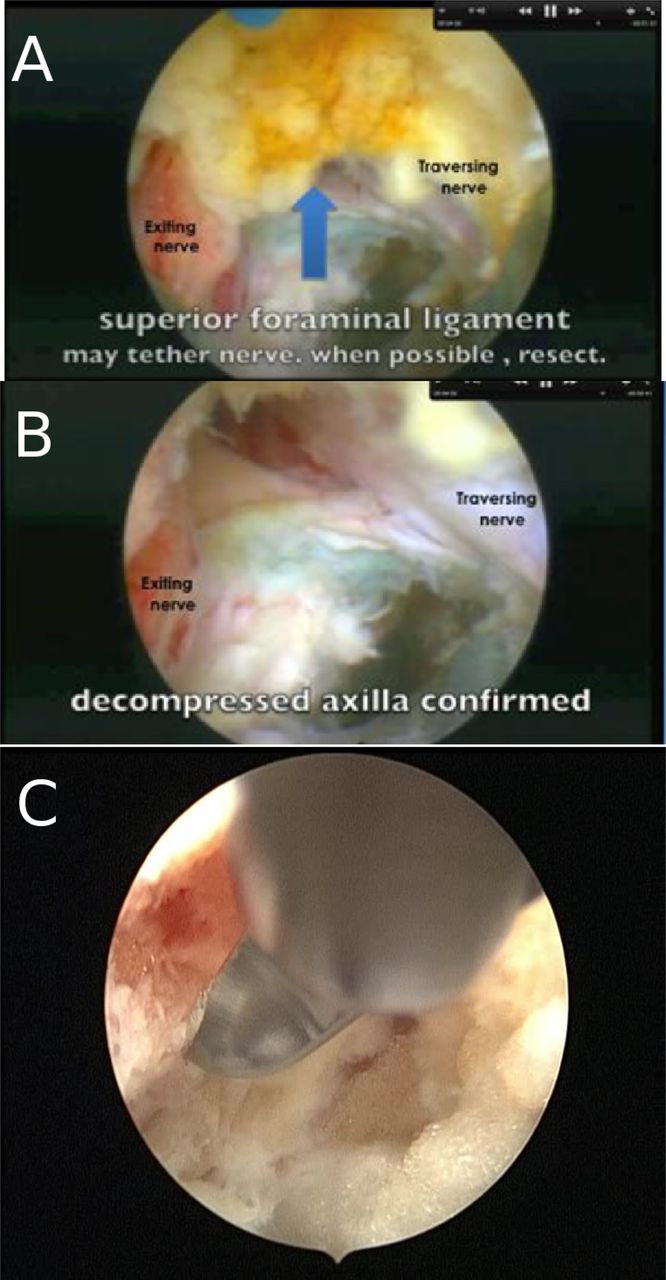
- Fig. 23
A. Cannula placement for foraminalplasty. B. Kerrison foraminoplasty. C. Diamond burr decompressing ventral aspect of the SAP. D. Relationship of the exiting nerve with the SAP. E. Bony specimen and foraminal disc fragment removed following foraminoplasty. F. The ligamentum flavum seen well.














Tables
Study
AuthorsInclusion Exclusion Type in most not known unless mentioned Intradiscal Follow-up
All followed up except where mentionedOutcome Year and Reference Schreiber suezawa leu Radiculopathy 1 N = 174 m 68 f106 age 39years [16-81] multiple level n = 25 +modified hijikata biportal 28mth , Gpe s/s score
85 e + g
Complications 10 %
Reoperation Rate 21%1986; 1988; 199136, 37, 38, 39 Savitz Radiculopathy, tension signs, neuro deficit 1,4 obese N = 300 m 132 f 168 16-81 years
multilevel n = 40
L2-S1+ Kambin technique 6 months Return to work at 6 months 67%
Complications 5.3 %
Reoperation Rate 1.3%40,41 1994, 1999 Mayer and brock Radiculopathy, tension signs, neuro deficit 1,3,4,5,8,9 N = 30 m11 f 19
multi level n = 1
L2-L5+peld 6-18 months Gpe s/s scope 67
e + g 33 moderate or poor [inclu reop]
90% returned to work at 6 months in 7.1+ - 4.2 wks
Complications 3.3%
Reoperation Rate 3.3%199342 Ditsworth Radiculopathy, tension signs, instability Flexible endoscope 5,8 N = 110 m 40 f 70
55 years[20-65]
all ldh
single level+ and
ic too24-48 months Gpe 91 exe +g
4.5 poor
rec 0
Complications 0.9%
Reoperation Rate 4.5 %43 1998 Hag Radiculopathy neurodeficit Sofamor danek system 2 N = 101
all ldh
single level L2S1
3 exclu as procedures had intraop problem+ 28 months[15-26]
9 did not respondps: good 66 satisfied 9 poor 25
Complications 7.6
Reoperation Rate 17199944 Hochschuller Radiculopathy AMD kambin method 1,4,7 N = 18 m5 f 13
31 years[18-55]
L3-S1+ 9 months [4-13] Reop 11% 199145 Kambin Radiculopathy tension signs, deficit AMD Kambin technique biportal n = 59 3,4,6 N = 175 m76 f 99
all ldh
Single level
L2-S1+pure 48 months [24-78]
3.4 did not respondGPE [mod presby st.luke score]
77 exc 11 good
12 failed
return to work 3 weeks 95%
Complications 5.3
Reoperation Rate 7.7199246 key: sequestrations[1], calcified or narrow disc[2], cauda equina syndrome[3], previous same level surgery[4], instability[5], large extra ligamentous disc[6], high iliac crest[7], stenosis[8], listhesis[9].
Study and author Indication Exclusion Total, sex distribution, age , type where known, levels Intra and extradiscal Followup
% nonresponsiveResults on GPE or Mcnab, excellent, poor, recurrence, complications, reoperative
NK is “not known”Year and reference Yeung and Tsou Prior disc surgery n = 31 radiculopthy neuro deficit 1,8 All herniations n = 307 m 102 f 205 age 18-72
Singles
l2 to s1+ yess RW Mean 19 months 8.8% non responders Macnab 84 poor 9.3% rec 0.7%
complic1ations 3.9
Reoperation Rate 4.6200247 Wojcik Radiculopathy 1, ddd N = 43 m25 f 18 intra hijikata method 18 months
16.3% nonrespondersGPE 64 good 36 satisfied 0 poor
Complications NK
Reop NK200448 Tsou and Yeung Radiculopathy neurodeficit 1,4 N219 m83 f 136
age 42[17-71] Central ldh
single level
L3S1+
yess
rw20 months [12-108] 11.9 non resp Gpe 91 e + g poor 5.2 rec2.7
Complications 2.7
Reoperation Rate 4.620023 Lew Radiculopathy tension signs neuro deficit 4 N = 47 m 12 f 35
51 years[30-70]
foraminal exforaminal
L1-L5
+ pedSurgical dynamics system 18 months [4-51] GPE 85 e and g 11 poor return to work 89% Complications 0
Reoperation Rate 11200149 Hoogland ? ? N = 246 nk nk Extra Thessys system 24 months Gpe 86% exc + g
7.7 poor
Complications 1.2
rec 3.5 [1 year]200350 Eustacchio Radiculopathy, tension signs neuro deficit 3 N = 122 m36 f 86
55 years [18-89]
all ldh
multilevel n = 4
L2-S1
10 exclu as stopped procedures but here we reviewedintra 35 months[15-35] Gpe 45 exe 27 good
27 poor
Prolo 71.9% exe + good retrun to work 94
rec 12
Complications 9
Reoperation Rate 27200251 Chiu Virgin and prior disc surgery pain in back, radiculopathy, neuro deficit 3 N = 2000 m 990 f 1010 44 years [24-92] single multiple level type nk stenosis and ddd included Intra and KARL STORZ eq TF MEAD 42 months [6-72- GPE 94 exc +g 3 poor Complications 1
Reoperation Rate nk200452 Ahn Prior disc surgery, tension signs, neuro deficit, radiculopathy 2,5,9 N = 43m11 f 32 46years[22-72 all rec after 6 months of microdiscectomy L3S1 Intra and Peld 24-39 months VAS 8.7 to 2.6 diff 70 % GPE 28 exc 63 good
4.7 poor
Complications 4.6
Reoperation Rate 2.3200453 Suess Radiculopathy deficit 3,8 N = 25 m 11 f 14 48 years [26-72] foraminal +exF single level L2-L5 PTFES sequestrectomy 6 weeks Pain leg vas 6.7 to 0.8 diff 88%
pain back 5.1 to 1.3 diff 75%
Complications 4
Reoperation Rate 8%200554 Schubert and hoogland Radiculopathy, tension signs, deficit, sequestration 4 N = 558 m 179 f 379 44 years [18-65 all ldh single level L2S1 Intra and Thessys system 12 months
8.7 non respPain leg 8.4 to 1 diff 88% pain back 8.6 to 1.4 diff 84%
GPE 51 exc 43 good
0.3 poor
rec 3.6
Complications 0.7
rec 3.6200555 Ruetten Radiculopathy deficit 1,4,8 N = 517m 277 f 240 38 years[16-78] all ldh multiple level n =46 L1-L5 Intra and RW elted extreme lateral transf n = 27 bilateral 12 months
10 non respPain leg 7.1 to 0.8 diff 89%
pain back 1.8 to 1.6 diff 13 %
ODI 78 to 20 diff 74% rec 6.9
Complications 0
Reoperation Rate 6.9200556 Ramsbacher Radiculopathy deficit 1,7,8 N = 39 m21 f 18 mean age 50 years all ldh single level L3S1 Intra and Sofamor danek TES transf endo sequestrectomy 6 weeks Pain leg 6.7 to 0.8 diff 88%
pain back5.1 to 1.3 diff 74%
ps 77% very satisfied +satisfied
Complications 5.1
Reoperation Rate 10%200057 Knight Prior surgery n = 75
back and leg pain radiculopathy
Includes DDD and lateral stenosis3 N = 250 48 years [21-86] all ldh single multiple level L2S1 Intra and ELF KESS RW 30 months [24-48] 3.2 non resp Pain vas more than 50% improved 56%
ODI 60% improved
Complications 0.8 %
Reoperation Rate 5.2 %1999 and 200115, 18 Schenkenbach and Hoogland Radiculopathy, tension signs, deficit ? N = 130 m43 f 87 39 years all ldh single level L2S1 Intra and Thessys system etd 12 months
5.1 non resppain leg diff 5.9 pain back diff 5.4 GPE 56exc 27 good 6 poor
return to work 6 weeks 70%
Complications 1.5
Reoperation Rate 4.6 %1998-99.28, 58 Morgenstern Radiculopathy deficit * study to compare normal vs intense PT postop revalidation 1 N = 144 m 48 f 96 all ldh multilevel n = 60 L1S1 Intra and Yess ess endoscopic spine surgery 24 months [3-48] GPE m 83 exc +good
3% poor
Complications 9%
Reoperation Rate 5.6%2005 59 Author Inclusion Exclusion Number, gender distribution, age, levels and type Misc Followup and did not respond in % Results Year & reference Tzaan Pain in leg and back 1,2,3,5,8 N = 134 m 56 f 78
22-71 years
All ldh
multiple level n =20 l2s1intra + peld 38 months [3-36]
0% nonrespondersGpe .m.28 excellent 61 good 3.7 poor
rec 0.7
Complications 6
Reoperation Rate 4.5200760 Shim Radiculopathy ? N = 71 m 39 f 32 45years[21-74]
n = 14
L5-S1
Interlaminar
single level
T12-S1Intra only 6 months [3-9] 0 non resp Gpe.m 33 exce 45 good
6.5 poor
Complications 2.8
Reoperation Rate 7%200761 Jang Radiculopathy 4,5,8,9 N = 35 m 20 f 15
61 years [22-84] foraminal extraforaminal
single level
L2-S1Intra + TPED system nk 18 months [10-35]
0 nonrespPain vas 8.6 to 3.2 diff 63% Gpd 86 exe and g 8.6 poor
rec 0%
Complications 17
Reoperation Rate 8.6200662 Iprenburg Nk 8 N = 149 m 62 f 87
43 years[17-82]
all ldh
single level
L3-S1Intra + Thessys system FU NK
29% nonrespvas nk od nk
rec 6
Complications or Reoperation Rate nk200763 Choi Radiculopathy tension signs neuro deficit 2,4,5,8 N = 41 m 23 f 18 59years[32-74] extraforaminal
single level
L4-S1
+ETFyess 34 months [20-58]
4.9 non resppain vas 8.6 to 1.9 diff 78% return to work 4-24 weeks mean 6
ODI 66.3 to 11.5 diff 83%
ps 92
rec 5.1
Complications 5.1 Reoperation Rate 7.7200764 Kafadar Radiculopathy, tension signs, deficit 2,4,5,8 N = 42 m 2 f 40
18-74 years
all ldh
single level
L45
8 excluded as procedure stopped but inclu hereKARL STORZ PETD 15 months [6-24]
0 non respGPE ss 14 exc 36 good
36 poor
rec 0
Complications 45
Reoperation Rate 17200665 Hoogland Recurrence only; radiculopathy, tension signs, deficit
Patients only with recurrences after micro or endo disc surgeryNk N = 262 m 76 f 186
46 years [18-80]
all ldh
single level
L2S1Intra + Thessys system 24 months
9% non respPain leg 8.5 to 2.6 diff 69% pain back 8.6 to 2.9 diff 66% GPE exc 51 good 35
poor 5
rec 6.3
Complications 1.1
Reoperation Rate 7200866 Sasani Radiculopathy, tension signs, neurodeficit 4 N = 66 m 36 f 30
52 years [35-73] foraminal exf
single level
L2-L5KARL STORZ PED 12 months
0 non resppain vas 8.2 to 1.2 diff 85% ODI 78 to 8 diff 90%
Complications 6.1
Reoperation Rate 7.6200767 Lee Radiculopathy, deficit, sequester 4,5,8 N = 116 m43 f 73
36 years [18-65]
single level
L2 S1Intra + Yess PELD 14.5 months [9-20]
o non respPain leg 7.5 to 2.6 diff 65% GPE m 45 exc 47 good
6 poor
return 2 work av 14 days [1-48 days]
rec 0
Complications 0
Reoperation Rate 0200768 Authors/year/hernation type procedure operating time (min)
/blood loss
(ml)clinical outcome criteria Reoperations complications Ruetten et al,
2008 lumbar recurrentTFE, IL FE
sequestrectomy24 (14 - 43)/
0VAS back: 14 to 15
VAS leg: 79 to 8
ODI: 80 to 20
NASS pain: 4.3 to 2.1
NASS neurology: 2.5 to 2.1
RTW 28 days5 overall (11.1%)
3 for recurrent herniation
2 for persistent leg paindural tears: 1
transient postopdysesthesia: 2
serious complications: 6%** overall 9 poor outcomes no subgrouping microsurgical sequestrectomy (paramedian approach) 58 (39-91)/
41 (10-205)VAS back: 15 to 14
VAS leg: 85 to 10
ODI: 84 to 21
NASS pain: 4.5 to 2.1
NASS neurology: 2.3 to 2.3
RTW 52 daysRuetten et al, 2008 lumbar
(median, lateral, extraforaminal)endoscopic interlaminar or transforaminal sequestrectomy 22
(13-46)/
0VAS back: 19 to 11
VAS leg: 75 to 8
ODI: 75 to 20
NASS pain: 4.6 to 2.1
NASS neurology: 3.1 to 2.1 RTW 25 days9 overall (9.9%)
6 for recurrent herniation
2 for repeated recurrence
1 fusion for progressive
LBPtransient postoperative dysesthesia: 3
serious complications: 0** 13 over all poor outcomes no subgroupings microsurgical sequestrectomy (paramedian or lateral) 43
(34-72)/
45 (5-235)VAS back: 15 to 18
VAS leg: 71 to 9
ODI: 73 to 24
NASS pain: 4.2 to 2.3
NASS neurology: 2.9 to 1.9
RTW 49 days10 overall (11.5%)
5 for recurrent herniation
5 fusions for progressive LBPtransient postoperative dysesthesia: 5 postoperative bleeding: 2 delayed wound-healing: 2 soft tissue infection: 1
transient urinary retention: 3 serious complications: 0Hermantin70 randomized controlled trial 60 pts Age 40 av >3 months pain LBP radicular pain, iamage conf L2S1 disc, cons tt ineffective Backpain, improvement,
return to work RTW,
patient satisfaction,
complications,
reopKrappel85 randomized controlled trial 40 pts 40 >1 month Mri conf disc herniation,pain, deficit, failed cons tt Mcnab, RTW, complications, reop, cost Mayer42 randomized controlled trial 40 41 6.9 Failed cons tt, small non contained disc Back leg pain, disability,symptom score,RTW,op time,reop Kim86 Retro 902 41 11 Pain,failed constt, single level Mcnab, op time, blood loss, complications, reop, radiology Lee72 Retro 60 39 >3 Ct mr conf disc, leg pain >back unilateral,failed cons tt Macnab, op time, length of hospitalization,radiological Lee75 Retro 54 45 Previous open surgery,recurrent radicular pain,MRI conf disc,failed cons tt Back leg pain,ODI,op time,length of hospitalization,complications,reop Ruetten74 randomized controlled trial 200 43 3 Radicular pain,deficit,failed cons tt Back leg pain,ODI,satisfaction,op time, blood loss, compli,reop,NASS score Ruetten73 randomized controlled trial 100 39 2 Recurred disc,MRI conf,leg pain, deficit,failed cons tt Back leg pain, ODI, satisfaction, op time, blood loss, compli, reop, NASS score Data source: Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis, Kamper et al. Eur Spine J (2014) 23:1021–1043. The data has been used to read and collate the references and make meaningful groups based on timeline. These studies are the only studies which have been recently considered to appreciate the state of endoscopy at present.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Master Techniques in Minimally Invasive Spine Surgery: Lumbar Endoscopic Spine Surgery
- Durotomy- and Irrigation-Related Serious Adverse Events During Spinal Endoscopy: Illustrative Case Series and International Surgeon Survey
- Durotomy- and Irrigation-Related Serious Adverse Events During Spinal Endoscopy: Illustrative Case Series and International Surgeon Survey
- Differential Agnostic Effect Size Analysis of Lumbar Stenosis Surgeries
- Difficulties, Challenges, and the Learning Curve of Avoiding Complications in Lumbar Endoscopic Spine Surgery
- Feasibility of Deep Learning Algorithms for Reporting in Routine Spine Magnetic Resonance Imaging
- Percutaneous Endoscopic Lumbar Discectomy Versus Microdiscectomy for the Treatment of Lumbar Disc Herniation: Pain, Disability, and Complication Rate--A Randomized Clinical Trial