


Article Figures & Data
Figures
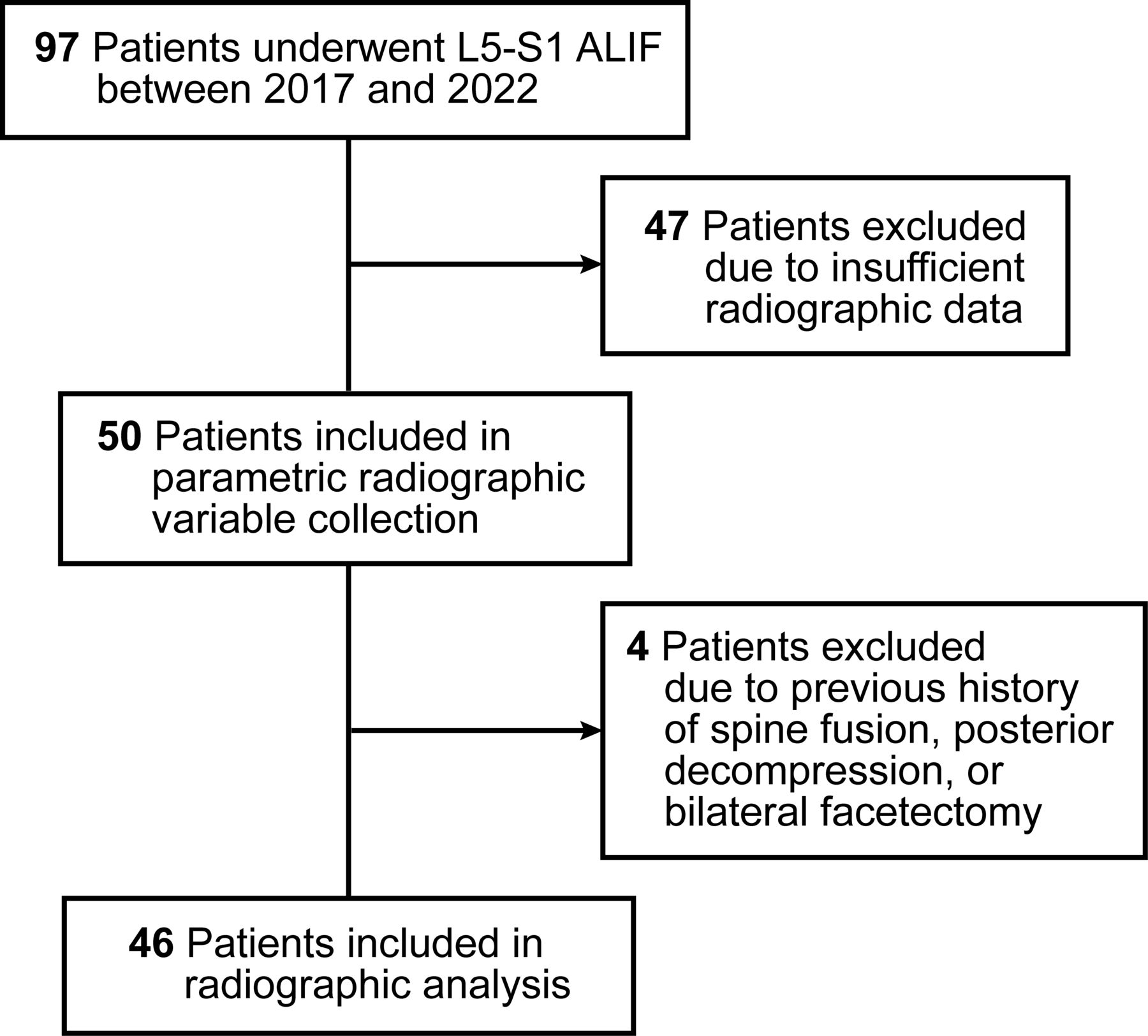
- Figure 1
Patient flowchart showing inclusion and exclusion criteria. ALIF, anterior lumbar interbody fusion. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
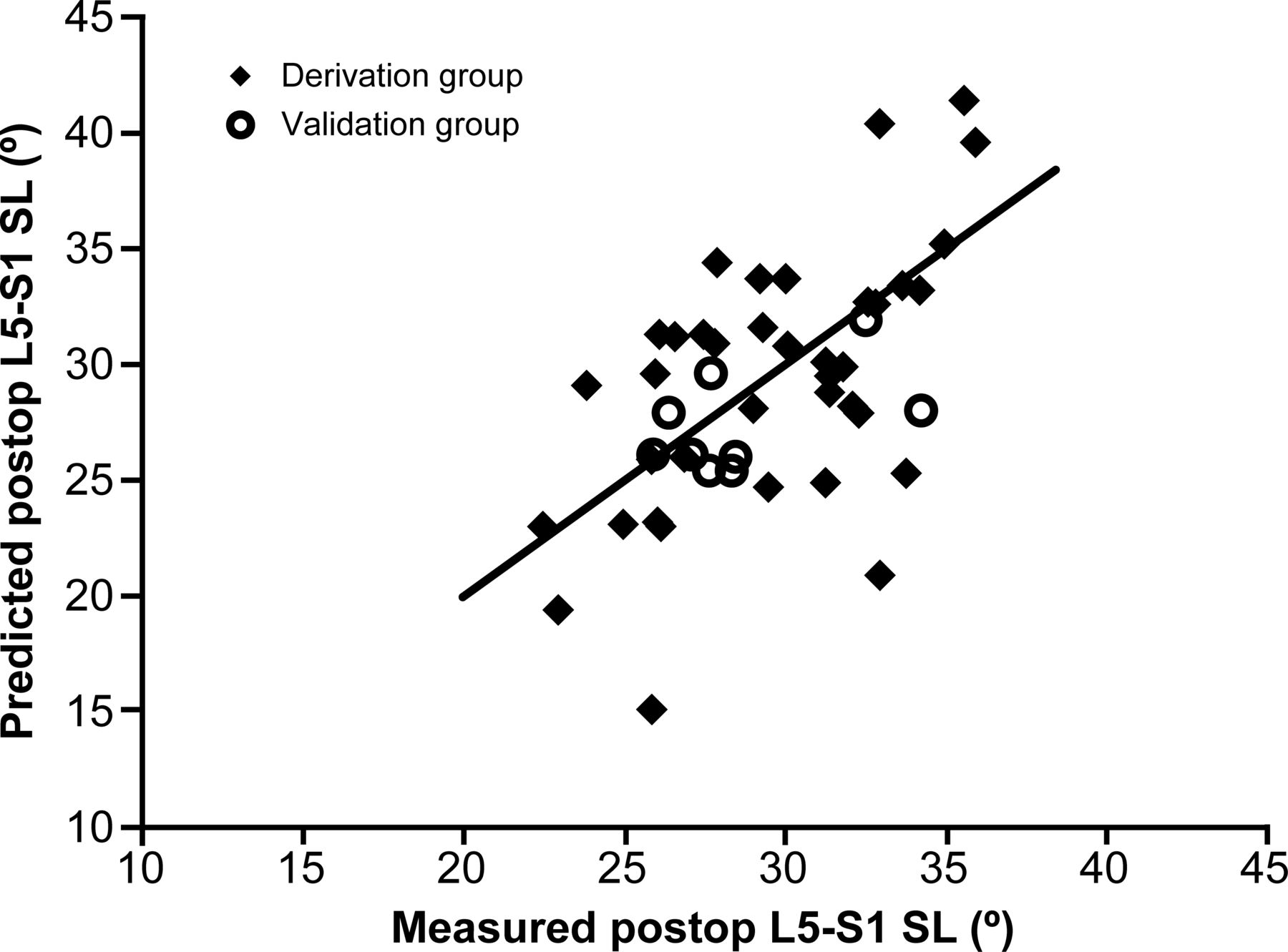
- Figure 2
Scatterplot of predicted vs measured postoperative (postoperative) L5 to S1 segmental lordosis (SL) in derivation (n = 46) and validation (n = 9) groups. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
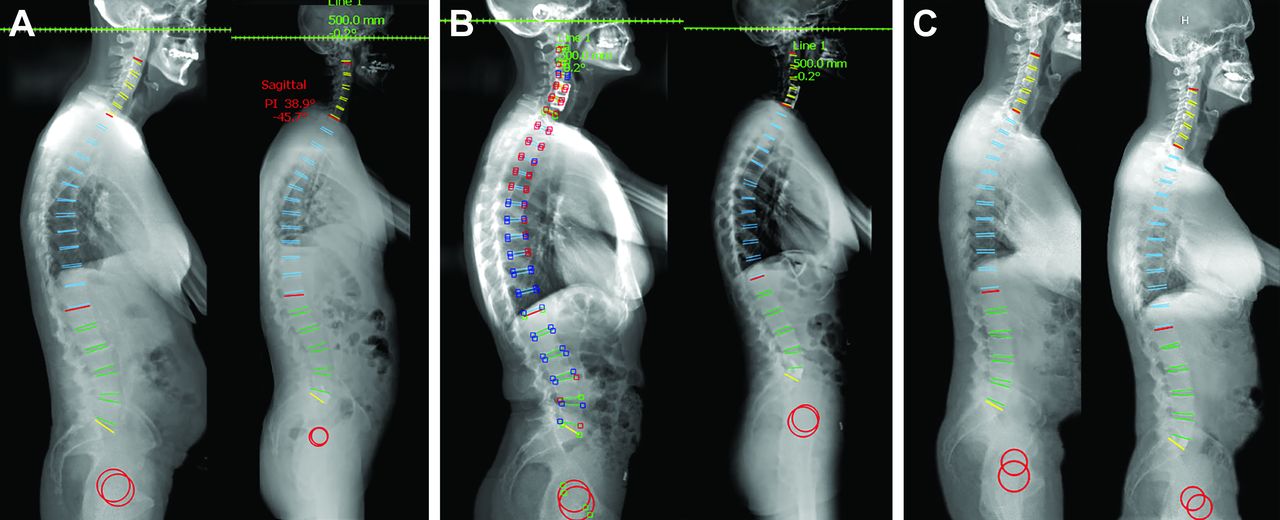
- Figure 3
Case examples demonstrating the use of the following formula for prediction of postoperative L5 to S1 SL: SLpost = 8.741 + (0.454 × C) + (0.595 × SLpre), where SLpost is the postoperative L5 to S1 SL in degrees, C is the cage angle in degrees, and SLpre is the preoperative L5 to S1 SL in degrees. Images were generated using Surgimap software (Nemaris, Inc., New York, NY), in which green indicates a value within the normative range, yellow indicates a measurement value just outside the normative range, and red indicates a measurement value far outside the normative range. (A) Case example from the derivation cohort. Preoperative (left) and postoperative (right) standing radiographs show a preoperative L5 to S1 SL of 23.9° and a postoperative L5 to S1 SL of 28.0°. Using the formula, postoperative L5 to S1 SL = 8.741 + (0.454 × 15°) + (0.595 × 23.9°), resulting in a predicted postoperative L5 to S1 SL of 29.7°. (B) Case example from the derivation cohort. Preoperative (left) and postoperative (right) standing radiographs show a preoperative L5 to S1 SL of 27.3° and a postoperative L5 to S1 SL of 37.2°. Using the formula, postoperative L5 to S1 SL = 8.741 + (0.454 × 20°) + (0.595 × 27.3°), resulting in a predicted postoperative L5 to S1 SL of 34.1°. (C) Case example from the validation cohort. Preoperative (left) and postoperative (right) standing radiographs show a preoperative L5 to S1 SL of 14.4° and a postoperative L5 to S1 SL of 27.9°. Using the formula, postoperative L5 to S1 SL = 8.741 + (0.454 × 20°) + (0.595 × 14.4°), resulting in a predicted postoperative L5 to S1 SL of 26.4°. SL, segmental lordosis. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.



Tables
Characteristic n (%) Age, y, mean (SD) 56 (13.5) Sex Woman 23 (50) Man 23 (50) BMI, mean (SD) 28.3 (4.9) Diabetes 5 (11) Smoking status Never smoker 29 (63) Former smoker 13 (28) Current smoker 3 (7) Unknown 1 (2) Surgical indication Spondylolisthesis 27 (59) Spondylosis 45 (98) Stenosis 44 (96) Spinal deformity 8 (17) Prior surgery at L5–S1 Any 13 (28) Prior hemilaminotomy at L5–S1 4 (9) Prior hemilaminotomy and microdiscectomy at L5–S1 9 (20) ALIF Standalone 24 (52) With posterior instrumentation 22 (48) Abbreviations: ALIF, anterior lumbar interbody fusion; BMI, body mass index.
Cage Characteristic n (%) Dimension, mm, mean (SD) Width 38 (5.25) Depth 28 (4.6) Length 7 (4.1) Material PEEK 23 (50) Titanium 23 (50) Angle 12° 2 (4) 15° 7 (15) 20° 29 (63) 25° 5 (11) 30° 3 (7) Abbreviations: ALIF, anterior lumbar interbody fusion; PEEK, polyetheretherketone.
Radiographic Characteristic Mean (SD) P a Preoperative Postoperative Pelvic tilt, ° 19.0 (8.4) 17.7 (8.2) 0.04 Pelvic incidence, ° 56.0 (15.4) 57.4 (12.9) 0.11 Sacral slope, ° 37.0 (11.3) 39.6 (10.0) 0.002 Lumbar lordosis, ° 52.4 (14.4) 54.8 (14.2) 0.03 PI − LL, ° 3.6 (12.2) 2.3 (10.9) 0.28 T2–T5 thoracic kyphosis, ° 15.4 (5.8) 14.3 (6.6) 0.19 T5–T12 thoracic kyphosis, ° 32.9 (6.9) 32.5 (8.5) 0.95 T1 pelvic angle, ° 15.2 (8.3) 13.9 (7.9) 0.08 Sagittal vertical axis, ° 31.2 (45.3) 19.7 (47.1) 0.12 L1–L2 SL, ° 0.2 (4.7) 0.7 (4.0) 0.03 L2–L3 SL, ° 6.7 (4.5) 4.9 (4.6) 0.002 L3–L4 SL, ° 9.4 (3.9) 7.1 (4.2) <0.001 L4–L5 SL, ° 16.4 (4.8) 14.4 (5.2) 0.002 L5–S1 SL, ° 19.6 (5.2) 29.6 (6.8) <0.001 Global tilt, ° 19.0 (9.9) 17.5 (9.4) 0.07 Anterior disc height, mm 9.5 (3.2) 19.7 (4.1) <0.001 Posterior disc height, mm 4.7 (1.5) 7.7 (2.5) <0.001 Neuroforaminal height, mm 12.2 (3.1) 14.6 (3.2) <0.001 Abbreviations: PI − LL, difference between pelvic incidence and lumbar lordosis; SL, segmental lordosis.
Note: Boldface indicates statistical significance at P < 0.05.
↵a By paired t test.
- Table 4
Summary of r and P values from Pearson correlation analysis including postoperative L5 to S1 SL vs cage angle and preoperative radiographic variables.
Preoperative Variable Postoperative L5–S1 SL P r Cage anglea 0.009 0.40 Pelvic tilt 0.43 0.12 Sacral slopea 0.02 −0.36 Lumbar lordosis 0.01 0.38 PI – LL 0.16 0.23 Sagittal vertical axis 0.86 0.03 L1–L2 SL 0.48 0.12 L2–L3 SL 0.13 0.24 L3–L4 SL 0.74 0.06 L4–L5 SL 0.007 0.42 L5–S1 SLa <0.001 0.54 T2–T5 thoracic kyphosis 0.87 0.02 T5–T12 thoracic kyphosis 0.60 −0.07 T1 pelvic angle 0.80 0.04 Global tilt 0.80 0.04 Anterior disc height 0.79 −0.04 Posterior disc height 0.87 −0.02 Neuroforaminal height 0.46 0.117 Cage height 0.36 −0.15 Cage width 0.61 −0.83 Cage depth 0.81 −0.04 Abbreviations: PI – LL, difference between pelvic incidence and lumbar lordosis; SL, segmental lordosis.
Note: Boldface indicates statistical significance at P < 0.05.
↵a Power > 0.8.
- Table 5
Summary of coefficients and P values from multiple linear regression analysis including postoperative L5 to S1 SL and preoperative variables with significance during univariate analysis.
Preoperative Variable Postoperative L5–S1 SL P C Cage angle 0.048 0.452 Sacral slope 0.92 0.02 Lumbar lordosis 0.44 0.10 L4–L5 SL 0.67 −0.15 L5–S1 SL 0.01 0.51 Abbreviations: C, coefficient; SL, segmental lordosis.
Note: Boldface type indicates statistical significance (P < 0.05).
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.