


Abstract
As the surgical treatment of spinal degenerative conditions increases, more patients will ultimately require revision spine surgery. Revision spine surgery is more technically demanding than primary surgery with increased complication rates and variable clinical outcomes. The freehand placement of pedicle screws into a previously operated and/or fused level is more difficult due to the altered anatomic landmarks and/or bone loss. Additional benefit of robotic spine surgery is appreciated during such revision spine surgical procedures with unusual anatomic considerations, whereby the preoperative planning using robotic planning software and computer-assisted robotic guidance play a crucial role in assisting the surgeon to “visualize the invisible.” We highlight 3 roles of this technology in 3 cases: planning strategic osteotomies, redrilling of screw holes, and insertion of revision screws in previously operated thoracolumbar and cervical spine regions.
- revision spine surgical procedures
- altered osseous anatomy
- preoperative planning
- robotic planning software
- computer-assisted robotic guidance
INTRODUCTION
As the surgical treatment of spinal degenerative conditions increases, more patients will ultimately require revision spine surgery. Revision spine surgery is more technically demanding than primary surgery with increased complication rates and variable clinical outcomes.1–5 When undertaking a revision operation, the surgeon must consider many factors that are not always applicable during a primary procedure (eg, altered vascular supply, postsurgical epidural fibrosis, muscle and ligamentous scarring, as well as altered osseous anatomy). At the time of revision surgery, the freehand placement of pedicle screws into a previously operated and/or fused level is more difficult due the altered anatomic landmarks and/or bone loss.6,7 Revision freehand placement strategies have been described, but even the most experienced surgeons state that they rely on virgin adjacent levels to find the precise entry site in the absence of remnant anatomic landmarks.6
A serendipitous potential benefit of robotic spine surgery (RSS) is appreciated during cases with unusual anatomic considerations.8 While the most studied application of RSS is the placement of thoracic and lumbar pedicle screws, numerous other applications have been described with good outcomes; cervical pedicle screws,9 S2 alar-iliac screws,10,11 interbody fusion devices,12 adolescent idiopathic scoliosis,13 infection,14,15 and primary and metastatic spinal tumors.16,17
Preoperative planning and robotic guidance techniques have demonstrated the ability to assist the surgeon to “visualize the invisible.”9 To that end, a retrospective case series published by Hu et al reported 98.9% accuracy of 960 robotically placed pedicle screws placed in 95 patients.18 Nearly 90% of patients in their series had significant deformity and/or prior surgery.
Over the past 17 years, the senior author (I.H.L.) has utilized Mazor (Medtronic, Minneapolis, MN) robotic guidance and preoperative planning software for revision reconstructions with altered anatomic landmarks. Cases from a recent 6-year period have been documented via a prospectively collected dataset. In total, 628 revision cases were done during this time, with 1047 screws implanted in existing screw tracts and 5214 screws implanted in newly drilled screw tracts. The rate of malpositioned screws requiring return to OR was 0.2% (13 out of 6261 screws in 8 out of 628 cases). The following 3 cases highlight the diverse capabilities of RSS to facilitate safe and reliable pedicle screw placement in the setting of revision spine surgery.
CASES
Case 1—Planning Osteotomies and Redrilling Pedicle Screw Trajectories
The patient is a 64-year-old woman who was severely limited in her day-to-day activities owing to substantial mechanical back pain, bilateral lower extremity radiculopathy, neurogenic claudication symptoms, and weakness. She had an extensive spine surgical history, having undergone 5 prior lumbar spine surgical procedures at outside institutions.
The clinical picture was consistent with iatrogenic flat back, adjacent segment deterioration with spondylolisthesis, postlaminectomy syndrome, lumbar spinal stenosis, and radiculopathy (Figures 1 and 2).

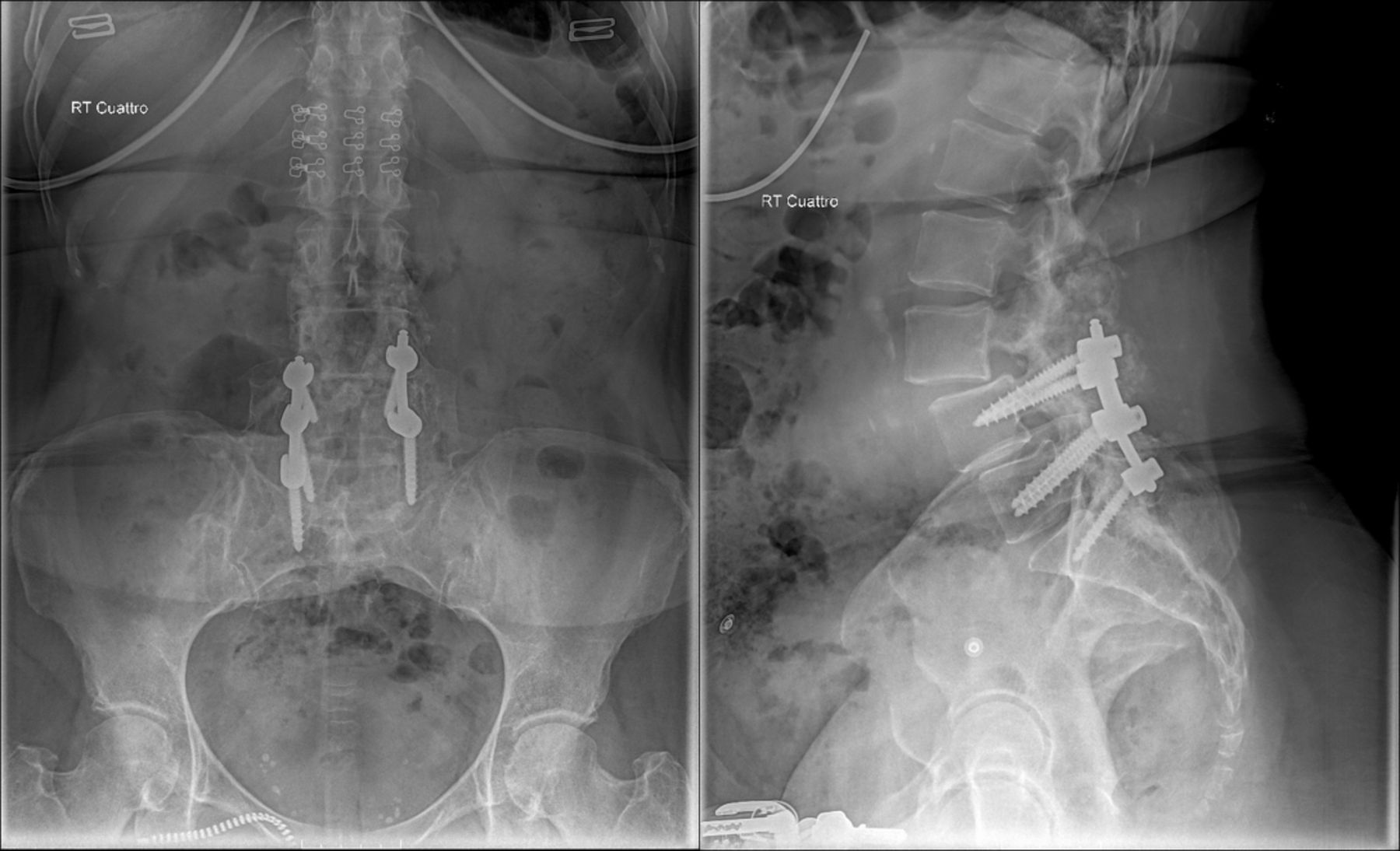
Case 1: Lumbar spine anteroposterior and lateral standing radiographic images of the lumbosacral spine demonstrated intact hardware from L4 to S1, evidence of an iatrogenic flat back, grade I spondylolisthesis of L4-L5 level, grade I adjacent segment spondylolisthesis at the L3-L4 level, and increased proximal lumbar lordosis to compensate for her iatrogenic flat back.

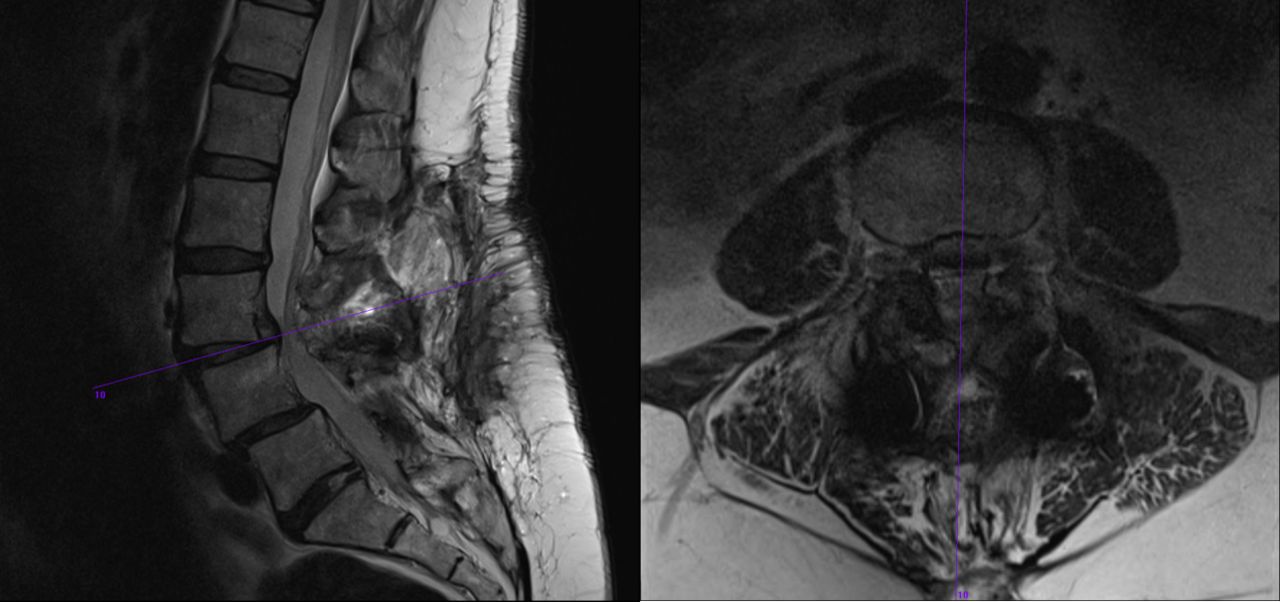
Case 1: Lumbar spine magnetic resonance images verified adjacent segment deterioration at the L3-L4 level as well as reduction in the degree of spondylolisthesis in comparison to the standing radiographic images. There was also evidence of central and lateral recess stenosis and a disc herniation at this level.
She underwent corrective reconstruction of her iatrogenic flat back deformity via a 3-staged approach utilizing the preoperative planning software and computer-assisted robotic guidance (Figures 3 and 4).
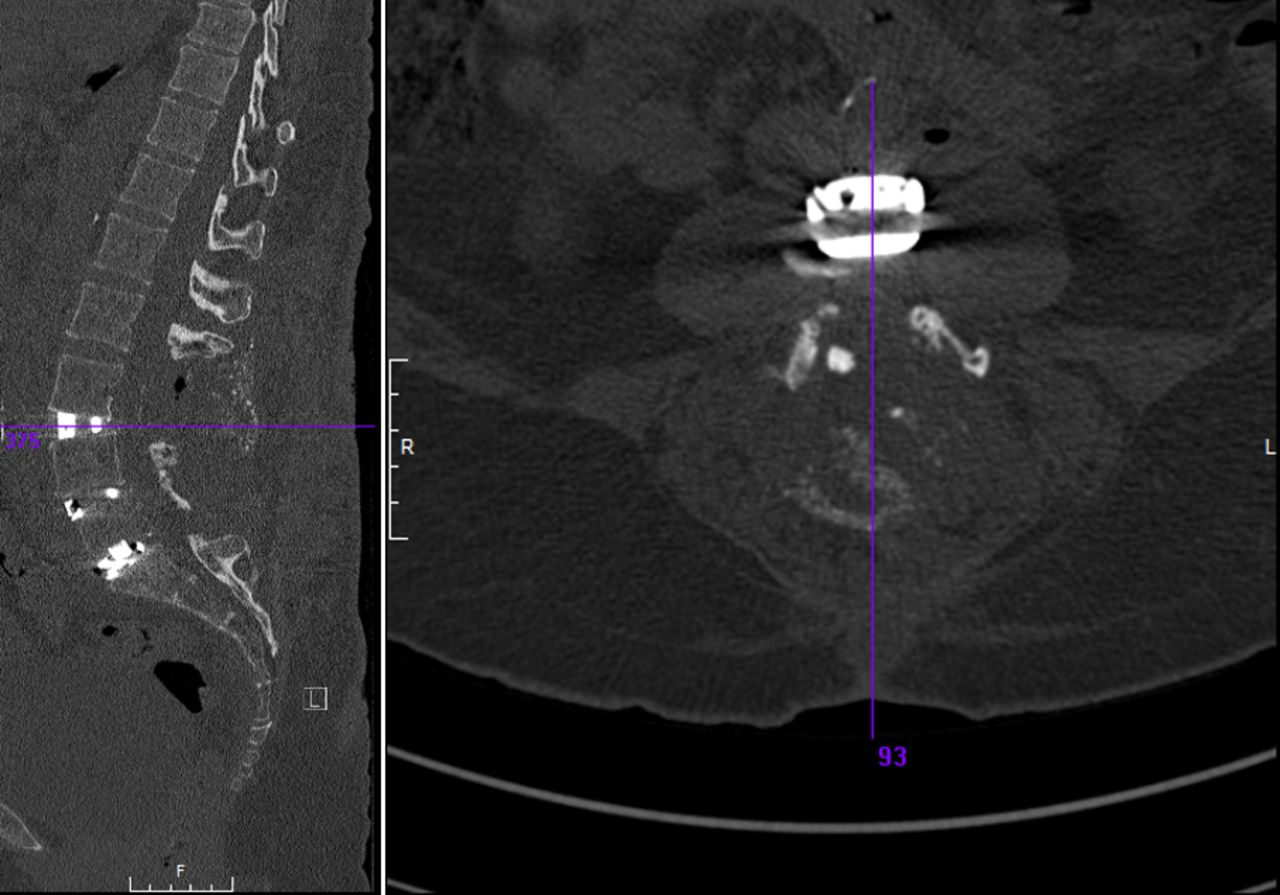
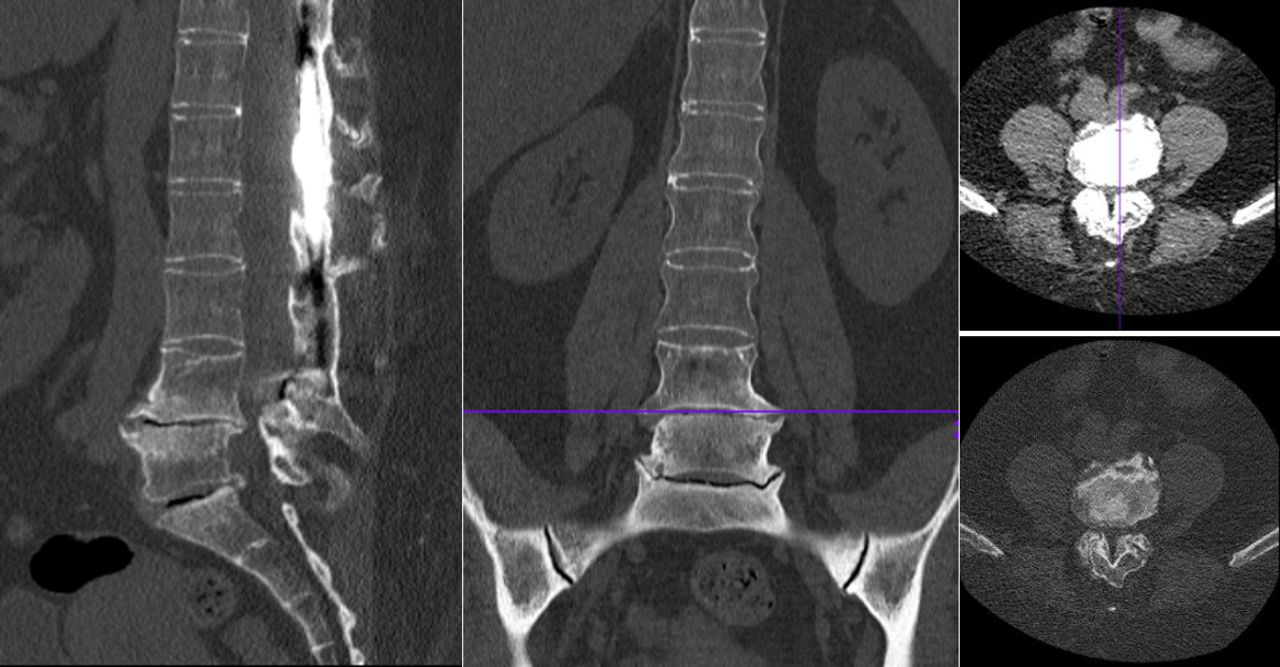
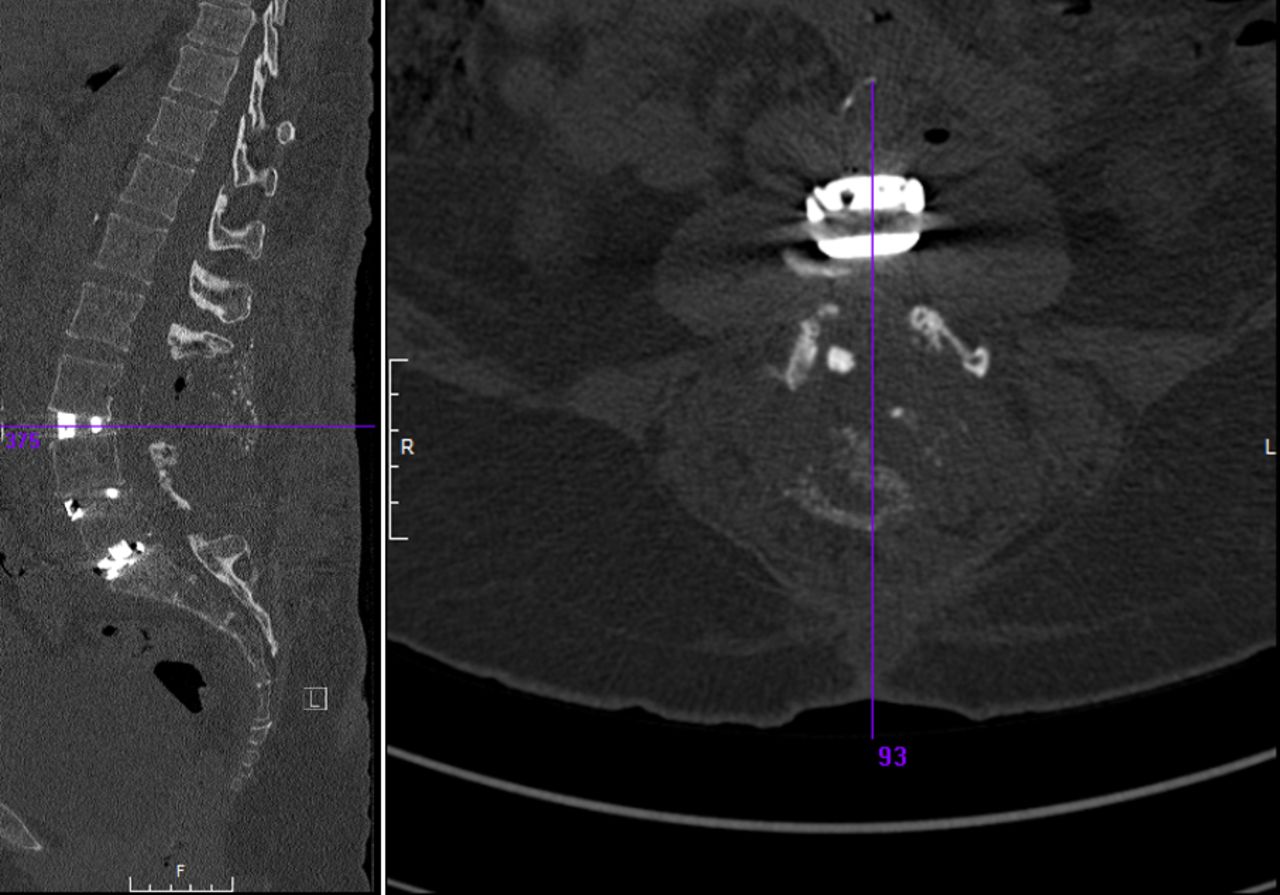
Case 1: Computed tomography images after stage II confirmed substantial restoration of lordosis and reduction of the spondylolisthesis at both the previously fused L4-L5 level as well as the adjacent L3-L4 level.
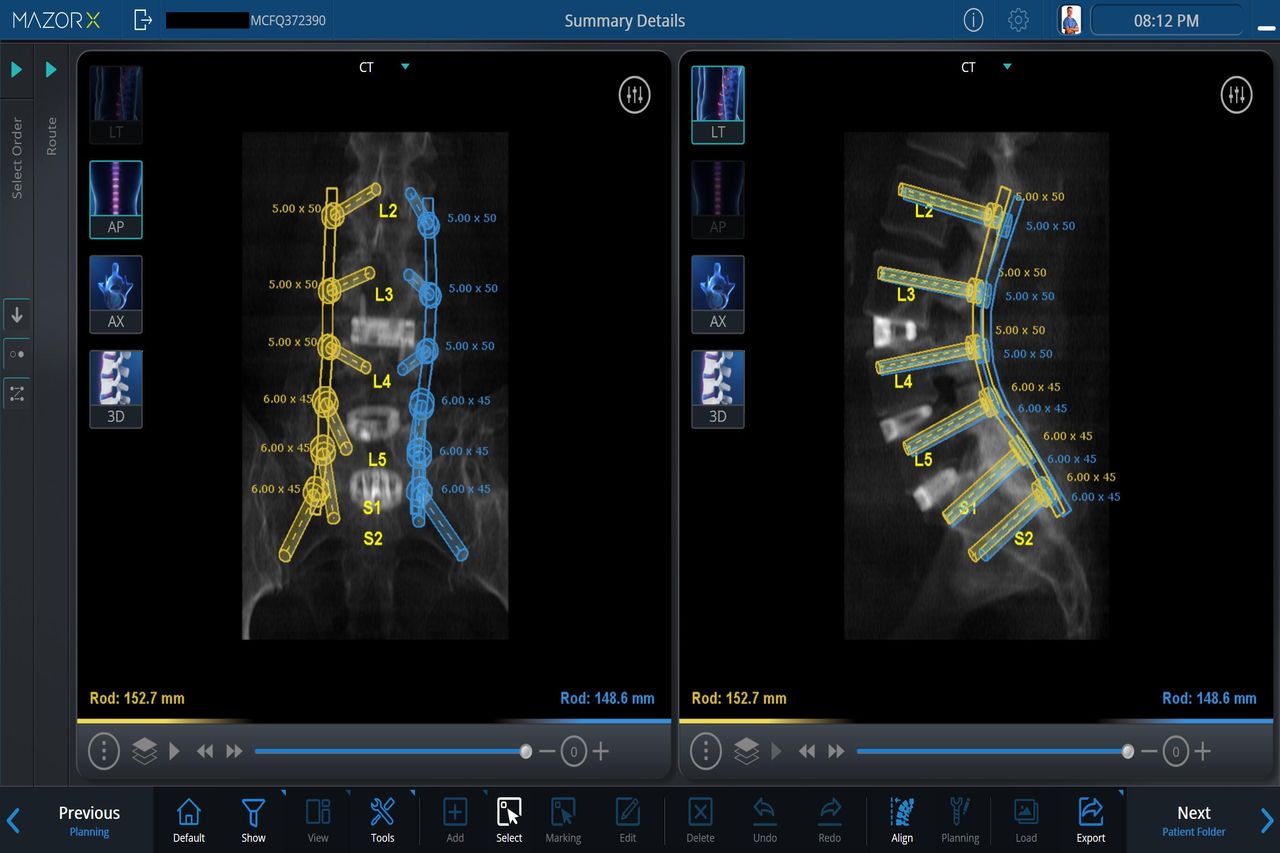
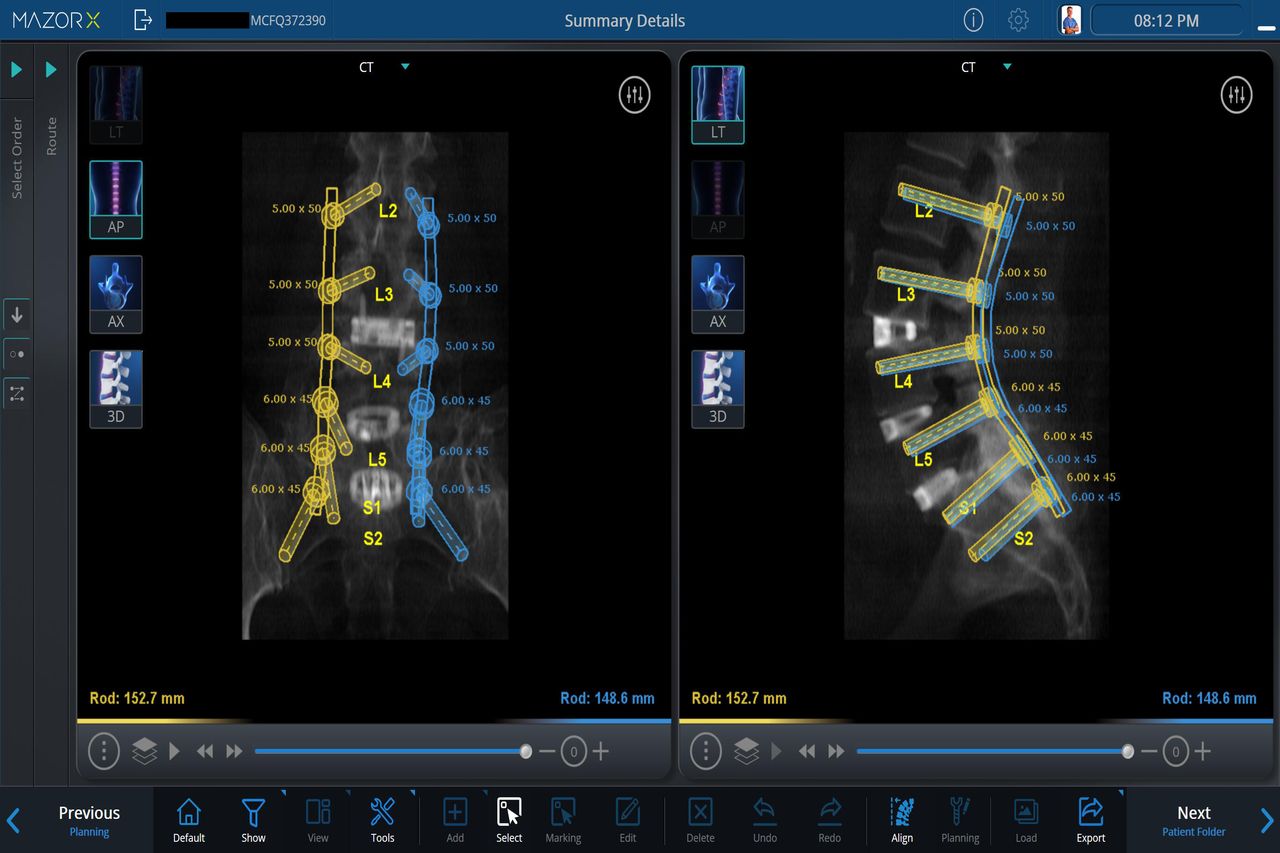
Case 1: Preoperative planning for robotic-assisted placement of pedicle screws.
Stage I: Posterior removal of spinal instrumentation, exploration of fusion, osteotomies of the fusion mass at L4 and L5, Smith Petersen/Ponte osteotomies at other levels, and bilateral laminotomy-foraminotomy decompression at the L3-L4 level.
Stage II (2 days later): Anterior L3-L4, L4-L5, and L5-S1 discectomy, decompression, and interbody fusion with structural graft.
Stage III (8 days after stage I): Revision posterior L3-S1 instrumentation, correction, and fusion with robotic-assisted insertion of pedicle screws.
The patient reported improvement in her lower extremity symptoms, was able to ambulate with a walker, and was discharged to inpatient rehabilitation 3 days after stage III (Figure 5).
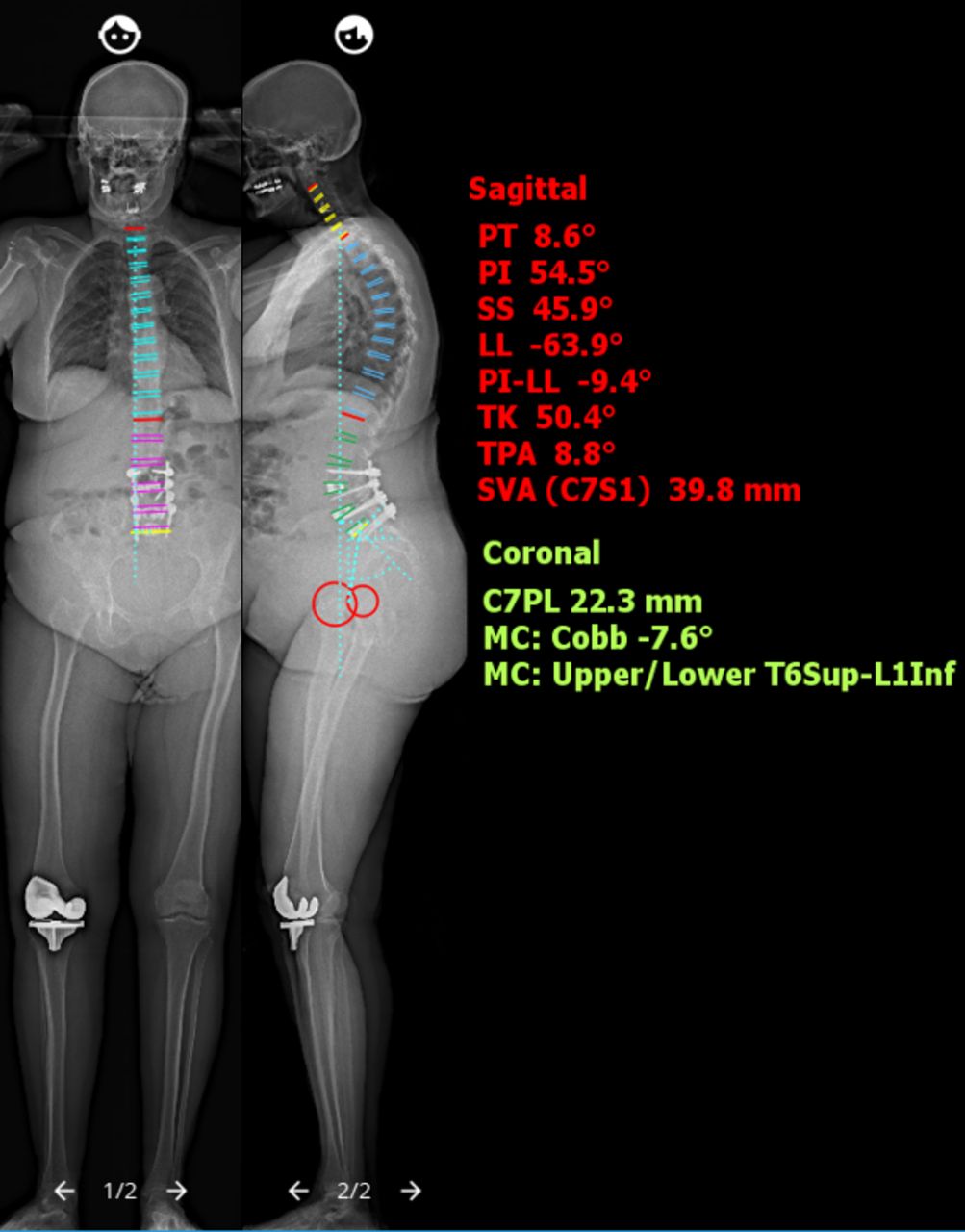
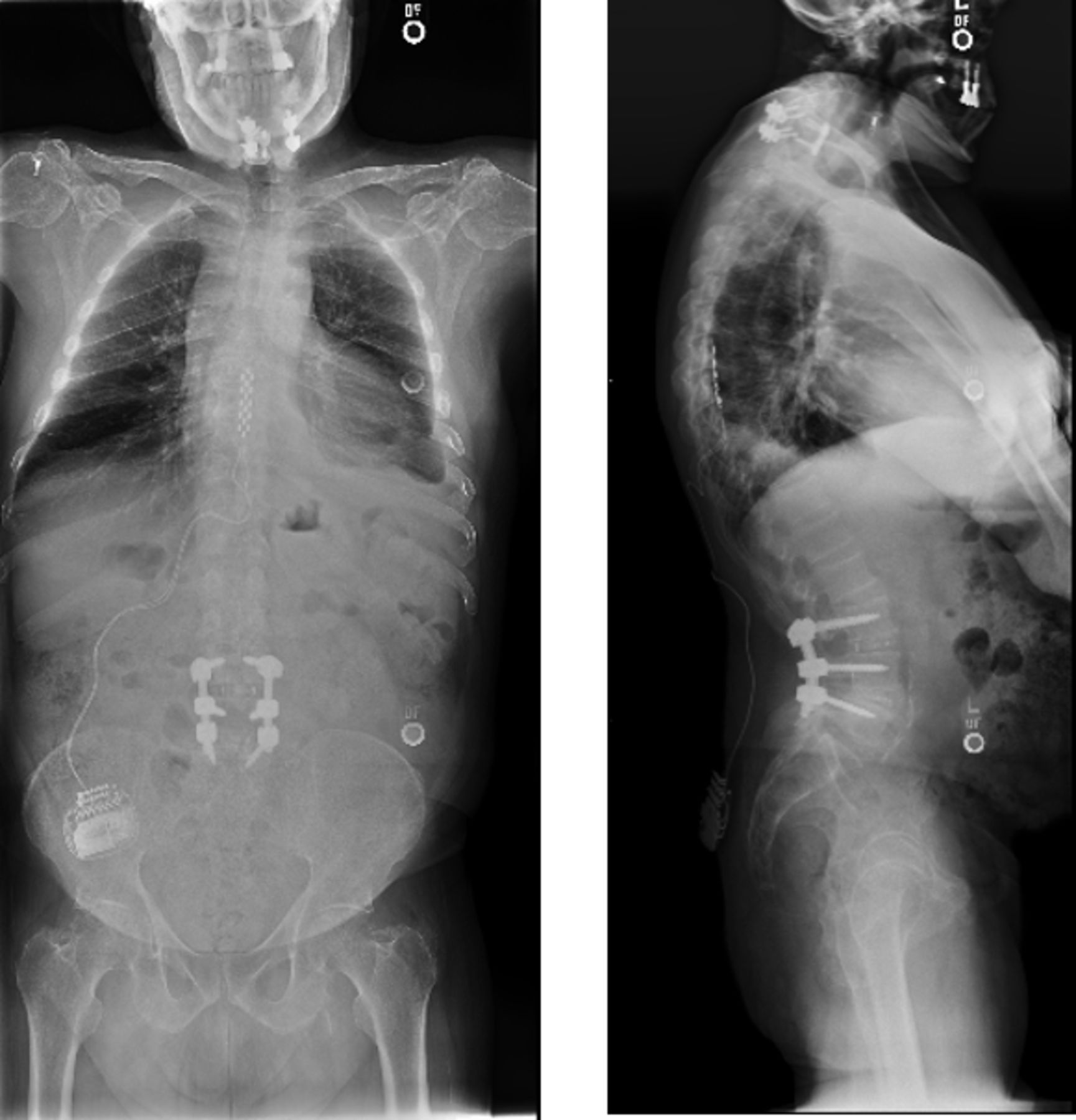
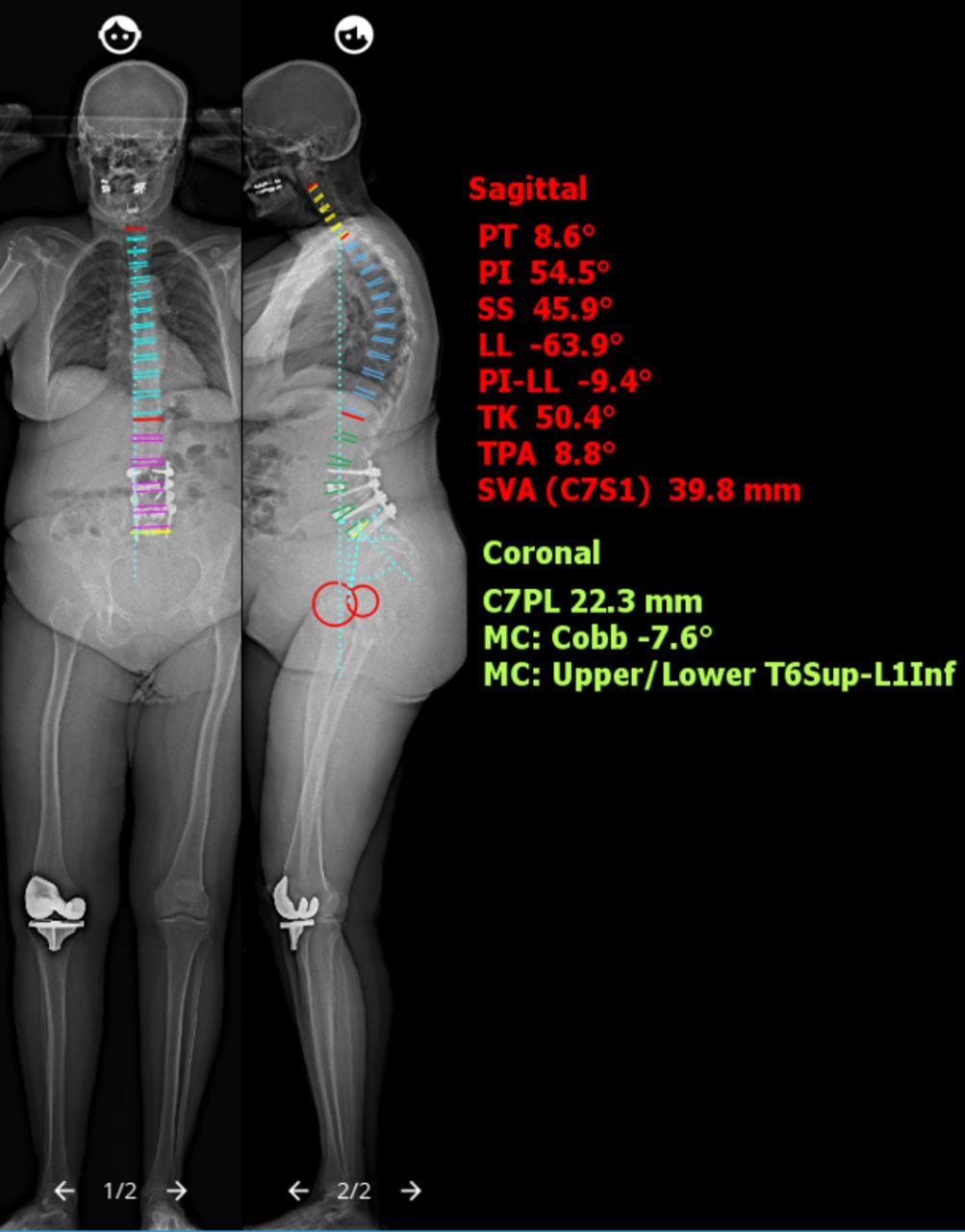
Case 1: Postoperative EOS ImagingTM (Electro Optical System) full-length spine radiographs demonstrate reduction of the spondylolisthesis and restoration of spinopelvic and sagittal parameters. PT, sagittal pelvic tilt; PI, pelvic incidence; SS, sacral slope; LL, lumbar lordosis; PI-LL, PI-LL mismatch; TK, thoracic kyphosis; TPA, T1 pelvic angle; SVA, sagittal vertical axis; C7PL, C7 plumb line; MC, major Cobb angle.
Revision spine surgical procedures are complicated by the distortion of known anatomic landmarks due to prior surgery and ongoing degeneration. These landmarks are important for safe bone work (osteotomies and decompressions) and placement of additional instrumentation. The preoperative planning software enables the planning of strategic decompressions, osteotomies, and pedicle screws. In addition, the software simulates the corrective surgical procedure and its effect on global spinal alignment, thereby allowing the planning of the osteotomy site, amount of correction required, and the evaluation of the potential global effect of the correction.
Through the preoperative planning software, we were able to estimate the extent of achievable correction per osteotomy, thereby allowing us to distribute the correction process across multiple levels. In doing so, we were able to achieve a more harmonious deformity correction instead of a focal sharp correction as would have been the case with a pedicle subtraction osteotomy.
With the aid of the robotic software, the preoperative planning process, and the robotic apparatus, we were able to accurately redrill new pedicle screw trajectories and had good purchase for most of the screws (the right L4-pedicle screw had inadequate purchase and was removed). The goals regarding ideal bone purchase and tulip alignment remain in the revision setting. However, the previous screw holes are typically not in the ideal position and the effort to redrill a screw hole manually is very difficult as the drill bit/screw tends to skive into the previous path. The use of preoperative planning and robotic guidance facilitates a more stable environment to drill new screws across a trajectory either crossing or realigning the previous screw hole.
Case 2—Placement of Pedicle Screws Into Fusion Mass
The patient is a 53-year-old woman with known adolescent idiopathic scoliosis who had undergone correction with a Harrington rod at age 13 years and presented with increasing complaints of mechanical low back pain, right buttock pain, sagittal imbalance, and worsening bilateral leg stenotic symptoms. Her main concern was difficulty with her day-to-day work and home activities.
The clinical picture was consistent with a flat back deformity, adjacent segment deterioration, and neurogenic claudication (Figures 6 and 7).
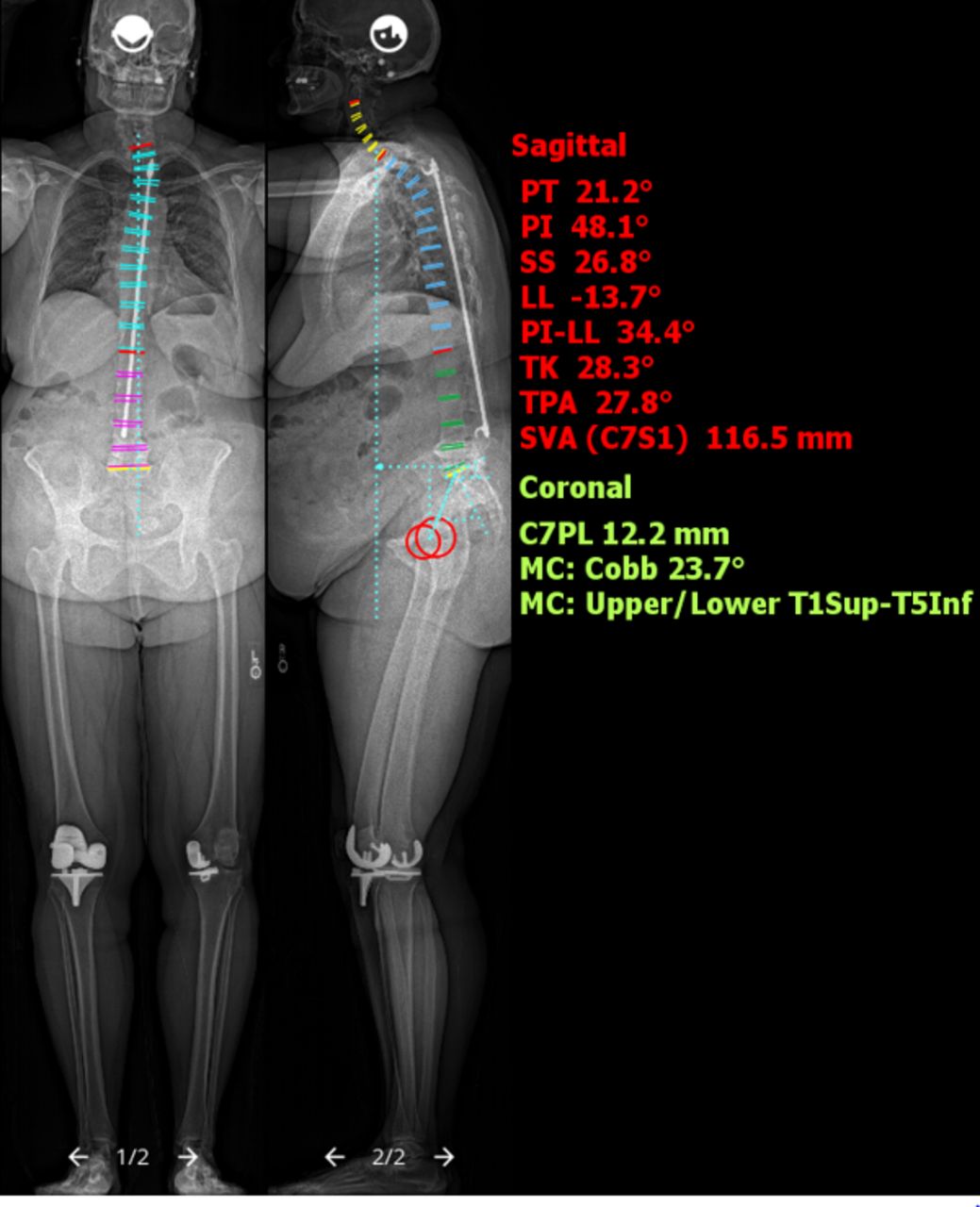
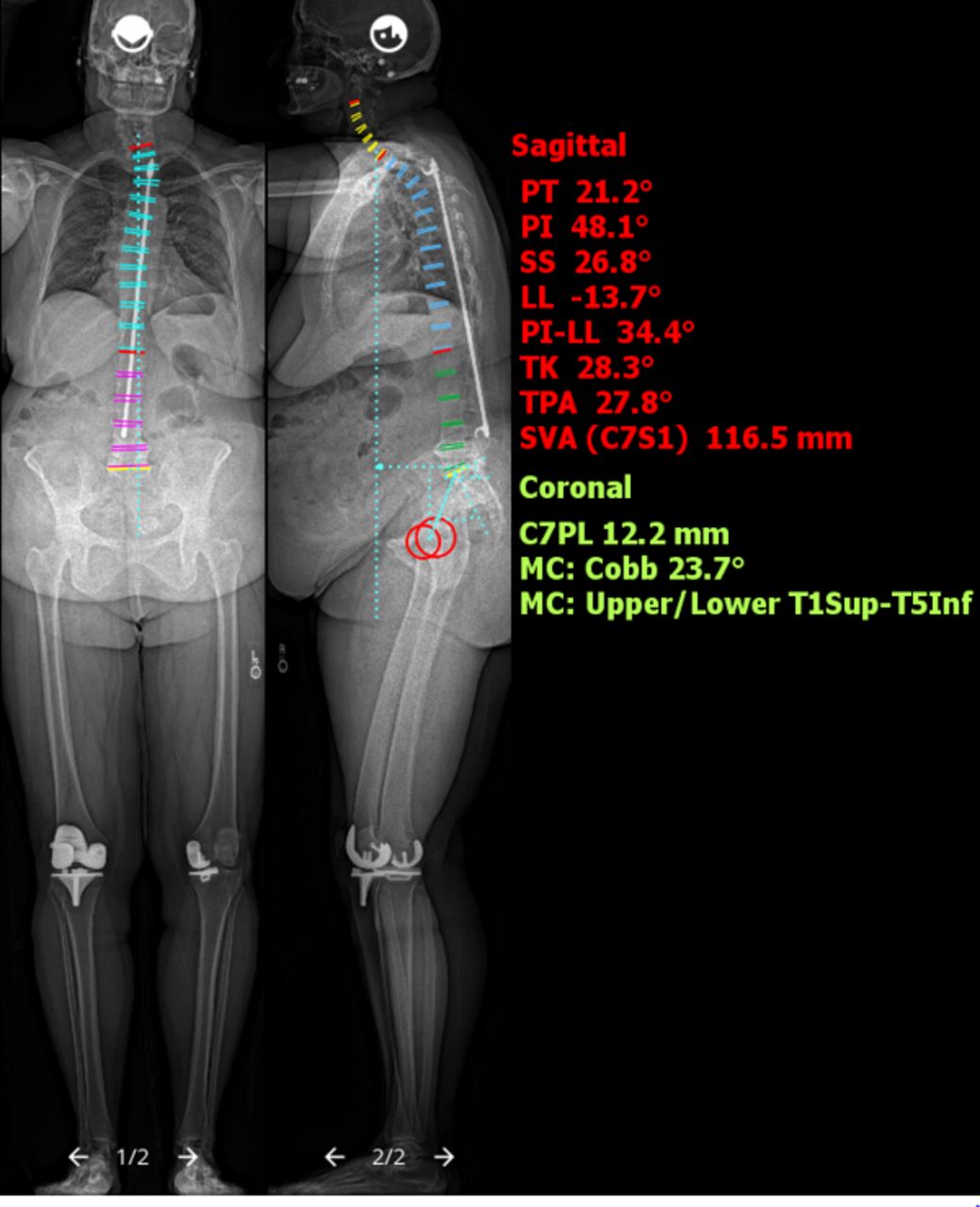
Case 2: Preoperative EOS ImagingTM (Electro Optical System) full-length spine films revealed Harrington rod fixation across the thoracolumbar spine with degenerative changes most pronounced from L4 to S1. PT, sagittal pelvic tilt; PI, pelvic incidence; SS, sacral slope; LL, lumbar lordosis; PI-LL, PI-LL mismatch; TK, thoracic kyphosis; TPA, T1 pelvic angle; SVA, sagittal vertical axis; C7PL, C7 plumb line; MC, major Cobb angle.
Case 2: Computed tomography images revealed end-stage deterioration at the L4-L5 and L5-S1 levels, with foraminal stenosis at both those levels. The proximal fusion was well healed with a solid posterior fusion mass.
She underwent a staged anterior-posterior reconstruction procedure:
Stage I: Anterior L5-S1 discectomy, decompression, and interbody fusion with structural graft, aimed to restore lordosis and act as a foundation for her posterior reconstruction (Figure 8).
Stage II: Open revision posterior instrumentation using robotic assistance (Figure 9) from L3 to S1 with bilateral open sacroiliac joint fixation along with multilevel decompressions and Smith Petersen osteotomies to relieve her stenosis and correct her sagittal malalignment (Figure 10).

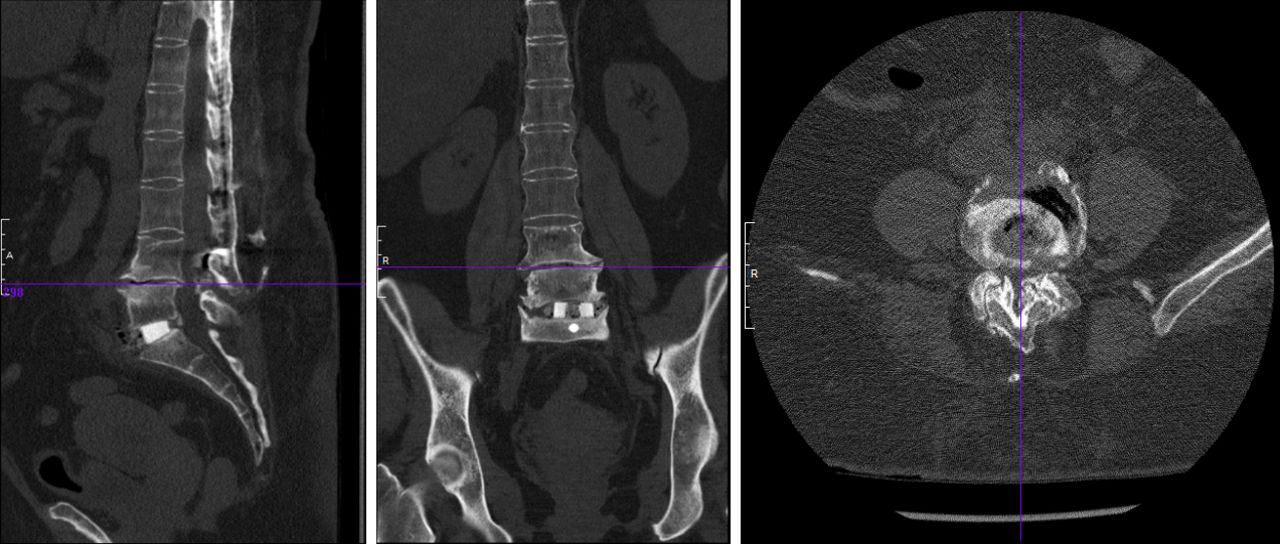
Case 2: Computed tomography images after stage I anterior fusion.

Case 2: Preoperative planning for robotic-assisted placement of pedicle screws. Note that screws placed through fusion mass where anatomic landmarks are lost.

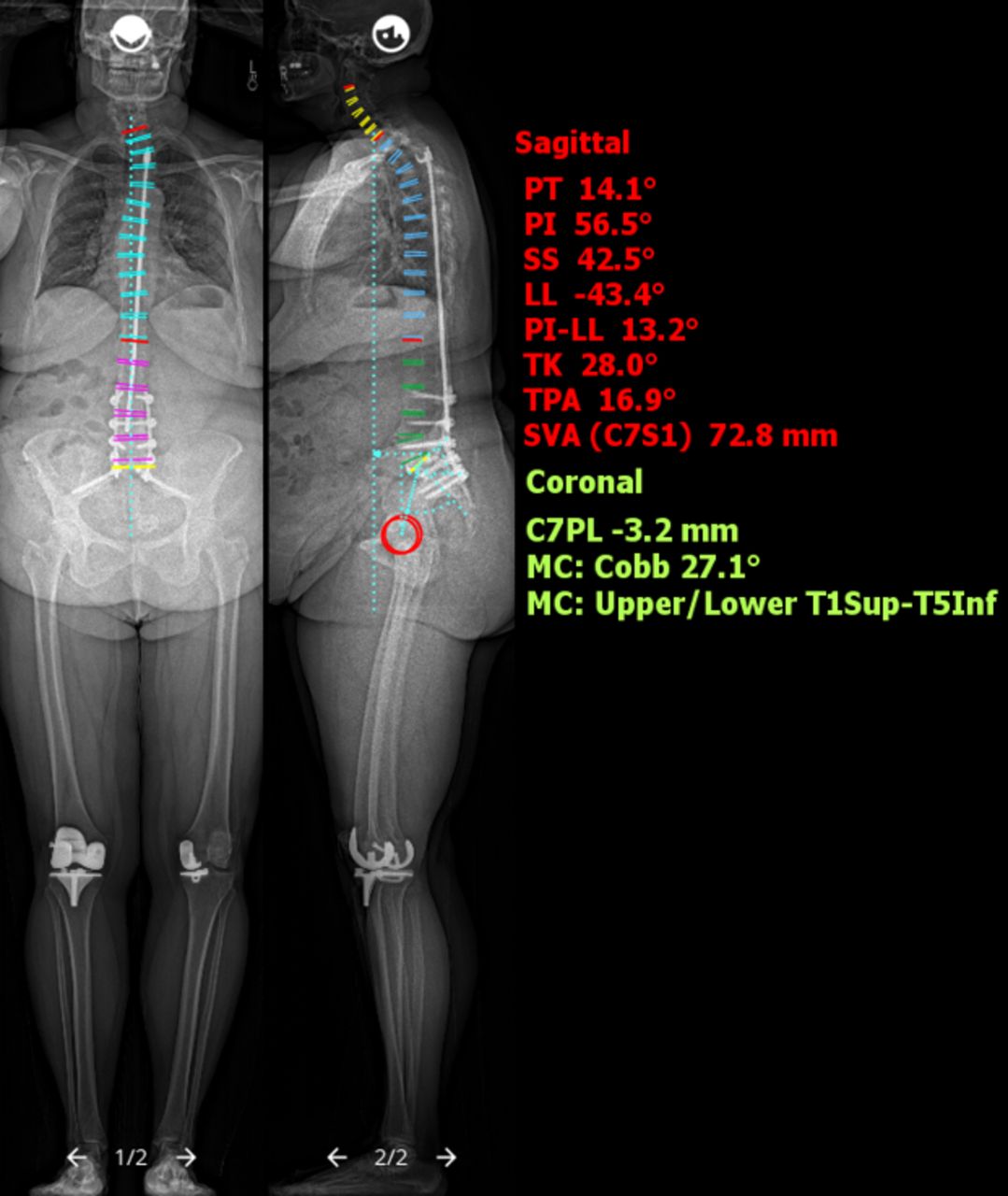
Case 2: EOS ImagingTM (Electro Optical System) full-length spine radiographic images after stage II posterior reconstruction revealed significant improvement in lumbar lordosis and sagittal parameters. PT, sagittal pelvic tilt; PI, pelvic incidence; SS, sacral slope; LL, lumbar lordosis; PI-LL, PI-LL mismatch; TK, thoracic kyphosis; TPA, T1 pelvic angle; SVA, sagittal vertical axis; C7PL, C7 plumb line; MC, major Cobb angle.
Although we had planned to perform an anterior interbody fusion at the L4-L5 level as well, at surgery, we found that the left common iliac vein was draped directly onto the osteophyte at this level, and as such, we elected not to perform it to avoid injuring the vein.
The patient recovered well and reported a notable improvement in her lower back pain and posture postoperatively.
With the robotic preoperative planning software, we are able to include possible instrumentation trajectories at extra levels as well as alternative trajectories in our plan, which included, in cases 1 and 2, one level above and fixation into the pelvis below. This highlights one of the advantages of robotic assistance over other techniques as navigation and fluoroscopy guidance providing advance preparation for potential worst surgical case scenarios by not having to figure out trajectories and alternatives intraoperatively.
Case 3—Revision Cervical Spine Reconstruction With Pedicle Screws
In this final case, we highlight the utilization of preoperative planning and robotic assistance for the insertion of cervical pedicle screws in the setting of altered anatomic landmarks. The patient is a 77-year-old man who presented with 12 months of severe functional disability, neck pain, bilateral upper extremity radicular symptoms, and a chin-on-chest deformity. He had previously undergone 2 cervical spine procedures involving instrumentation and fusion via both the anterior and posterior approaches and had autofusion of the adjacent levels immediately cranial to the surgically fused levels. The clinical picture was consistent with a postlaminectomy cervical kyphosis with chin-on-chest deformity.(Figures 11–13)

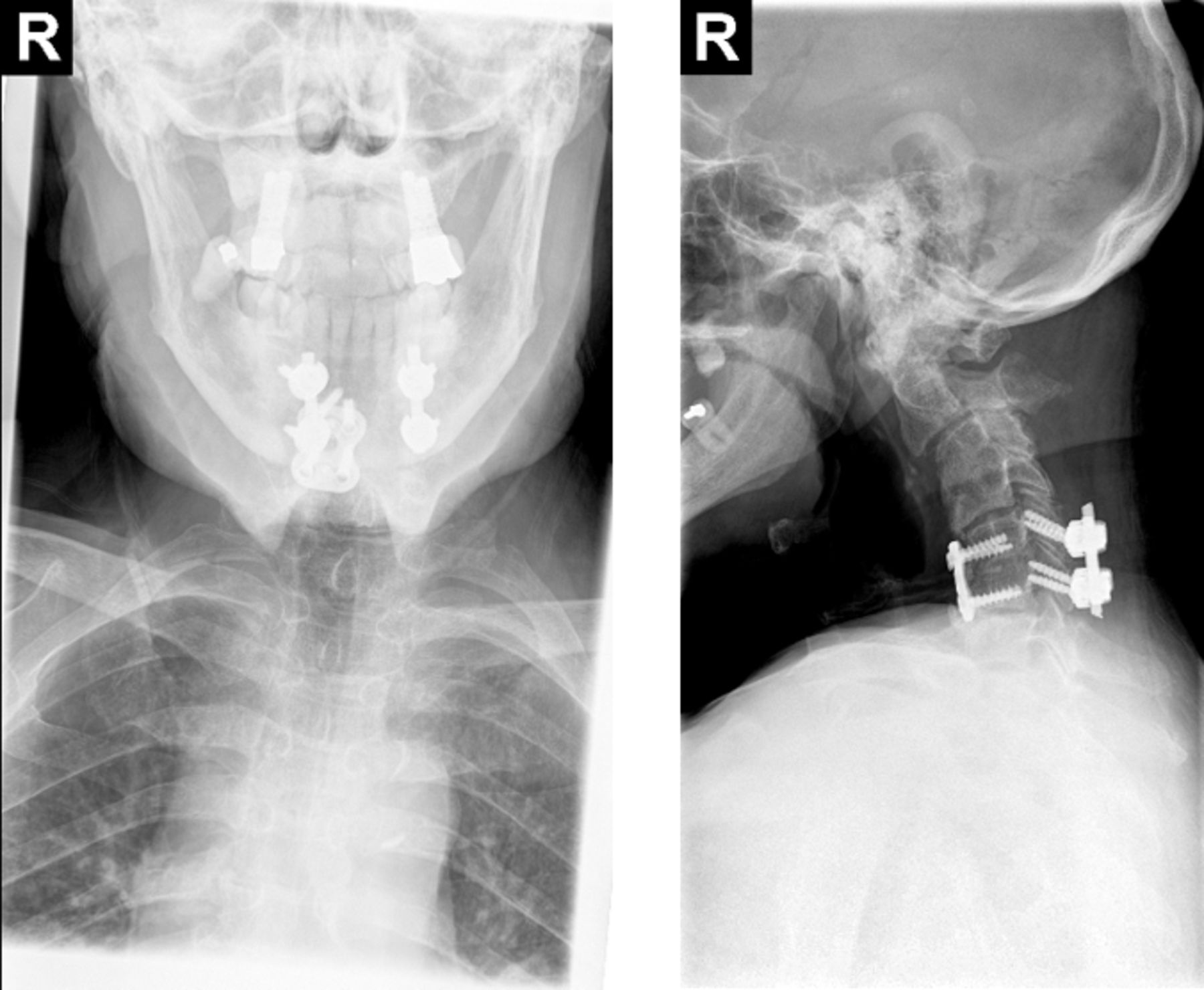
Case 3: Cervical spine anteroposterior and lateral radiographs demonstrate kyphotic sagittal alignment of the cervical spine with a grade II anterolisthesis of C2 on C3, autofusion of C3 and C4, and retrolisthesis of C4 on C5. Prior instrumented fusion of C5-C6 with anterior plating and posterior lateral mass screw that appeared to be intact.
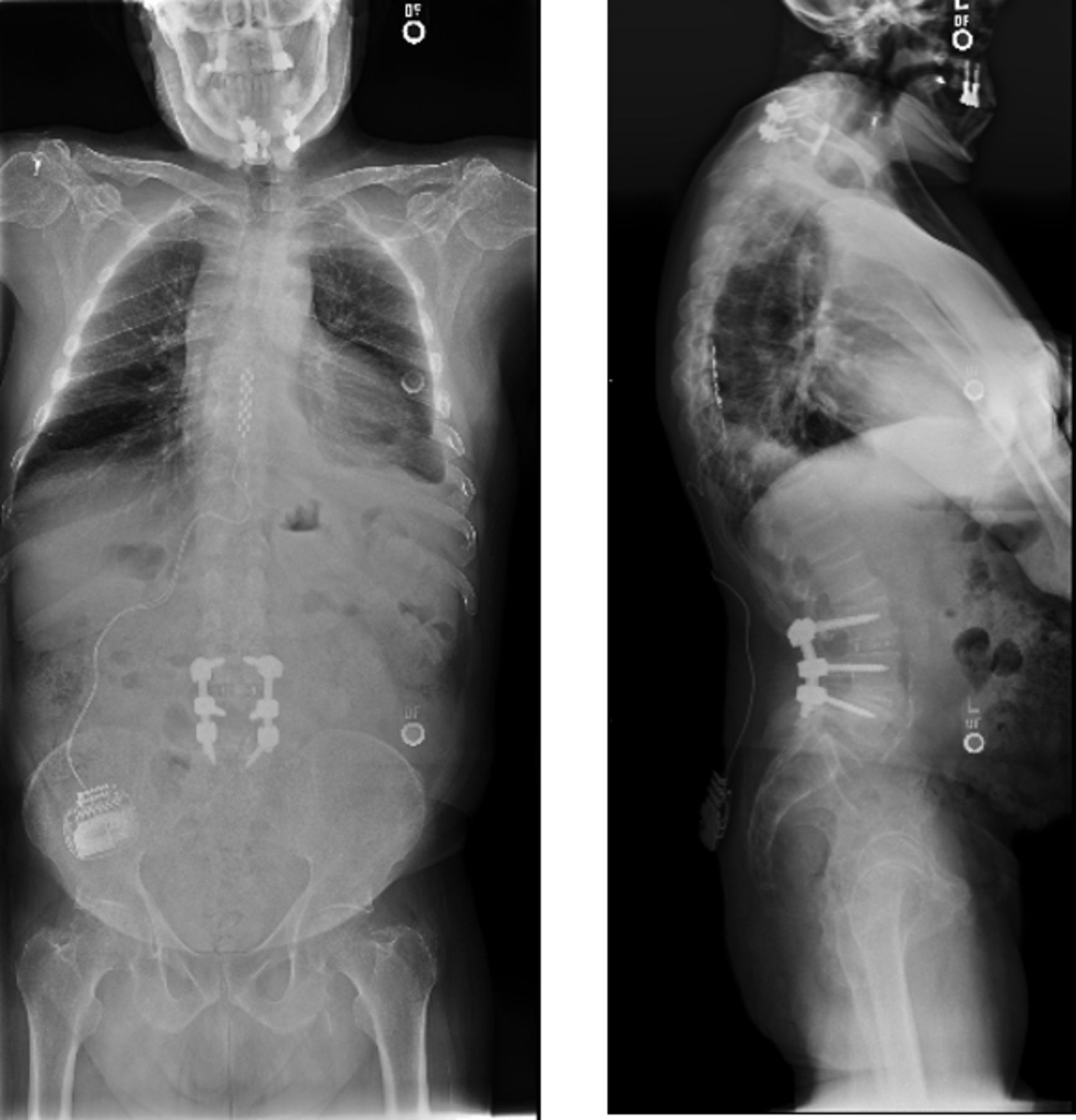
Case 3: Full-spine radiographs demonstrate the patient’s chin-on-chest deformity.

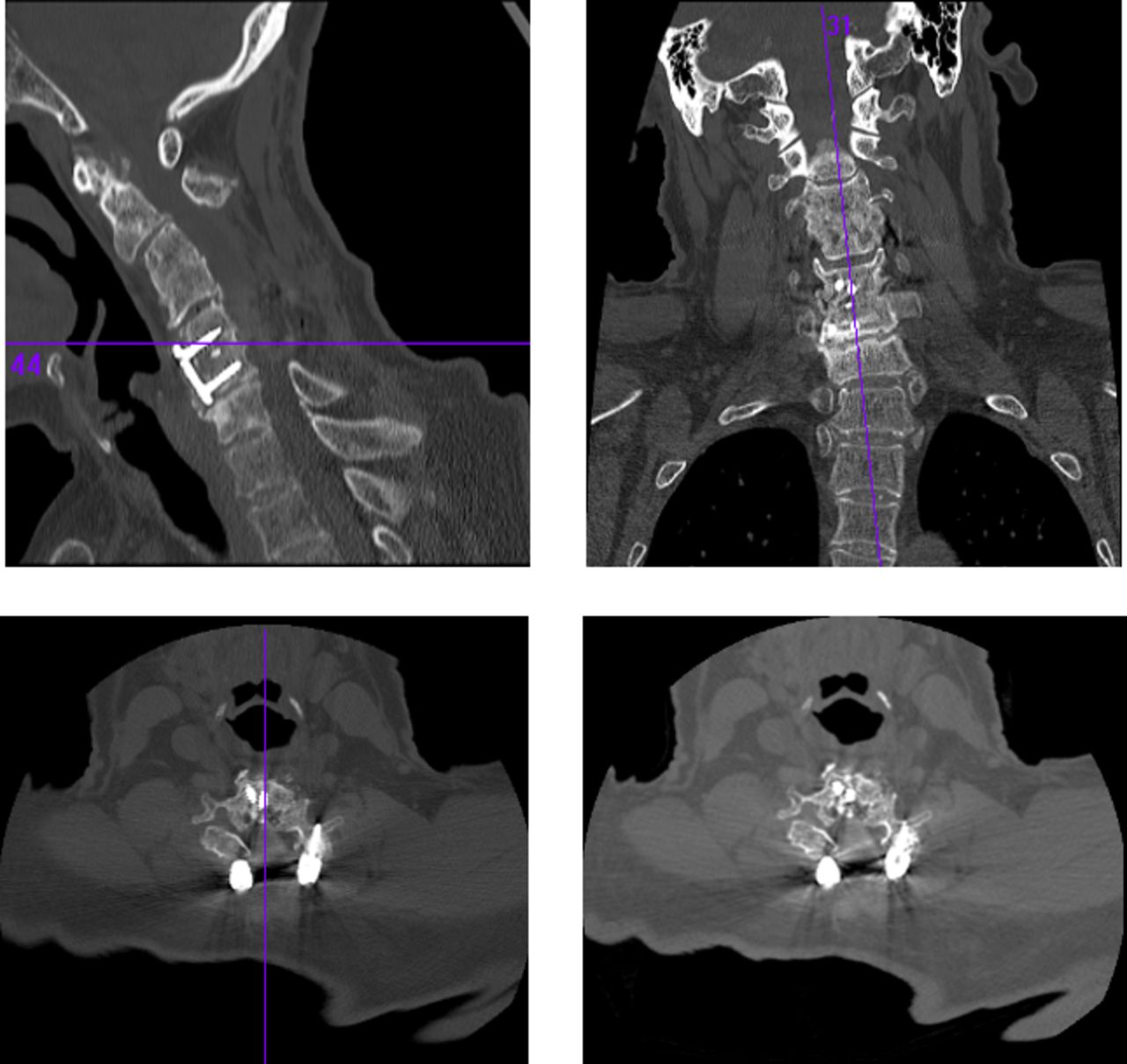
Case 3: Preoperative cervical spine computed tomography images. The images showed loss of disc space height at C6-C7, evidence of laminectomies from C3 to C6, and evidence of autofusion at the C3-C4 level.
The patient underwent removal of his posterior instrumentation, multilevel Smith Petersen osteotomies to facilitate restoration of cervical lordosis, new cervical and thoracic pedicle screw instrumentation, followed by correction of his deformity and spinal fusion (Figures 14 and 15).
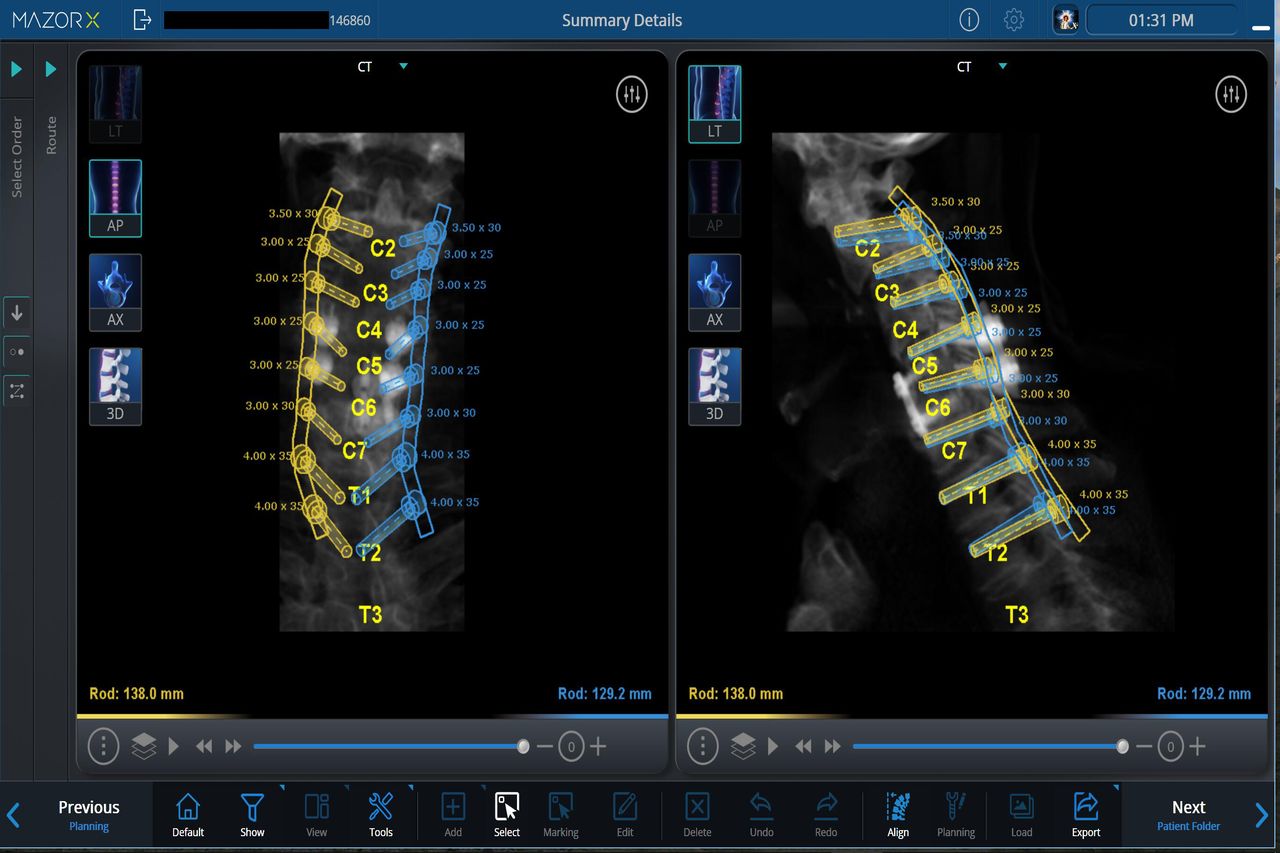
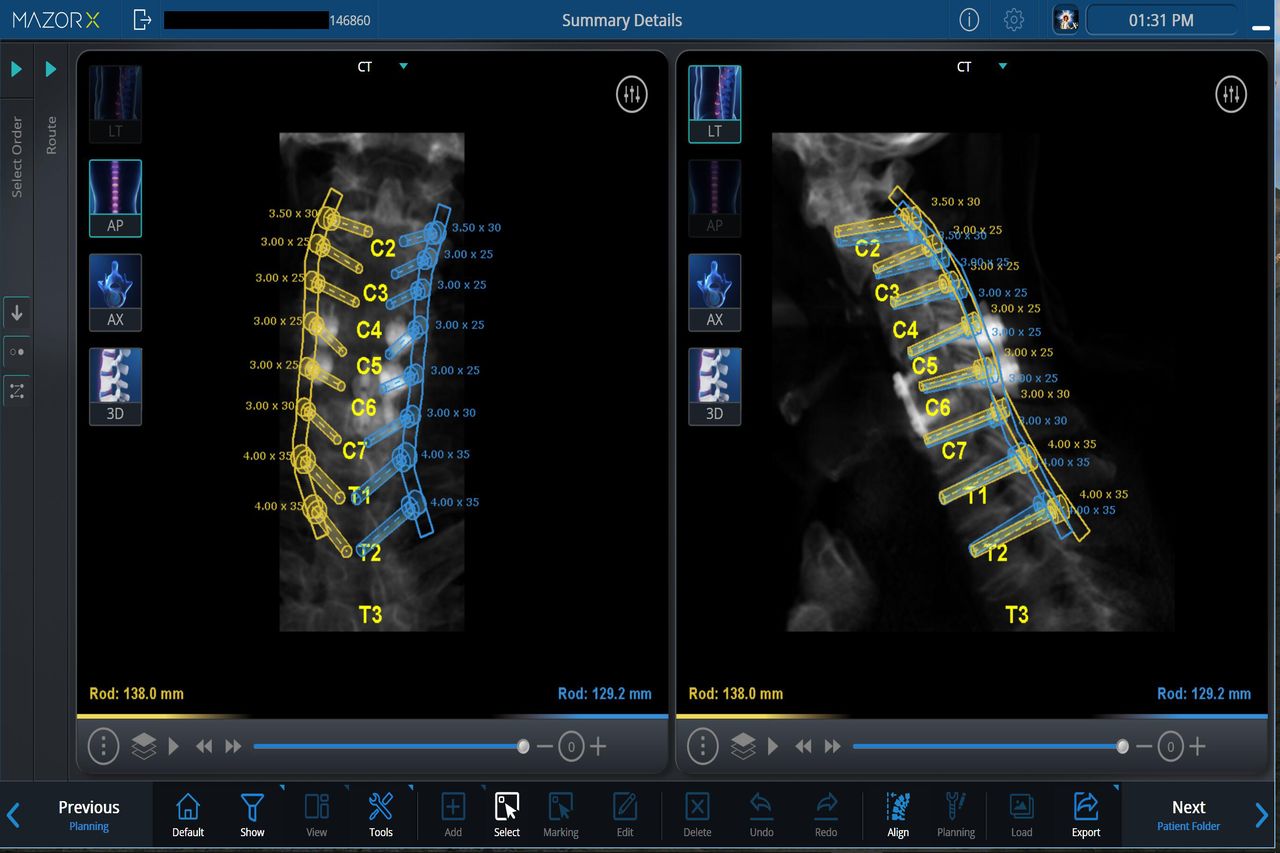
Case 3: Preoperative planning for robotic-assisted placement of cervical pedicle screws.
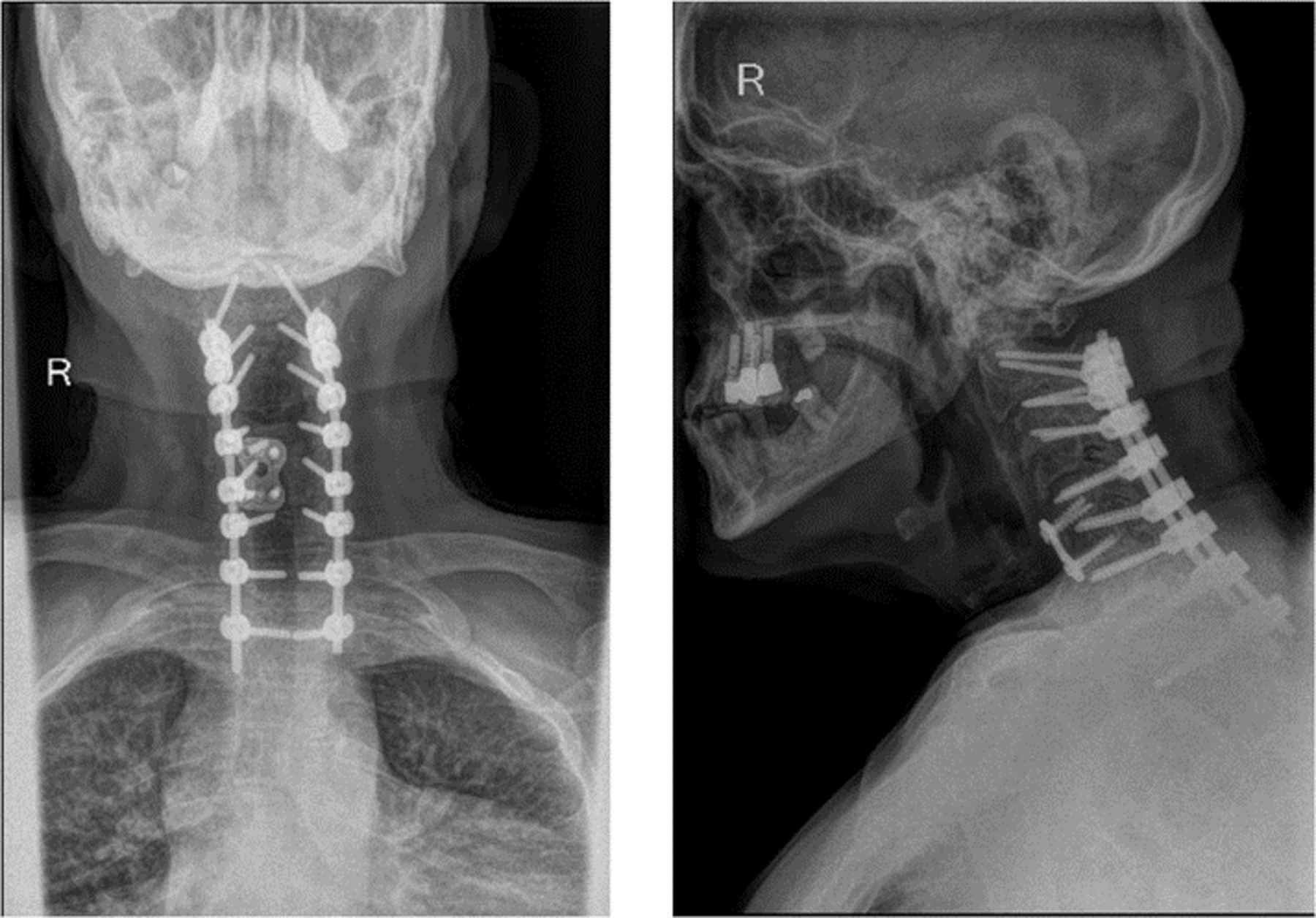
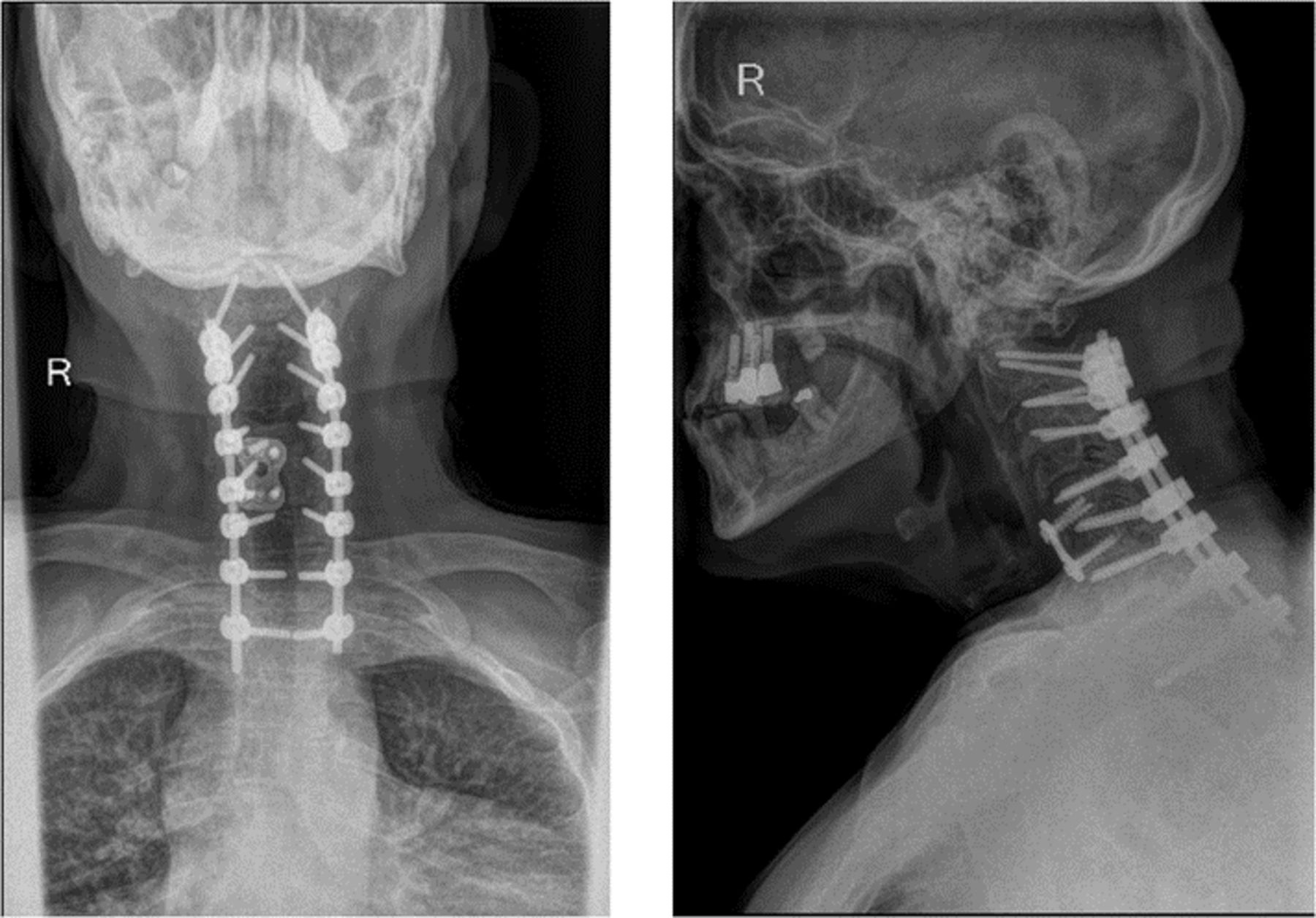
Case 3: Postoperative radiographic images show the final construct with pedicle screw fixation and deformity correction.
Cervical pedicle screws provide increased fixation and greater correction potential19 than lateral mass screws, but they have a high risk trajectory due to the adjacent neurovascular structures. This unique case is further complicated by distorted cervical spine anatomy as a result of both previous cervical spine surgeries and end-stage degeneration. Computer-assisted robotic guidance technology provides the surgeon with a safe and reproducible way to efficiently perform the procedure. Preoperative planning using the robotic software and the intraoperative registration processes improve the robot’s ability to localize the cervical pedicle screw trajectories accurately even in the face of complex, distorted anatomy, and prior screw paths.
The patient tolerated and recovered from the procedure well. His postoperative imaging revealed substantial cervical spine deformity correction (Figure 16). He reported significant improvement in his posture and neurologic symptoms with some predictable limitations associated with lost cervical range of motion.

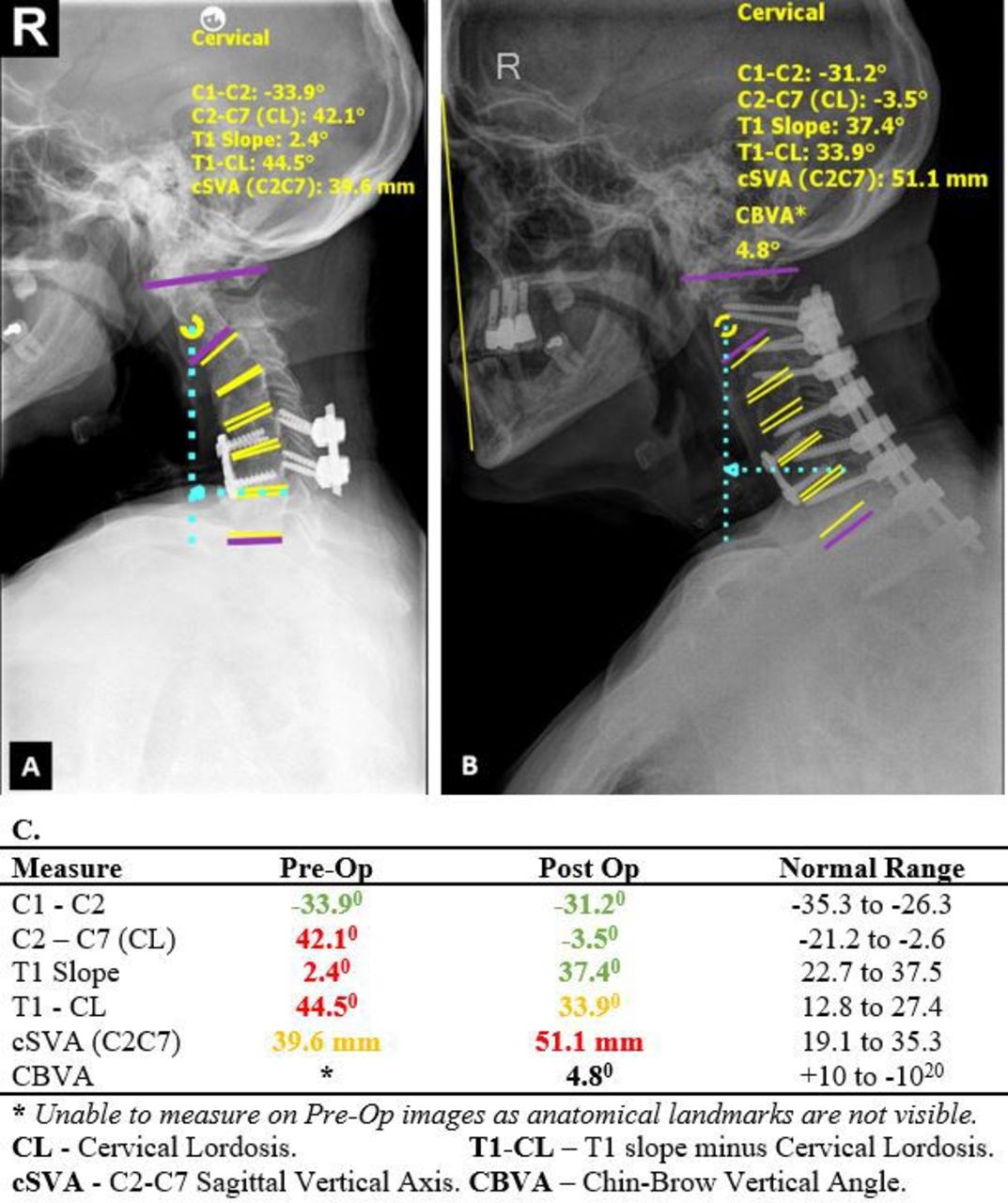
Case 3: Pre- and postoperative lateral radiographs demonstrate significant improvement in sagittal alignment (normal range for CBVA20.
CONCLUSION
While revision spine surgery presents a number of unique challenges, robotic assistance facilitates the safe and reproducible placement of instrumentation in this setting. However, as highlighted by the preceding cases, the advantages of the robotic platform extend well beyond instrumentation placement. Preoperative planning and intraoperative registration allow the surgeon to “visualize the invisible” and accurately predict deformity correction. Ultimately, the full capabilities of RSS will extend well beyond screw placement and allow the surgeon to perform all aspects of complex procedures with not yet appreciated reproducibility, safety, and accuracy.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosures and Conflicts of Interest Alexander M. Satin reports royalties and consulting fees from DeGen Medical, Inc; payment for expert testimony for the U.S. Department of Justice; a leadership or fiduciary role in the NASS Patient Safety Committee and the CSRS Publication Committee; and stock/stock options from Agada Medical. Stanley Kisinde reports no disclosures. Isador H. Lieberman reports consulting for Bioventus, ECential Robotics, Medtronic, Safe Orthopaedics, and SI-Bone; royalties from Globus Medical and SI-Bone; and serving on the scientific advisory board for SI-BONE.
Disclosure The authors report no financial disclosures related to this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.