


Article Figures & Data
Figures
- Figure 1
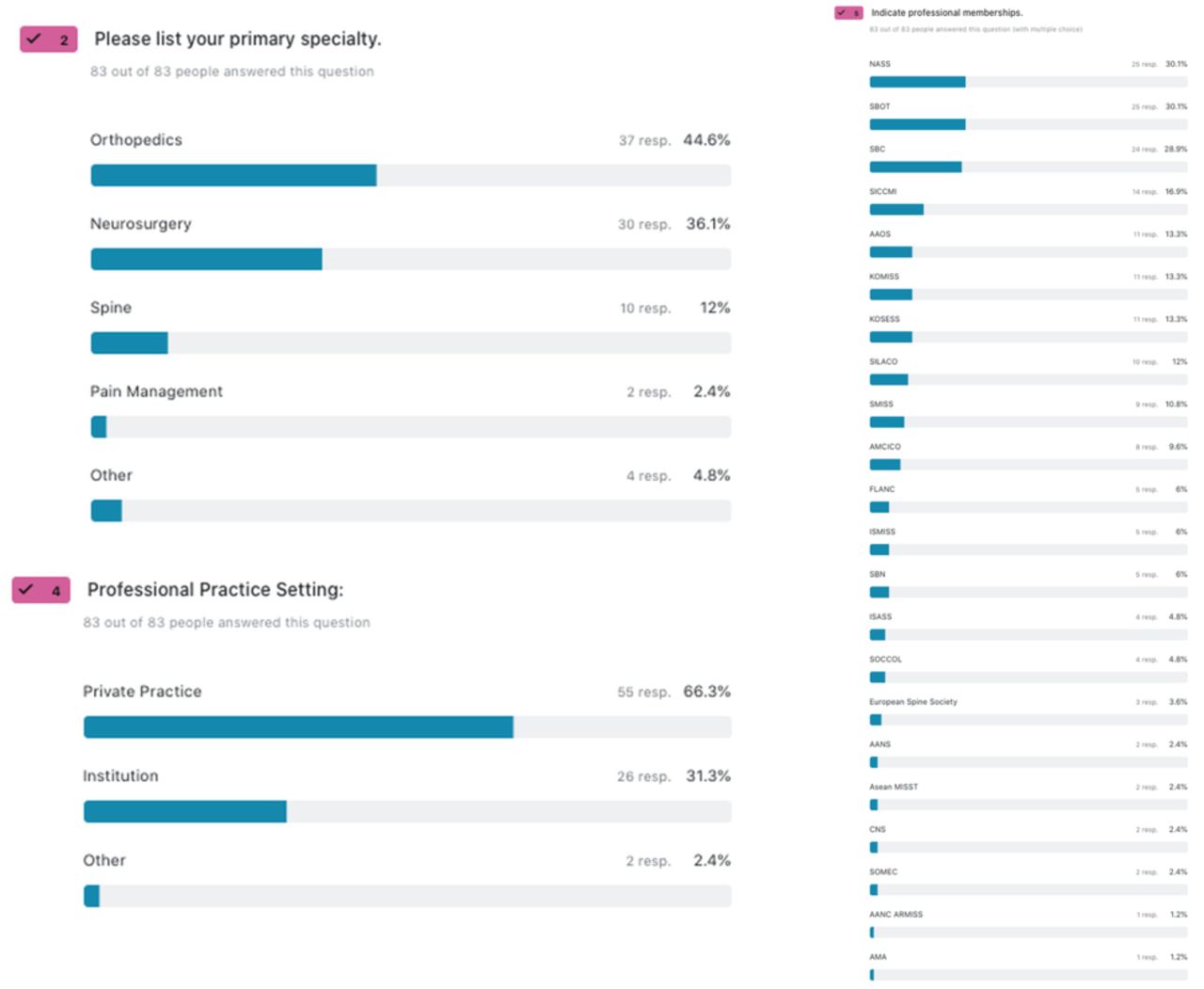
The majority of responding surgeons were orthopedists (44.6%), followed by neurosurgeons (36.1%) and designated spine specialists (12.0%). Only 2.4% of respondents were pain management physicians. Most respondents were in private practice (66.3%), and 31.3% practiced in institutions. The represented respondents’ societies in decreasing order (considering multiple memberships per respondent) were as follows: NASS, North American Spine Society (30.1%); Brazilian Society of Orthopedics and Traumatology (SBOT, Sociedade Brasiliera de Ortopedia y Traumatologia; 30.1%); Brazilian Spine Society (SBC, Sociedade Brasiliera de Columna; 28.9%); Interamerican Society for Minimally Invasive Spinal Surgery (SICCMI, Sociedad Interamericana De Cirugia De Columna Minimamente Invasiva; 16.9%); AAOS, American Academy of Orthopedic Surgeons (13.3%); KOMISS, Korean Minimally Invasive Spine Society (13.3%); KOSESS Korean Endoscopic Spinal Surgery Society (13.3%); SILACO, Sociedad Iberolatinoamericana de Columna (12.0%); SMISS, Society For Minimally Invasive Spine Surgery (10.8%); Mexican Spine Society (AMCICO, Asociación Mexicana de Cirujanos de Columna, A. C.; 9.6%); Latin American Federation of Neurosurgical Societies (FLANC, Federacion Latinoamericana de Sociedades De Neurocirurgia; 6.0%); Brazilian Neurosurgery Society (SBN, Sociedade Brasiliera de Neurocirurgia; 6.0%); ISASS, International Society For The Advancement Of Spine Surgery (4.8%); Colombian Spine Society (Sociedad Colombiana de Cirurgia, SOCCOL; 4.8%); European Spine Society (3.6%); AANS, American Association of Neurological Surgeons (2.4%); Asean MISST (2.4%); CNS, Congress of Neurological Surgeons (2.4%); Mexican Endoscopic Spine Surgery Society (SOMEC, Sociedad Mexicana de Endoscopia de Columna; 2.4%); AMA, American Medical Assocition (1.2%); and German Spine Society (DWG, Deutsche Wirbelsäulengesellschaft; 1.2%).
- Figure 2
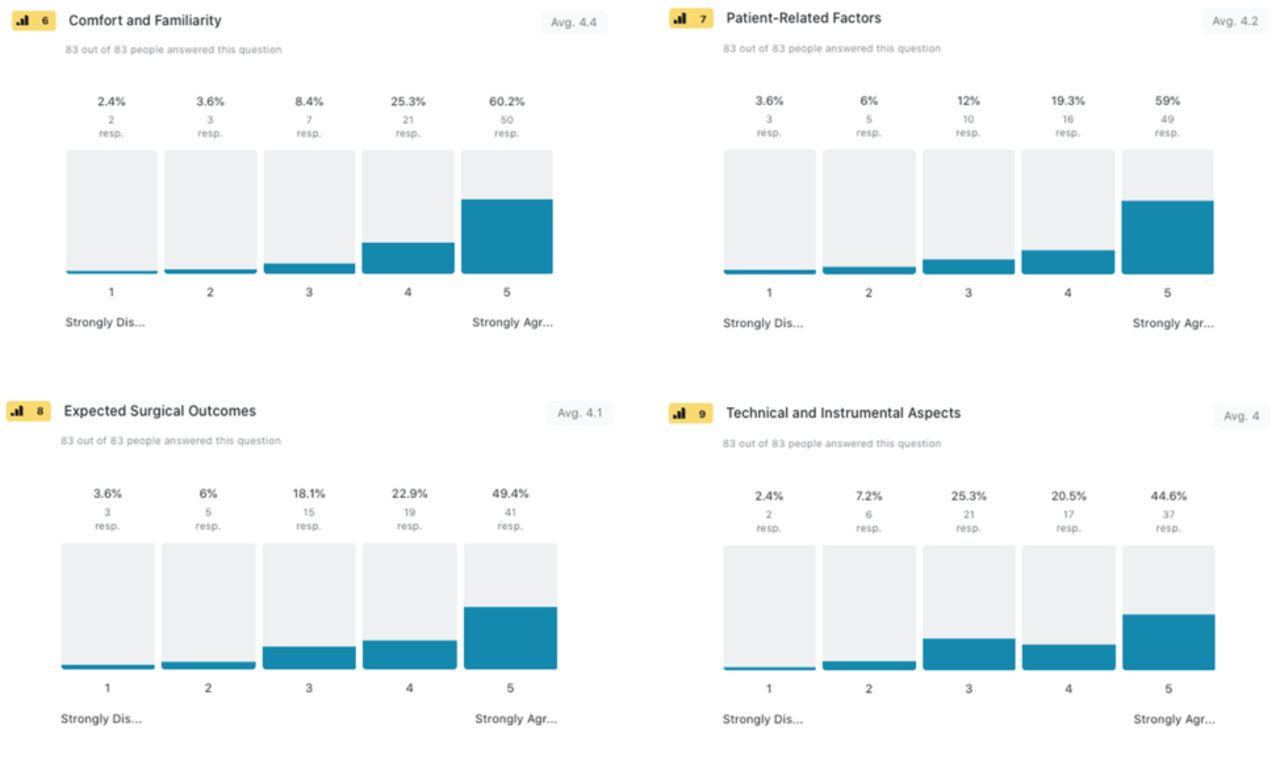
Descriptive statistics showed comfort level and procedural familiarity (60.2%) and patient-related factors (59.0%) being the most influential factors when choosing a lumbar endoscopic decompression procedure. Secondary components of surgical decision-making were expected surgical outcomes (49.4%) and technical and instrumental aspects (44.6%).
- Figure 3
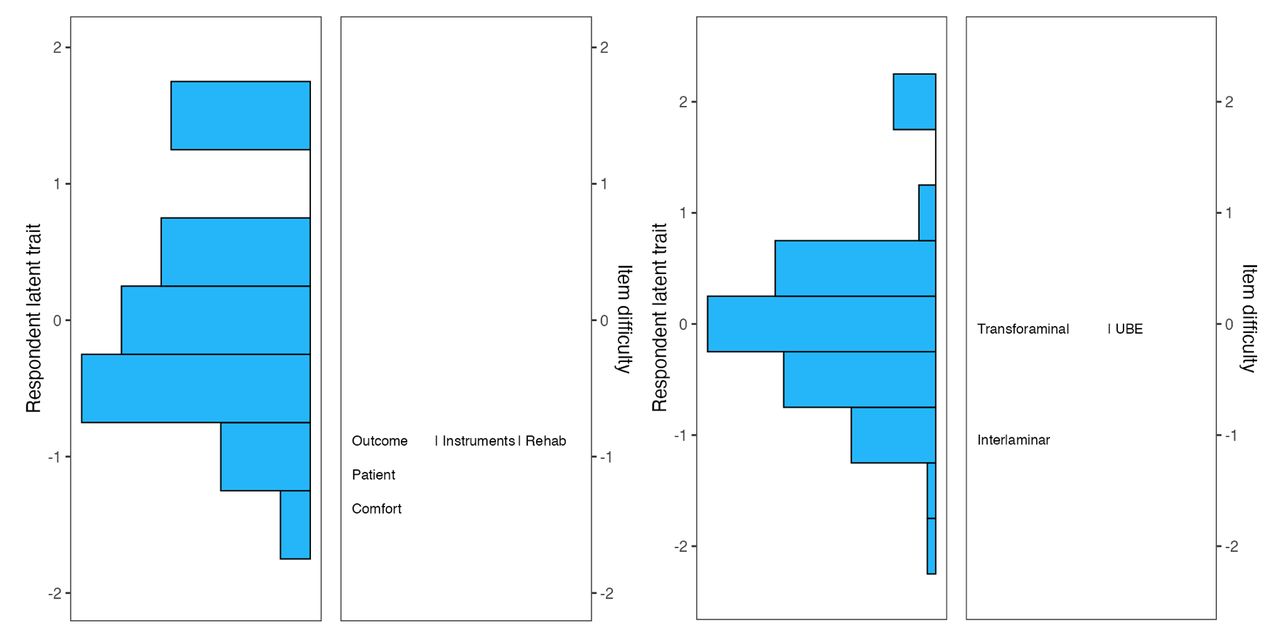
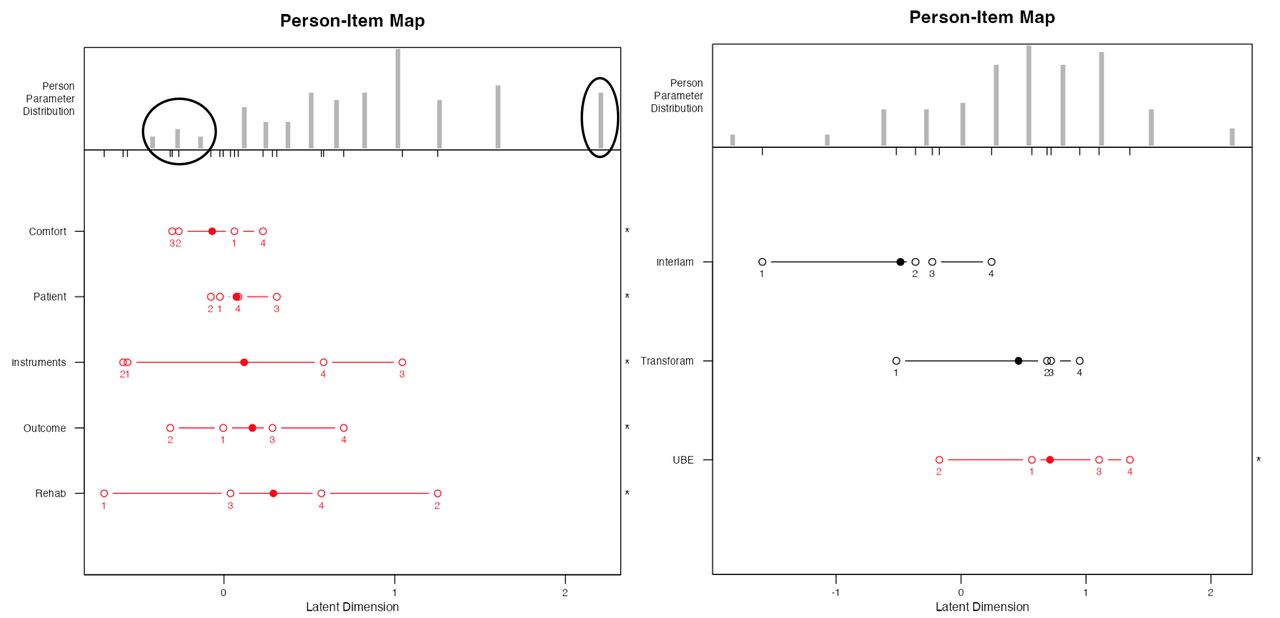
The item response theory polytomous Rasch partial agreement analysis was employed to assess spine surgeons’ level of endorsement of 6 test items (patient outcomes, comfort with the procedure, instruments, patient factors, rehabilitation, and preferred lumbar endoscopic stenosis decompression technique) regarding the endoscopic lumbar decompression surgery (Table 1). Shown is the resulting Wright plot. On the left, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability. The surgeons represented by horizontal bars at the top indicated a higher level of endorsement for the individual test components of endoscopic spinal surgery (positive logits) than those on the bottom (negative logits). On the right, the higher-level endorsement harder to agree on items are listed at the top vs the easier to agree ones on the bottom. There was an assessment gap at the top of the Wright plot and redundancy between test items such as patient outcomes, technical aspects and instruments, patient rehabilitation considerations, and transforaminal and unilateral biportal (UBE) technique, illustrating the need for a more granular assessment of surgeons’ decisions by refining the test.
- Figure 4
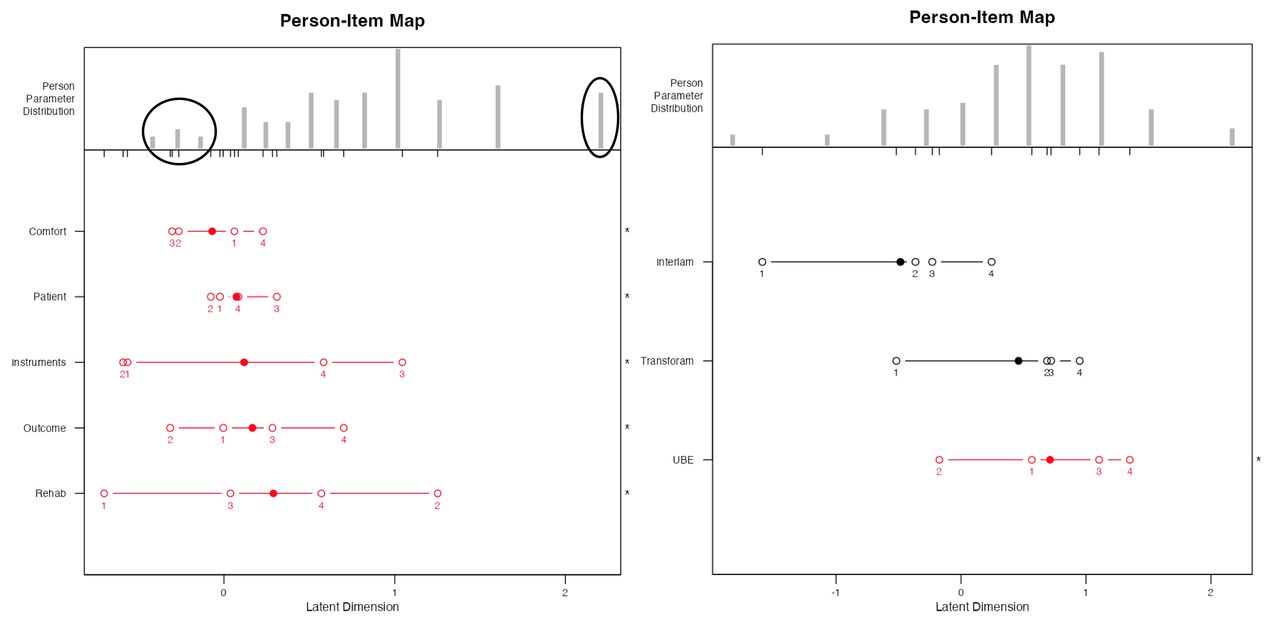
The person-item maps show the logarithmically transformed person and item positions on a unified continuum using the logit measurement unit, transitioning ordinal data to equal-interval data. This method charts both person and item positions (in logits) along the x axis. Within Rasch modeling, these values are labeled as “locations” rather than “scores.” A surgeon’s logit location indicates their natural log odds of agreement with a series of items. Individuals with pronounced adherence to the considered attitude affirm items favorably, positioning them further to the right on the scale. The solid dots indicate the mean person location scores. The items “comfort level with the endoscopic procedure,” “patient-related factors,” “interlaminar,” and “transforaminal technique” were easier to agree on (Tables 1 and 2). These items also had the smallest spread of logit locations. The more challenging items to agree on were “clinical outcomes,” “postoperative rehabilitation,” and “unilateral biportal (UBE).” Contrary to the descriptive statistical analysis (Figure 5), the mean logit location (items more shifted to the right of the plot) showed more intense partial agreement for the transforaminal rather than the interlaminar technique being the best lumbar endoscopic stenosis decompression procedure. In comparison, the items testing the importance of endoscopic instruments, clinical outcomes, rehabilitation, and the relevance of UBE had a wider spread of logit locations. The person-item maps also illustrate that items were reasonably well distributed. However, some surgeons could not be measured as reliably as the majority by this set of items, indicating the test items were either too intense or not intense enough for them. The black circles highlight these areas. The analysis also showed disordered thresholds of endorsement for the 5 test items shown in the left plot and UBE (right-sided plot), suggesting that surgeons had difficulty consistently discriminating between response categories ranging from strongly disagree (1), disagree (2), agree (3), to strongly agree (4)—a problem observed when there are too many response options (all disordered items shown in red). Examining the order and location of these test items revealed an uneven distribution of the ranked order of item difficulties or intensities along the logit continuum. The authors considered collapsing adjacent item categories for these 6 items where the problem occurred. However, they refrained from doing so to expose the wide variety of item difficulties or intensities as they may illustrate the true complexity of the thought process of surgical decision-making. In comparison, the logits for item categories regarding transforaminal and interlaminar technique were ordered (all ordered items shown in black), suggesting a good fit to the Rasch model without any statistically significant difference between the observed values and the values predicted by the model (Table 2).
- Figure 5
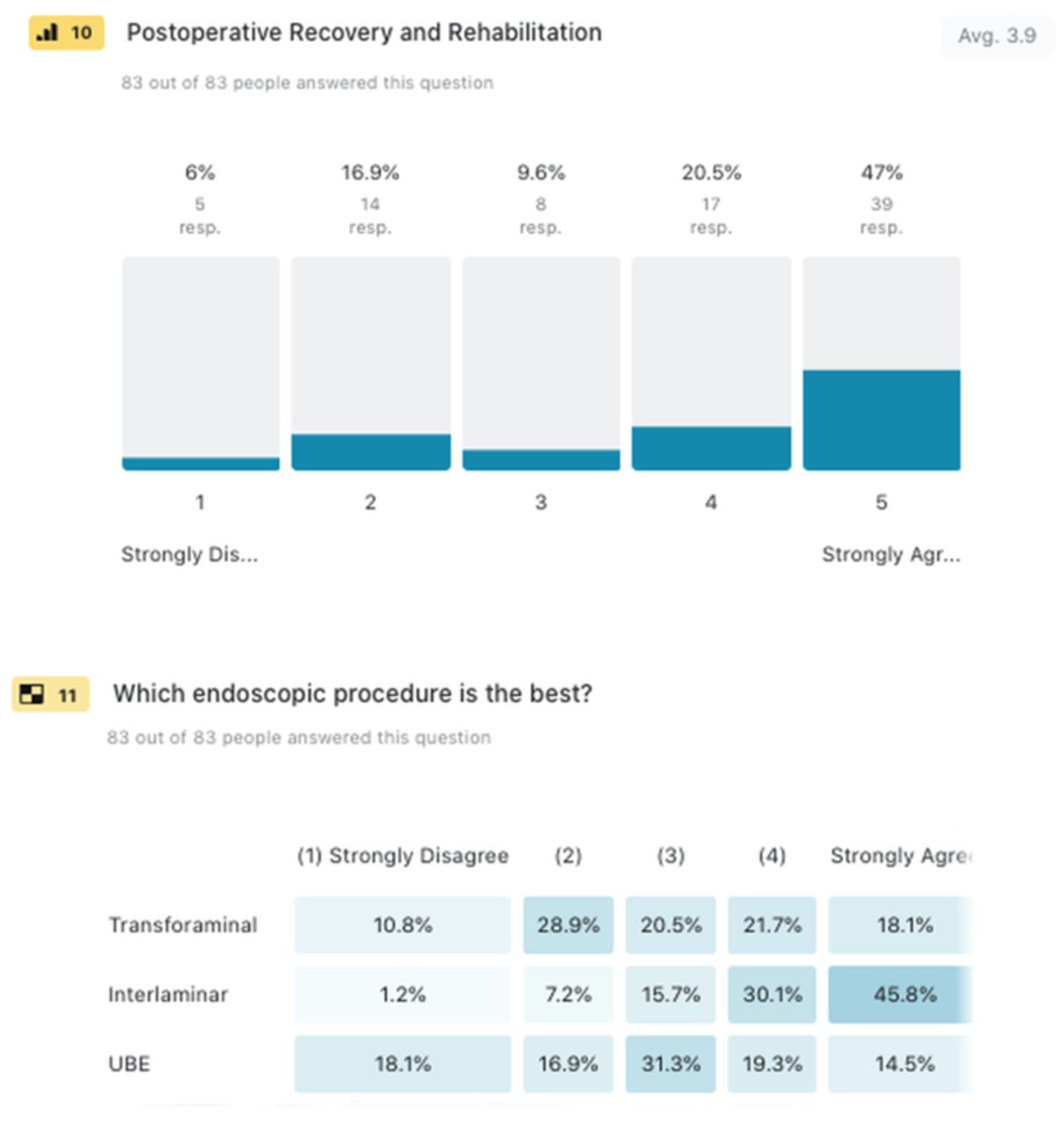
Ease of postoperative recovery (47%) was also considered an essential confounding factor in surgeons' decision-making on the most appropriate choice of lumbar endoscopic decompression surgery for symptomatic spinal stenosis. However, the descriptive statistical breakdown of the level of agreement or disagreement of the best endoscopic technique for lumbar spinal stenosis decompression lacked granular detail. Although the descriptive cross-tabulation analysis on its surface suggested that the transforaminal technique (39.8%) was least applicable to lumbar endoscopic spinal stenosis decompression and the interlaminar technique (75.9), no conclusion could be drawn about the unilateral biportal (UBE) technique with 33.8% identifying the technique as an applicable to endoscopic decompression of lumbar spinal stenosis, vs 35% disagreeing with that statement, and 31.3% of responding surgeons being undecided.
- Figure 6
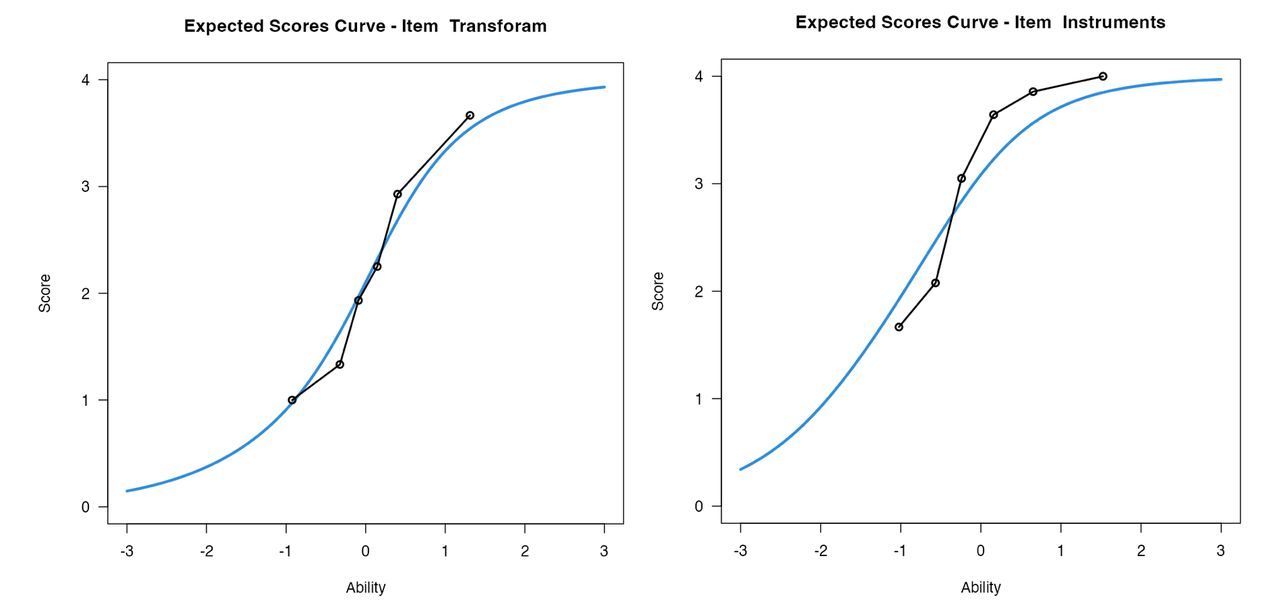
Each item underwent a visual review of its graphical representation using its item characteristic curve (ICC) to assess the alignment between anticipated and actual values. Exemplary ICCs are displayed for the item “transforaminal” (on the left)—deemed the best fit, in contrast to “instruments” (on the right)—now regarded as one of the least fitting items. Dots graphically denote the average response of individuals in each class interval, while the solid blue curve represents the expected values predicted by the Rasch model. Given the close alignment of these points for every 1 of the 8 test items (only 2 shown here), none were excluded.
- Figure 7
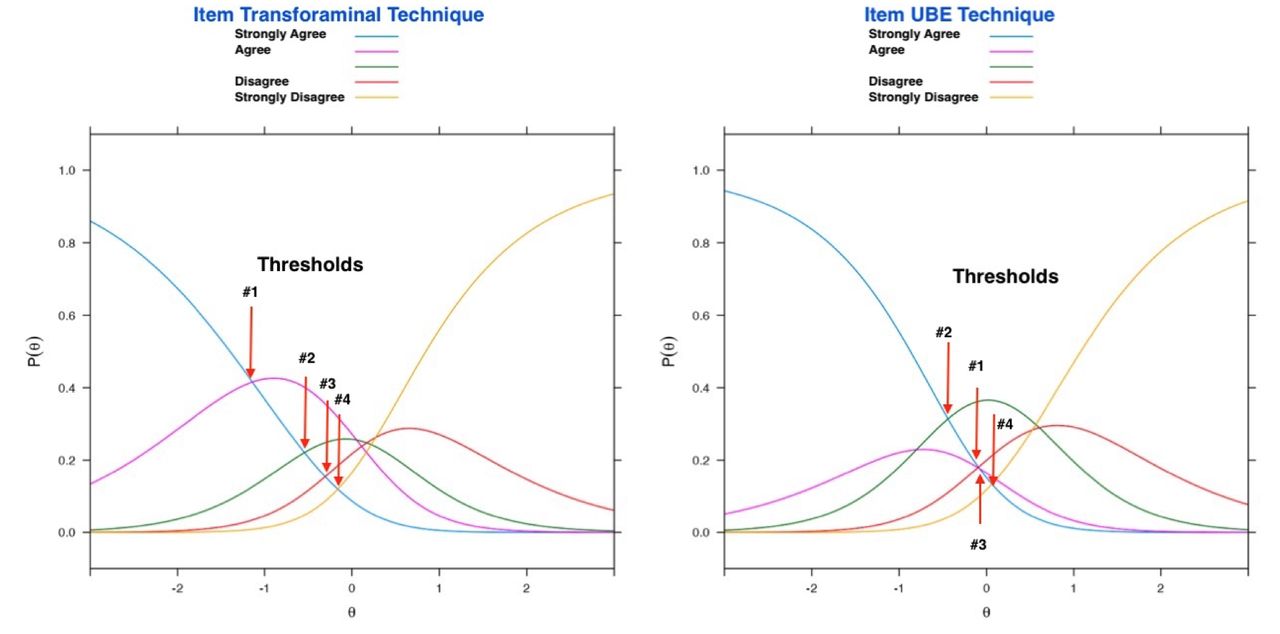
Category probability curve (CPC) is shown for test items “transforaminal” and unilateral biportal (“UBE”). They visually depict the relationship between the probability of a particular category being chosen and the respondent surgeon’s stance, generated for each category. Ordered sequencing of the thresholds (crossover between CPCs of 2 neighboring categories having an equal likelihood of selection) was graphically demonstrated for “transforaminal.” Hence, the data conformed to the Rasch model. This was not the case for the other test items including “UBE” where these threshold points were disorderly sequenced, where the first threshold (ie, where the probability of responding in either category 0 or 1 intersect) occurred after the second threshold (where categories 1 and 2 intersect) along the logit continuum suggesting that for surgeons located anywhere along the response continuum, and especially for those surgeons located at the maximum value for this category, disagreeing with the item (ie, selecting category strongly disagree) is never the most probable response.






Tables
- Table 1
Rasch model item statistics of the rating scale model for confounding factors impacting surgical decision-making.
Test Items Measure SE Measure Infit Outfit Comfort −1.353 0.133 0.924 0.809 Patient −1.159 0.122 1.448 1.542 Outcome −0.993 0.114 0.936 0.963 Instruments −0.867 0.110 0.761 0.749 Rehab −0.785 0.107 1.058 1.048 Model Fit Person Reliability P Scale 0.381 0.061 Note: Infit = Information-weighted mean square based on the χ2 statistic with each observation weighted by its statistical information (model variance). This is more sensitive to unexpected patterns of observations by persons on items that are roughly targeted at them (and vice-versa). Outfit = Outlier-sensitive means square statistic is more sensitive to unexpected observations by surgeons. Infit and outfit data between 0.6 and 1.4 indicate good fit of the Rasch model. MADaQ3 = Mean of absolute values of centered Q_3 statistic with P value obtained by Holm adjustment; Ho = the data fit the Rasch model.
- Table 2
Rasch model analysis item statistics of the rating scale model for selecting 1 of 3 endoscopic techniques as the best for lumbar spinal stenosis decompression.
Endoscopic Techniques Measure SE Measure Infit Outfit Transforaminal −0.0967 0.0959 1.024 1.027 Interlaminar −1.0080 0.1177 0.985 0.990 UBE 0.0136 0.0959 0.956 0.951 Model Fit Person Reliability P Scale 0.328 1.000 Note: Infit = Information-weighted mean square based on the χ2 statistic with each observation weighted by its statistical information (model variance). This is more sensitive to unexpected patterns of observations by persons on items that are roughly targeted at them (and vice-versa). Outfit = Outlier-sensitive means square statistic is more sensitive to unexpected observations by surgeons. Infit and outfit data between 0.6 and 1.4 indicate good fit of the Rasch model. MADaQ3 = Mean of absolute values of centered Q_3 statistic with P value obtained by Holm adjustment; Ho = the data fit the Rasch model.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.