


Abstract
Background Minimally invasive spine surgery (MIS) has revolutionized fixation of thoracolumbar fractures with burst elements. Recent studies have proven that percutaneous pedicle screw instrumentation is as effective as open instrumentation but with reduced intraoperative blood loss and operative duration. Techniques such as short-segment pedicle screw fixation including the fractured vertebra have shown satisfactory radiological correction and functional outcomes, avoiding the need for extensile posterior constructs.
Objective In the present study, the authors our technique utilizing unipedicular index vertebra fixation and manipulation in MIS for thoracolumbar fractures with burst elements. To our knowledge, this technique is not well described in literature as open approaches are often adopted for the above. The authors sought to highlight the 2-year radiological and functional outcomes of 20 consecutive patients who underwent this technique.
Methods A retrospective review of prospectively collected data was conducted on 20 patients with thoracolumbar fractures with burst elements who underwent fixation using our technique. Patient data collected included demographic characteristics, mechanism of injury, associated injuries, neurological deficit at the time of admission, pre- and postoperative neurological evaluation, and length of hospital stay. Radiological investigations included plain radiographs, computed tomography of the spine with reconstruction, and magnetic resonance imaging of the spine, which provided data for radiological fracture classifications such as AO Spine and derivation of Thoracolumbar Injury Classification and Severity Score, as well as preoperative planning. Radiological investigations in the postoperative period were carried out by standing radiographs or EOS whole spine at each postoperative follow-up for up to 2 years. Radiological parameters—vertebral wedge angle, regional kyphosis angle, coronal Cobb angle, and anterior and posterior vertebral body heights—were recorded at preoperative, intraoperative, postoperative, and up to 2-year follow-up. Clinical outcome scores (visual analog score [VAS] and Oswestry Disability Index [ODI]) were also recorded at similar timepoints.
Results Radiological outcomes reflect significant lordotic corrections of the vertebral wedge angles up to 2-year follow-up when compared with preoperative values (intraoperative: P = 0.06; postoperative: P = 0.001; 3 months: P = 0.002; 6 months: P = 0.004; 1 year: P = 0.011; 2 years: P = 0.016). Additionally, significant lordotic corrections of regional kyphosis angles (intraoperative: P = 0.00; postoperative: P = 0.00; 3 months: P = 0.031; 6 months: P = 0.039) and increases in anterior vertebral body heights (postoperative: P = 0.001; 3 months: P = 0.010; 6 months: P = 0.020) at up to 6-month follow-up were found. Preoperatively, median VAS of 85 (range 30–100) and ODI of 90 (range 40–98) were recorded. Statistically significant improvements in VAS and ODI were found across all timepoints when compared with preoperative values, with a mean VAS of 11.5 (SD 4.8) and ODI of 9.9 (SD 4.5) at 2-year follow-up.
Conclusion Surgical management of thoracolumbar fractures with or without neurological deficit has a role in reducing nursing requirements and postoperative morbidity in patients with polytrauma and other associated injuries. Our approach in treating thoracolumbar fractures with burst elements using MIS short-segment fixation and unipedicular screw manipulation technique shows satisfactory radiological correction and high rates of fracture union while reducing approach-related morbidity and improving functional outcomes.
Level of Evidence 3.
- thoracolumbar
- burst fracture
- flexion-distraction, indirect reduction
- minimally invasive surgery
- short-segment instrumentation
Introduction
Vertebral burst fractures result from vertical compression trauma across the anterior and middle columns with disruption of the posterior vertebral body cortex with or without retropulsion.1 High energy flexion distraction vertebral fractures are characterized by osseous and/or ligamentous posterior ligamentous complex injuries.2 These fractures are usually associated with disruption of the posterior vertebral body cortex with or without retropulsion and are likely to be unstable. Furthermore, most flexion-distraction injuries are associated with burst elements of the superior aspect of the vertebral body. The above-mentioned injuries account for the majority of the thoracolumbar fractures involving burst elements. These fracture types are described in most classifications, including Denis and AO classification,2 as well as the Thoracolumbar Injury Classification and Severity Score (TLICS)3 for thoracolumbar fractures.
Surgical intervention for thoracolumbar fractures involving burst elements is indicated in patients to (1) prevent neurological deterioration, (2) allow early mobilization in the setting of polytrauma, and (3) prevent potential risk of deformity progression.4,5 Minimally invasive surgery (MIS) of the spine has revolutionized fixation of thoracolumbar fractures with burst elements.6 Recent studies have proven that percutaneous pedicle screw instrumentation is as effective as open instrumentation, with reported reduction in intraoperative blood loss and operative duration.7,8 Moreover, techniques such as short-segment pedicle screw fixation with intermediate screws at the fractured level have shown satisfactory biomechanical stability, radiological correction, and functional outcomes, thus avoiding the need for extensile posterior constructs or anterior reconstruction.9 However, there is still a paucity of studies that delve into the effectiveness of treating burst fractures with short-segment pedicle screw fixation with intermediate unipedicular screw at the fractured level—either through open or MIS approaches.
In the present study, we aimed to describe our technique utilizing MIS short-segment unipedicular screw fixation and manipulation of the index vertebra. To our knowledge, this is the first such described MIS short-segment fixation technique with biomechanical description to achieve fracture reduction and alignment. In addition, we aimed to highlight the 2-year radiological and functional outcomes of 20 consecutive patients who underwent the said technique of fracture fixation.
Methods
All patients who underwent surgery for single-level thoracolumbar fractures with burst elements at our tertiary spine and level 1 trauma center between May 2013 and May 2019 were analyzed for prospectively collected data. Institutional review board approval (DSRB ref: 2021/00687) was obtained prior to data collection and analysis. A waiver of informed consent was granted due to the anonymization protocols and retrospective nature of the data. Inclusion and exclusion criteria for both our technique and study can be found in Table 1.
Inclusion and exclusion criteria.
Patient data collected included demographic characteristics, mechanism of injury, associated injuries, neurological deficit at time of admission with pre- and postoperative neurological evaluation, and length of hospital stay. Radiological investigations included plain radiographs, computed tomography (CT) of the spine with reconstruction, and magnetic resonance imaging of the spine, which provided data for radiological fracture classifications such as AO Spine and derivation of TLICS, as well as preoperative planning. Radiological investigations in the postoperative period were carried out by standing radiographs or EOS whole spine at each postoperative follow-up for up to 2 years. These investigations provided data for radiological parameters, namely vertebral wedge angle, regional kyphosis angle, coronal Cobb angle, and anterior and posterior vertebral body height (Figure 1A). Additionally, CT images at the last follow-up were evaluated for Hounsfield units (HU) at the fractured vertebral level—calculated by an integrated software that measures HU at the midbody’s elliptical region of interest and avoids areas of attenuation (eg, posterior venous plexus and focal heterogeneity). The evidence of fracture healing was obtained from relevant postoperative radiographs and CT of the spine, which was conducted from 3 to 9 months. Operative parameters recorded were time to operating theatre, instrumented levels, operative duration, and intraoperative blood loss and transfusion. Clinical outcome indicators evaluated were the American Spinal Injury Association Impairment Scale (ASIA), visual analog score (VAS), and Oswestry Disability Index (ODI). Any postoperative complications including implant failure were documented.

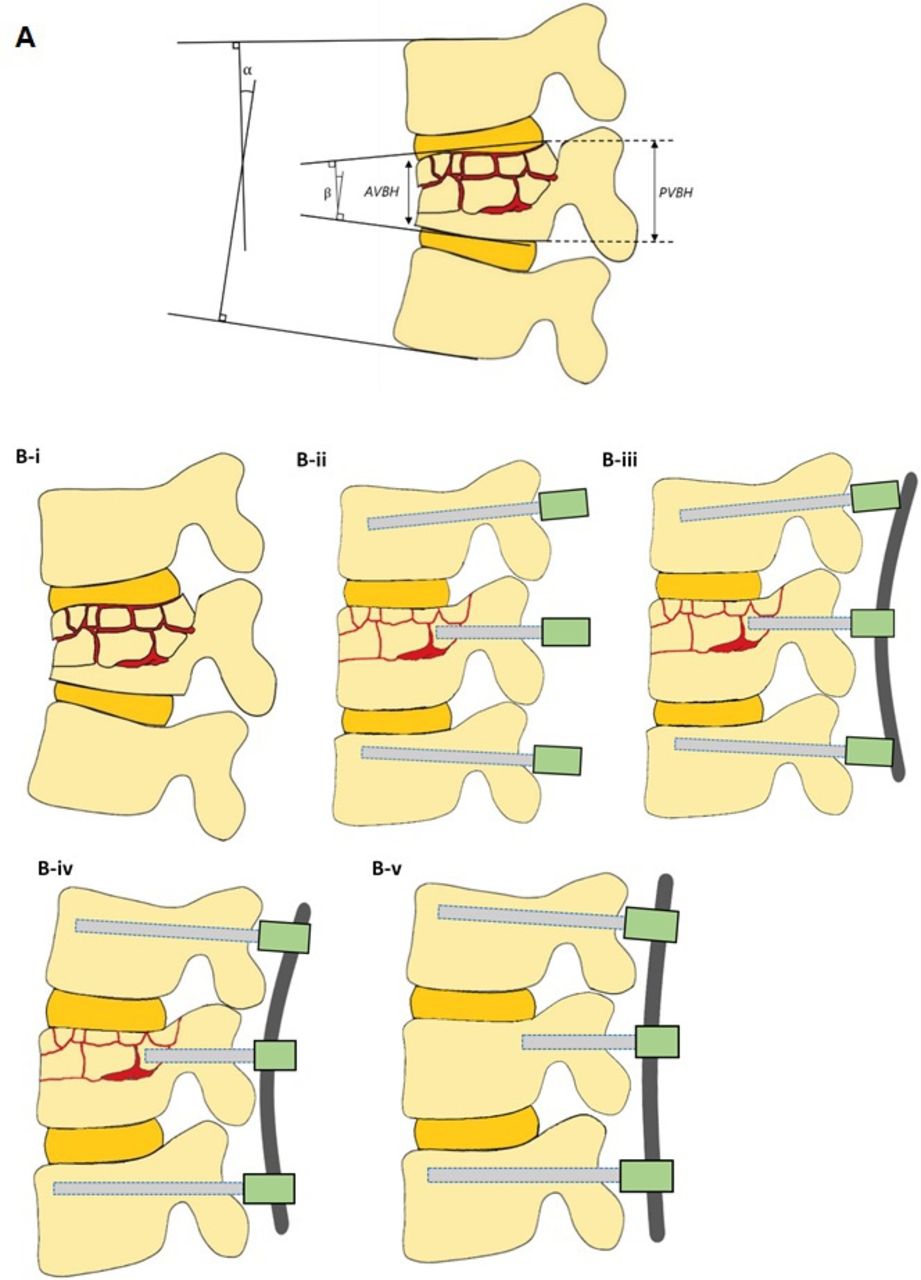
(A) Pictorial representation of radiological parameters—vertebral wedge angle vs regional kyphosis angle. (B) Graphical representation of short-segment minimally invasive surgery fixation of thoracolumbar fractures with burst elements highlighting procedural nuances A: α, regional kyphosis angle; β, vertebral wedge angle; AVBH, anterior vertebral body height; and PVBH, posterior vertebral body height. B-i: Thoracolumbar fracture with burst elements. B-ii: Placement of bilateral pedicle screws into adjacent vertebrae, with one shorter pedicle screw inserted proud into fractured vertebra. B-iii: Fixation of contoured convex rod on intermediate short pedicle screw. B-iv: Fixation of contoured convex rod on screws in the adjacent vertebrae. B-v: Postoperative healed fracture maintaining correction.
Surgical Technique
All patients underwent the novel surgical technique as described (Figure 1B). All included patients were operated under general anesthesia with neuromonitoring. We positioned patients on a standard Jackson table (MizuhoOsi, Union City, California, USA; an operating table with jelly bolsters under the chest and iliac crest would suffice as well) to help in postural correction of the kyphus at the fracture level. This usually results in partial correction of the deformity, which was noted down from biplanar image intensifier images. MIS instrumentation was then performed using standard percutaneous pedicle screw systems under image guidance (REVERE Stabilization system by Globus or EVEREST MIS system by K2M). Alternatively, a navigation system (O-arm with guides) can also be utilized. Pedicle screws were first inserted at the level cephalad to the fractured vertebra and were directed inferiorly and medially in the vertebral body, entailing the entry point to be placed at a superior lateral aspect of the pedicle (Figure 2B). Next, 2 pedicle screws were inserted at the level caudad to the fractured vertebra, which were directed superiorly and medially in the vertebral body; the entry point was thus to be placed at inferior lateral aspect of the pedicle (Figure 2B). The aforementioned four screws were positioned such that their tulip heads were flushed to the facet capsule. In most of our cases, we observed that a larger burst fragment was in continuity with one of the pedicles of the fractured vertebra. Thus, the final unipedicular screw was inserted at the fractured vertebra such that it engaged the larger burst fragment. This screw was shorter in length, reaching only the posterior third to middle of the vertebral body, and it was kept proud (usually 1–4 screw threads). The prominence of this screw was directly proportional to the vertebral wedge angle.

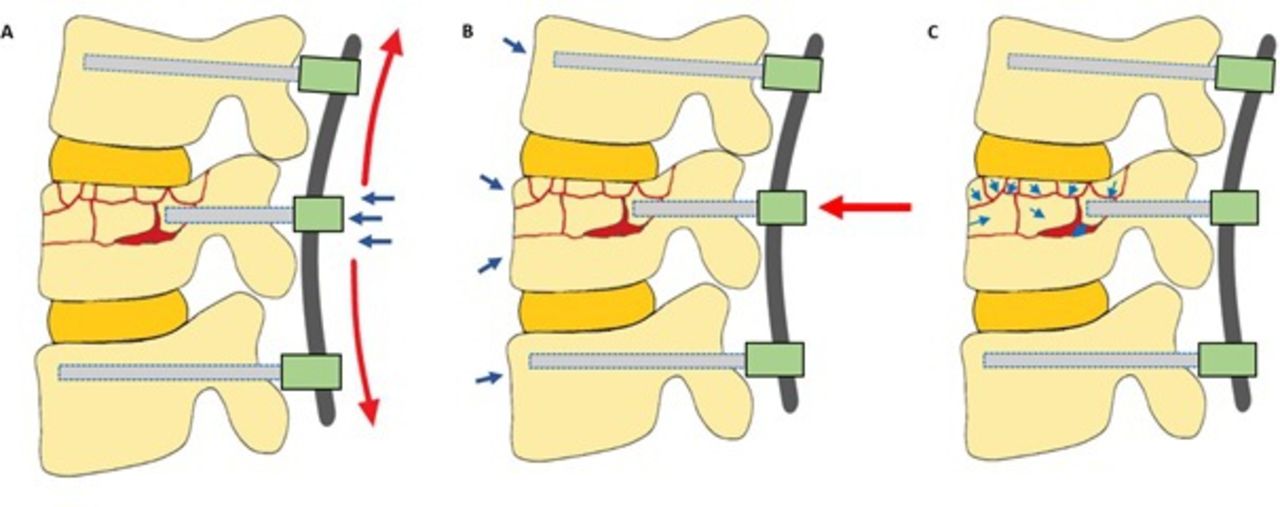
Force diagram of pedicle screw-rod construct implanted with our technique. (A) Increased sagittal and anterior directed forces as a result of concave rod with shorter, proud intermediate pedicle screw placement. (B) Anterior directed forces from screw-rod construct with reactive posterior directed forces from anterior ligamentous complex and periosteal sleeve, reducing the burst fragments and intact bone close. (C) Interfragmentary motions of burst fragments.
After pedicle screw insertion, contoured convex rods of appropriate length were passed through the tulips using the MIS technique. The locking nut was first applied at the fracture vertebra level to hold the rod in the correct alignment (Figure 2C). Next, locking nuts were applied concurrently on the cephalad level followed by the caudad level (Figure 2D). The kyphosis correction was subsequently measured off image intensifier radiographs. While we did not encounter any worsening of neuromonitoring signals, we recommend direct decompression by doing MIS laminotomy or laminectomy should there be a drop in neuromonitoring signals (especially in worsening of motor evoked potential).
Postoperatively, patients were recommended to mobilize immediately as dictated by pain and other associated injuries. Standard postoperative analgesia and rehabilitation were prescribed, and all patients were fitted with a custom-made thoracolumbosacral orthosis, which they work for a minimum of 6 weeks to ensure construct stability. Patients were discharged once fit, taking into account other injuries comanaged by other specialties. The complete course of a typical patient’s correction of the fracture vertebra is highlighted in Figure 3.

Pre-, intra-, and post-operative radiographs of a patient with flexion distraction injury with burst elements. (A) Preoperative computed tomography (CT), sagittal view. (B) Intraoperative correction sagittal radiograph. (C) Immediate postoperative CT sagittal and coronal views. (D) 6-month follow-up anteroposterior and lateral views. (E) 2-year follow-up anteroposterior and lateral views.
Statistical Analysis
Statistical analysis was performed with the use of SPSS statistical software (version 2022; IBM). Patients’ demographic and clinical characteristics were analyzed descriptively. Numerical variables were summarized by mean (SD) or median (min – max), whichever was more appropriate, whereas categorical variables were summarized by frequencies including number and percentage of the patients in each group. Intra- and post-operative outcomes were compared with preoperative measurements by using Wilcoxon sign rank test.
Results
Baseline Characteristics
A total of 20 patients (mean age 34.5 years) comprising 14 men and 6 women with thoracolumbar fractures with burst elements who underwent MIS short-segment fixation were included in the present study (Table 2). Mechanism of injuries was primarily fall from height (n = 17) or motor-vehicular accidents (n = 3). Based on the ASIA neurological grading system, 8 patients (40%) and 12 patients (60%) were ASIA grade E and D, respectively. Mean time to admission was 4.7 hours, with mean time to operating room recorded as 69.5 hours. Patients were followed up for a minimum of 2 years. In total, 17 patients (85%) suffered associated injuries aside from thoracolumbar fractures owing to polytrauma.
Individual clinical characteristics.
Operative Details and Complications
The mean operative duration was 108.6 minutes, with a median intraoperative blood loss of 55 mL (range 10–1300 mL; Table 3). No patients suffered iatrogenic neurological deficits or infection. No intraoperative complication was noted. The median length of hospital stay was 11.5 days. One case of implant failure was noted, with implant cutout of the L1 vertebra superior endplate at 3 months postoperatively with no neurological sequelae.
Baseline characteristics.
Radiological Outcomes
Radiological assessment of the sagittal plane revealed a preoperative median vertebral wedge angle of 16.8° (range −12.2°–30.0°) at the fractured level, with a statistically significant lordotic correction to 5.0° (range −3.2°–18.0°) intraoperatively during prone positioning (Table 4). While slight deterioration in lordotic correction of the fractured vertebra was noted between he immediate postoperative period to 3-month follow-up (from median vertebral wedge angle of 1.8°–5.4°), the wedge angle did not deteriorate further from 3-month follow-up onward. Moreover, median vertebral wedge angles were all significantly more lordotic compared with preoperative values at up to 2-year follow-up.
Radiological outcomes and clinical outcomes.
The preoperative median regional kyphosis angle was 10.2° (range −27.9°–28.6°). Statistically significant lordotic correction was reflected during intraoperative prone-positioning, at the immediate postoperative period, and at 3- and 6-month follow-up (Table 5). Assessment of coronal Cobb angles of adjacent vertebrae reflected a nonstatistically significant improvement from the preoperative period up to the 2-year follow-up at various timepoints. Statistically significant increases in anterior vertebral body height at the fractured level were recorded at up to 6-month follow-up, whereas posterior vertebral body heights remained stable with no significant changes from the preoperative period up to 2-year follow-up. Fracture healing was radiologically appreciable across all patients by 6-month follow-up. At final follow-up, the mean CT HU of included patients’ mid-vertebral body at the fractured level was 270.3 (SD 44.3).
Comparison of radiological and clinical outcomes to preoperative values.b
Clinical Outcomes
Preoperative median VAS was 85 (range 30–100) and ODI was 90 (range 40–98) (Table 4). Statistically significant improvements in VAS and ODI were found across all timepoints when compared with preoperative values, with a mean VAS of 11.5 (SD 4.8) and ODI of 9.9 (SD 4.5) at 2-year follow-up (Table 5).
Discussion
Thoracolumbar fractures with burst elements result from axial compression with loss of vertebral height and increase in vertebral kyphus angle, with or without posterior ligamentous complex (PLC) injury and neurological deficits.10 In patients with significant wedge kyphosis, severe canal compromise and loss of anterior vertebral body height may warrant direct decompression and anterior vertebral reconstruction.11 A total of 9 patients sustained flexion-distraction injuries with PLC disruption and burst elements, causing thecal compression, which was adequately reduced and indirectly decompressed. Surgical management of thoracolumbar fractures with or without neurological deficit has a role in reducing nursing requirements and postoperative morbidity in patients with polytrauma and other associated injuries.7,12 In our series, a total of 17 patients had associated injuries aside from the spine; these injuries were managed surgically and had good postoperative recovery.
Thoracolumbar burst fractures with kyphus angle ≤25° with no or mild to moderate neurological deficit can be treated via our MIS short-segment unipedicular fixation technique—whereby a moderate degree of kyphus angle can be sufficiently corrected through prone positioning and intraoperative rod fixation. Treatment of thoracolumbar burst fractures with MIS short-segment fixation techniques has been described in the literature, often with percutaneous insertion of 2 pedicle screws at the fractured vertebral level and adjacent vertebral levels above and below.13–15 While studies have reported promising radiological and clinical outcomes,4,16 from our experiences, insertion of a single pedicle screw at the burst fracture level is preferred due to a major bony fragment attached to one intact pedicle, with the other pedicle often discontinuous with smaller burst fragments—whereby instrumentation should be avoided. Bilateral insertion of pedicle screws at the fracture level should be considered only when both pedicles are attached to major bony fragments so as to avoid unnecessary soft tissue dissection and disruption of posterior elements.
Biomechanical Instrumented Correction
In the present study, radiological outcomes reflect significant lordotic corrections of the vertebral wedge angles up to 2-year follow-up when compared with preoperative values. Additionally, significant lordotic corrections of regional kyphosis angles and increases in anterior vertebral body heights up to 6-month follow-up were found. These findings are indicative of how the described surgical technique leverages the benefits of biomechanical instrumented correction with the principle of biological osteosynthesis. With the pedicle screw-rod construct arrangement, restoration of near-normal height of the burst vertebra with enhanced lordotic correction was achieved through sagittally and anteriorly directed forces (Figure 2A). This also reduced the stretch of the PLC sustained during flexion-distraction injuries, thus mitigating soft tissue trauma. Furthermore, the shorter pedicle screw, which was inserted proud at the fracture level, allowed for a larger, anteriorly directed force with resultant posteriorly directed forces from anterior ligamentous complex and periosteal sleeve to achieve indirect fracture reduction. This is akin to the concept of primary fixation by using instrumentation to bridge fracture fragments together with intact bone17 (Figure 2B). These forces, coupled with insertion of 1 shorter pedicle screw at the fractured vertebral level, allowed for increased interfragmentary motion with improved secondary bone healing17 (Figure 2C). Appropriate rigidity for fracture healing is accomplished via the screw-rod construct and postoperative bracing. Our technique was found to be effective with evidence of fracture healing across all patients at 6-month follow-up, with satisfactory mean HU of 270 at final follow-up, indicating good bone mineral density and healing. One patient who was found to be noncompliant in postoperative bracing experienced pedicle screw cutout of the L1 endplate without neurological deficits, the sole construct failure from the present study, with an HU of 201.18
Biological Osteosynthesis
The aforementioned biomechanically driven benefits are further augmented by our novel technique following the principle of biological osteosynthesis, entailing maximal preservation of vasculature with minimal dissection of soft tissue.19 This is reflected with no intraoperative complications, no postoperative infections, and evidence of significant improvements in functional outcomes and pain scores (VAS and ODI) compared with preoperative values. In our study, no rod or screw breakages were encountered up to 2-year follow-up despite anterior column injury, suggesting that our technique allows for optimization of the body’s own bone-healing potential.17 The use of MIS technique coupled with insertion of only 1 shorter pedicle screw at the fracture level reduces tissue dissection and approach-related morbidity compared with more conventional open techniques and/or insertion of 2 bilateral pedicle screws of standard length at the fracture level, evident with our reported median intraoperative blood loss of 55 mL. Intraoperative neuromonitoring also did not reveal any worsening of signals across all patients, most likely due to (1) increase in canal space attributed to indirect reduction from intraoperative positioning, (2) indirect decompression of thecal elements by anterior translation of burst fragments through short-screw instrumentation at the index level, and (3) minimal soft tissue dissection. However, we recommend consideration of direct decompression via MIS laminotomy or laminectomy should intraoperative neuromonitoring reflect worsening signals.
Limitations
In view of the small number of included patients in the present study, studies with a larger population and longer follow-up duration should be conducted to validate the outcomes and feasibility of this technique. We also suggest biomechanical studies to further substantiate our clinical findings as described to further fortify the proof of concept for this novel technique.
Conclusion
Our approach in treating thoracolumbar fractures with burst elements with MIS short-segment fixation and novel screw placement with manipulation shows promising outcomes. This technique has achieved satisfactory radiological correction and high rates of fracture union whilst reducing approach-related morbidity and improving functional outcomes.
Acknowledgments
We would like to acknowledge Sridharan Alathur Ramakrishnan and Ms. Laranya Kumar for their help in data collection and manuscript editing.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.