


Article Figures & Data
Figures
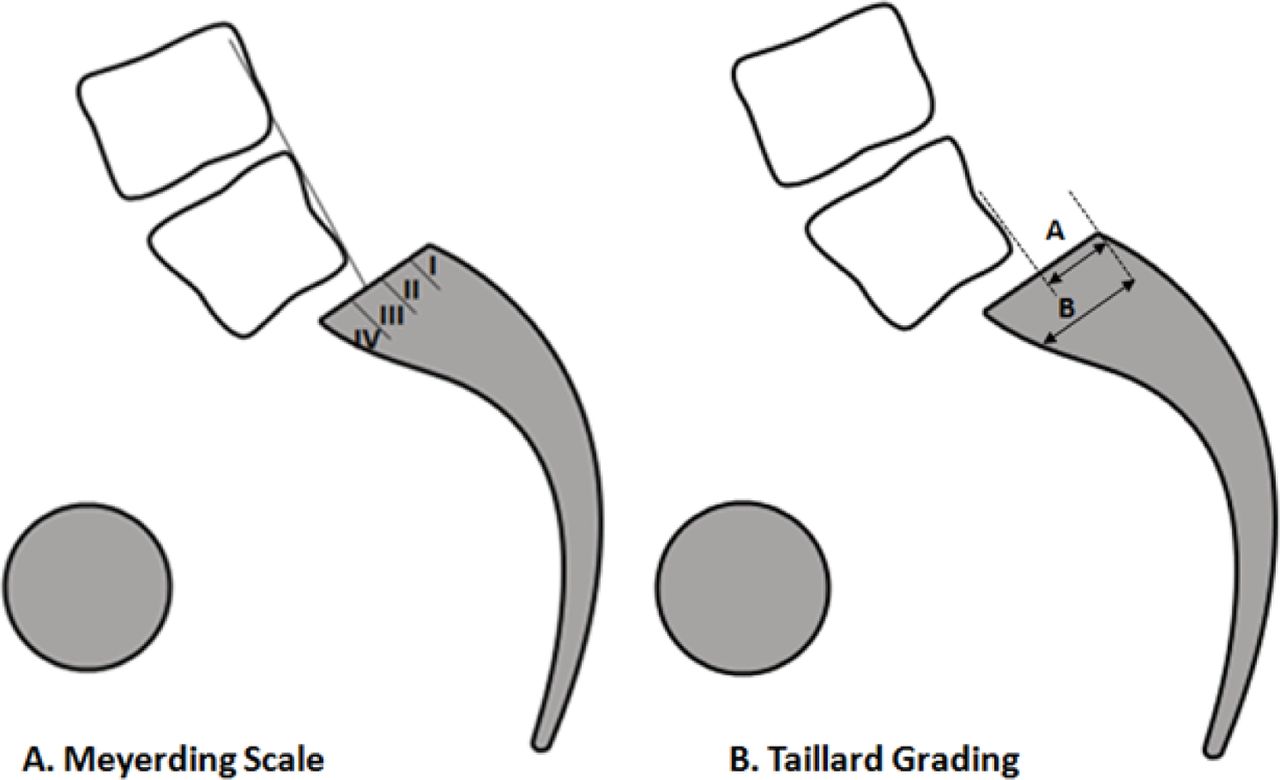
- Fig. 1
Measurement of slip angle. Meyerding scale divides the lower vertebral body into quarters and a grade of I to IV assigned respectively. Taillard grading calculates the percentage of the slip from the lower vertebra.
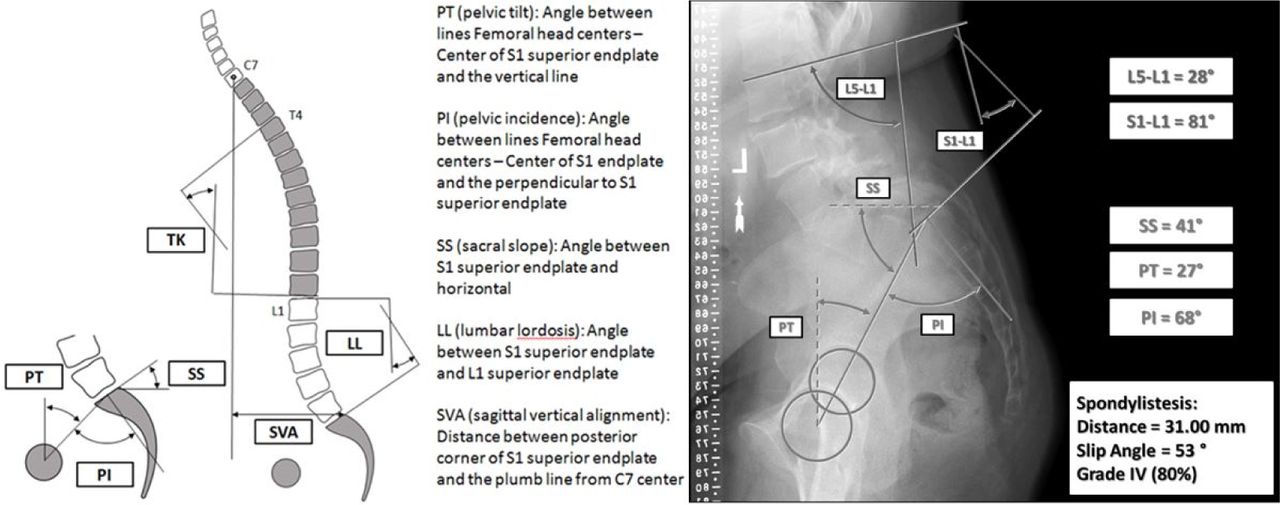
- Fig. 2
Left: Illustration of the spinopelvic parameters; Right: CT image of patient with HGS illustrating radiographic parameters (lumbar lordosis, pelvic tilt, sacral slope and pelvic incidence.
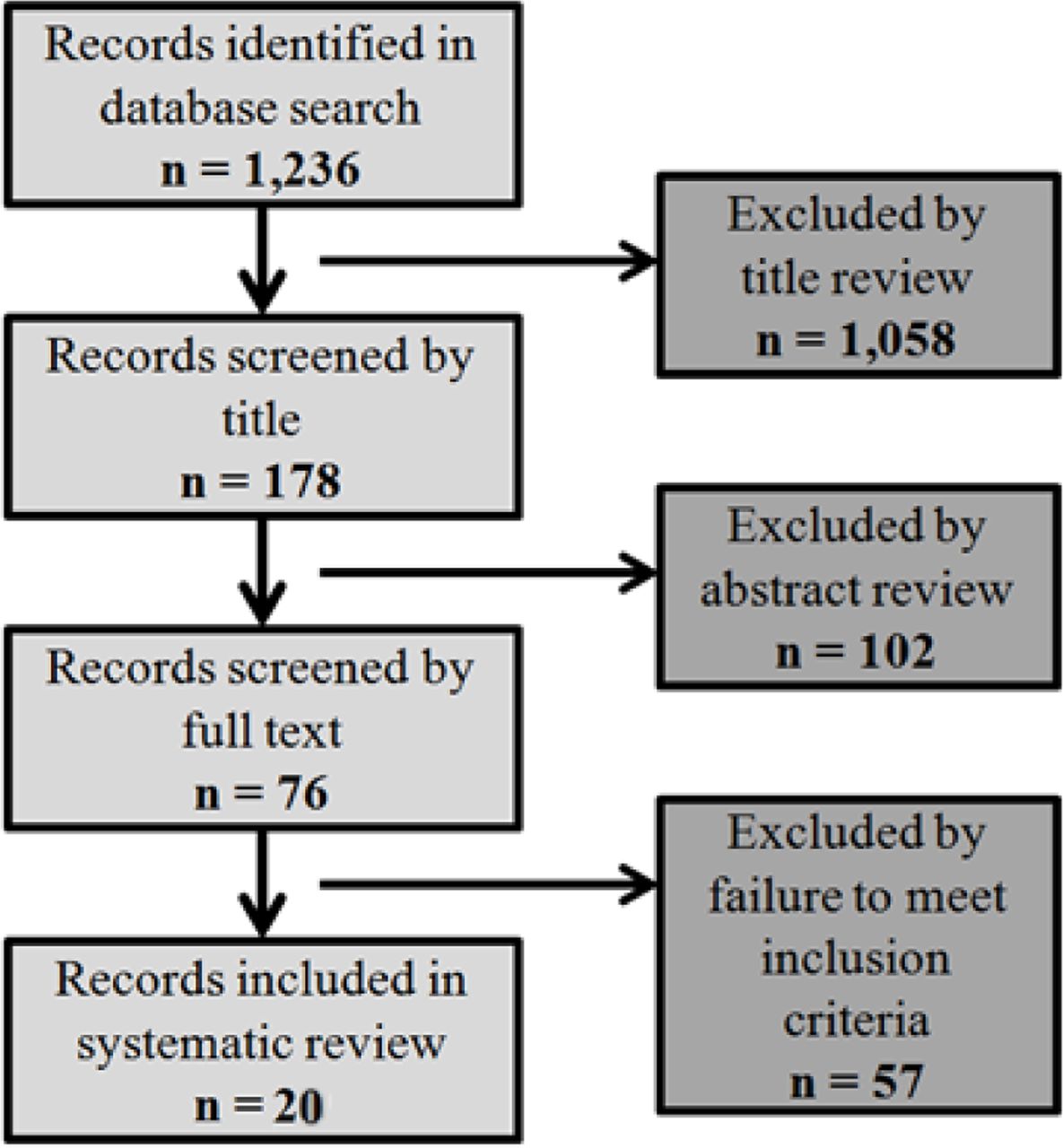
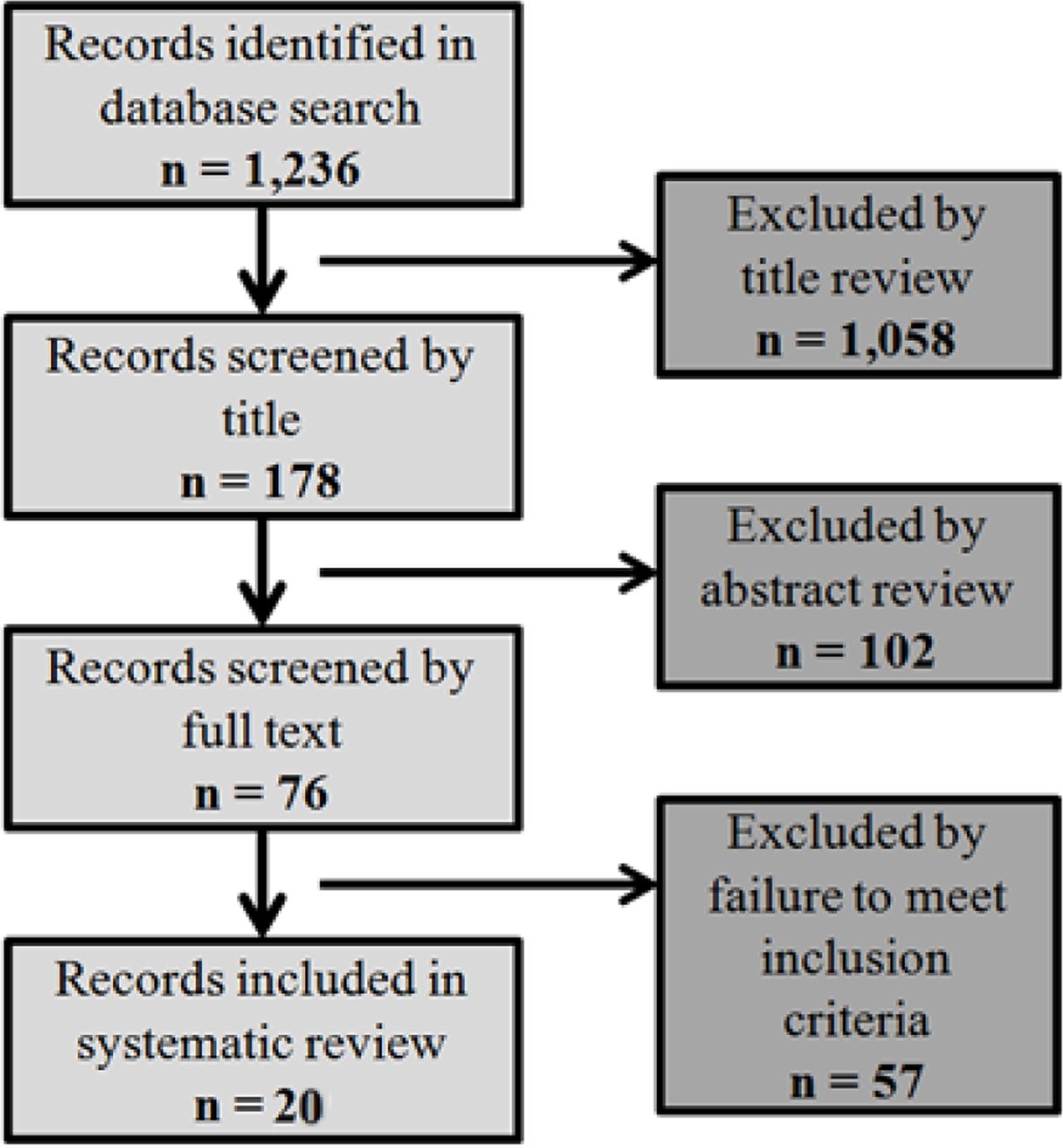
- Fig. 3
Literature review flowchart.


Tables
Study Component Inclusion Exclusion Subjects Patients with high-grade isthmic spondylolisthesis • N < 10 patients
• Spondylolisthesis caused by underlying disorder
• Low-grade, degenerative or dysplatic spondylolisthesis
• Infection
• TumorStudy Design • Randomized and non-randomized controlled trials
• Retrospective Reviews
• Radiographic studies evaluating subject outcome• Cadaver studies
• Case reports
• Meeting abstracts/ lectures
• Biomechanical analyses
• Studies evaluating classification systems
• Studies not written in English
• <2-yr follow-up (for clinical studies)
• Studies before 2002Intervention May or may not undergo operative treatment Radiographical measures • Percent slip
• Pelvic incidence
• Sacral slope
• Lordosis/kyphosis
• Level of spondylolisthesisNA Clinical factors • Complications
• Comorbidities
• Neurological statusNA Surgical factors • Levels of fusion
• Instrumentation
• Decompression
• ApproachNA Outcomes • Reduction of slip angle
• Radiological outcome
• Functional scores
• ComplicationsNA Types of Studies Therapeutic Studies Investigating the Results of Treatment Prognostic Studies Investigating the Outcome of Disease Diagnostic Studies Investigating a Diagnostic Test Economic and Decision Analyses Developing an Economic or Decision Model Level I 1. Randomized controlled trial
a. Significant difference
b. No significant difference but narrow confidence intervals
2. Systematic review2 of Level-I randomized controlled trials (studies were homogeneous)1. Prospective study1
2. Systematic review2 of Level-I studies1. Testing of previously developed diagnostic criteria in series of consecutive patients (with universally applied reference “gold” standard)
2. Systematic review2 of Level-I studies1. Clinically sensible costs and alternatives; values obtained from many studies; multiway sensitivity analyses
2. Systematic review2 of Level-I studiesLevel II 1. Prospective cohort study3
2. Poor-quality randomized controlled trial (e.g., <80% follow-up)
3. Systematic review2
a. Level-II studies
b. nonhomogeneous Level-I studies1. Retrospective study4
2. Study of untreated controls from a previous randomized controlled trial
3. Systematic review of Level-II studies1. Development of diagnostic criteria on basis of consective patients (with universally applied reference “gold” standard)
2. Systematic review2 of Level-II studies1. Clinically sensible costs and alternatives; values obtained from many studies; multiway sensitivity analyses
2. Systematic review2 of Level-II studiesLevel III 1. Case-control study5
2. Retrospective cohort study4
3. Systematic review2 of Level-III studies1. Study of non-consecutive patients (no consistently applied reference “gold” standard)
2. Systematic review2 of Level-III studies1. Limited alternatives and costs; poor estimates
2. Systematic review2 of Level-III studiesLevel IV Case series (no, or historical, control group) Case series 1. Case-control study
2. Poor reference standardNo sensitivity analyses Level V Expert opinion Expert opinion Expert opinion Expert opinion 1. All patients were enrolled at the same point in their disease course (inception cohort) with ≥80% follow-up of enrolled patients. 2. A study of results from two or more previous studies. 3. Patients were compared with a control group of patients treated at the same time and institution. 4. The study was initiated after treatment was performed. 5. Patients with a particular outcome (“cases” with, for example, a failed total arthroplasty) were compared with those who did not have the outcome (“controls” with, for example, a total hip arthroplasty that did not fail). AUTHOR Level of evidence (CP judgement on JBJS) Mean FU (years) Study Design/Type N Cases/Grade (G) if available Patient Factors (previous surgery, age, sex) Type/Level of Spondylolisthesis 2002_Hanson Level IV - therapeutic, non-comparative retrospective, case series 4.6 yrs (2-7) Retrospective clinical N = 17 (n = 15 G4; n = 2 G3) 10 primary and 7 revision, pediatric and adult (9-56, 20.3 mean), 15F 2M Isthmic, L5-S1 2002_Curylo Level III - prognostic, retrospective study with no control group n/a Retrospective radiographic n = 45 Avg age 22 (11-55), 37F 16M Spondyloptosis, bony dysplasia 2002_ Hanson Level II - prognostic, retrospective, with control n/a Retrospective radiographic N = 80 (20 HG, 20 LG, 20 adult control, 20 pediatric control) Mean age: HG (17.7, 10-50), LG (26.6, 15-51), adult (60), ped (11.8) Isthmic 2002_Molinari Level III - therapeutic retrospective comparative study 3.1 yrs (2-10) Retrospective clinical N = 31 (Higher Grade tended to get reduction and internal stabilization) 31 primary, 6 revision, adolescent (13.5, 9-20) Isthmic and dysplastic 2003_Huang Level II - prognostic, retrospective study, with control n/a (preop x-rays only) Retrospective radiographic N= 36 (n = 22 HG, n = 14 LG) Adolescents and adult: Avg 21.3 yrs (12-53), 24 women, 12 men, HG age 25.3, LG age 15.4 Isthmic only, L5-S1 only 2005_DeWald Level III - prognostic, retrospective, with no control 6.6 yrs (1-14) Retrospective review and literature review N = 21 5 revisions, Avg age 35 yrs (21-68), 13F 8M Developmental (dysplatic) and acquired (isthmic), L5-S1 and L5-L6 2005_Shufflebarger Level IV - therapeutic, case series 3.3 yrs (2-5) Prospective clinical, single arm cohort N = 18 Avg age 14 yrs (10-16), 11 women, 7 men Isthmic dysplastic 2005_Vialle Level IV - prognostic case series n/a Radiographic analysis and clinical review N = 100 Avg age 13.8 yrs (8-17), 67 women, 33 men Isthmic (with dysplastic posterior elements) 2006_Helenius Level III - therapeutic, retrospective comparative study 17.2 yrs (11-26) Retrospective comparative n = 21 posterolateral
n = 23 anterior
n = 26 circumferentialAvg age 14.4 yrs, 25 women, 45 men High-grade isthmic 2006_Poussa Level III - therapeutic, retrospective comparative study 14.8yrs (11.6-18.7) Retrospective follow-up, comparative, nonrandomized N = 22, n = 11 reduction Avg age 14.7 yrs (11-18) 16F 6M (split evenly between groups) Isthmic >60%, 3 exaggerated lumbar lordosis, 1 scoliosis n = 11 in situ Isthmic >50%, Scoliosis n = 3 due to slip, Gait problems n = 3 2006_Vialle Level IV - therapeutic, case series 18 yrs Retrospective case series; clinical and radiographic outcomes N = 40, all HG 13.5 yrs (6-18), 25F 15M all L5-S1, isthmic and/or dysplastic 2007_Hresko Level II - prognostic, retrospective study n/a Retrospective review, radiographic database of HGIS comparison to controls N = 133 HG, asymptomatic controls matched by PI 17 yrs (inclusion 10-40yrs), 70%F Developmental spondylolisthesis, L5-S1 2007_Vialle Level II - prognostic, retrospective study n/a Retrospective radiographic review w/ healthy control group Total N = 244 patients, N = 300 control; HG n = 174: G3= 98, G4= 59, G5= 17 N = 244: 13.9 yrs (6-25), 158F 86M Developmental spondylolisthesis 2008_Rodriguez-Olaverri Level III - therapeutic, retrospective comparative study 35 months (24-48) Retrospective review of two treatments - radiographs and clinical n = 20 TLIF, n = 2 Transsacral 30yrs (19-48) Mean grade 3.6 Meyerding (3-5) 2008_Sasso Level IV - prognostic, retrospective case series 39 months (30-71) Retrospective clinical study n = 25 29.8yrs High-grade isthmic spondylolisthesis 2009_Hresko Level IV - prognostic, retrospective case series 2-yr min, mean 7.5±5.4 Retrospective review n = 26 13.1 +/-3.3 yrs. 20F 6M High-grade spondylolisthesis 2010_Sansur Level II - prognostic retrospective study NA Retrospective large-scale database n = 10,242 Age >65 has higher comp rate, but not after adjusting for grade/type Degenerative and isthmic spondylolisthesis 2011_Jalanko Level III - therapeutic, retrospective comparative study HG 18 yrs (12-25) Retrospective comparative study n = 41 children, n = 19 HG 12 yrs (8-14) HG- 13F 6M Isthmic spondylolisthesis, low back pain in most or risk of progression HG 15 yrs (11-26) n = 41 adolescent matched controls (matched for treatment, gender, and slip severity), n = 19 HG 16 yrs (13-19) HG- 13F 6M 2012_Kasliwal Level II - prognostic, retrospective study n/a, short-term Retrospective study of database N = 165; n = 88 pediatric: n = 40 G3, n = 34 G4, n = 14 G5 23% revisions (overall). 13.9 yrs (7-18); 61F 27M Isthmic in n = 56 n = 77 adult: n = 53 G3, n = 17 G4, n = 7 G5. Isthmic n = 47 23% revisions (overall). 44.4 yrs (19-84); 44F 33M Isthmic in n = 47 2014_Wang Level II - prognostic, prospective cohort N/A Prospective clinical, two study arms Isthmic n = 64 44.5 yrs (13-65); 30F 34M Isthmic spondylolisthesis on L5 AUTHOR Pelvic Incidence (°) Sacral Slope (SS)/ Inclination (SI) (°) Slip Angle (°) Additional radiography (findings for radiographic studies) Conclusion 2002_Curylo Control: 48.2-53.2 Patient: 76 ± 10 NA NA Sacral Kyphosis (°): 56 ± 15 62% of patients had posterior element dysplasia Progression is linked to shear stress-related to increased verticality of lumbosacral joint, predetermined by PI and sacral anatomy 2002_ Hanson Ped Control/Adult Control/LG/HG: 47.4/57/68.5/79 SI Ped Control/Adult Control/LG/ HG: 52/50/48/42 Ped Control/ Adult Control/ LG/HG: -12/-15/ 9/26 Lumbar Lordosis (LL) (°) Ped Control/Adult Control/LG/HG: 58/58/61/58 Significant correlation between PI and Meyerding-Newman scores (p = 0.03); PI may be a good predictor of progression 2003_Huang HG: 79.6 ± 1.9 SI HG: 34.2 ± 5.1 HG: 20.3 ± 2.8 (p < 0.001) Slip%: 79.9 ± 4.2% (p < 0.001) No difference in PI or sacral inclination between HG and LG (p = 0.66, 0.33, respectively). Slip percentage and slip angle are predictive of progression. LG: 72.9 ± 3.7 SI LG: 46.5 ± 3.8 LG: -8.5 ± 5.4 (p < 0.001) Slip%: 29.5 ± 3.9% (p < 0.001) 2005_Vialle Analyzed S1 plate for bony hook/outgrowth, condensed and necrotic anterior edge, round convexity median section. Sagittal inclination, sacral angle, S1 hypoplasia, S1 bony hook negatively correlates with lumbosacral kyphosis severity; Reducibility is better without hook/L5 bony outgrowth. S1 index (cranial plate/caudal plate length) correlated with grade slip, lumbosacral kyphosis, and reducibility of kyphosis 2007_Hresko Asymptomatic: 50 ± 10.7 SS Asymptomatic: 40 ± 8 NA Asymptomatic: Pelvic tilt (PT) 10 ± 7.6 HG patients have higher PT, SS and PI, but higher PI controls also have high PT and SS. HG divided into the “unbalanced” high PT/low SS and the “balanced” low PT/high SS. Balanced is more similar to asymptomatic controls 78.9 ± 12.1 SS Balanced: 59.9 ± 11.2 NA Balanced: Pelvic tilt (PT) 21.3 ± 8.2 Slip%: 68 ± 46.9% (p = 0.13) SS Unbalanced: 40.3 ± 9.0 NA Unbalanced: PT 36.5 ± 8.0 Slip%: 78 ± 23.7% (p = 0.13) 2007_Vialle Control: 54.7 ± 10.7* SS Control: 41.9 ± 8.4* NA LL (°): -43.13 ± 11.2*
PT (°): 13.2 ± 6.1*
Lumbosacral angle (LSA) (°): 109.94 ± 7.2*PI is significantly higher in spondylolisthesis, but not clearly correlated with the grade of slipping; lumbosacral kyphosis evaluated by LSA possibly the most important factor. Patient: 73.1 ± 11.3* SS Patient: 46.6 ± 12.6* NA LL (°): -70.22 ± 17.3*
PT (°): 26.5 ± 10.9*
LSA (°): 82.3 ± 21.2*2014_Wang ODI 0-22: 74.6 ± 11.6 ODI 0-22: 52.3 ± 9.4* NA ODI 0-22:
Spondylolisthesis grade: 62.8 ± 10.4*
LL (°): 56.5 ± 9.4*
PT (°): 22.3 ± 6.3*
TK (°): 41.2 ± 8.8
SFHD (°): 44.9 ± 10.3*
SFVD (°): 109.5 ± 15.6*
SC7D (°):23.2 ± 34.3*Spondylolisthesis grade, SS, PT, SC7D, LL, SFVD, SFHD, PT/SS, SFHD/SFVD, LL/TK are significantly associated with clinical symptoms of severe isthmic spondylolisthesis; SS (-0.981, strong) and SFVD (-0.802, strong) are most significant correlations with low back pain ODI 23-45: 77.9 ± 12.7 ODI 23-45: 44.5 ± 9.0*
*p < 0.0001ODI 23-45:
Spondylolisthesis grade: 74.5 ± 11.5*
LL (°): 56.5 ± 9.4*
PT (°): 33.4 ± 8.1*
TK (°): 37.6 ± 7.4
SFHD (°):53.5 ± 10.8*
SFVD (°): 81.1 ± 11.7*
SC7D (°): 41.1 ± 37.4*AUTHOR Approach Fusion levels/ Instrumentation Graft Decompression Reduction 2002_Hanson Posterior: n = 2 Ant/Post: n = 15 (performed in two separate stages, usu. 5 days later) n = 2 none, n = 11 L4-S1, n = 1 L3-S1 + ilium, n = 1 L4-S1 + ilium, n = 1 L5-S1 + ilium, n = 1 T5-sacrum + ilium; Pedicle screws. Fibular dowel graft (allograft n = 11, autograft n = 6) Wide decompression of the L5-S1 root n = 15: Grade 4/3 Pre-Op to Grade 1/3 Post-Op n = 2: no change 2002_Molinari n = 18 Posterior; n = 11 Group 1A Group 1A = L4-sacrum No instrumentation NA Group 1A = No decompression Group 1A = in situ n = 7 Group 1B Group 1B = L4-sacrum Posterior instrumentation NA Group 1B = Posterior decompression Group 1B = 6/7 patients n = 19 Circumferential with anterior support (Group 2) n = 16 separate anterior approach, n = 3 PLIF in lieu of anterior approach Circumferential with anterior structural support; n = 3 Structural graft and posterior fixation Anterior structural graft Group 2 = Posterior decompression Group 2 = 19/19 patients 2005_DeWald n = 10, Ant. interbody cage/ graft n = 9, Post. interbody cage/graft n = 2, Ant. Pedicle screws/graft n = 1 NA, n = 11 L4-S1, n = 5 L5-S1, n = 3 L3-S1, n = 1 L4-L6 Interbody cages/strut graft; Pedicle screws Bone on bone, fibermetal trans-sacral strut, fibular allo-graft trans-sacral strut, autograph cortical iliac trans-sacral strut NA n = 16/21 (14 partial reduction) 2005_Shufflebarger Posterior lumbar interbody fusion n = 18 L5-S1; Harm's cage, posterior monosegmental compression instrumentation with pedicular fixation Autogenous iliac crest graft Gill decompression n = 18 (% slip avg pre-op 77%- > post-op 13%) 2006_Poussa Anterior/ Posterolateral L4-S1 n = 9, L5-S1 n = 2, transpedicular magerl/dick, anterior L5-S1 NA Laminectomy n = 11 (all) Yes Anterior/ Posterolateral without instrumentation L4-S1 n = 7, L5-S1 n = 4, no instrumentation, anterior L5-S1 NA Laminectomy n = 7 NO (some due to interbody grafts) 2006_Helenius Group 1A: Posterolateral in situ n = 4 L5-sacrum, n = 16 L4-sacrum, n = 1 L3-sacrum; No instrumentation Autologous iliac crest bone graft Not performed None Group 1B: Ant intercorporeal fusion, transperitoneal, resected ant/inf edge L5 for access if necessary n = 23 L5-S1 No instrumentation Autologous iliac crest bone graft; wedge interbody grafts From patient's positioning on operating table and wedge-shaped grafts Group 2: Circumferential: anterior/posterolateral, n = 17 one operation, n = 9 staged n = 14 L4-S1, n = 12 L5-S1 No instrumentation Autogenous bone graft None 2006_Vialle Same-day, staged posterior-anterior approach Anterior plate to S1, plates through S1 to iliac wings n = 40 Instrumentation in all patients Posterior: No grafting Anterior: ICBG through anterior plate Posterior decompression and removal of posterior arch of L5 Complete reduction in all patients 2008_Rodriguez-Olaverri Group A: Unilateral TLIF Posterior with transforaminal lumbar interbody implants L4, L5, S1, ilium Rods, screws and two titanium mesh cages Posterolateral: autogenous local graft + allograft L5 nerve root, L5 arch and pars interarticularis decompres Partial reduction via interbody packed titanium cage and hip extension positioning Group B: Transsacral Posterior only Transsacral screws thru L5-S1, pedicle screws L4 Posterolateral: autogenous local graft + allograft L5 nerve root, L5 arch and pars interarticularis decompression Partial reduction via hip extension positioning 2008_Sasso n = 8 Posterior-only, n = 17 Anterior-posterior (paramedian rectus-sparing mini-open retroperitoneal) same-day surgery L4-S1 Pedicle screws Posterior: Fibular allograft Anterior: Fibular strut graft plus femoral ring allograft S1 Gill laminectomy Reduced with patient positioning, no additional attempts at reduction 2009_Hresko n = 21 Posterolateral, n = 5 Posterolateral + anterior discectomy/interbody fusion L4-sacrum n = 13 Jackson intrasacral rods, n = 13 Luque box instrumentation NA Laminectomy and nerve root decompression on case-by-case basis Partial reduction achieved by prone positioning and lumbar lordosis. Achieved 10° reduction in 10% of all patients AUTHOR Approach/Study Groups Radiography, fusion status postop Neuro/clinical deficit Change in clinical evaluation (e.g. ODI, SF-12, others) Complications Clinical Recommendations 2002_Hanson Posterior: n = 2 Ant/Post: n = 15 Posterior: Grade 1 (n = 15), grade 2 (n = 1), no fusion (n = 1) Anterior: Grade 1 (n = 16), broken strut (n = 1). NA Post-op ODI= 11.4, SRS= 37.3, SRS satisfaction= 14.1 1 broken strut graft (in situ anterior only), no neurological deficits, no infection Partial reduction of high-grade isthmic spondylolisthesis with fibular strut grafting is a safe, effective procedure. No difference between allograft and autograft 2002_Molinari Group 1A (n = 11) Group 1A = 45% pseudarthrosis No neurologic deficit in patients treated with in situ; Transient neurologic deficits (n = 4/26); Failed intra-op wake-up test (n = 1) that resolved immediately after releasing the reduction, foot drops (n = 2) and bilateral extensor hallucis longus weakness (n = 1) Pain score: 3/10 Function score: NA Satisfaction score: 8.4/11 36% had progression Anterior structural grafting combined with posterior instrumentation and fusion is effective in achieving fusion in HGS patients. Outcomes for function, pain, and satisfaction are excellent in those patients who obtain solid fusion regardless of the surgical procedure Group 1B (n = 7) Group 1B = 29% pseudarthrosis Pain score: 3.6/10 Function score: 12.6/15 Satisfaction score: 9.4/11 29% instrumentation failure and partial loss of reduction Group 2: Circumferential (n = 19) Group 2 = 0% pseudarthrosis Pain score: 2.5/10 Function score: 13.7/15 Satisfaction score: 9.7/11 11% implant complications and partial loss of reduction 2005_DeWald Ant. interbody cage/graft (n = 10), post. interbody cage/graft (n = 9), anterior pedicle screws/graft (n = 2) 0% pseudarthrosis Hypesthesias or dysesthesias on the dorsum of one or both feet (n = 8); extensor hallus longus weakness (n = 2); cauda equina syndrome (n = 1) Used an unofficial clinical evaluation format: 12 excellent, 7 good, 1 fair, and 1 poor clinical outcome Instrumentation failure (n = 1), Iliac vein thrombosis, pulmonary embolus, pancreatitis, and temporary retrograde ejaculation (n = 1 each) Pediatric patients can be treated successfully by non-instrumented posterior in situ fusion, but instrumentation should be used in adults. Recommends use of adjunctive fixation for adults. 2005_Shufflebarger Posterior lumbar interbody fusion All patients achieved arthrodesis No neurologic complications NA Urinary tract infections (n = 3), ileus (n = 2), cholelithiasis (n = 1), no infectious or instrumentation complications Reducing slip and lumbosacral kyphosis will provide ideal biomechanical environment. Structural anterior column support and posterior transpedicular instrumentation provide more resistance to shear forces than posterior instrumentation alone. 2006_Helenius Posterolateral in situ Nonunion (n = 3)Progression (n = 4) General back pain (BP) (n = 9)BP radiating down leg (n = 5)Neuro deficiencies/ hamstring tightness (n = 14) SRS = 89.7. ODI = 9.7: severely disabled (n = 1), moderately disabled (n = 2)VAS = 22.6 Nonunion (n = 3)Re-operation (n = 1) Circumferential fusion provided significantly better long-term clinical, radiographic, and SRS total score than posterolateral or anterior fusion for HGIS Anterior intercorporeal fusion, trans-peritoneal Progression (n = 1) SRS = 93.2, ODI = 8.9: moderately disabled (n = 4), VAS = 24.1; scored best on SRS self-image Post-op peroneal palsy (n = 1), L5 /S1 radicular pain (n = 3), spondyloptosis (n = 1) Circumferential Nonunion (n = 1) Progression (n = 3) Least lumbosacral kyphosis progression SRS = 100, ODI = 3.0, VAS = 5.5. Scored best on SRS pain and function Nonunion (n = 1), wound infection (n = 1), scoliosis and gait difficulties (n = 1) 2006_Poussa Reduction (n = 11) 18% pseudarthrosis (n = 2) L5 nerve root injury during decompression (n = 1) ODI = 7.2, SRS = 90 Mild muscle atrophy: iliopsoas (n = 7), back L3 (n = 4)/L5 (n = 6); Severe atrophy: back L5 (n = 3) Fusion in situ should be considered as a method of choice in severe L5 isthmic spondylolisthesis In situ (n = 11) All fusions healed appropriately Immediate post-op peroneal palsy 18% (n = 2) ODI = 1.6, SRS = 103.9, better SRS pain and post-op function Mild muscle atrophy: iliopsoas (n = 2), back L3 (n = 2)/L5 (n = 4) Severe atrophy: iliopsoas (n = 1) 2006_Vialle Same-day, staged posterior-anterior approach Fusion achieved in all patients BP (n = 12), BP/bilateral leg pain (n = 11), BP/unilateral leg pain (n = 9), radicular (n = 6), neuro complications (n = 12): L5 incomplete deficit (n = 5), unilateral L incomplete deficit (n = 6), unilateral L5 hypoesthesia (n = 1); 10/12 recovered neurologically within 18months. Beaujon functional score: Pre-op mean 14.2 (5-20); Post-op 20+ in n = 35; 15-19 in n = 5 from BP/leg pain. JOA Pre-op mean 10 (2-15); Post-op 15 in n = 35; 12-14 for n = 5. Intra-op complications: iliac vein lesion and technical difficulty with plate (n = 2). Implant complications: Kyphosis due to plate hitting L4-5 (n = 2), broken screws (n = 2), late infections (n = 5) This technique proved to provide an excellent fusion rate and satisfactory final functional outcomes, but due to the unusually high rate of late infections that may be related to the surgical approach, we do not recommend this technique for HGIS treatment. 2008_Rodriguez-Olaverri Group A: Unilateral TLIF Posterior with transforaminal lumbar interbody implants 100% fusion Back/leg pain resolved in 90%, no neurologic deficits SRS pre-op: pain 4.8, self-image 3.8, fxn 4.8; SRS pos-opt: pain 4.6, self-image 3.6, fxn 4.5 Durotomy (n = 7), infections (n = 3) Both procedure A and B appear to be safe and effective surgically and radiographically, but we must note that the average operation time was longer in procedure A (4.45 hrs) than in procedure B (3.25 hrs) Group B: Transsacral Posterior only Solid fusion in 19/ 20 subjects Back/leg pain resolved in 80%, no neurologic deficits SRS pre-op: pain 4.7, self-image 4.1, fxn 4.7; SRS post-op: pain 4.3, self-image 4.4, fxn 4.3 Durotomy (n = 1), pseudarthrosis (n = 1), implant failure (n = 1) 2008_Sasso Posterior-only (n = 8), Anterior-posterior same-day surgery (n = 17) 100% fusion, no increase in slip grade or angle. No permanent neurologic deficits or deterioration; transient radiculitis 1-month post-op (n = 1) SRS: Extremely or somewhat satisfied (n = 24). Pain: 8.2 pre-op, 3.4 post-op Hardware removal due to prominence after fusion achieved (n = 1); equivalent EBL This technique offers excellent fusion results, good clinical outcomes, and prevents further sagittal translation and lumbosacral kyphosis progression. 2009_Hresko Posterolateral (n = 21), Posterolateral + anterior discectomy/interbody fusion (n = 5) Grade A (definite solid fusion) (n = 22); Grade B (probable solid fusion) (n = 4) NA NA Re-operation (n = 5), loss of L4-L5 motor strength (n = 1), removal prominence (n = 1), revision due to instrument failure (n = 3), transient neurapraxia (n = 6), permanent unilateral L5 weakness (n = 1) No correlation between improvement in pelvic version and amount of reduction. Other factors, such as achievement of solid arthrodesis, may be more important than reduction of spondylolisthesis in determining spinopelvic sagittal balance. 2010_Sansur N = 10,242; No fusion/ decompression (n = 532), combined ant/post (n = 893), ant only (n = 286), post fusion w/o instrument (n = 491), post fusion w/ instrument (n = 4117), TLIF/PLIF (n = 3860) NA The rate of neurological complications was highest in the decompression/no fusion group, but it was not significantly different from other groups (p = 0.10) NA 9.2% complications rate Most common complications = dural tear (2%), infection (2%), neurologic (1.2%), implantrelated (0.7%) Grade level and age but not surgical approach and history of previous surgery significantly correlated with increased complication rates. 2011_Jalanko HGS in children (<12.5 years old for females; <14.5 years old for males) Non-unions but no effect on long-term outcome (n = 5) Posture/gait abnormality (n = 10), SRA positive (n = 14), scoliosis (n = 8) At final follow-up: SRS-24 = 92, ODI = 4.5%, VAS = 9mm Revision due to nonunion (n = 3), Transient L5 paresis (n = 1) Recommend circumferential in situ fusion for high-grade slips; spinal fusion can be carried out at an early age for HGS with good long-term clinical, functional, radiographic and health-related quality-of-life outcomes. HGS in adolescents Non-unions but no effect on long-term outcome (n = 3) Posture/gait abnormality (n = 1), SRA positive (n = 5), scoliosis (n = 4) At final follow-up: SRS-24 = 94, ODI = 8.7%, VAS = 25.1mm Revision due to nonunion (n = 1), S1 root decompression (n = 2), wound infection (n-1) 2012_Kasliwal Pediatric (≤18 years old) NA Nerve root (n = 9), cauda equina (n = 2), lumbar nerve palsy (n = 2), peroneal n. palsy (n = 2) NA 24% of total patients had a complication Osteotomy was the only surgical predictor of neurologic deficit; new neurologic deficit post-op did not correlate to decompression, reduction or revision surgery Adults (>18 years old) NA Nerve root (n = 8), cauda equina (n = 0), lumbar nerve. palsy (n = 1), peroneal nerve. palsy (n = 0) NA 26% of total patients had a complication Baseline strength: HIGH = majority of articles Level I/II LOW = majority of articles Level III/IV Upgrade: Large magnitude of effect and/or dose response gradient Downgrade: Inconsistency of results, indirectness of evidence, imprecision of effect estimates Strength of evidence Conclusion/Comments Baseline Upgrade Downgrade Question 1: What is the effectiveness of the various surgical approaches for HGS? Clinical outcome (Pain, function, etc.) Low Three LOE III and one LOE IV retrospective cohort studies reported good outcomes for function, pain, and satisfaction in patients with solid fusion regardless of the surgical procedure, but circumferential fusion provided the best clinical outcome results. LOW NO NO Radiographic outcome Low One LOE III and two LOE IV retrospective cohort studies reported no difference in fusion rate, but two Level III Evidence and one Level IV Evidence studies reported significantly higher pseudarthrosis rate in posterior-only procedures. LOW NO NO Question 2: What is the effectiveness of additional surgical maneuvers for HGS? Reduction Low Overall, the evidence on the incorporation of reduction is inconsistent. Three LOE III and two LOE IV clinical studies reported negative clinical outcome in partial reduction group with worse ODI and SRS scores but positive radiographic outcome with less pseudarthrosis and deformity progression on reduction of slip angle and slip grade. One LOE IV study reported full reduction in 95% of patients undergoing complete reduction but had high complication rate. For children and adolescents, in situ fusion with long-term follow-up is recommended. LOW NO NO Instrumentation Low No studies used instrumentation as the sole primary variable. Most studies included instrumentation with varying surgical approaches or other additional surgical maneuvers such as reduction. Use of instrumentation is dependent on surgical approach and surgeon preference. Luque box, Jackson intrasacral rod and double-plate technique are not recommended. LOW NO NO Decompression Insufficient There is no study directly examining decompression as an independent variable. Three Level III Evidence studies performing in situ fusion without decompression reported good clinical and radiographic outcome. Higher-level studies reporting on decompression are necessary for a definitive conclusion. LOW NO NO Question 3: What is the comparative safety of the various surgical approaches for HGS? Circumferential vs. Posterior-only vs. Anterior-only Low Three Level III Evidence and one Level IV Evidence retrospective cohort studies report no long-term difference in complications. Operation time and hospital stay was slightly higher in circumferential procedures. One Level IV Evidence retrospective study reported higher operative blood loss in PLIF compared to ALIF, but outcomes were similar. LOW NO NO Question 4: Who is at risk for progression to higher grade spondylolisthesis? Pelvic Incidence HIGH Two Level II Evidence studies indicated no correlation between higher PI and progression. HIGH NO NO Sacral slope HIGH Two Level II Evidence studies indicated no correlation between higher SS and progression. They reported that higher PI controls have high PT and SS and that SS may be predictive of reducibility. HIGH NO NO Age and grade of spondylolisthesis HIGH One Level II Evidence study indicated positive correlation between higher PI, age and grade of spondylolisthesis but not of progression. HIGH NO NO
In this issue




{kind=link}
{kind=link}
{kind=link}