


Abstract
Background The effects of epidural steroid (ES) administration following open or minimally invasive surgery lumbar discectomy have been extensively studied. However, no research has investigated the impact of steroids following the unilateral biportal technique endoscopic lumbar discectomy (UBE-D) for lumbar disc herniation. This study aims to evaluate the efficacy of ES administration in controlling postoperative pain and disability scores following UBE-D for single-level lumbar disc herniation.
Methods This double-blind, randomized, placebo-controlled trial was conducted between June 2021 and June 2023. Eighty-two patients were assessed, and 60 were eligible and randomized to receive either ES (n = 30) or saline (placebo; n = 30) after UBE-D. The Outcome measures included visual analog scale scores for pain, Oswestry Disability Index scores, morphine consumption over 24 hours, serum C-reactive protein levels, and the occurrence of complications over a 6-month follow-up period.
Results The baseline characteristics were comparable between the 2 groups, with no significant differences observed. Analysis of visual analog scale scores for back and leg pain, as well as Oswestry Disability Index scores, at various postoperative time points (6 hours, 12 hours, 24 hours, 2 weeks, 6 weeks, 3 months, and 6 months), showed no statistically significant differences between the ES and placebo groups (P values ranged from 0.47–0.94). Additionally, no significant differences were found in morphine consumption within the first 24 hours postoperatively (P = 0.85), length of hospital stay (P = 0.36), or C-reactive protein levels at 24 hours and 3 weeks postoperatively (P values ranged from 0.54–0.79) between the 2 groups. Importantly, no postoperative or steroid-related complications were reported in either group within the 6-month follow-up period.
Conclusions ES administration after UBE-D did not significantly reduce postoperative pain, disability scores, or morphine consumption compared with placebo. The findings suggest that routine use of ESs in this context may not provide additional benefits.
Clinical Relevance Clinicians should reconsider the use of epidural steroids as part of standard postoperative management after UBE-D, as the lack of significant improvement in patient outcomes indicates that alternative pain management strategies may be more effective.
Level of Evidence 1.
INTRODUCTION
Lumbar disc herniation is a prevalent issue in the middle-aged population and significantly impacts quality of life. Back pain and leg pain arise from both compression and the inflammation process initiated by disc herniation. Spontaneous regression of herniated disc tissue can indeed occur in most patients, with approximately 60% to 90% of individuals experiencing relief through conservative strategies.1–4 These strategies include bed rest, exercise, epidural steroid (ES) injections, medications, and physical therapy. If pain persists despite conservative treatment, lumbar discectomy may be recommended to alleviate compression of the disc. However, the persistent pain following lumbar disc herniation results from ongoing compression and inflammation processes, leading to peridural fibrosis. This pain may even worsen after surgery due to surgical trauma to connective tissue, dura, and nerve roots. Various methods, including oral administration, patient-controlled analgesia, local anesthetics, ES injection, and early physical therapy, have been employed to reduce postoperative pain in lumbar discectomy.5–7
Furthermore, current evidence indicates that corticosteroids possess an analgesic mechanism, working to reduce pain sensitization by inhibiting sensory transmission through nociceptive C-fibers at dorsal root ganglion cells in rat neurons.8 This mechanism has been shown to significantly decrease postoperative radicular pain when administered via epidural injection after both open and microsurgery lumbar discectomy.1,2,9,10 Previous meta-analyses have consistently suggested that intraoperative ES administration may provide benefits, including the reduction of pain and the shortening of hospital stays following lumbar disc herniation surgery.10–12
Endoscopic spine surgery has evolved into a practical, minimally invasive technique for decompression in patients with spinal disc herniation. Endoscopic spine discectomy can be categorized based on its endoscopic properties. Percutaneous endoscopic (full-endoscopic) procedures are typically characterized using a working channel endoscope, where the working channel and the optics are integrated into the same tubular device. Another category is the biportal endoscopic system, which features separate optical and working channels.13
In the preceding 2 randomized controlled trials (RCTs)1,2 investigating the effects of perioperative ES administration after percutaneous endoscopic lumbar discectomy (PELD), Shin et al2 concluded that ES injection may reduce postoperative pain, while Keorochana et al1 found no significant difference between groups. However, both trials had small sample sizes, focused solely on the percutaneous endoscopic group, and administered the steroid intraoperatively, potentially leading to the steroid extinguishing beyond the operating field due to irrigating fluid. Therefore, our study represents the first RCT focused on ES administration through catheterization in unilateral biportal endoscopic discectomy (UBE-D). It was designed to assess postoperative pain, disability scores, and morphine consumption. Additionally, the investigation was conducted to compare UBE-D with a placebo for the treatment of single-level lumbar disc herniation.
MATERIALS AND METHODS
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and received ethical approval from the Thammasat University Ethics Committee (protocol ID: MTU-EC-OT-0-247/64). Written informed consent was obtained from all participants. The study was registered at ThaiClinicalTrials.org with the identifier TCTR20220826005. All procedures were executed by a single surgeon (R.A.). A total of 82 eligible patients at our institution, all of whom had a diagnosed herniated disc, underwent assessment.
Study Population
A double-blinded, randomized, placebo-controlled trial was conducted at Thammasat University Hospital, Thammasat University, from June 2021 to June 2023. All participants were enrolled by an orthopedic spine surgeon (R.A.) and included in the study if they met the following criteria: the patient had radiculopathy (pain or neurological deficit) lasting for at least 12 weeks and had failed conservative treatment; lumbar disc hernia confirmed by magnetic resonance imaging in accordance with clinical findings; and the patient was willing to participate and provided consent. Patients were excluded if there were spinal stenosis, segmental instability, or spondylolisthesis; any previous lumbar surgery at the affected level; underlying diseases (immunocompromise, diabetes mellitus, or chronic medical illness); vertebral fracture, spinal tumor, or infection; or a history of steroid allergy.
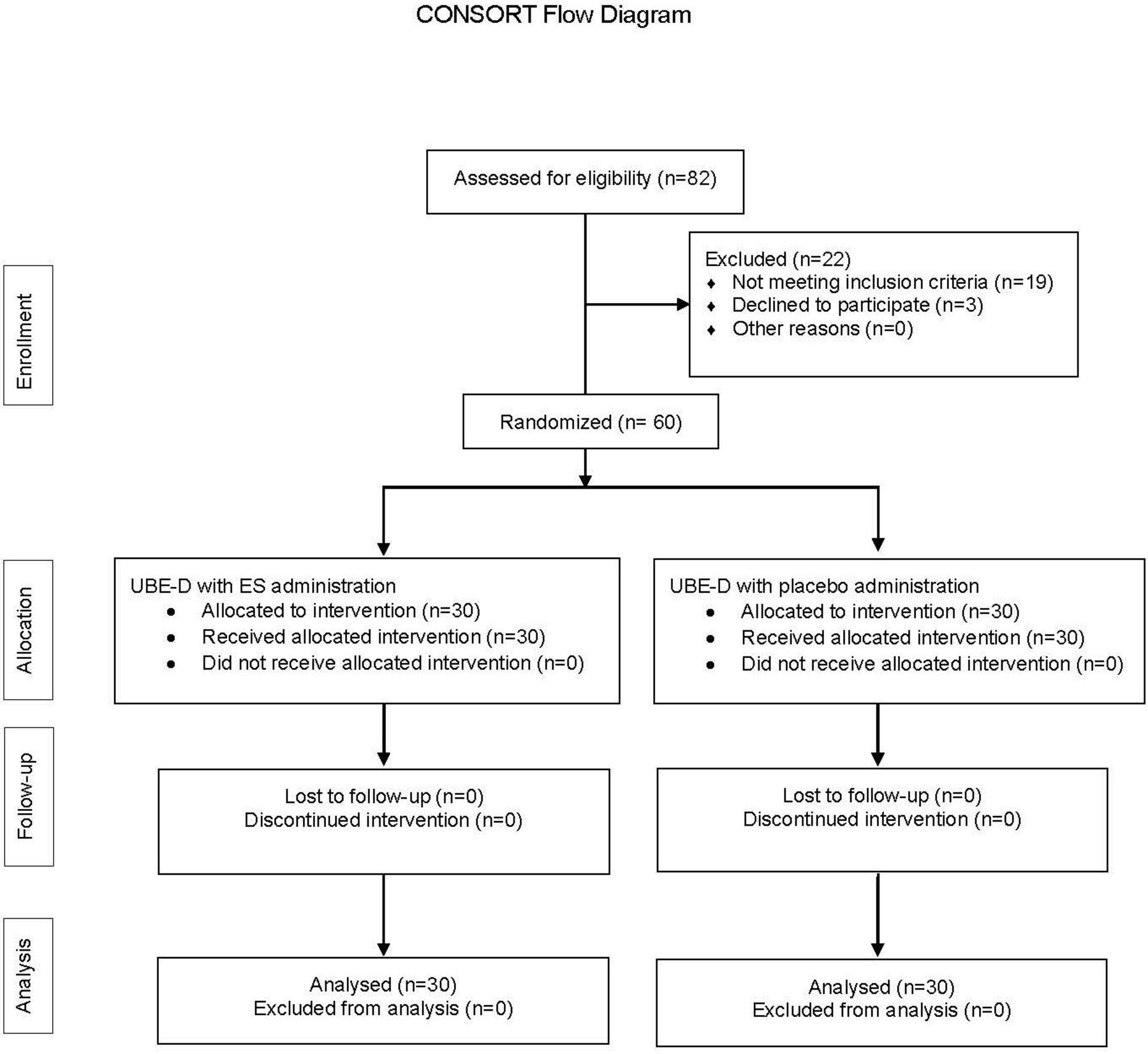
Nineteen patients who did not meet the inclusion criteria and 3 who refused to participate in the study were excluded, resulting in a total of 60 registered patients(Figure 1). Eligible participants were randomly assigned to receive either ES or saline (placebo) after UBE-D. Block randomization was performed using a computerized sequence generator with a ratio of 1:1 and a block size of 4. This process was overseen by T.B., who was not involved in patient recruitment or data collection. Stata (version 15) was used to generate random sequence lists. The surgeon (R.A.) and patient were blinded to group assignment.

Consolidated Standards of Reporting Trials (CONSORT) flow diagram. ES, epidural steroid; UBE-D, unilateral biportal endoscopic discectomy.
Demographic data and postoperative assessments were collected by the research assistant who was not involved in the group assignment or the study protocol. The assessed outcomes included visual analog scale (VAS) scores for leg and back pain, Oswestry Disability Index (ODI) score,14 morphine consumption, and complications (urinary retention, wound difficulties, and symptom recurrence) at 6-month follow-up.
Surgical Technique and ES Administration
A single orthopedic spine surgeon (R.A.) executed identical procedures on all patients. Prior to the surgery, each patient received a prophylactic antibiotic in the form of a 2 g injection of cefazolin administered 30 minutes before the commencement of the procedure. Following anesthesia, patients were positioned in the prone posture, with the knee joint flexed in the range of 15° to 30° and hip flexion between 20° and 40° degrees.
Under fluoroscopic guidance, 2 separate 5- to 6-mm stab skin incisions were made just medial to the upper and lower pedicles of the index level. Before making the marked skin incisions, a standard sterile preparation was conducted. The portal was carefully created to allow adequate instrument access through the superficial fascia, ensuring sufficient saline flow. A muscle detacher was employed to create space for water flow through a portion of the proximal lamina and the interlaminar space. In the left-sided approach, the upper portal served as the viewing portal, while the lower portal functioned as the working portal. An arthroscopic irrigation system was utilized in the procedure, enabling saline irrigation fluid to drain from the viewing portal to the working portal.
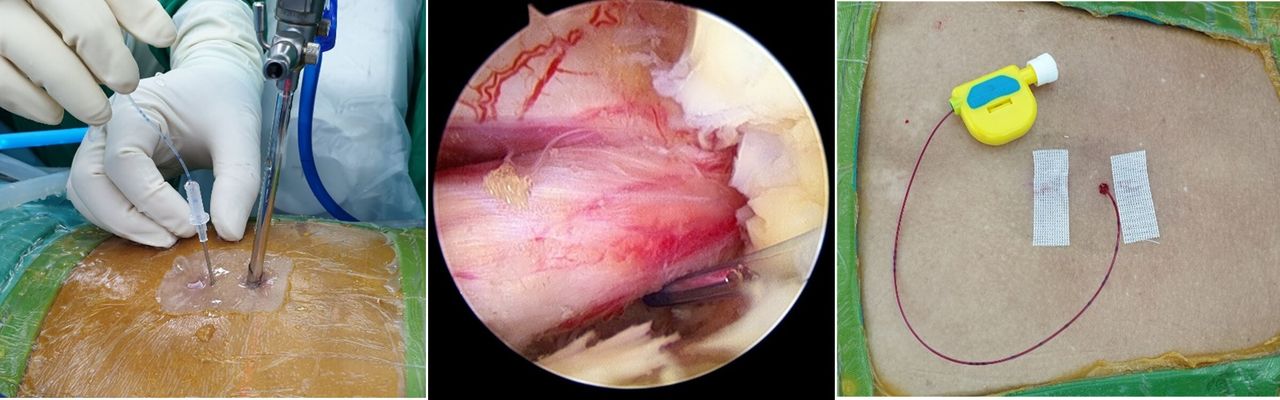
Ipsilateral laminotomy was performed using a high-speed burr. The ligamentum flavum covering the dura and nerve root was removed, and discectomy was performed under endoscopic view. Before closing the wound, we placed the epidural catheter inside the interlaminar space, ensuring the catheter’s tip was near the traversing nerve root. Subsequently, wound closure was performed (Figure 2).

The 12-gauge, 50-mm needle was inserted through the patient’s skin into the interlaminar space near the traversing nerve root. Subsequently, the epidural catheter was threaded through the needle, positioning its tip proximate to the traversing nerve root. Following the closure of the wound, either the epidural steroid or placebo was injected for up to 2 hours postoperatively.
After the postoperative period of 2 hours, a solution was prepared by mixing 1 mL of triamcinolone (40 mg) with 4 mL of saline, and it was injected through the epidural catheter for each patient in the ES group. In contrast, each patient in the placebo group received an injection of 5 mL of saline through the epidural catheter. This procedure was conducted by a senior resident who was not involved in patient selection and assessment.
Postoperative Protocol
All patients received the same postoperative pain control protocol: Morphine intravenous, as needed for pain if visual analog scale >5; acetaminophen 500 mg orally every 6 hours; toperizone 2 mg orally twice per day with meals; naproxen 250 mg orally twice per day with meals; and gabapentin 300 mg orally at night. Patients were encouraged to progressively transition from bed to walking starting 4 hours postoperatively.
Statistical Analysis
The sample size estimation was based on the difference in the mean, with the minimal clinically important change of VAS for back pain set at 2.15 The SD between the ES group and the placebo group in our pilot study was 1.49 and 1.71, respectively. The sample size was calculated for a 2-sample comparison of means (2-tailed), assuming an alpha level of 0.05 and a power of 0.9. Thus, the sample size required for each arm of the study was 14 patients. To account for unexpected dropouts, the sample size was increased by 20%, resulting in 16 per group (a total of 32 patients).
Normally distributed continuous variables were reported as mean and SD and were compared using 2-sided independent 2-sample t tests. Categorical data were presented as percentages and compared using the Fisher exact test. Continuous outcomes, including VAS back and leg pain and ODI, were compared between treatment groups using a mixed linear regression analysis. An intention-to-treat analysis was used to compare variables between the 2 groups. All analyses were performed using STATA software version 15.0. A difference was considered statistically significant if the P value was less than 0.05.
RESULTS
Demographics
A comprehensive comparison of demographic data was conducted between the 2 study groups: the ES group and placebo group each consisted of 30 patients. The assessed demographic characteristics included sex, age, weight, height, body mass index, surgical level, operative time, preoperative C-reactive protein (CRP), and preoperative scores for VAS of back and leg pain, as well as ODI. In terms of gender distribution, the ES group had 43.3% men and 56.7% women, compared with 33.3% men and 66.7% women in the placebo group (P = 0.592). The mean age for the ES group was 49.2 years (SD 15.28) and 53.03 years (SD 11.64) for the placebo group (P = 0.271). Similarly, no significant differences were observed in weight, height, or body mass index between the 2 groups (P = 0.261, 1.138, and 0.861, respectively).
The surgical-level distribution demonstrated no statistically significant differences, with most cases involving L4/L5 in both groups. Operative time also showed no significant distinction between the ES and placebo groups (P = 0.631). Preoperative CRP levels exhibited no significant difference between the 2 groups (P = 0.851). Analysis of preoperative scores, including VAS for back pain, VAS for leg pain, and ODI, did not reveal statistically significant differences (P values of 0.151, 0.821, and 0.121, respectively; Table 1).
Comparison of demographic data between the 2 study groups.
Visual Analog Score and Oswestry Disability Index
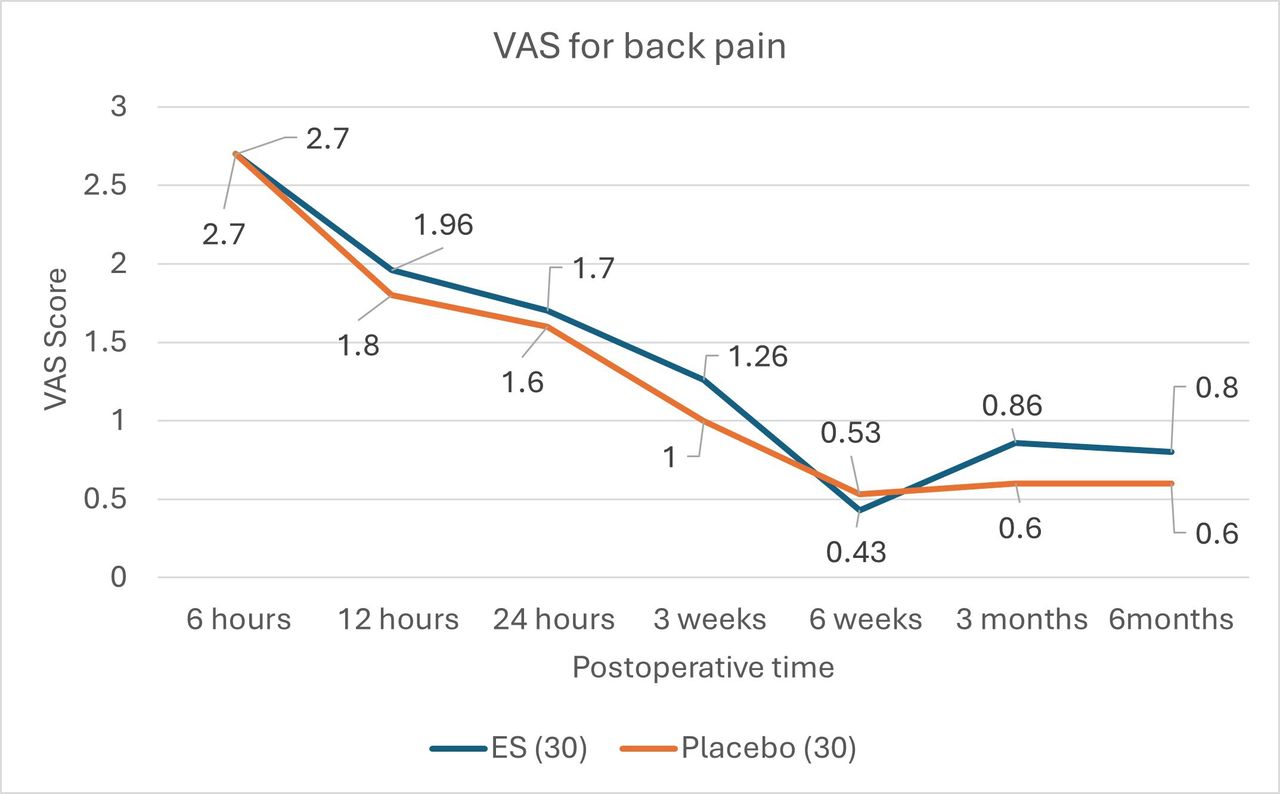
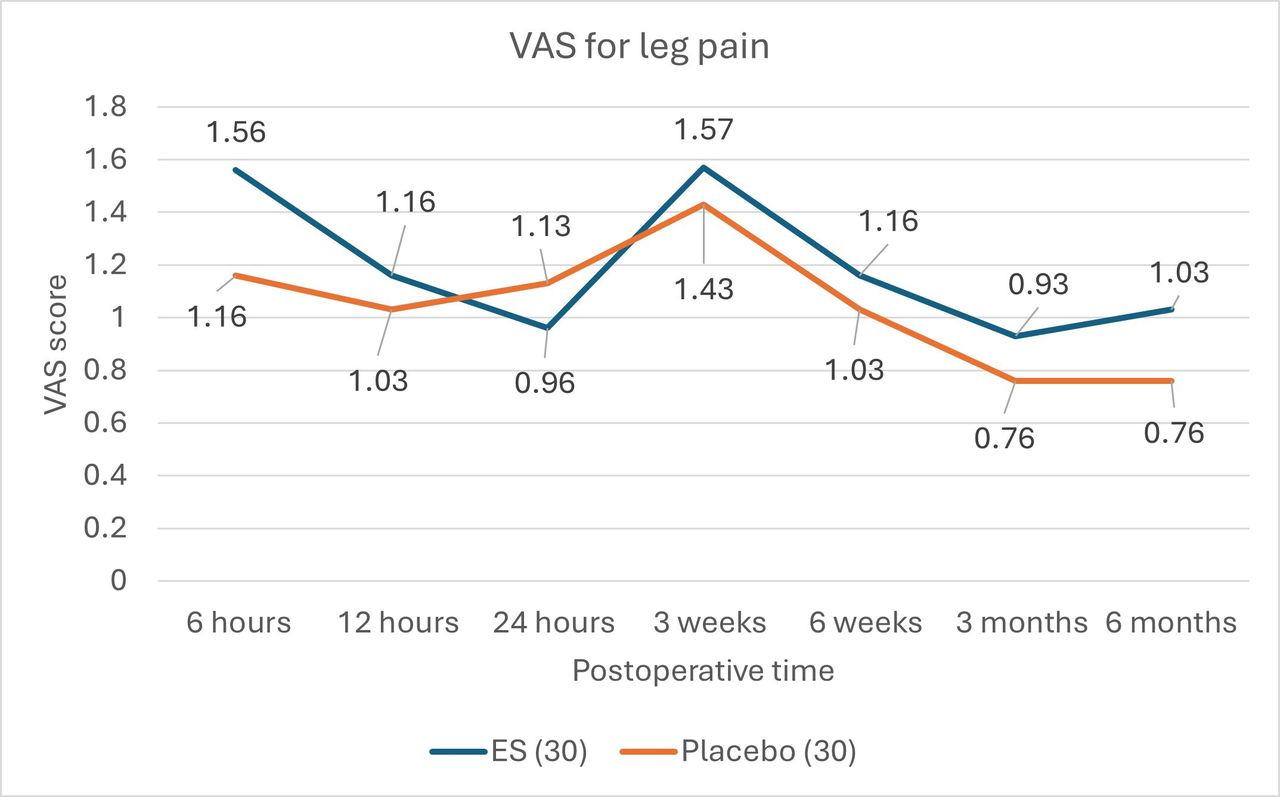
The comparison of VAS and ODI scores between the 2 study groups revealed that VAS back pain scores at various postoperative time points, including 6 hours, 12 hours, 24 hours, 3 weeks, 6 weeks, 3 months, and 6 months, showed no statistically significant differences between the ES and placebo groups (P values ranging from 0.5–0.94). Similarly, VAS leg pain scores at the same time points did not show significant distinctions between the 2 groups (P values ranging from 0.6–0.86). The analysis of ODI scores at 3 weeks, 6 weeks, 3 months, and 6 months postoperatively also did not reveal significant differences between the ES and placebo groups (P values of 0.47, 0.97, 0.87, and 0.75, respectively; Table 2; Figures 3–5).

Mean values of VAS of back pain after unilateral biportal endoscopic discectomy. VAS, visual analog scale; ES, epidural steroid.

Mean values of VAS of leg pain after unilateral biportal endoscopic discectomy. VAS, visual analog scale; ES, epidural steroid.

Mean values of ODI after unilateral biportal endoscopic discectomy. ODI, Oswestry Disability Index; ES, epidural steroid.
Comparison of VAS and ODI scores data between the 2 groups.
Outcomes and Complication
The first 24-hour morphine consumption level, measured in milligrams, showed a mean of 1.3 (SD 2.32) for the ES group and 1.2 (SD 1.86) for the Placebo group, with no statistically significant difference observed (P = 0.854). The postoperative length of hospital stay, measured in days, revealed a mean of 1.53 (SD 0.56) for the ES group and 1.4 (SD 0.56) for the placebo group, demonstrating no significant distinction between the 2 groups (P = 0.366).
Analysis of CRP levels at 24 hours postoperatively displayed a mean of 7.824 (SD 7.03) for the ES group and 7.25 (SD 9.9) for the placebo group, with no statistically significant difference noted (P = 0.79). Similarly, at 3 weeks postoperatively, CRP levels showed a mean of 3.715 (SD 6.34) for the ES group and 5.07 (SD 10.57) for the placebo group, without significant differences between the groups (P = 0.549). Regarding complications within 6 months postoperatively, both groups reported zero instances of postoperative complications or steroid-related complications (Table 3).
Comparison of outcomes and complications between the 2 groups.
DISCUSSION
The anti-inflammatory potency of corticosteroids has been well-recognized for more than 70 years. These agents exert their anti-inflammatory effects primarily through the inhibition of phospholipase A2. This enzyme is responsible for converting membrane phospholipids into arachidonic acid, which subsequently leads to the production of various proinflammatory mediators.16
In previous studies, ES following lumbar disc herniation surgery has emerged as a promising intervention for pain reduction. A comprehensive systematic review by Jamjoom et al,10 encompassing 16 research studies, including RCTs and cohort studies, examined the efficacy of ES in postoperative pain control. The collective findings underscore the potential of ES to alleviate early postoperative pain and reduce the need for pain medication, all without a concomitant increase in complications. Ranguis et al9 contributed to the body of knowledge through a systematic review involving 12 RCTs, focusing on the application of ES after surgery for degenerative spine disease. The discerning results demonstrated that ES exhibits a notable capacity to mitigate back pain at 12 to 24 hours postoperation and radicular pain at 1 week to 1 to 2 months postoperation. Furthermore, ES was associated with a reduction in postoperative analgesic consumption and a shortened length of hospital stay. Arirachakaran et al17 conducted a comprehensive systematic review and meta-analysis examining the impact of ES administration in lumbar discectomy compared with placebo. Their findings revealed significant reductions in back pain at 1 week and 1 month, leg pain at 1 week and 1 month, and morphine consumption and hospital stay within the ES-treated group. However, in the context of surgical approaches, the study demonstrated that the conventional approach experienced a notable reduction in morphine consumption with ES, while the minimally invasive approach did not exhibit the same effect.
Our findings suggest that ES does not reduce postoperative pain, disability scores, or 24-hour morphine consumption compared with placebo after UBE-D in lumbar disc herniation. However, our results contrast with previous meta-analyses,9,10,17 which reported that intraoperative ES provides some benefits, such as reduced postoperative pain, decreased morphine consumption, and shortened hospital stays. Nonetheless, these meta-analyses have several limitations. Many of the included studies employed various methods of steroid administration, including oral, intravenous, and epidural routes. Additionally, the participants often had a combination of lumbar stenosis and lumbar disc herniation, and the surgical techniques varied widely, ranging from conventional surgery to minimally invasive procedures such as microdiscectomy or PELD.
Our results align with those of Keorochana et al,1 who conducted a double-blinded, randomized, placebo-controlled trial comparing postoperative morphine consumption and pain between ES and placebo in PELD. They found no statistically significant difference in morphine consumption and postoperative pain during the 1-month follow-up between the groups. This may be because postoperative pain, as measured by the VAS, is relatively low after endoscopic surgery due to the minimally invasive nature of the procedure.18 In biportal endoscopic surgery, the limited muscle dissection and minimal innervation damage involved in endoscopic discectomy likely contribute to reduced postoperative pain.
ES use is associated with rare but serious complications, including central nervous system issues such as spinal cord infarction, ischemic stroke, visual impairment, and paralysis. The primary mechanism thought to underlie these complications is embolic infarction, which may occur when the steroid unintentionally enters an artery. These adverse events are most often reported during ES injections performed with contrast media and C-arm guidance.16,19 Conversely, complications arising from steroid use during intraoperative endoscopy are extremely uncommon. In our study, we positioned the catheter close to the traversing nerve root under endoscopic direct visualization, thereby minimizing the risk of inadvertent intra-arterial injection of the steroid. Additionally, while steroids are known to potentially elevate the risk of postoperative wound infections, our findings did not support this, as no infections were observed. The endoscopic technique, being minimally invasive, coupled with constant fluid irrigation, likely helps in reducing the incidence of postoperative infections.
To the best of our knowledge, our study represents the first double-blind RCT that assessed UBE-D with the use of ES compared with a placebo to reduce postoperative pain, reduce morphine consumption, and improve disability scores. The limited existing literature on the use of ES in endoscopic discectomy has primarily focused on PELD with small sample sizes. Additionally, endoscopic surgical procedures necessitate the use of irrigating fluid to dilate the operating field and clear away debris and blood. In our study, we administered ES after wound closure using an epidural catheter, injecting the ES or placebo directly into the epidural space. This approach was adopted to prevent steroid dispersion beyond the operating field, which could occur due to fluid irrigation in endoscopic procedures.
Our study is not without limitations. First, the sample size calculation was conducted to assess the primary outcome and may not adequately represent secondary outcomes, including disability scores, morphine consumption, and serum CRP levels. Second, we did not evaluate nerve root inflammation intraoperatively, such as increased vascularity or redness. Lastly, this study specifically focused on UBE-D, and its findings may not be readily generalized to other techniques of minimally invasive surgery for lumbar discectomy.
CONCLUSION
The present study found that ES administration following UBE-D for single-level lumbar disc herniation did not result in significant improvements in postoperative pain, disability scores, or morphine consumption compared with placebo. The lack of statistically significant differences in key outcomes suggests that routine use of ESs in this context may not provide additional benefits. Consequently, their use for pain management after UBE-D should be reconsidered, and alternative strategies may need to be explored.
Acknowledgments
We thank Miss Benjamat Srising, who conducted the patient interviews for raw data collection.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Research Ethics The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Thammasat University (protocol code: protocol ID: MTU-EC-OT-0-247/64).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.