


ABSTRACT
Background: Kyphosis secondary to pyogenic spondylodiscitis is rare and its management can be very challenging.
Methods: In this report, we present the case of a 28-year-old woman, with past history of type 1 diabetes and kidney failure on hemodialysis. Her current complaint is chronic middle and low back pain with kyphotic attitude. She had undergone posterior fixation for T12 fracture 3 years earlier, which was complicated by surgical site infection to Pseudomonas aeruginosa, with secondary kyphosis proximally. X-ray showed a 64° kyphosis with complete fusion between T8 and T10, and MRI showed persistent infection foci.
Results: The patient underwent a pedicle subtraction osteotomy at the level of T9 with instrumentation from T5 to L1. Thoracic kyphosis was corrected to 39°. Samples taken from the remaining collections returned positive for multidrug-resistant Pseudomonas aeruginosa, and the patient was kept on intravenous antibiotic (Colistine) for 2 months. She could walk on day 1, with a satisfactory clinical and radiological result at 3 years.
Conclusions: Literature is sparse on the management of post–pyogenic infection kyphosis in immunocompromised patients. The current case shows that aggressive correction techniques such as pedicle subtraction osteotomy can be performed in such cases but within a multidisciplinary team to deal simultaneously with the different issues of the fragile patient.
- kyphosis
- pyogenic spondylodiscitis
- Pseudomonas aeruginosa
- pedicle subtraction osteotomy
- immunocompromised patient
INTRODUCTION
The number of pyogenic spinal infections has increased during the past decades in relation to the greater number of older patients and also immunocompromised patients (chronic renal failure, diabetes type 1, long-term steroid intake, HIV, chronic immunosuppression).1 The spine accounts for about 0.15% to 3.90% of all cases of osteomyelitis, but despite this relatively low rate, its consequences may be devastating, resulting in severe back pain, kyphotic deformity, and neurological impairment.2 Secondary kyphosis after infection has been widely described in the literature for tuberculosis cases3,4 but rarely for pyogenic microorganisms.5,6 Staphylococcus aureus is the most common organism identified with postoperative spinal infections, followed by Streptococcus. Pseudomonas aeruginosa is a relatively uncommon cause, as it accounts for about 5% of the cases.7,8 In a recent study,9 it was stated that occult infections are present in 9.3% of patients who underwent revision spine surgery and hardware removal, although they did not have clinical signs of infection; however, the common inflammatory markers such as C reactive protein, erythrocyte sedimentation rate, and procalcitonin do not seem sensitive enough to detect these occult infections. The combination of a rigid kyphosis secondary to a previous postoperative spinal infection and an occult infection remaining from that postoperative infection is not common and may require a specific management, especially when aggressive surgery is required and the patient is in the “immunocompromised” category.
CASE DESCRIPTION
A 28-year-old woman had been complaining of middle and low back pain with kyphotic attitude for almost 3 years. Her past history revealed insulin-dependent type 1 diabetes with kidney failure requiring 3 hemodialysis sessions per week; she had sustained 3 years before, in another country, a T12 compression fracture that was surgically treated with T10 to L2 posterior fixation; this was complicated by surgical-site infection to multidrug-resistant P. aeruginosa with spondylodiscitis T8-9 and T9-10. According to the patient, she was managed conservatively with intravenous (IV) antibiotics for over 6 weeks, but the discharge would not stop and the wound did not heal. Hardware was removed at 3 months, which led to progressive healing but with the occurrence of a secondary kyphosis proximally. Total period of IV antibiotics was around 6 months.
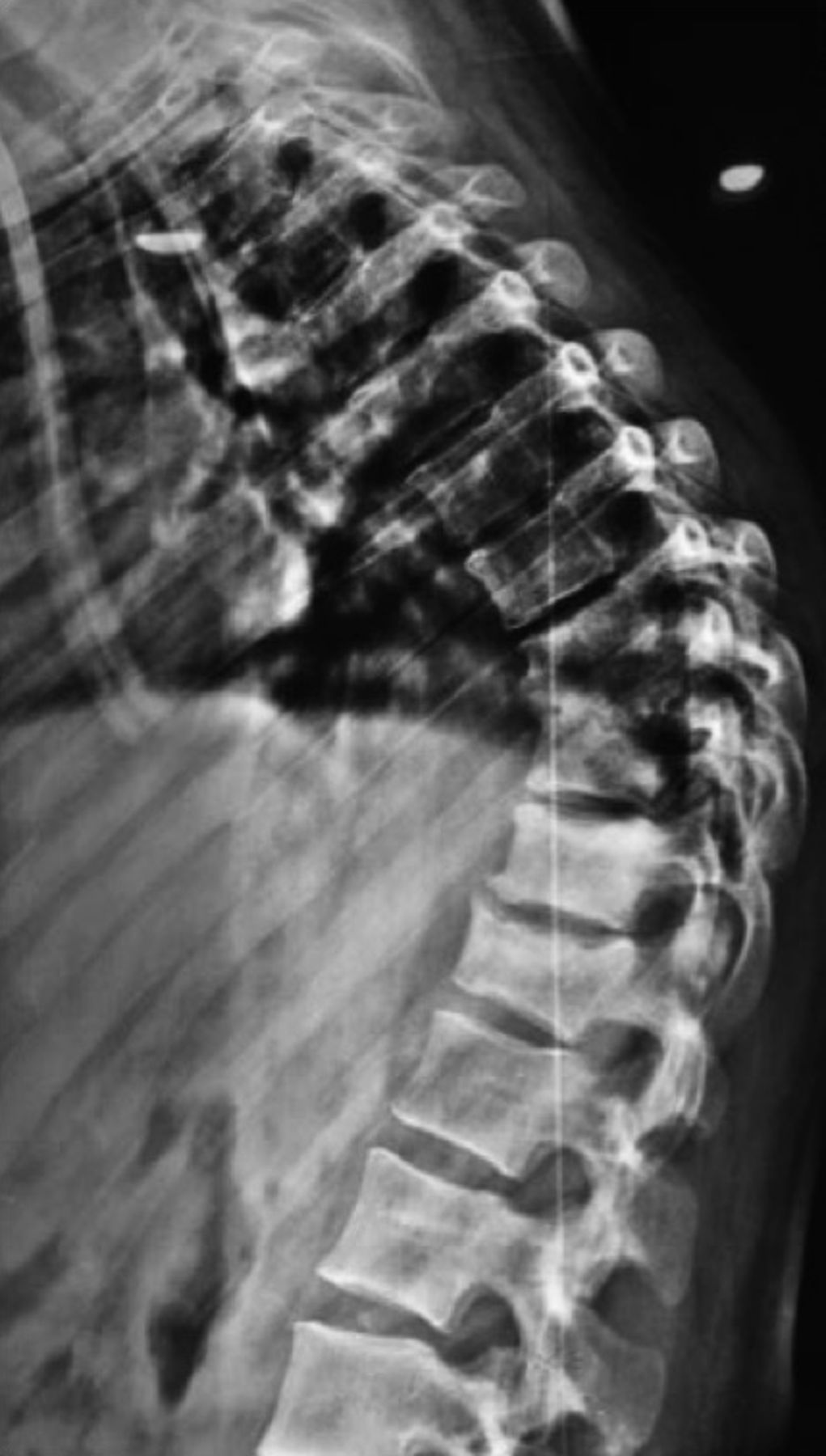
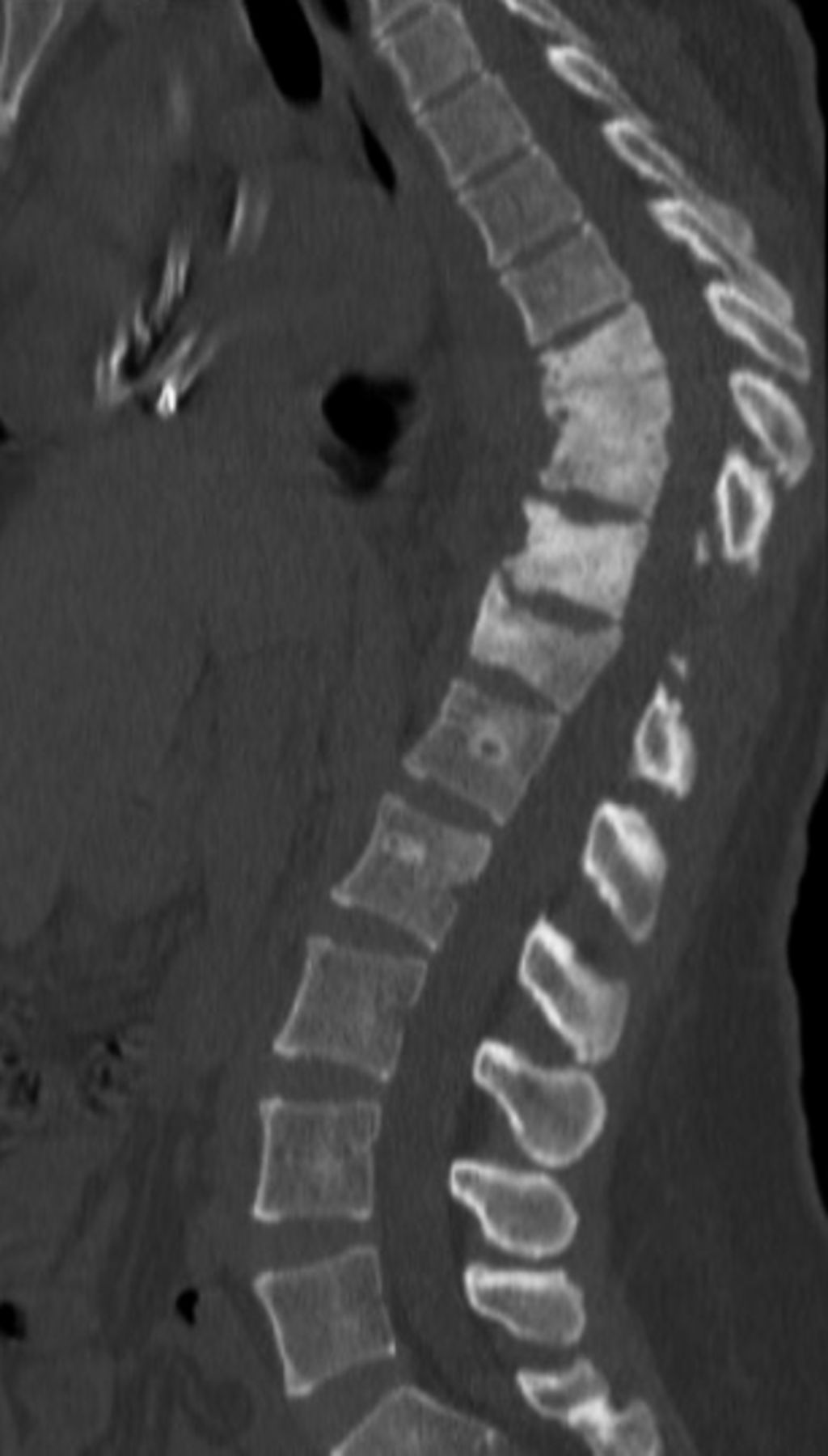
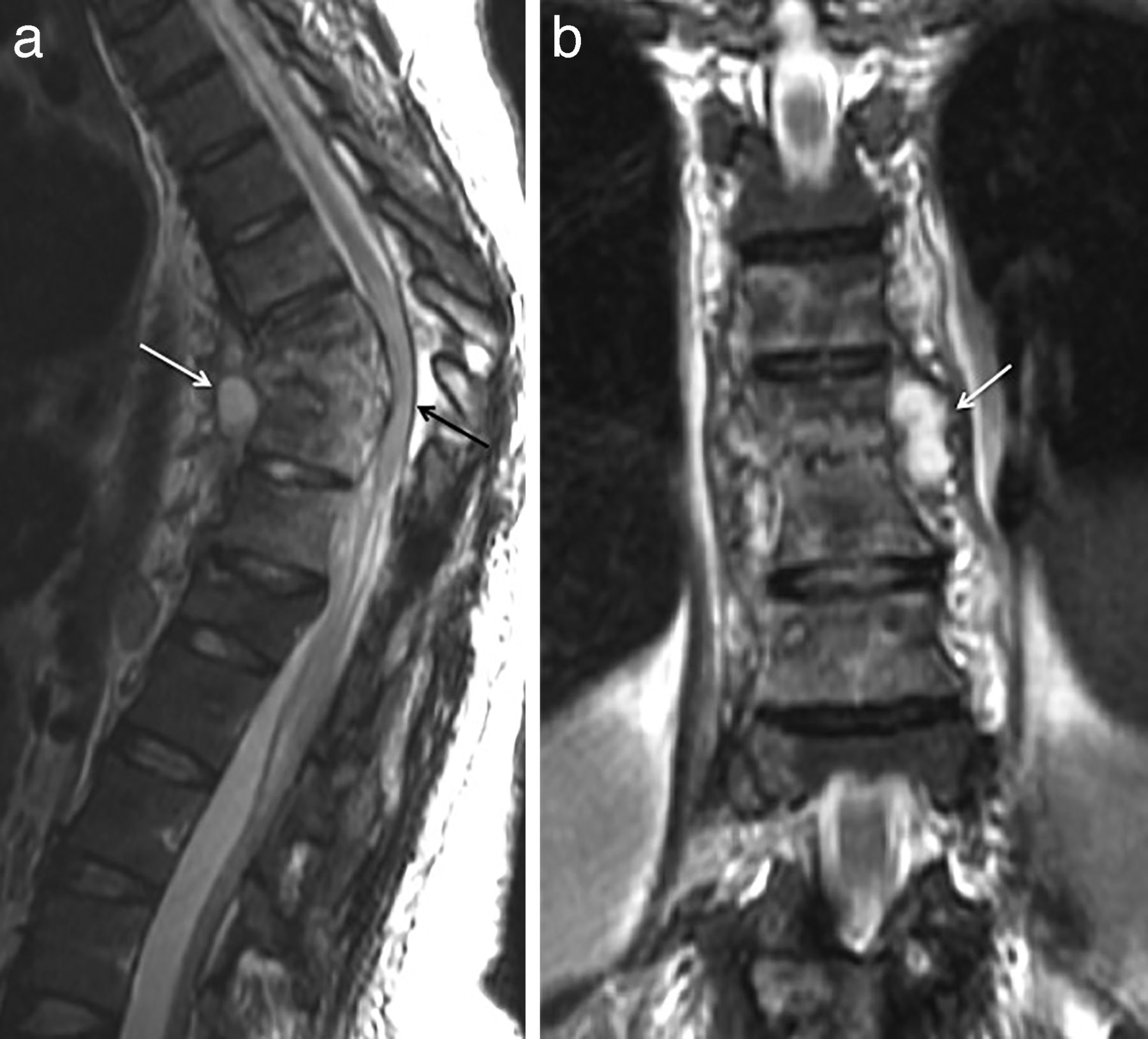
Physical examination revealed middle back pain at the level of the previous surgery with a significant thoracic kyphosis clinically, associated with low back pain probably due to a facet joint syndrome because hyperlordosis could be noted. A 3-year-old thoracic x-ray brought by the patient showed the onset of the kyphosis proximally to the initial construct with the T10 screws inside the T9-10 disk space (Figure 1), and according to the patient, the rods at that time were palpable below the skin proximally but not out of the skin. Six months after hardware removal, thoracic x-ray revealed a significant kyphosis (Figure 2). Full-spine anteroposterior and lateral x-rays at the time of presentation revealed a thoracic kyphosis of 64°, with compensatory hyperlordosis of 67° and no coronal deformity (Figure 3a, b). Computed tomography (CT) scan confirmed the complete fusion between T8 and T10, with vertebral body sclerosis between T8 and T12 (Figure 4). A potential differential diagnosis is stable nonunion, but different coronal and sagittal images showed no differentiation between the T8 and T9 vertebral bodies laterally, thus confirming the fusion. MRI showed paraspinal collections (anterior and lateral) suggestive of remaining infection foci, in addition to spinal canal narrowing at the kyphosis level (Figure 5a, b).

Thoraco-lumbar sagittal X-ray 3 years before presentation showing the onset of the kyphosis proximally to the initial construct with the T10 screws inside the T9-10 disk space.
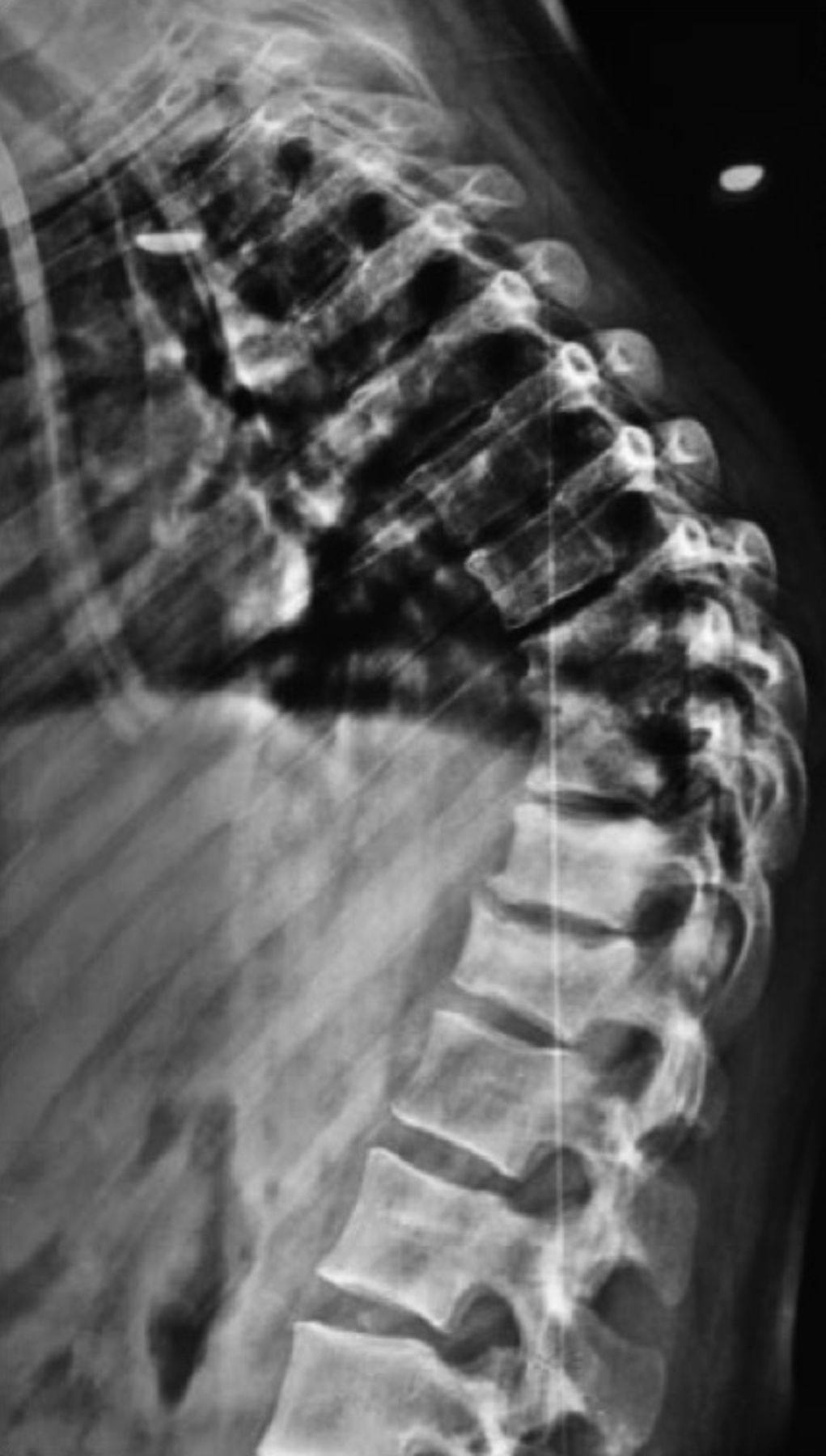
X-ray showing a significant kyphosis 6 months after hardware removal.

Full spine anteroposterior and lateral x-rays at the time of presentation revealing a thoracic kyphosis of 64°, with compensatory hyperlordosis of 67° and no coronal deformity (a and b).
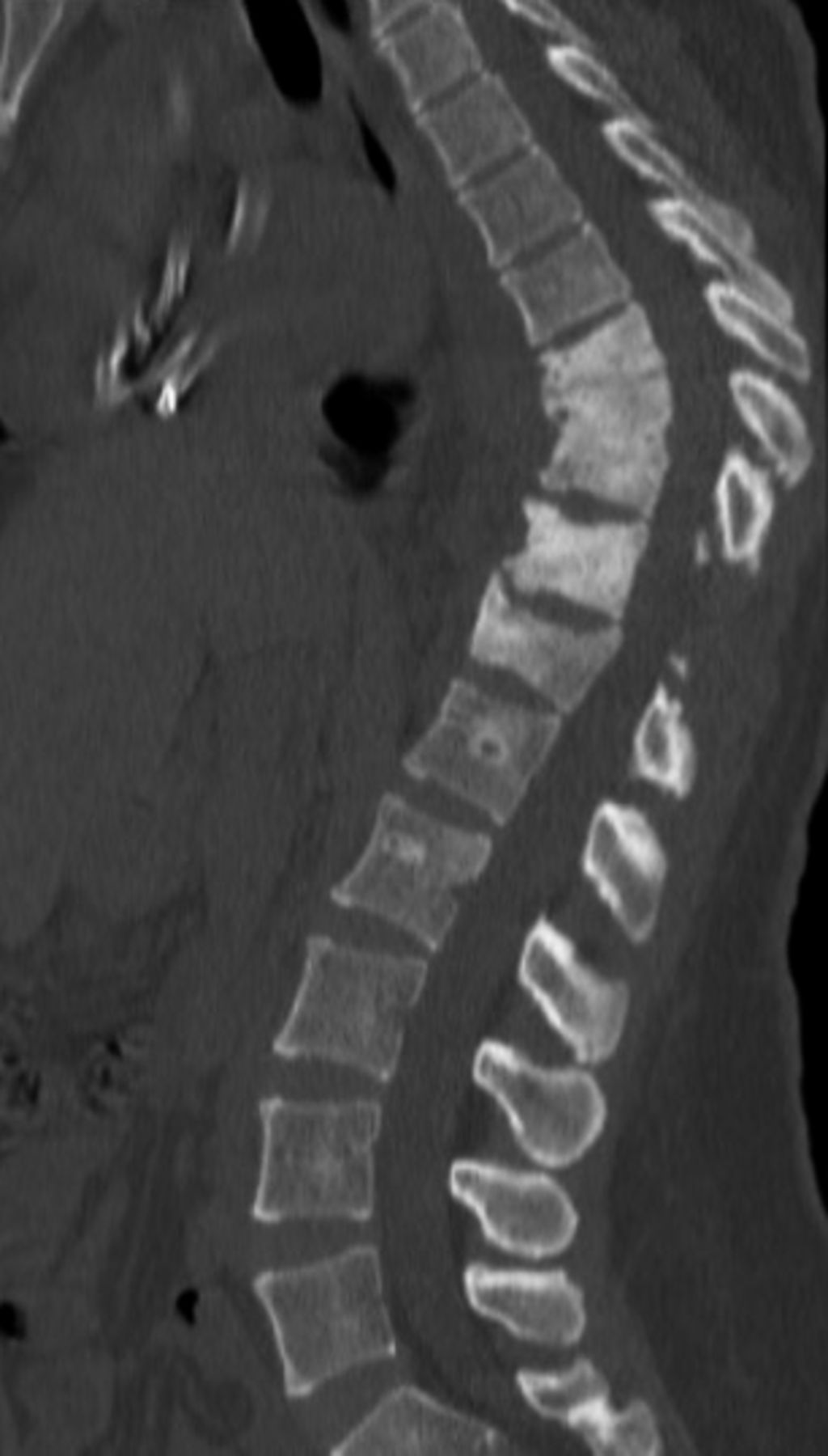
Computed tomography scan showing the complete fusion between T8 and T10, with vertebral body sclerosis between T8 and T12.

MRI revealing paraspinal collections anteriorly (a, white arrow) and laterally (b, white arrow) suspicious of remaining infection foci, in addition to spinal canal narrowing at the kyphosis level (a, black arrow).
After discussion with the anesthesiologist, nephrologist, and endocrinologist, the patient underwent a pedicle subtraction osteotomy (PSO) at the level of T9 with instrumentation from T5 to L1.
SURGICAL TECHNIQUE
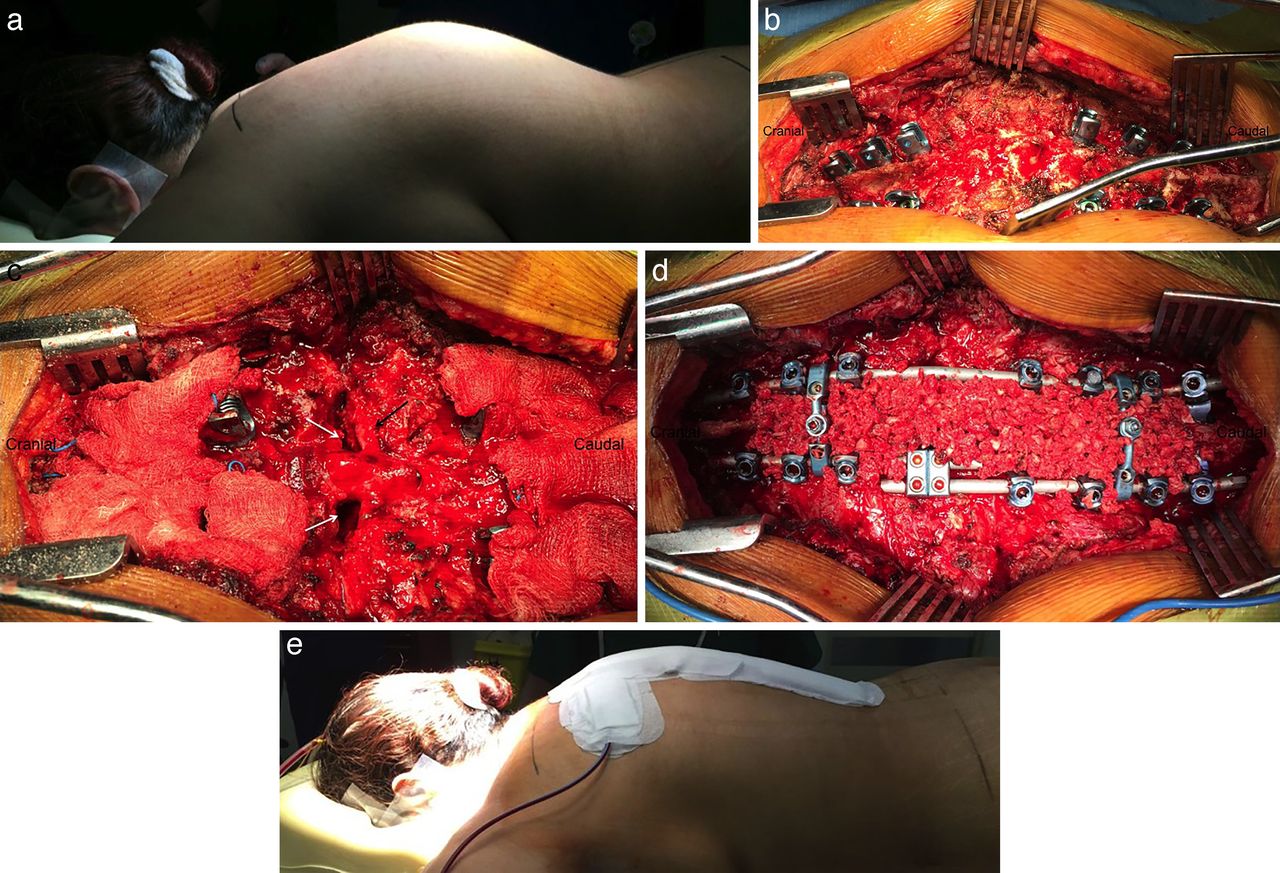
The patient was installed in a prone position, on 4 cushions (Figure 6a). During the surgery, we used transcranial motor-evoked potentials, somatosensory evoked potentials, and free-running electromyography (EMG) of the lower extremities as well as evoked EMGs with pedicle-screw stimulation.

Intraoperative images showing the thoracic hump (a), spinal exposure, and screws insertion from T5 to L1 but sparing T8 to T10 (b); pedicle subtraction osteotomy performed at the level of T9 (c, white arrows); the right T9 root is clearly visible (c, black arrow); reduction of the kyphosis and placement of autologous bone graft (d); clinical aspect at the end of the procedure (e).
The operative field was exposed from T5 to L1; a posterior cutaneous midline incision was made. The spine was exposed subperiosteally, going laterally to the costotransverse junction. Resection of the inferior articular processes at all levels was performed bilaterally to provide maximum flexibility to the spine. We next used the freehand technique to place the pedicle screws from T5 to T7 and from T10 to L1 (Figure 6b); 2 sublaminar offset hooks were put at the distal level of the construct to increase the resistance to pullout forces. To expose the lateral wall of T9, the transverse processes were removed with a rongeur, and the proximal 3 cm of the right and left ribs (including the rib head) were removed. A Cobb elevator was then placed, bilaterally, on the lateral wall of the vertebra and moved anteriorly to the anterolateral quadrant to retract all the lateral soft tissues. A suspicious collection was noted on the left side and several samples were taken and sent for culture; a complete Surgicel (Johnson & Johnson, New Brunswick, New Jersey) was left in place to maintain a safe distance between the bone and the soft tissues. Two complete foraminotomies (both cephalad and caudad to the pedicles on both sides) were made, achieved by complete laminectomy of the concerned level, with partial laminectomies of the levels just above and just below. This enabled surrounding of the pedicles. Both pedicles were then removed, exposing the posterior wall of the vertebra, and the nerve roots above and below were identified. After retraction of the lower nerve root, 2 osteotomes are placed above and below each pedicle. Cancellous bone was removed in a wedge fashion from posterior to anterior on both sides. Because retraction of the cord is prohibited at the level of the thoracic spine, direction of the osteotomes for removal of the medial part of the bone becomes horizontal, and the medial part of the posterior wall was finally removed with an up-angled pituitary rongeur (Figure 6c). For the correction technique, at first, cantilevering of the spine was performed with 2 prebent titanium alloy rods connected by a domino on the left side. Further closure of the osteotomy by compression with the use of the domino was applied; the rod was then completely locked. During the osteotomy closure, an audible crack was noted; this was due to the fracture of an anterior osteophyte and the complete sclerosis at the osteotomy site. The bone-on-bone contact at the osteotomized level was checked, and the spinal cord was carefully controlled because kinking could occur in case of important reduction. The contralateral rod was placed and secured. The fixation was completed by the placement of two cross-link connectors between the 2 rods, 1 proximal and 1 distal. The prepared autologous bone grafts were placed to cover the maximum surface (Figure 6d). Postoperative improvement of the gibbosity could be seen (Figure 6e).
RESULTS
The patient could walk on day 2 with a thoracic lumbar orthosis, to be used for 3 months, and with assistance from a physical therapist. She was discharged on day 14 with proper wound healing. Postoperative CT scan confirmed good correction at the PSO level with a bone-on-bone contact (Figure 7), and x-rays showed a correction of the thoracic kyphosis to 39° with correction of the compensatory hyperlordosis to 50°. Samples taken from the remaining collections returned positive for multidrug-resistant P. aeruginosa sensitive to only Colistine, and the patient was kept on intravenous antibiotic for 2 months. She showed satisfactory clinical and radiological result at 3 years (Figure 8a, b).

Postoperative CT scan confirming the kyphosis reduction with bone-on-bone contact at the osteotomy level.

Full-spine x-rays 3 years after the surgery showing a stable reduction and construct.
DISCUSSION
Thoracic kyphosis secondary to pyogenic spondylodiscitis is challenging when it comes to its surgical management, especially in a patient with comorbidities. In fact, spinal surgery is associated with significantly higher mortality rates in patients with chronic kidney disease compared with patients with normal kidney function.10 Therefore, management should be done within a multidisciplinary team with permanent involvement of different specialties; thus, in addition to the spine surgeon and infection disease specialist, an endocrinologist and nephrologist must be involved if diabetes and renal failure are present; the sugar rate must be closely monitored and well controlled prior to the surgery,11 and dialysis sessions must be well scheduled around the surgical date, with usually 1 session the day before.12–14
There is a controversy in the surgical management of secondary kyphosis after pyogenic infection because no evidence-based guidelines exist, given that what is mainly found in the literature is case reports. Surgery can be achieved by an anterior-only approach with instrumentation5 when infectious involvement has been recent (less than 6 weeks) with no rigid deformity, which enables correction and reconstruction with multilevel cages in the apical disks with anterior instrumentation. Surgery can also be performed by a double approach that can be either anterior/posterior or posterior/anterior in the same setting or sequentially15; the anterior part enables debridement, decompression, and anterior fusion with a strut graft, and the posterior part enables posterior instrumentation and fusion. This technique is also advised in cases of kyphosis secondary to a recent infection with an ongoing infectious process with hypersignal seen at the disk levels on the MRI, because it provides a smaller loss of correction when compared with either the posterior-only or anterior-only approach. To palliate the loss of correction of the posterior-only technique, a technique of long posterior instrumentation with short fusion and without debridement of the infected tissue has been described16 that can strongly reduce the kyphotic deformity and prevent loss of reduction. But in cases of a rigid kyphosis secondary to an old infection with complete vertebral fusion, it is advised to perform a posterior-only approach with the use of aggressive corrective techniques such as PSO or vertebral column resection. This has been widely described in the literature for tuberculosis patients,17,18 as it allows an important amount of correction in a one-stage surgery.
P. aeruginosa is a relatively uncommon cause of pyogenic spondylodiscitis, as it accounts for only 5% of the cases,7,8 mainly encountered in the background of IV drug use and immunocompromised patients. It is frequently multidrug-resistant, and therefore the close involvement of the infection disease specialist is mandatory during the course of treatment.
In the case of our patient, given the angulation of the kyphosis, with complete vertebral fusion at the apex, and also the fragility of the patient with renal failure, a posterior-only approach with pedicle subtraction osteotomy at the level of T9 was done with instrumentation from T5 to L1. Such an aggressive correction technique could be successfully performed in this case, even when the initial responsible germ was multidrug-resistant P. aeruginosa, but within a multidisciplinary team to simultaneously deal with the different issues of the fragile patient.
Footnotes
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2019 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.