


Abstract
Background Yolk sac tumors (YST) are malignant neoplasms. They are a subtype of germ cell tumors and typically originate in the gonads although extragonadal origins of such tumors have been described. Yolk sac tumors are commonly found in the gonads of infants and children and are extremely rare in adults. The goal of this case report is to describe the clinical presentation of a rare case of metastatic extragonadal yolk sac tumor originating from the mediastinum and causing an acute conus medullaris syndrome in an adult male.
Methods A 47-year old male presented to our emergency department with a one-day history of bilateral lower extremity weakness, urinary retention and bowel incontinence. Imaging revealed a destructive lesion and a burst fracture of the first lumbar vertebral body (L1) with severe spinal canal stenosis. An urgent spinal decompression and fusion was performed. Oncologic workup revealed a yolk sac tumor originating from the mediastinum.
Results His neurologic function, including motor strength, bowel and bladder function improved in the postoperative period. Chemotherapy regimen of ifosfamide, etoposide and cisplatin was administered and radiation therapy was administered to the spine tumor bed.
Conclusions Yolk sac tumors, although rare, should be considered in the long list differential diagnosis of an otherwise healthy male presenting with conus medullaris or spinal cord compression from metastatic disease without evidence of a testicular mass. Prompt diagnosis with urgent decompression of neural structures and stabilization of the spine may result in improvement in neurological function.
Introduction
Yolk sac tumors (YST) are malignant neoplasms. They are a subtype of germ cell tumors. Germ cell tumors occur primarily in the gonads. In 1-5% of cases, these tumors originate in some specific extragonadal sites (notably midline structures from the pineal gland to the coccyx).1, 2 Yolk sac tumors are commonly found in the gonads of infants and children and are rare in adults.3 In this article, we describe the case of an extragonadal yolk sac tumor originating from the mediastinum and presenting as a burst fracture with acute cord compression in an adult male.
Case Report
History
A 47-year-old male with no past medical history was in his usual state of health when he presented to the Emergency Room (ER) with a one-day history of sudden-onset of bilateral lower extremity weakness, back pain, saddle anesthesia, urinary retention and loss of bowel function.
Examination
On examination, cranial nerve and upper-extremity neurological function were normal. Motor strength in the right lower extremity was grade 3 for hip flexors and quadriceps, and grade 4+ for tibialis anterior, extensor hallicus longus and gastrocnemius-soleus function. Motor strength in the left lower extremity was grade 3 for hip flexors, tibialis anterior, extensor hallicus longus and gastrocnemius-soleus and grade 4- for quadriceps function. Sensation was diminished to light touch in the T12-S3 dermatome bilaterally. Patella and achilles tendon reflexes were normal. No clonus was present. A Babinski's reflex was present bilaterally and the patient had a diminished rectal tone.
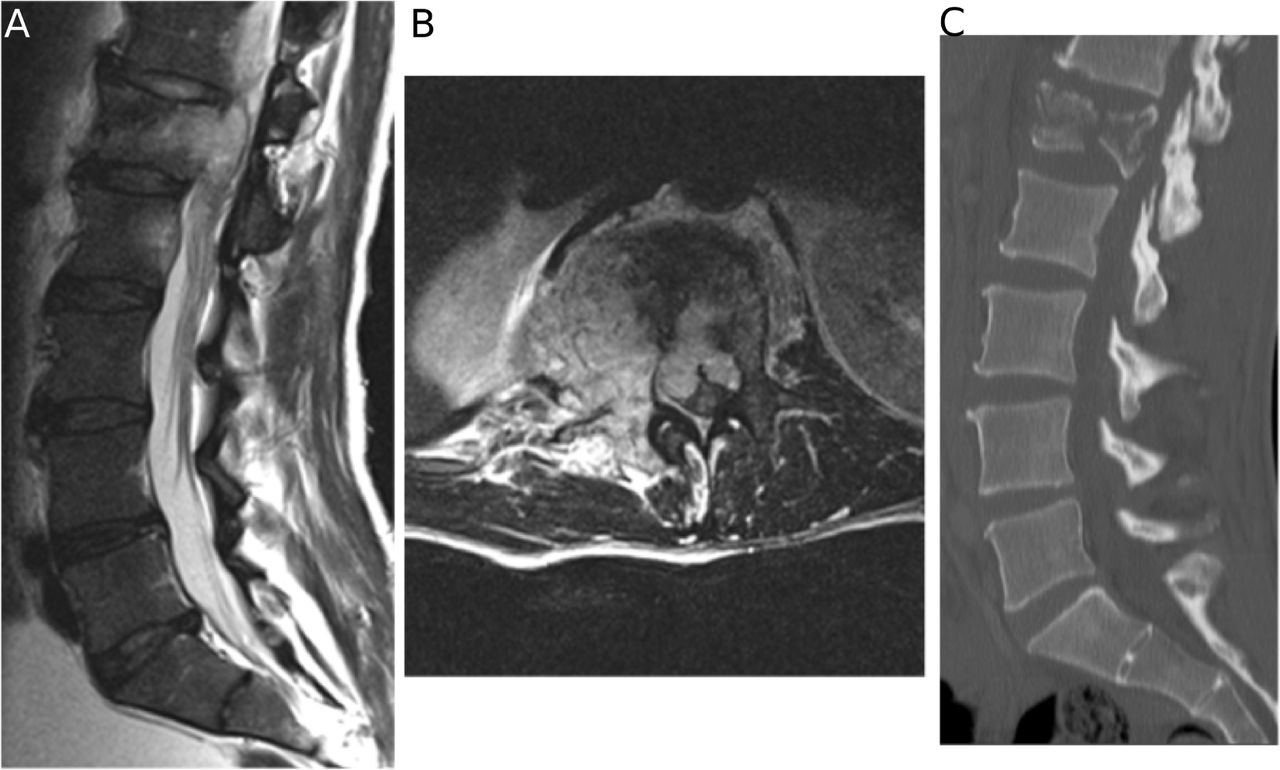
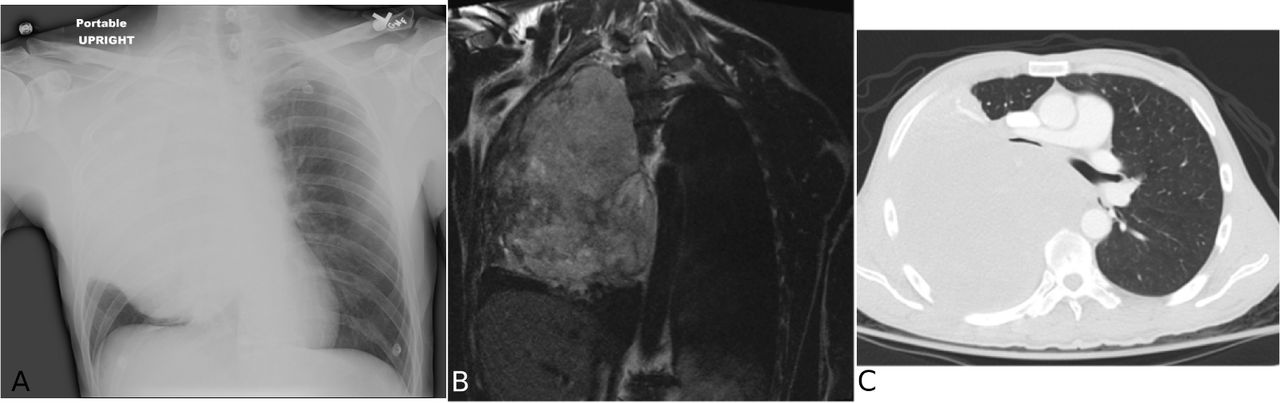
Magnetic resonance imaging (MRI) demonstrated a destructive mass lesion of L1 with epidural spread resulting in severe stenosis and compression of the conus medullaris. A pathologic burst fracture was also present at L1 (Figure 1). Chest computed tomography (CT) scan demonstrated a large right chest wall heterogeneous mass measuring 153 x 135 mm occupying the majority of right hemithorax and exerting considerable mass effect and compression on the trachea, atelectatic right lung, right mainstem bronchi, right lobar bronchi, right pulmonary artery, and the left atrium (Figure 2).
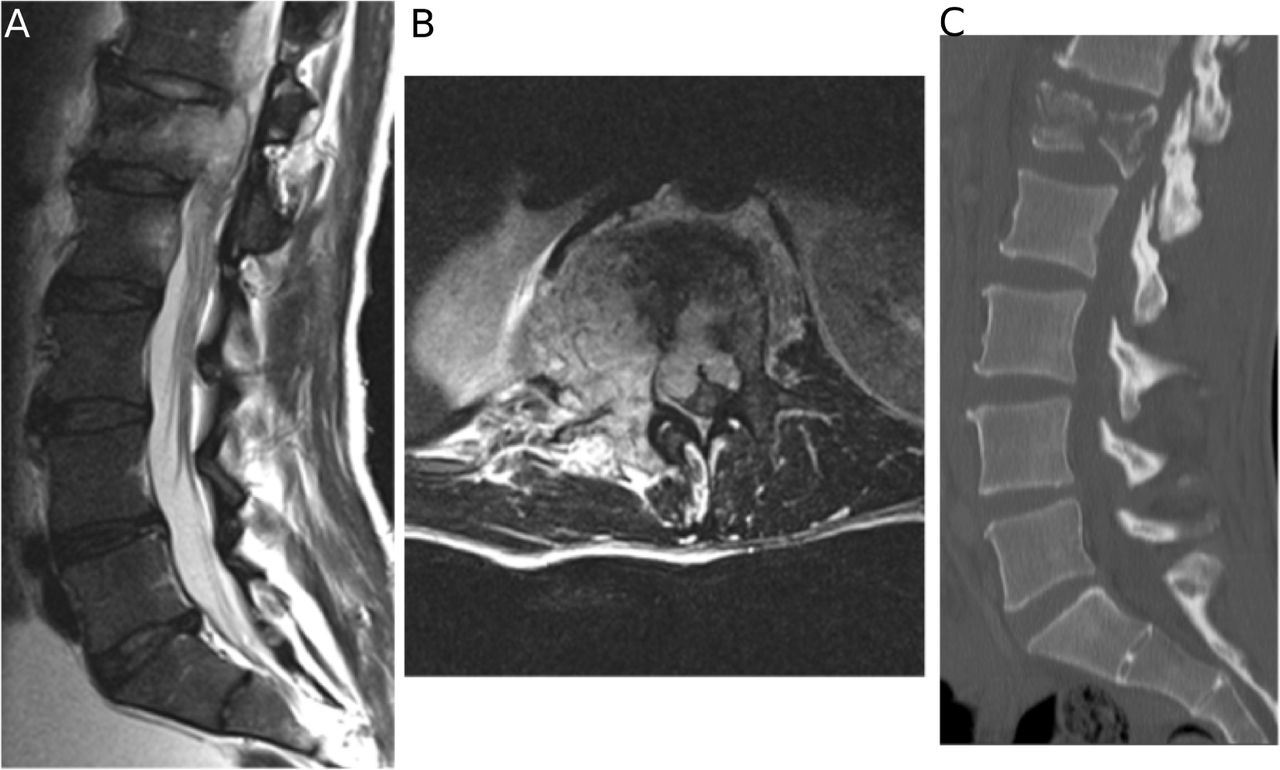
(A) Sagittal T2 and (B) axial T2 MRI demonstrating a destructive mass involving L1 with epidural involvement resulting in severe spinal canal stenosis. (C) Sagittal CT scan demonstrating a burst fracture of L1.
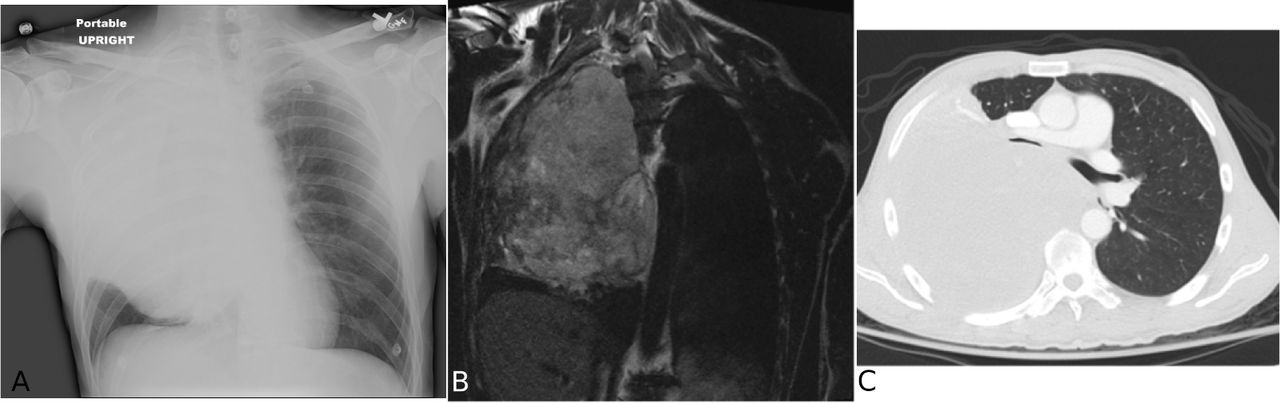
(A) Anterior-posterior chest x-ray (B) Coronal T2 MRI and (C) axial CT scan demonstrating a massive lesion in the right hemithorax obliterating the right lung and exerting considerable mass effect on the airway and vascular structures.
Operation and postoperative course
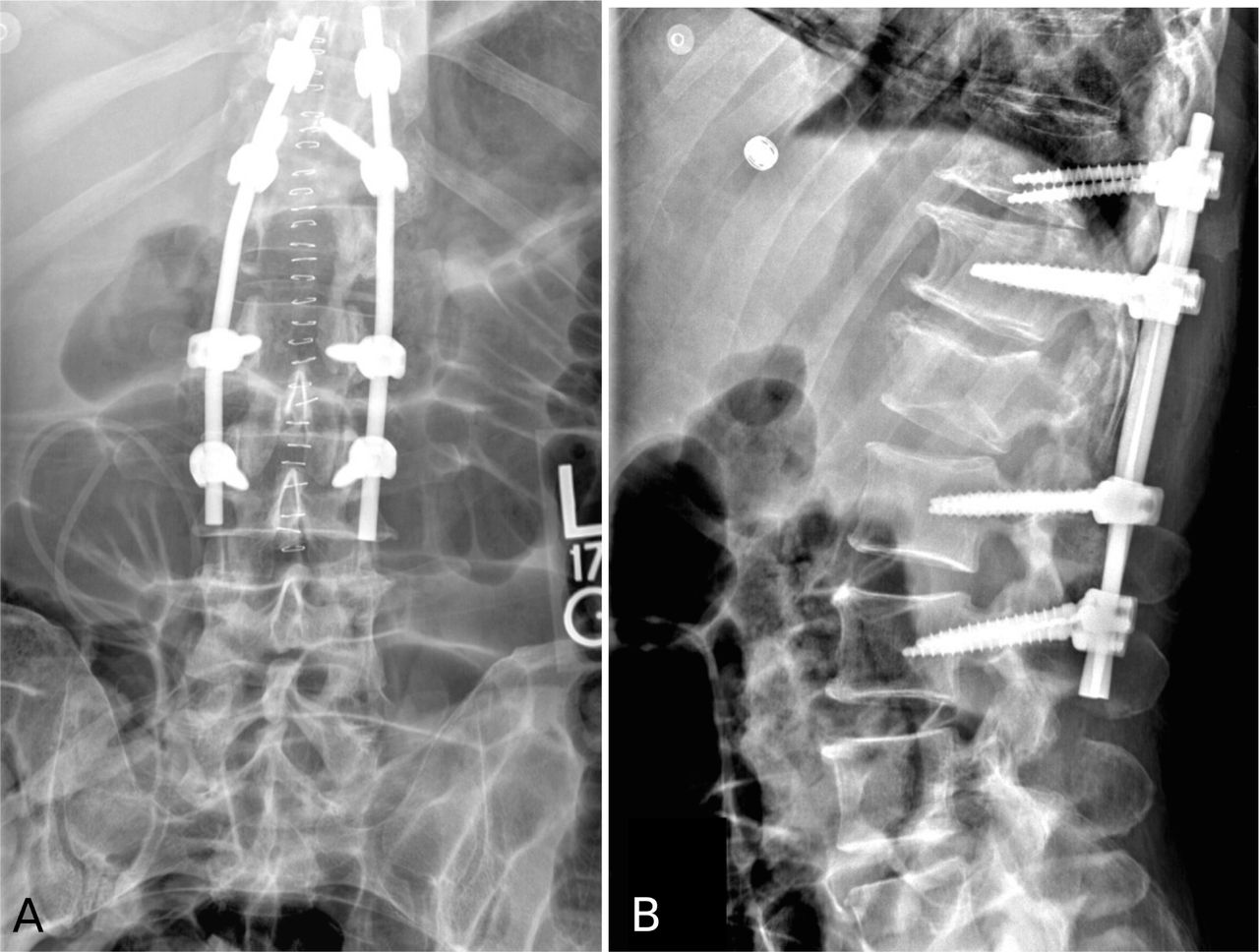
The patient was taken urgently to the operating room from the ER. A laminectomy was performed from T12-L2. The dura was noted to be under significant pressure. The right superior and inferior facet of L1 as well as the right L1 pedicle and transverse process were removed in order to ensure adequate exposure and decompression of the spinal canal anteriorly and minimize retraction of the spinal cord. Given the fact that the patient had not undergone a complete malignancy workup and his life expectancy could not be prognosticated at the time of surgery, the decision was made to not perform an extensive procedure such as a complete vertebrectomy with cage reconstruction. Using an extracavitary approach, the tumor was debulked and the spinal canal was decompressed anteriorly until there was no mass effect on the spinal cord. After adequate decompression was achieved, the spine was stabilized with pedicle screw and rod instrumentation at T11, T12, L2 and L3 (Figure 3). Tumor specimens were obtained for culture and histopathological review at the time of surgery.
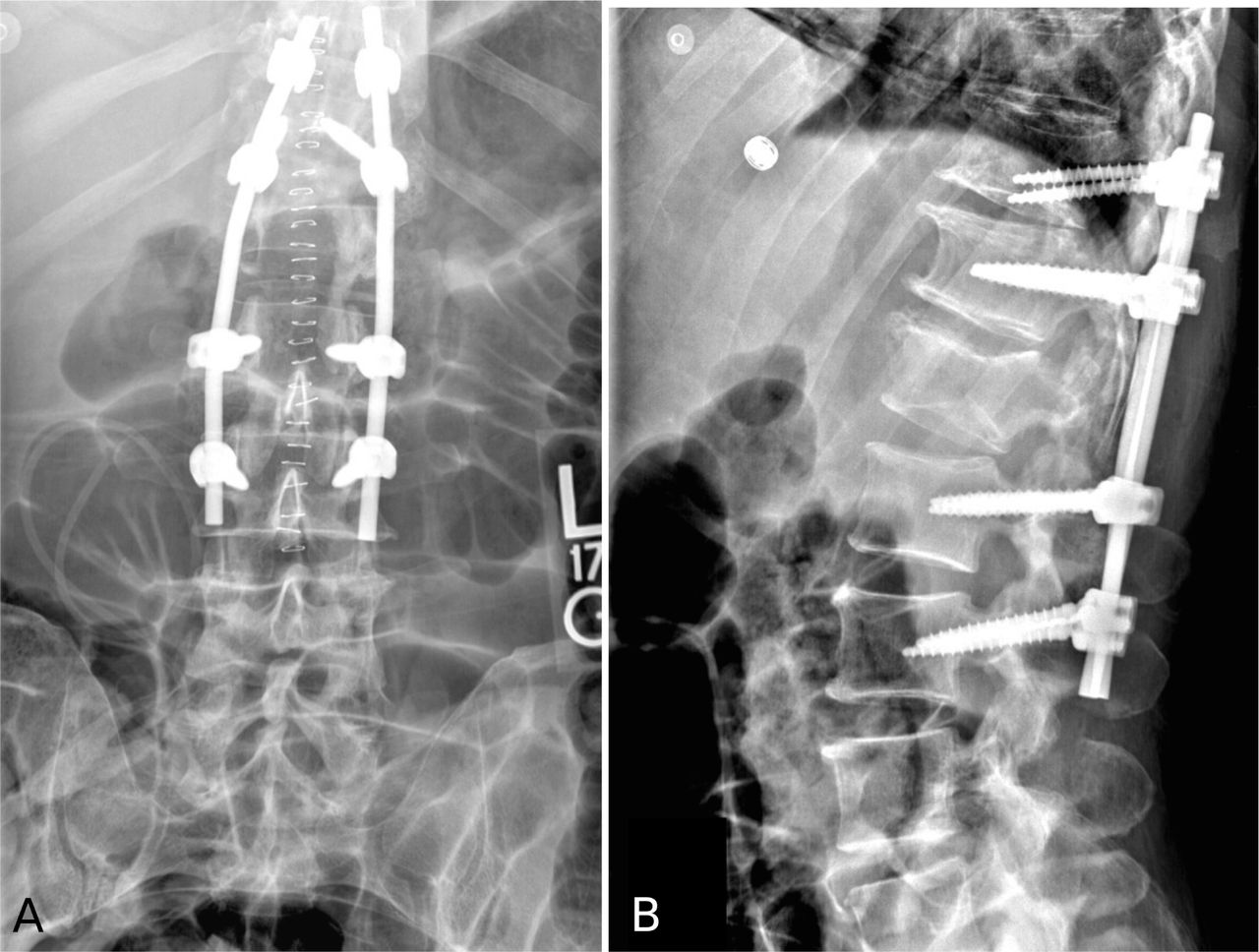
C(A) Anterior-posterior and (B) lateral spine x-ray demonstrating pedicle screw and rod instrumentation at T11, T12, L2 and L3.
Immediately postoperatively, a malignancy workup was initiated. Positron emission tomography–computed tomography (PET-CT) revealed a necrotic tumor originating in the mediastinum and extending towards the right hemithorax with metastasis to the right renal cortex, right inguinal canal and the thoracolumbar spine. Laboratory values showed elevated levels of alpha-fetoprotein (AFP) and betahuman chorionic gonadotropin hormone of 4770ng/ mL and 190mIU/mL, respectively. A scrotal ultrasound revealed no evidence of a mass lesion. Postoperatively, the patient's motor function improved to 5/5 strength throughout the bilateral lower extremities. He also made a complete recovery of his bowel and bladder functions.
Pathologic findings
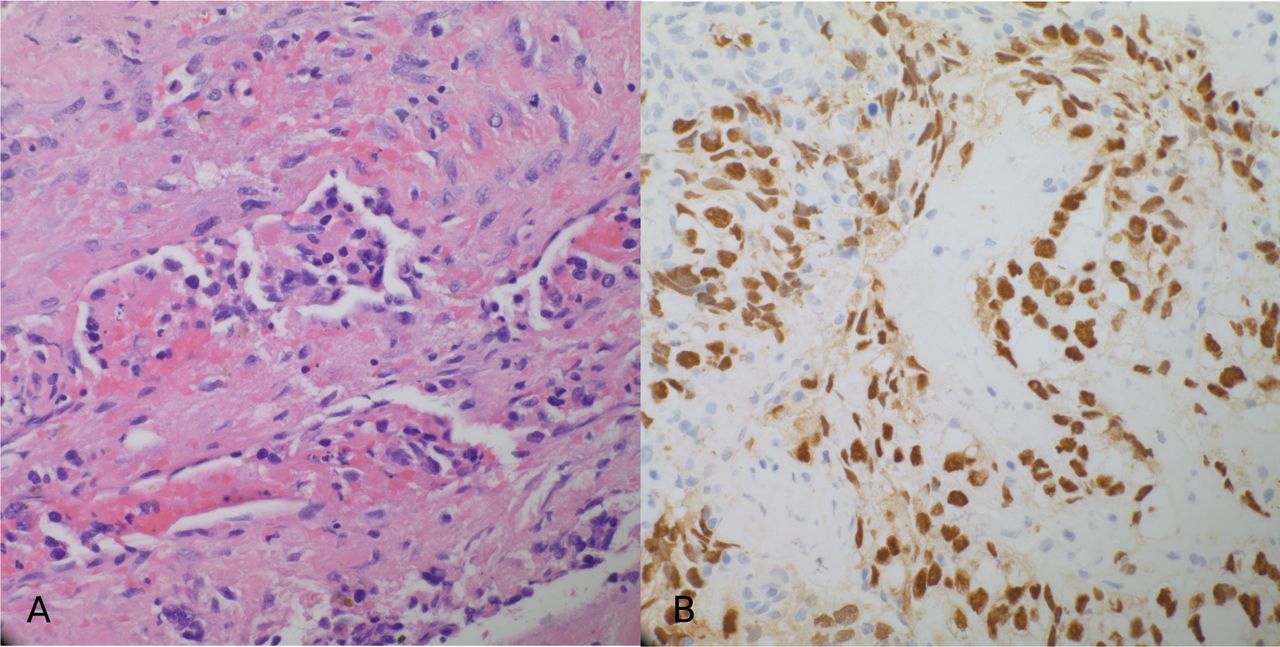
Microscopic examination of the tumor revealed polygonal cells with moderate amounts of clear to lightly eosinophilic cytoplasm, arranged in solid, microcystic and papillary architecture. Several foci of tumor cells oriented about small vascular profiles reminiscent of Schiller-Duval bodies were identified. Also present were intracytoplasmic hyaline globules. Immunohistochemical studies showed the tumor cells to be positive for SALL4, cytokeratins AE1/ AE3 and CAM 5.2 (Figure 4). Given the presence of the mediastinal and chest wall mass, the elevated serum AFP levels, and the histologic and immuno-histochemical features, a diagnosis of a poorly differentiated malignant neoplasm consistent with yolk sac tumor was rendered.

(A) Histopathologic (hematoxylin and eosin) section showing polygonal tumor cells surrounding a small blood vessel (400X magnification). (B) Immunohistochemical study of tumor cells demonstrating strong nuclear positivity for SALL4 (400X magnification).
Adjuvant therapy
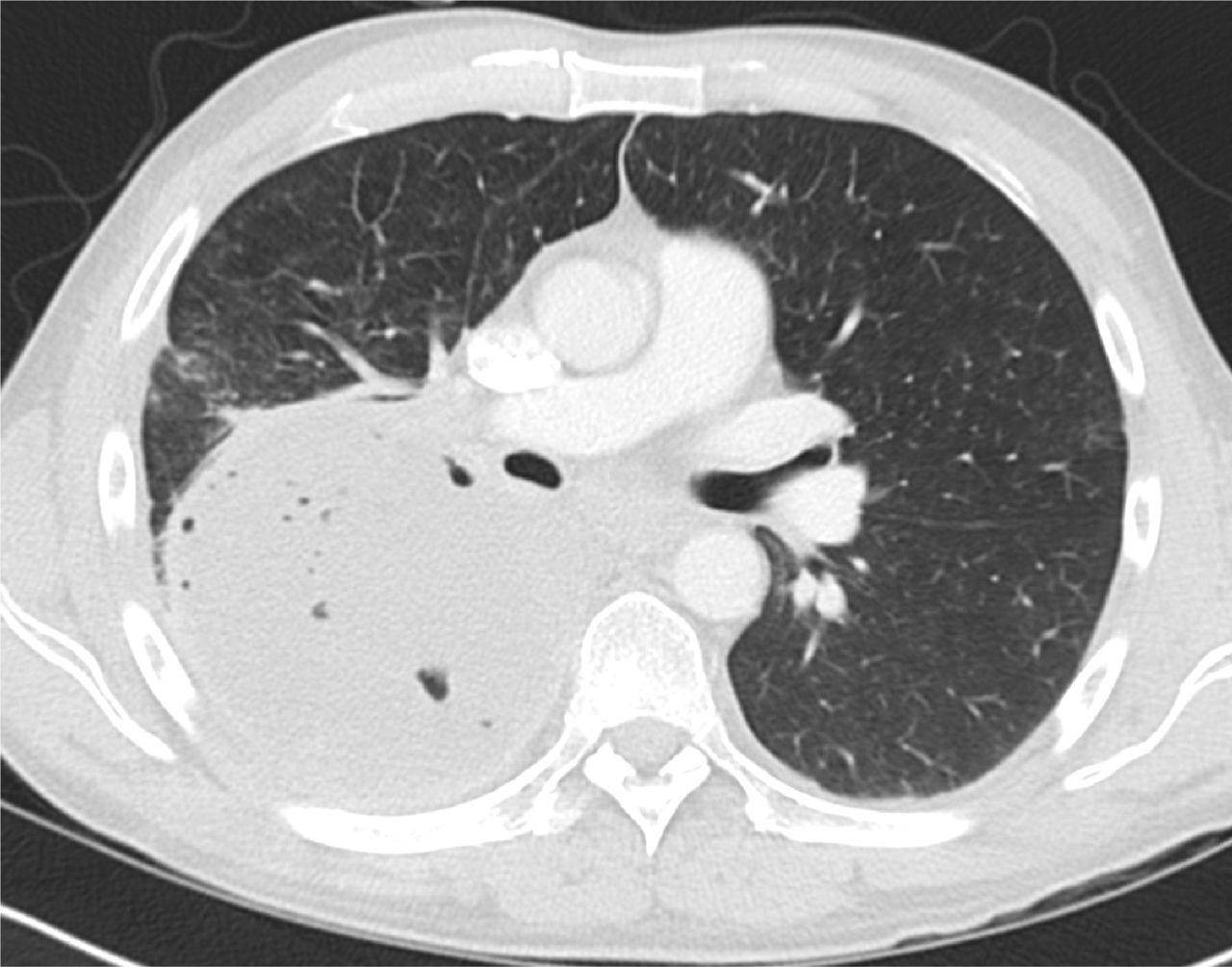
Four cycles of chemotherapy consisting of ifosfamide, etoposide and cisplatin was initiated and radiation therapy was administered to the spine operative bed. After chemotherapy and radiation, his alpha-fetoprotein and beta-human chorionic gonadotropin hormone normalized to 8.4ng/mL (from 4770ng/mL) and 1mIU/mL (from 190mIU/mL), respectively. A chest CT scan obtained approximately 3 months after surgery also confirmed an interval decrease of the right chest wall mass (Figure 5).

Axial CT scan demonstrating an interval decrease of the right chest wall mass.
Follow-up
The patient was subsequently lost to follow-up 5 months from the day of presentation. It remains unclear if he his deceased or moved back to his native country of Russia.
Discussion
Metastatic cancer to the brain and spinal cord is a well-established cause of neurological dysfunction in patients with malignancies. It is estimated that 2-5% of patients with cancer have evidence of epidural metastasis.2, 3, 4–6, 10 Lung, prostate, and breast cancer each account for 15–20% of all cases in adults.2, 5, 6–8 In children, sarcomas, neuroblastomas, Hodgkin's disease, and germ cell tumors are the most common cause of epidural metastasis.7, 8, 9–12
Spinal cord compression from yolk sac tumors in children has been described in the literature.3, 4, 9, 11–14 However, this is the first study to describe an extragonadal yolk sac tumor originating from the mediastinum of an adult male that subsequently caused an acute conus medullaris syndrome.
The anterior mediastinum is the most common site of extragonadal germ cell tumors. Benign mature teratoma or seminoma are the most common subtype while nonseminomatous germ cell tumors (NSGCT) such as yolk sac tumors are rare.1, 14 Primary mediastinal NSGCT carry a poor prognosis with 40–50% 5-year relative survival rates after chemotherapy and surgery. The survival rate is 25% if there is evidence of metastatic disease.1, 15 Primary mediastinal NSGCT has the worst survival of all extragonadal germ cell tumors due to large tumor bulk at diagnosis, resistance to chemotherapy and difficulty in removing all residual disease after chemotherapy.
In this study, we present the first case of an extragonadal yolk sac tumor originating from the mediastinum of an adult male, and metastasizing to the spine, resulting in an acute conus medullaris syndome. Urgent decompression of the neural elements followed by stabilization of the spine is paramount in relieving pain and maximizing the chance of neurological recovery. Laboratory, radiologic and histological evaluation is key in promptly establishing a diagnosis and selecting the appropriate treatment modality.
Disclosures
The authors have declared no relevant disclosures.
- Copyright © 2015 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.