


Article Figures & Data
Figures
- Figure 1
The pelvis is secured with circumferential tape that is affixed to the bed distal to the bed break. Tape should be proximal to the greater trochanter and distal to the iliac crest to avoid draping out of any planned incisions.
- Figure 2
The chest is secured with circumferential taping.
- Figure 3
The pelvis and legs are further secured with circumferential taping.
- Figure 4
The pelvis and legs are further secured with circumferential taping (view from above).
- Figure 5
The table is then “broken” to improve access between the 12th rib and the iliac crest. The amount of table break is greater for levels more cephalad or more caudal due to these structures.
- Figure 6
After securing the patient to the bed, the bed is rotated to obtain a perfect anteroposterior fluoroscopic image. C-arm position is impacted by room orientation and size. Having the intensifier on the posterior reduces surgeon radiation but comes at the cost of ergonomic challenges working around the larger portion of the C-arm.
- Figure 7
Example of marking for L3-L4 and L4-L5. Each disc space angle is marked more broadly, in addition to anterior and posterior aspects of the vertebral body and superior and inferior endplates.
- Figure 8
Example of shallow docking technique. After seating the initial dilator on top of the psoas and dilating up to the retractor, the retractor is then opened superficially to the muscle, allowing the surgeon direct visualization of the muscle prior to piercing the psoas with the initial dilator. An endoscopic Kittner sponge can be used to clear any retroperitoneal fat if there is an obscured view of the psoas.
- Figure 9
After the initial dilator is seated in the psoas muscle under electromyography stimulation, the superficially positioned retractor is then removed.
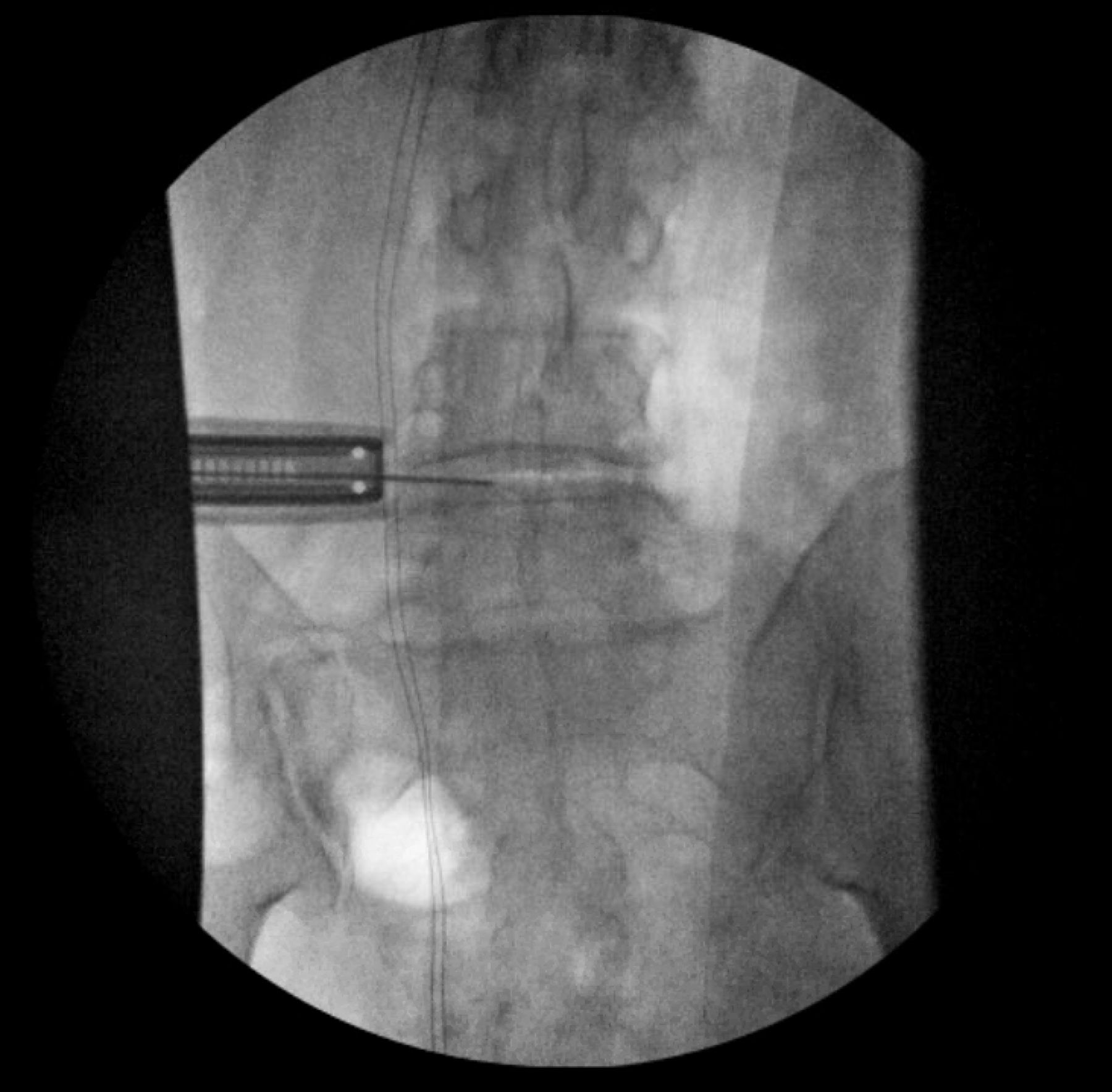
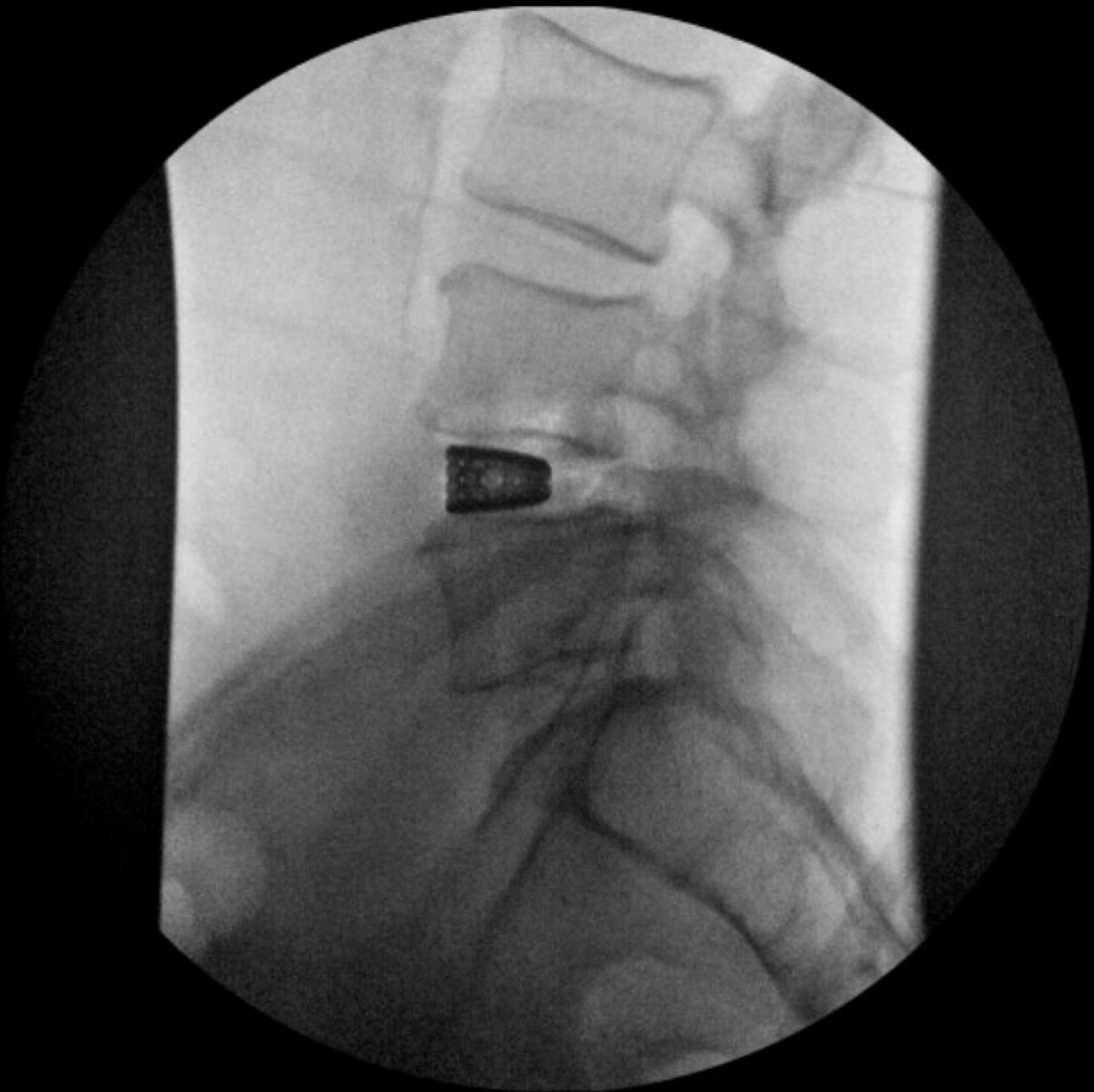
- Figure 10
Position of the initial dilator is confirmed at the level of the disc space on lateral fluoroscopy.
- Figure 11
Sequential dilation through the psoas is performed under live, directional electromyography. The position of the plexus should be identified posteriorly.
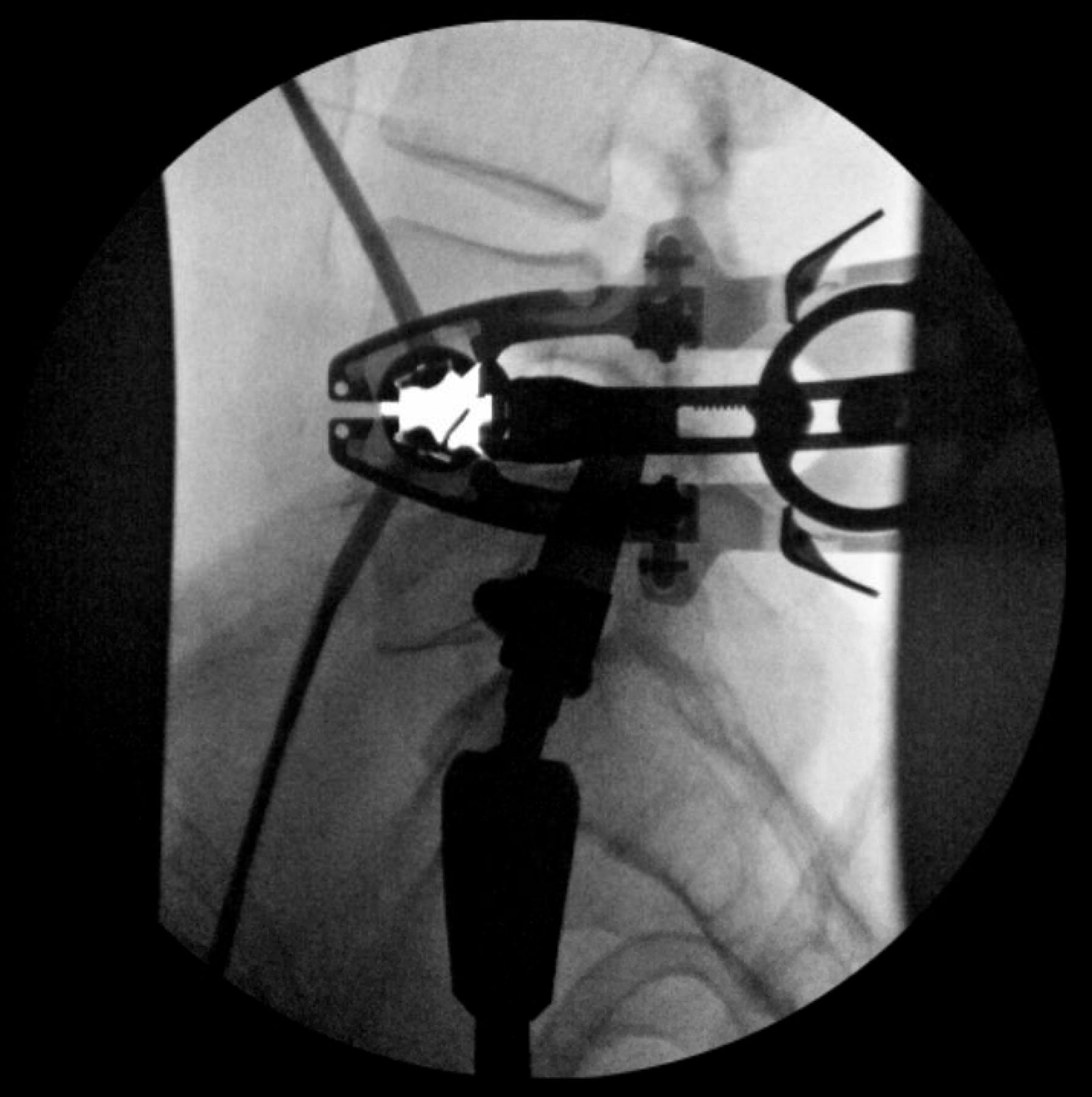
- Figure 12
Orientation of the retractor is confirmed relative to the disc space on anteroposterior view.
- Figure 13
Orientation of the retractor is confirmed relative to the disc space on the lateral view. The retractor is slightly opened to allow electromyography stimulation along the anterior aspect of the posterior blade prior to shim placement.
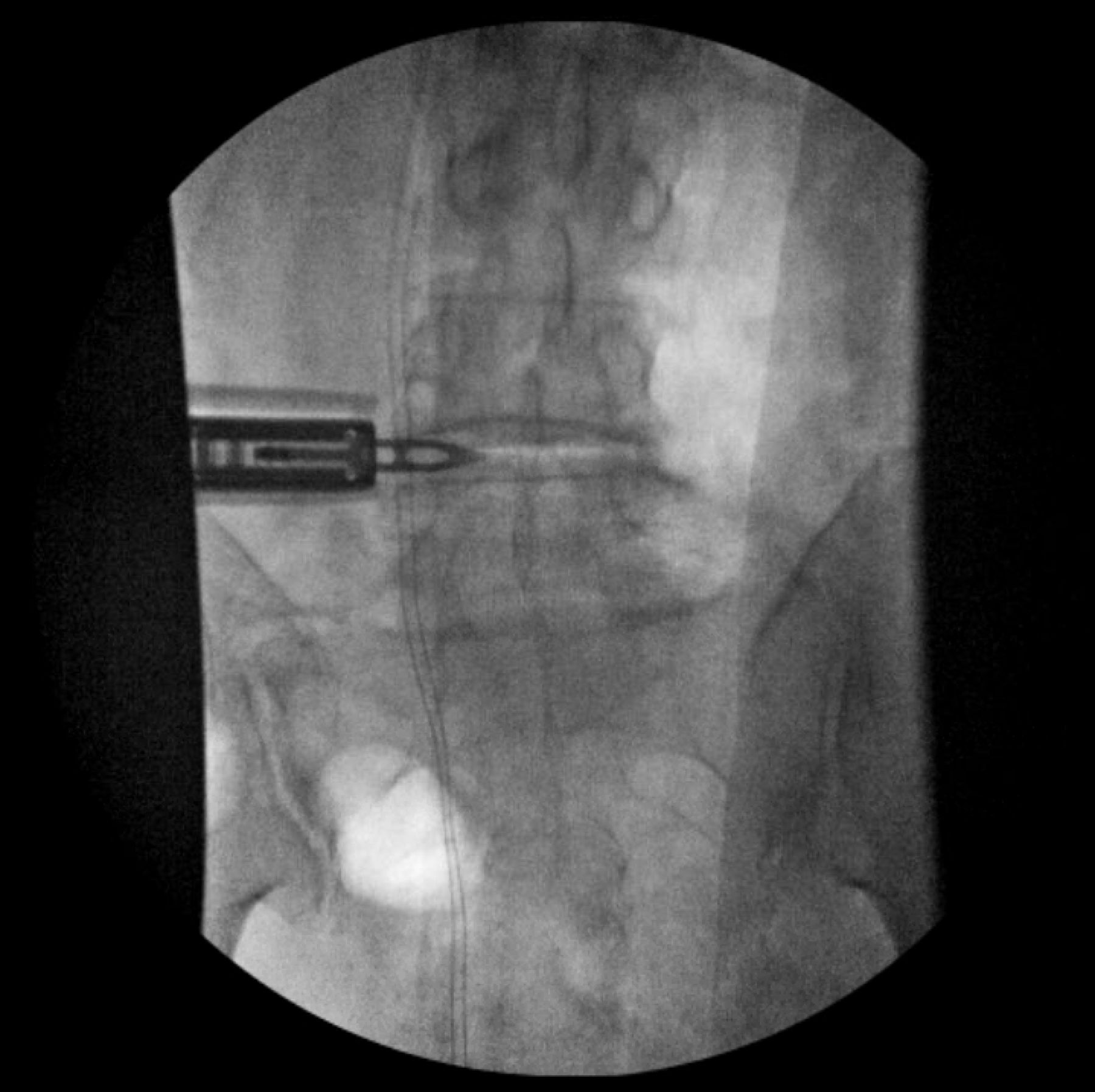
- Figure 14
The shim is then placed under anteroposterior fluoroscopy.
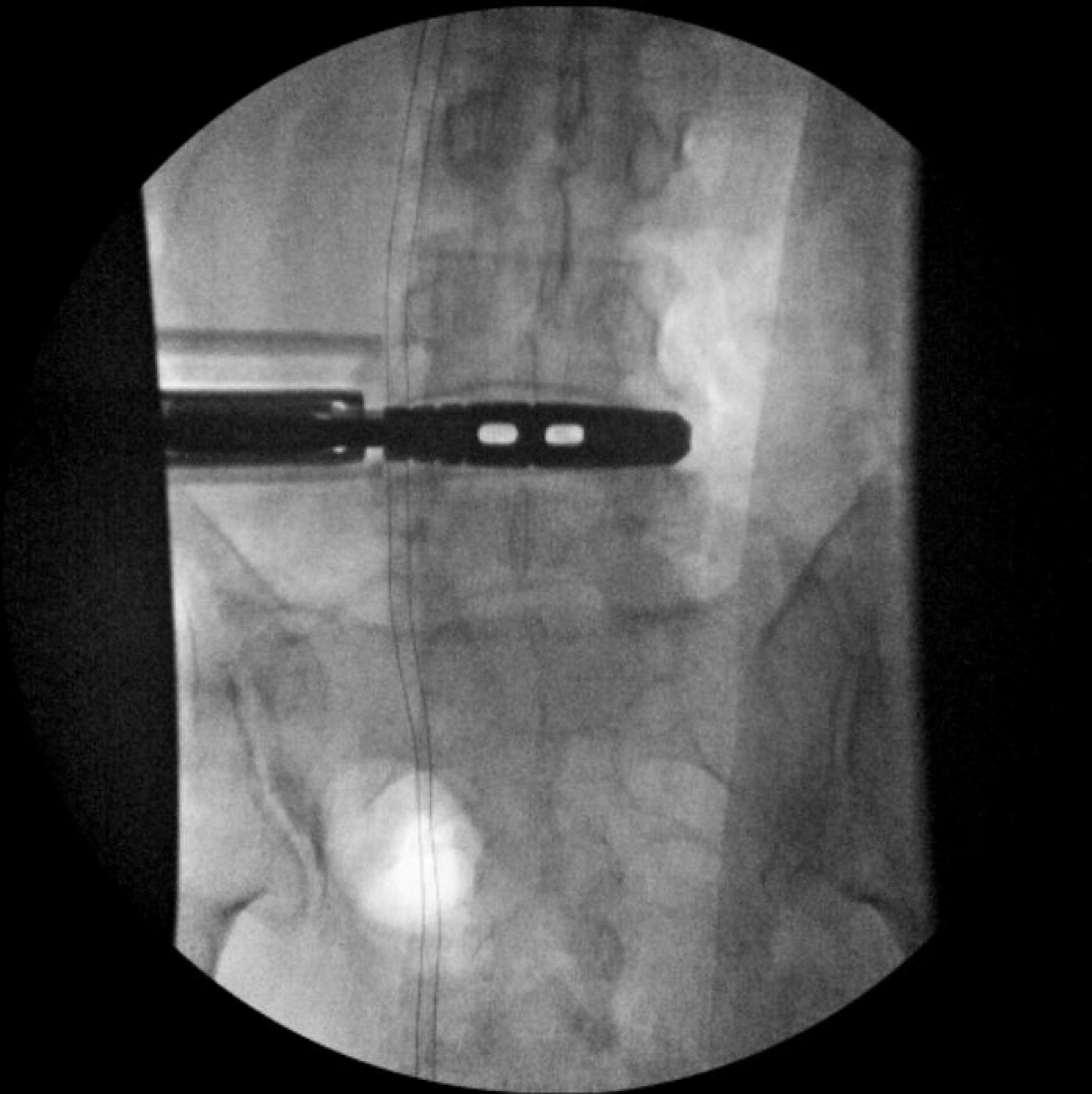
- Figure 15
The retractor is then opened. The position of the anterior and posterior blades as well as the retractor orientation/angle should be noted to allow for further visual landmarks of the operative “safe zone.”
- Figure 16
Trialing is performed under anteroposterior fluoroscopy. After determining the appropriate implant length and height, position of the trial is confirmed on lateral imaging.
- Figure 17
After determining the appropriate implant length and height on the anteroposterior view, position of the trial is confirmed on lateral imaging.
- Figure 18
The final implant is then placed on anteroposterior fluoroscopy.
- Figure 19
The insertion handle is removed, and final position of the implant is confirmed on the anteroposterior view.
- Figure 20
Final position of the implant is confirmed on the lateral view.




















In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.