


Article Figures & Data
Figures
- Figure 1
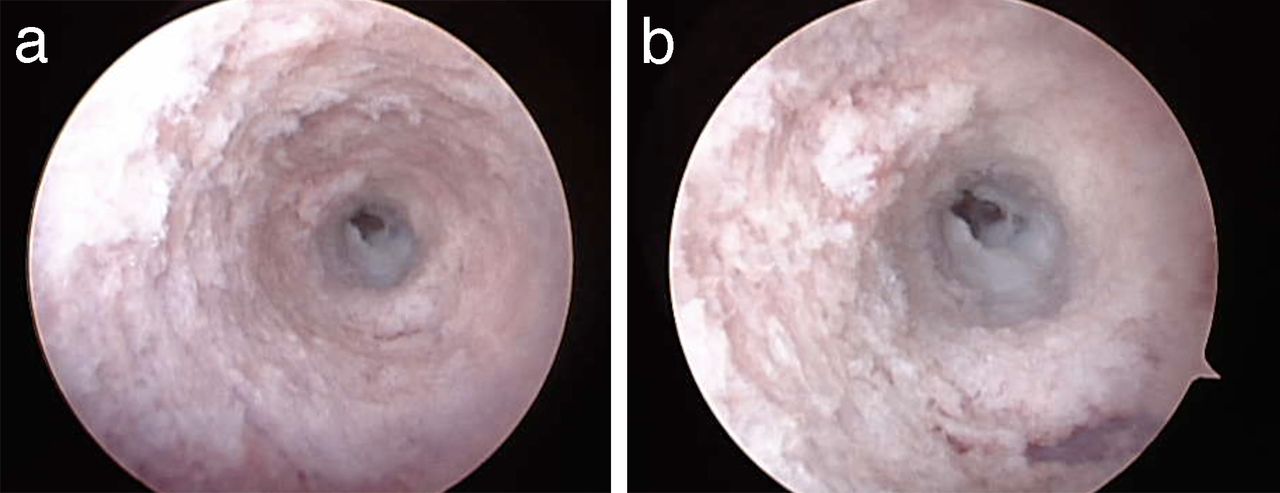
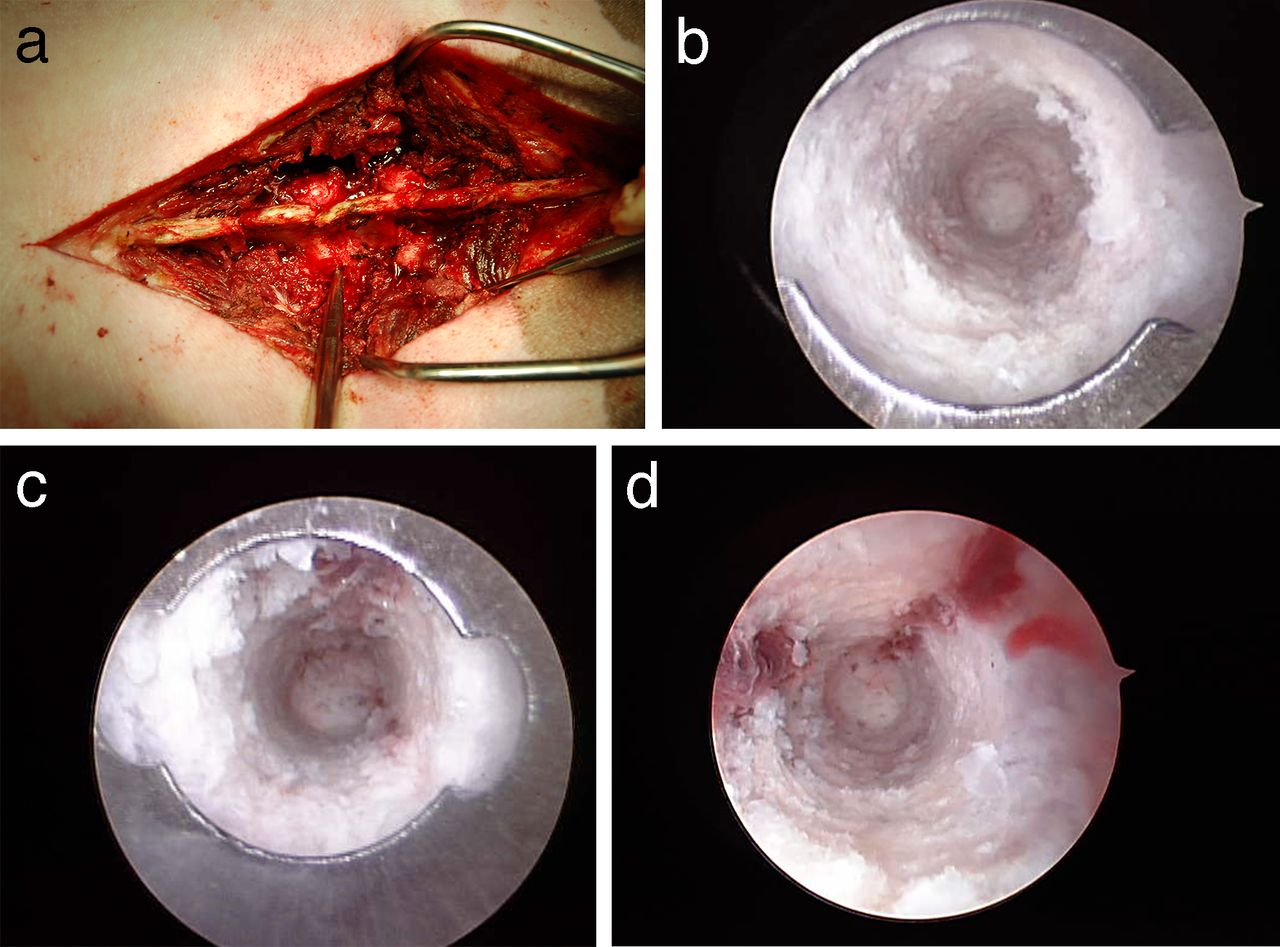
(a) Photograph of the instrument in the wound while visualization was being performed. The instrument is visible adjacent to the lumbar facet joints. Cranial is to the left and caudal is to the right. There was only trace fluid extravasation of irrigation from into the wound. The endoscopic instrument is designed to achieve a seal with the endosteal pedicle surface. (b) Endoscopic view of an intact pedicle. The distal tip of the cannula with batwing indentation to determine orientation is visible. A complete tube of ivory bone is visible through the cannula. Medial is to the right side of the screen. (c) Endoscopic view of an intact pedicle. A complete tube of white bone is visible through the cannula. At the 12 o'clock position, red, cancellous bone is visible. (d) Endoscopic view of an intact pedicle. A complete tube of white bone is visible through the cannula. At the 1 o'clock and 9 o'clock positions, red, cancellous bone and marrow are visible.
- Figure 2
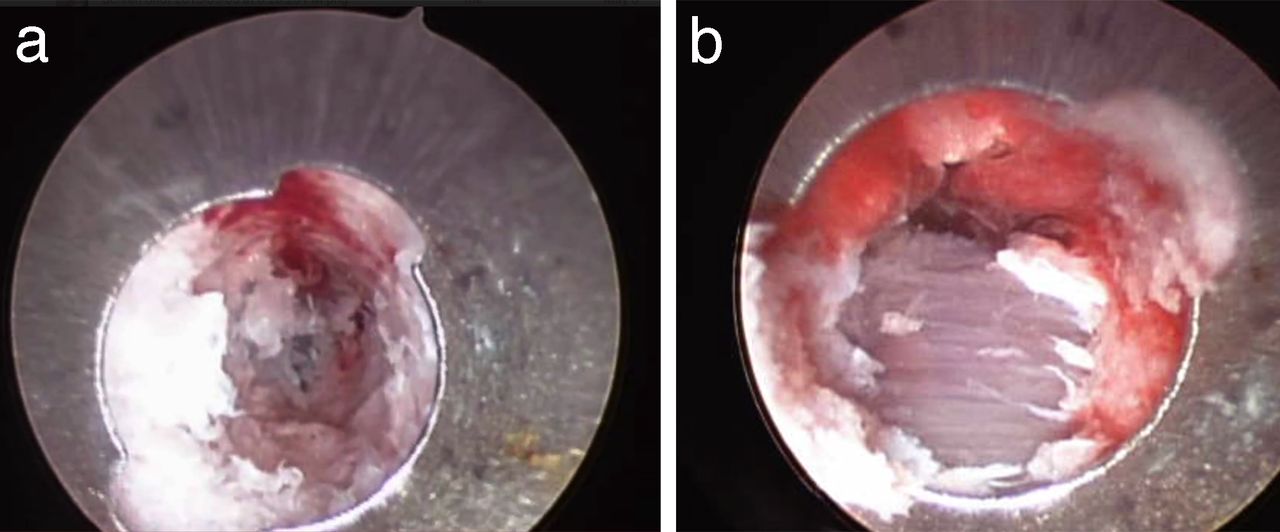
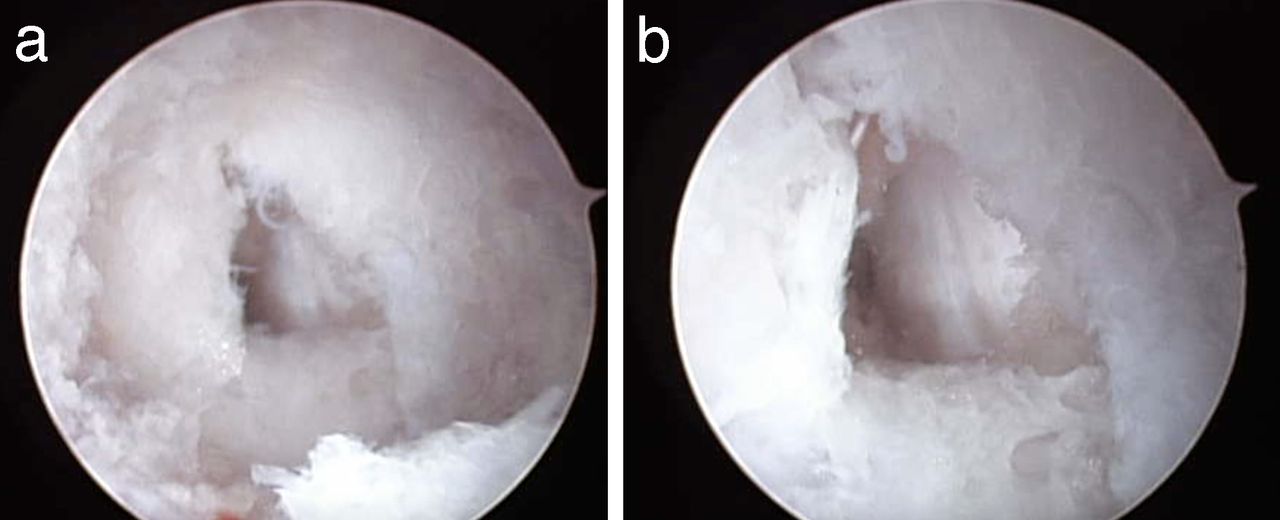
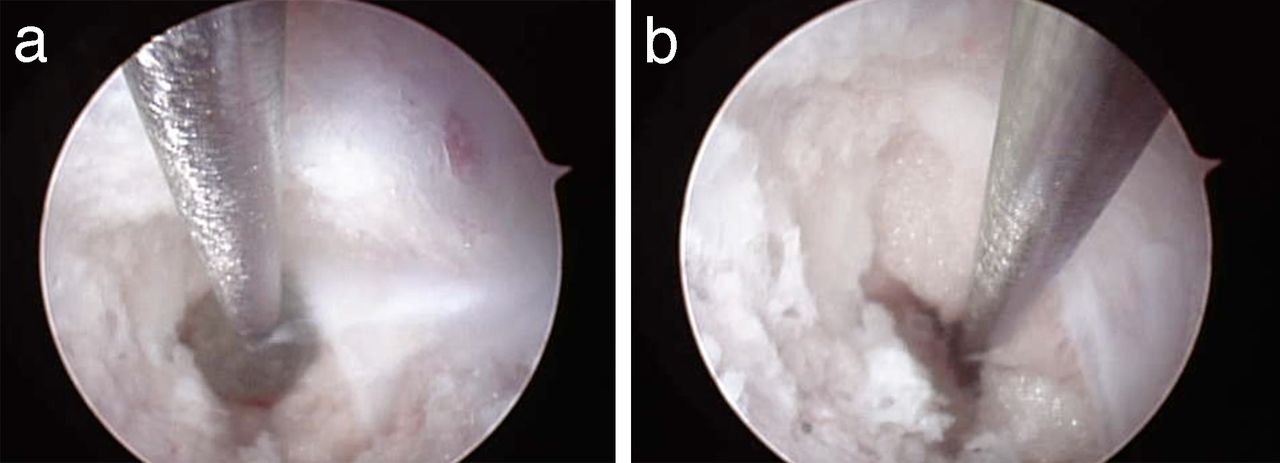
(a) Endoscopic view of a medial pedicle wall breach into the spinal canal. The triangular breach was deliberately created with a gearshift. Within the breach linear vertical fragments of ligamentum flavum are visible. (b) Close-up view of the medial pedicle breach. At approximately 4 o'clock yellow epidural fat is visible in the defect.
- Figure 3
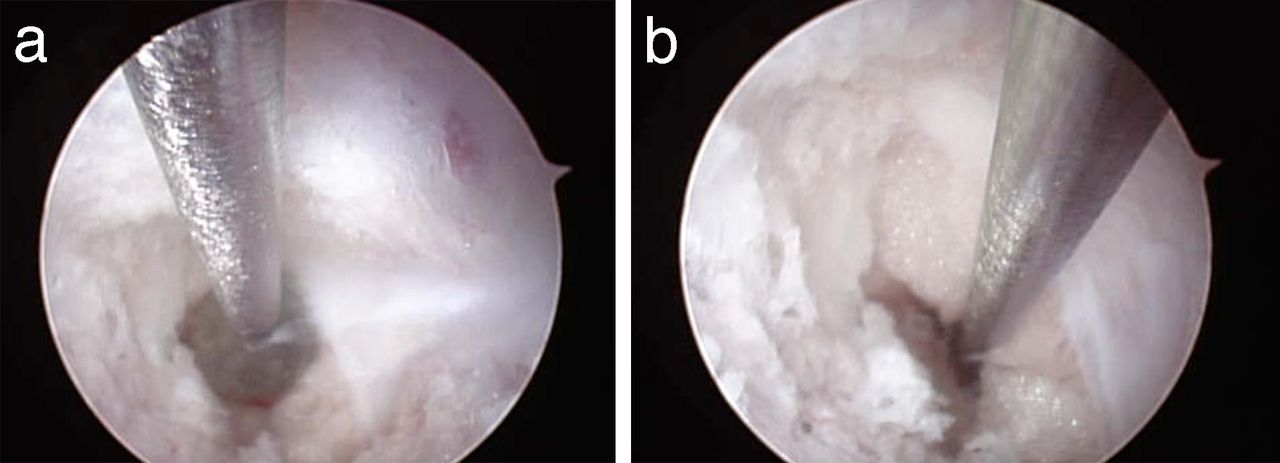
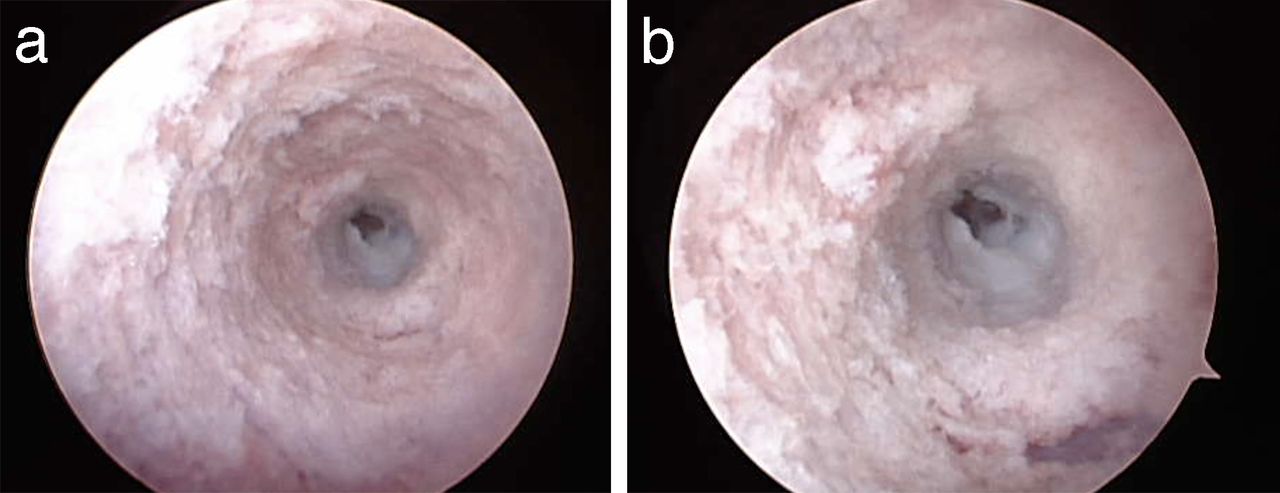
(a) Endoscopic view of anterior pedicle breach. The pedicle side walls display ivory cortical bone. The white anterior longitudinal ligament is visible in the center of the screen. It is lighter colored than the adjacent, ivory colored bone. There is a square-shared defect in the anterior longitudinal ligament. (b) Close-up view of the anterior pedicle breach. The white anterior longitudinal ligament and anterior defect are visible. The surrounding bone walls are intact.
- Figure 4
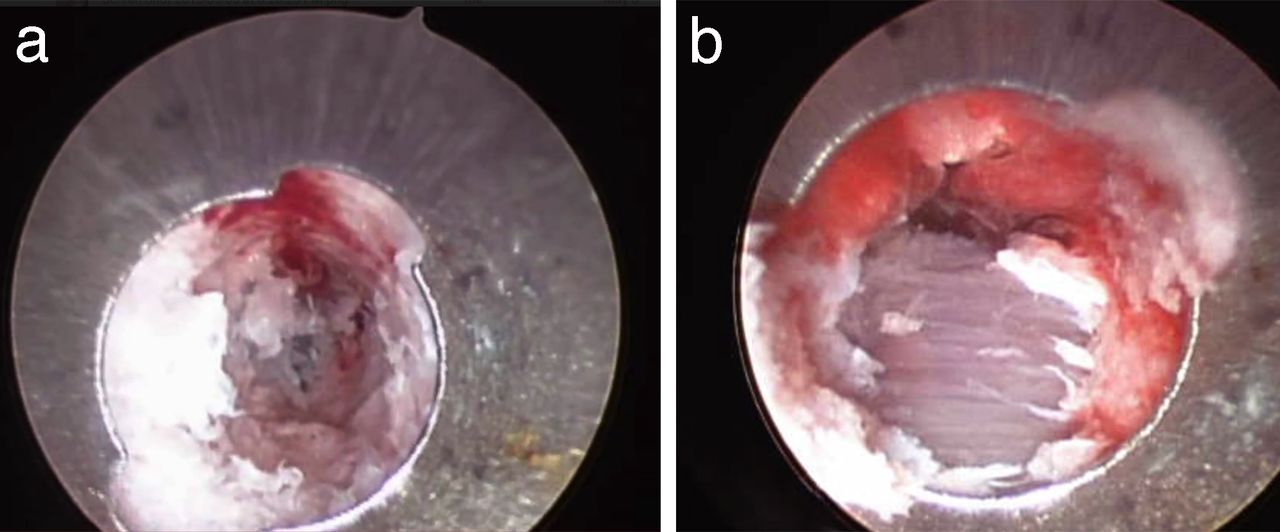
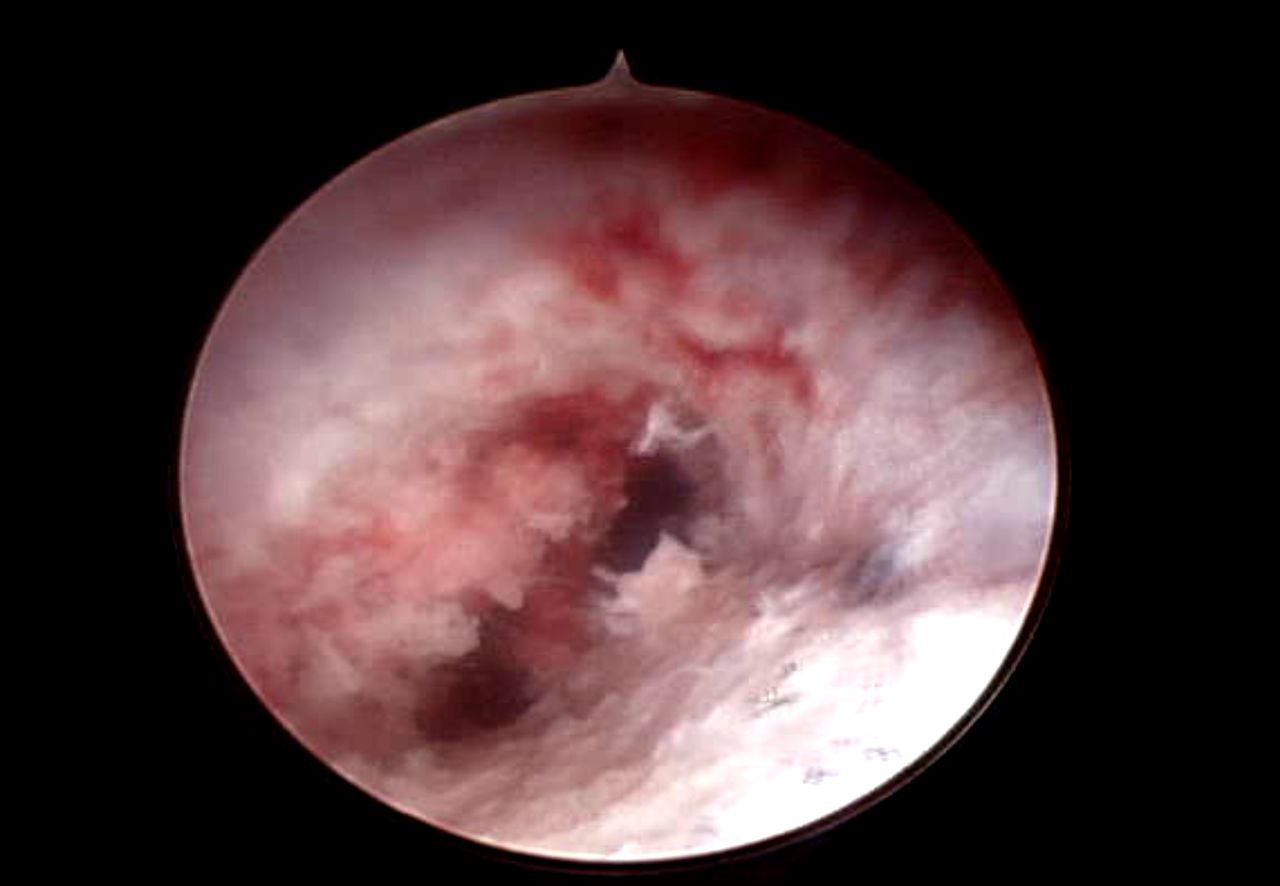
(a) Endoscopic view of lateral pedicle wall breach. In the center-left of the field there are purple horizontal fibers of paraspinous muscles. (b) Close-up view of lateral pedicle wall breach. The horizontal muscle fibers are visible through the defect.
- Figure 5
(a) Endoscopic view with ball-tip probe inside of the pedicle. The endoscopic instrument is alongside the ball-tip probe. The ball is adjacent to a defect in the medial pedicle wall. Epidural fat is distal to the tip of the ball. Ligamentum flavum is to the right side of the ball. (b) Probing the spinal canal defect. The ball-tip probe has been advanced under endoscopic guidance into the spinal canal outside of the pedicle. Epidural fat is adjacent to the shaft of the probe. The ligamentum flavum has been reflected laterally.
- Figure 6
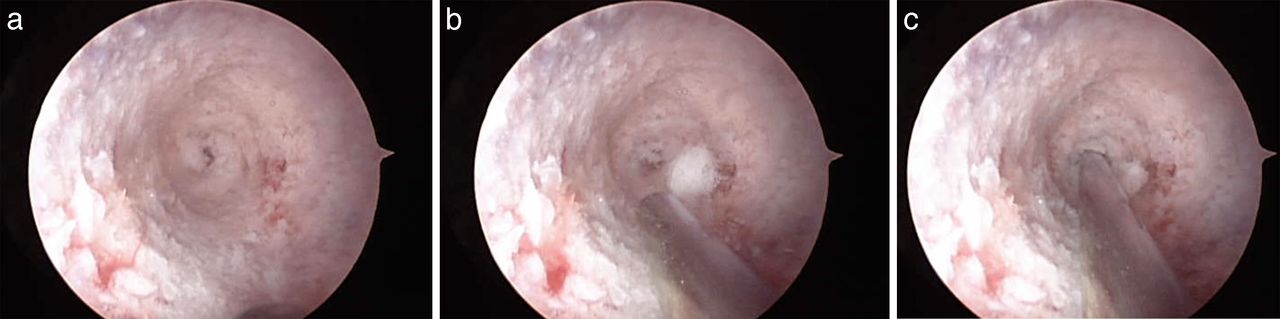
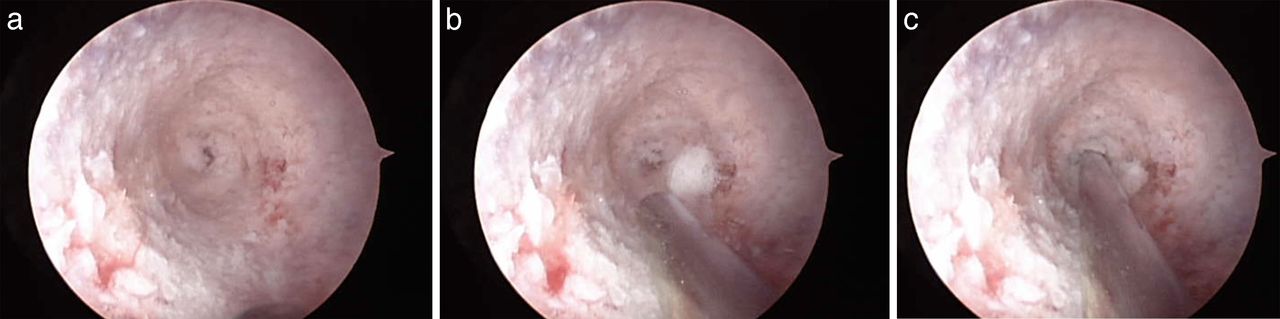
(a) Endoscopic view with anterior defect in the center of the field. The remainder of the pedicle walls are intact. (b) Endoscopic view with anterior defect in the center of the field. A guidewire is being advanced alongside the endoscopic instrument at the 6 o'clock position. (c) Guidewire placed into the anterior vertebral body defect under endoscopic guidance.
- Figure 7
Endoscopic view of a pedicle with 2 divergent paths. One path is at approximately 2 o'clock and one path is at 7 o'clock.
- Figure 8
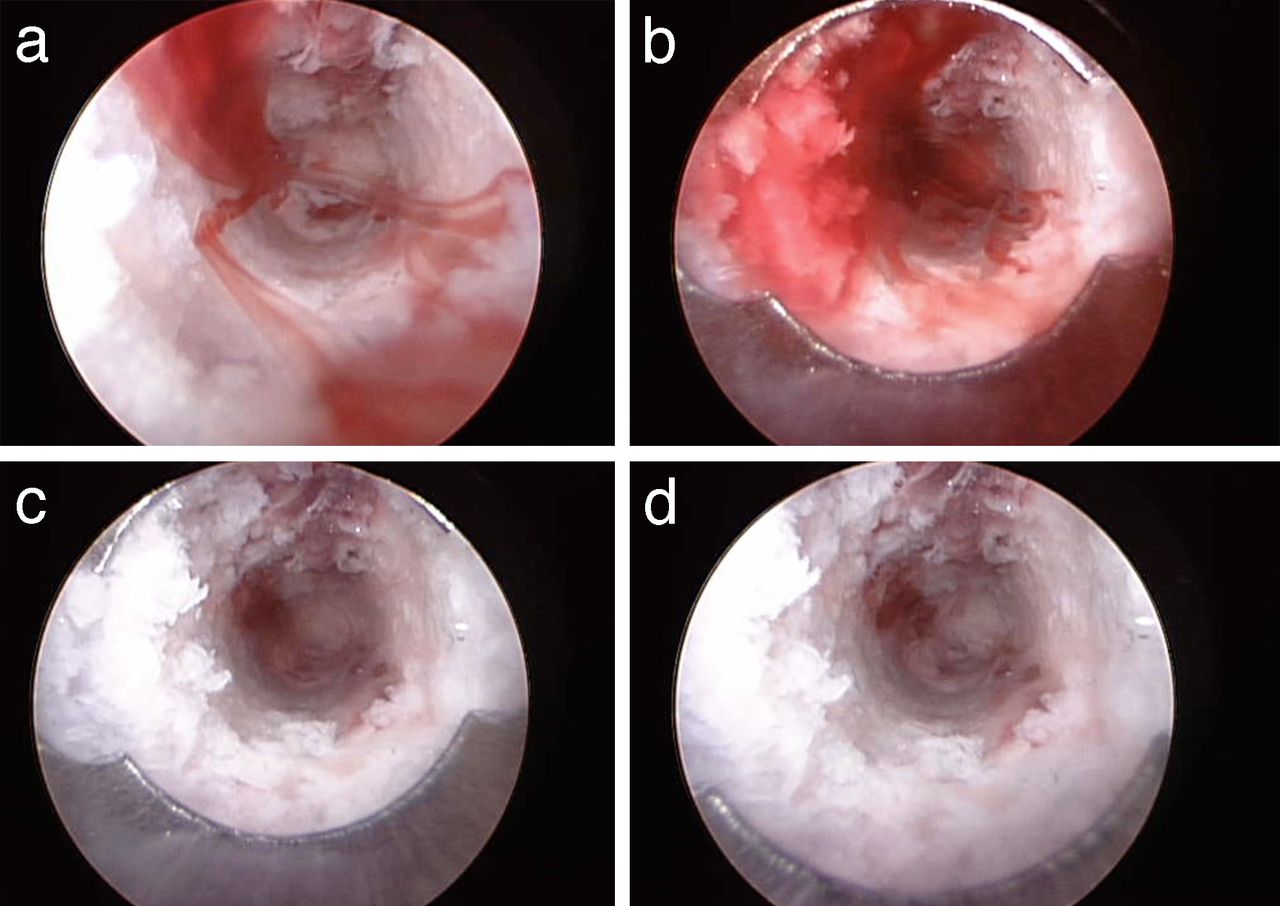
(a) Endoscopic view of a pedicle with intact walls (Figure 1b) immediately after irrigation fluid was stopped. Bony bleeding resumed immediately. The bleeding appears to have formed linear, ribbon-shaped lamellae. (b) Endoscopic view of a pedicle with intact walls with bleeding allowed to continue further. Blood filled the entire inner aspect of the pedicle. (c) Endoscopic view of pedicle with irrigation reestablished. The blood began to clear. (d) Endoscopic view of pedicle with irrigation reestablished. The blood cleared easily.




In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.