


ABSTRACT
Background: Studies reporting multilevel anterior cervical corpectomy (>2 levels) and reconstruction in patients with long-segment anterior cervical compression are few and surgical outcomes are variable with increased surgical morbidity and a high incidence of graft-related complications. The aim of this study is to evaluate the effectiveness and safety of cervical corpectomy and anterior reconstruction of 3 or more levels in patients with long-segment anterior cervical compression.
Methods: We retrospectively reviewed patients who had undergone 3 or more levels of anterior cervical corpectomy and reconstruction from 2014 to 2018. Clinical and radiological parameters such as Nurick grading, modified Japanese Orthopedic Association (mJOA) score, cervical segmental angle, cervical sagittal angle, graft subsidence, and fusion rate were evaluated preoperatively and at a 2-year follow-up. Patients were divided into 2 groups according to their anterior reconstruction, either with fibular strut autogenous graft or titanium mesh cage and rigid anterior cervical plating for subgroup analysis. Patients whose bone stock was found to be poor had undergone posterior instrumentation as a staged procedure.
Results: There were 48 patients (mean age: 58.17 years) in the cohort: 42 had undergone 3-level and 6 had undergone 4-level cervical corpectomy with an ossified posterior longitudinal ligament and multilevel cervical spondylotic myelopathy being the main surgical indications. C5 to C7 corpectomy was most common. Of the cohort, 83.4% had standalone anterior reconstruction and only 8 patients (16.6%) had supplementation with posterior instrumentation. Our subgroup analysis showed statistically significant change in Nurick grading, mJOA score, cervical segmental angle, and sagittal angle in both groups at a 2-year follow-up (P < .05). Overall fusion rate was 89.5%. Decreased incidence of graft subsidence, statistically significant less graft subsidence (P = .002) and a higher fusion rate (P = .001) were noted in titanium mesh cage group at 2-year follow-up.
Conclusions: Multilevel anterior cervical corpectomy and reconstruction is a safe and efficacious procedure. A titanium mesh cage filled with autogenous bone graft and a rigid anterior cervical plate gives best results. Posterior instrumentation should be considered along with a multilevel cervical corpectomy construct in patients with poor bone stock.
Level of Evidence: 4.
INTRODUCTION
Single-level anterior cervical corpectomy and reconstruction is a well-recognized and well-documented procedure with predictably favorable outcome.1 However, multilevel cervical corpectomy (3 or more levels) and reconstruction for long-segment anterior compressive pathology is not frequently done and the surgical outcome is perceived to be worse due to surgery-related morbidities and a higher incidence of graft-related complications.2 Hence, some authors have advocated avoidance of greater than 2 levels of cervical corpectomy.3,4 A failure rate of 33% to 70% has been documented in the literature for 3 or more levels of anterior cervical corpectomy and reconstruction.5–7
The presence of an anterior cervical plate following 3-level corpectomy shifts the instantaneous axis of rotation of cervical spine anteriorly resulting in change in loading pattern of the long graft with no loading occurring during flexion movements of cervical spine and more excessive distractive loading occurring during extension movements of cervical spine at the caudal graft level. This results in anterior dislodgement of the long graft at the caudal level with subsequent anterior dislodgement of the plate and posterior cephalad displacement of the graft compromising the cord. Hence few surgeons prefer posterior instrumentation with 3 or more cervical corpectomy constructs; the rationale is that it shifts the instantaneous axis of rotation posteriorly and decreases the stress at the caudal vertebral body, where the stress seems to be high following 3 or more anterior cervical corpectomy constructs.8,9
The aim of our study was to review a single surgeon's experience and document the clinical and radiological outcomes of multiple levels (3 or more) of cervical corpectomy and anterior reconstruction.
MATERIALS AND METHODS
We retrospectively reviewed consecutive patients who had undergone 3 or more levels of anterior cervical corpectomy and reconstruction at our tertiary care unit from April 2014 to March 2018. The senior author (S.K.H.) performed all operations and a right-sided anterior cervical approach was the preference. Patient demographics, comorbidities, indication for surgery, and peri-operative data were all collected from available medical records. Clinical and radiological parameters were documented preoperatively and at 2 years of follow-up. Clinical outcome measures were recorded with Nurick grading10 and the modified Japanese Orthopedic Association score (mJOA).10 Radiological measures included cervical segmental angle, cervical sagittal angle, graft subsidence, and fusion rate. The above clinical and radiological parameters were documented preoperatively, in the immediate postop period, and at a 2-year follow-up. The fusion rate was analyzed using Bridwell criteria11 at the end of 2 years. Cervical segmental angle, cervical sagittal angle, and graft subsidence were measured using PACS software (Picture Archiving Communication System 20/20 Opal rad imaging software version 20.15.2).
To measure cervical segmental angle12 a line was drawn parallel to the superior endplate of the superior-most vertebra and another parallel line was drawn parallel to the inferior endplate of inferior vertebra to be involved in the fusion, and the angle between the 2 lines was measured.
To measure cervical sagittal angle12 parallel lines were drawn, inferior to the C2 and C7 vertebral bodies, perpendicular lines were drawn to the above lines, and the angle was measured.
To measure graft subsidence12 lines were drawn parallel to the superior endplate of superior vertebra and inferior endplate of inferior vertebra of the graft or cage. Midpoints of the above lines were marked, and another line was drawn connecting the midpoints. The line was measured for graft-cage height. It was measured in immediate postoperative period and at follow-ups. The difference in values at immediate postoperative period and at 2-year follow-up was taken as graft subsidence.
In our series all patients had anterior reconstruction with either an autogenous fibular strut graft or a titanium mesh cage packed with bone graft and rigid anterior cervical plating. Initially patients had anterior reconstruction with an autogenous fibula strut graft and rigid anterior cervical plate and later on our senior surgeon started using a titanium mesh cage filled with bone graft and rigid anterior cervical plating. Patients were divided into 2 groups according to anterior reconstruction with either autogenous fibular strut graft (group A) or titanium mesh cage and rigid cervical plating (group B) for subgroup analysis. Patients whose bone stock was found to be poor had undergone posterior instrumentation as a staged procedure. Institutional Review Board (IRB) exemption was granted from the IRB of Apollo hospitals for the study as it is a retrospective observational study. Ethical approval was waived by the local Ethics Committee, in view of the retrospective nature of the study and because all the procedures being performed were part of the routine care. Informed consent was obtained from the patients for undergoing the study.
Statistical analysis was done using SPSS software version 25.0 (IBM Corp, Armonk, New York). P < .05 was considered statistically significant. All continuous variables were represented by mean ± SD. Categorical variables were expressed as a percentage. Comparison of pre- and postcontinuous variables was done by paired t test. Comparison of continuous variables between 2 groups (A and B) was done by independent-sample t test.
RESULTS
There were 48 patients in the cohort. Mean age of patients was 58.1 years (range 48.4–75.6 years) with 79% of the cohort being females. Forty-two patients had undergone 3-level and 6 patients had undergone 4-level anterior cervical corpectomy and reconstruction.
Ossified posterior longitudinal ligament (OPLL) was the most common indication (62.7%) followed by cervical spondylotic myelopathy (19.4%). Other indications included complex cervical spine trauma (7.0%), spondylodiscitis (4.5%), implant failure due do prior surgery (4.3%), and metastases (2.1%). The commonest causative organism for spondylodiscitis was Mycobacterium tuberculosis. The multiple vertebral metastasis necessitating multilevel cervical corpectomy was from renal cell carcinoma in our series. The traumatic cases had a fall from height with axial loading ± flexion component as the mechanism of injury. The patients who had been operated for implant failure had index surgery elsewhere and screw failure at the caudal vertebral body with graft dislodgement being the reason for revision. Four patients had a history of thyroidectomy procedure prior to the cervical corpectomy. The majority of the patients had undergone C5 to C7 corpectomy (67%) followed by C4 to C6 corpectomy (Table 1). The majority of the patients had standalone anterior reconstruction with either fibular strut graft or titanium mesh cage and rigid anterior cervical plating. Eight patients (16.6%) whose bone stock was found to be poor from the feedback during screw insertion through the anterior cervical plate holes were supplemented with posterior instrumentation.
Levels of cervical corpectomy undergone by the study cohort.
Forty percent of the patients had systemic diseases including diabetes mellitus and systemic hypertension as comorbidities; 33.3% patients had history of smoking and 27.3% patients had osteoporosis. Of our cohort, 33.3% had multiple comorbidities (more than 2 comorbidities) (Table 2).
Comorbidity factors of patients.
Mean duration of surgery was 105 minutes (range 97–113 minutes) with mean surgical time for group A 111 minutes, and for group B, 99 minutes. Mean blood loss was 95 mL (range 85–105 mL). Mean duration of hospital stay was 2.1 days. The intraoperative complications included dural tear or cerebrospinal fluid (CSF) leak (8.3%) and small esophageal tear (2%). Postoperative C5 palsy (12.5%), transient hoarseness of voice (12.5%), and self-limiting temporary dysphagia (10.4%) were the commonest findings noted in the immediate postoperative period. There was no graft or anterior cervical plate dislodgement in our series at the 2-year follow-up. Common perioperative complications observed in our series are listed in Table 3.
Surgical complications encountered by the study cohort.
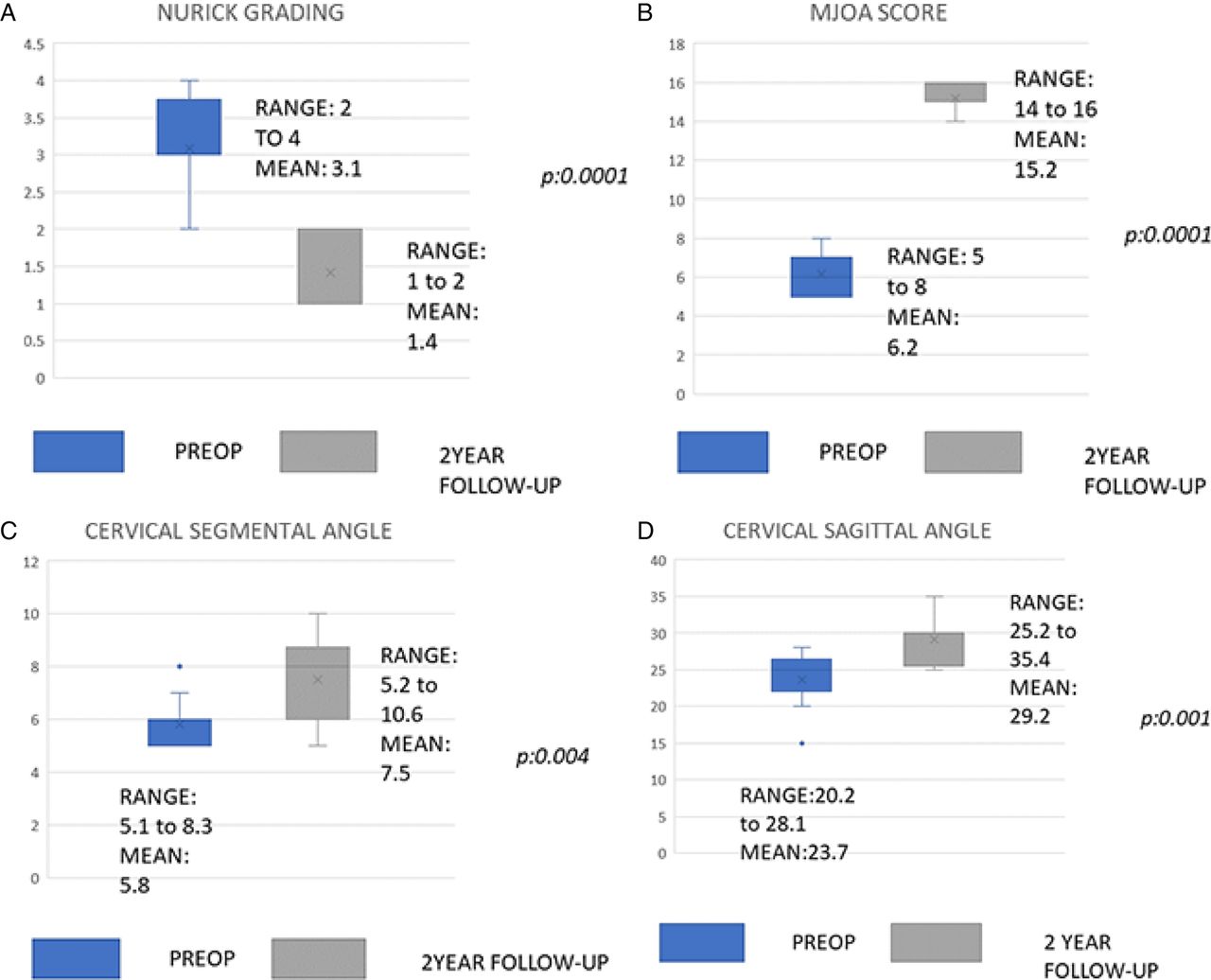
In group A, the Nurick score changed from baseline mean 3.0 ± 1.3 to 1.4 ± 1.0 postoperatively and mJOA score improved from 6.1 ± 2.2 to 15.1 ± 1.4. Similarly, radiological parameters of cervical segmental angle changed from 5.8° ± 1.8° to 7.5° ± 1.2° and cervical sagittal angle changed from 23.6° ± 7.4° to 29.1° ± 6.8°. In group B, the Nurick score changed from baseline mean 3.0 ± 1.3 to 1.9 ± 1.5 at 2-year follow-up, mJOA score improved from 4.9 ± 2.1 to 14.2 ± 2.9, cervical segmental angle changed from 5.1° ± 2.0° to 7.0° ± 3.3°, and cervical sagittal angle changed from 22.7° ± 7.2° to 30.1° ± 8.1°. Mean graft subsidence in group A was 3.0 ± 1.5 mm and in group B was 2.0 ± 1.1 mm. The incidence of graft subsidence was least with group B (25%, 6/24 patients), when compared to group A (41%, 10/24 patients). Mean change in all the parameters in both the groups A and B were statistically significant: P < .05. Statistics of group A and group B revealing the change in parameters between preoperative and at 2-year follow-up are tabulated in Tables 4 and 5, respectively. Figures 1 and 2 reveal box-and-whisker plot chart analysis of groups A and B, respectively.
Statistics of group A (autogenous fibular strut graft).
Statistics of Group B (titanium mesh cage and rigid cervical plating).
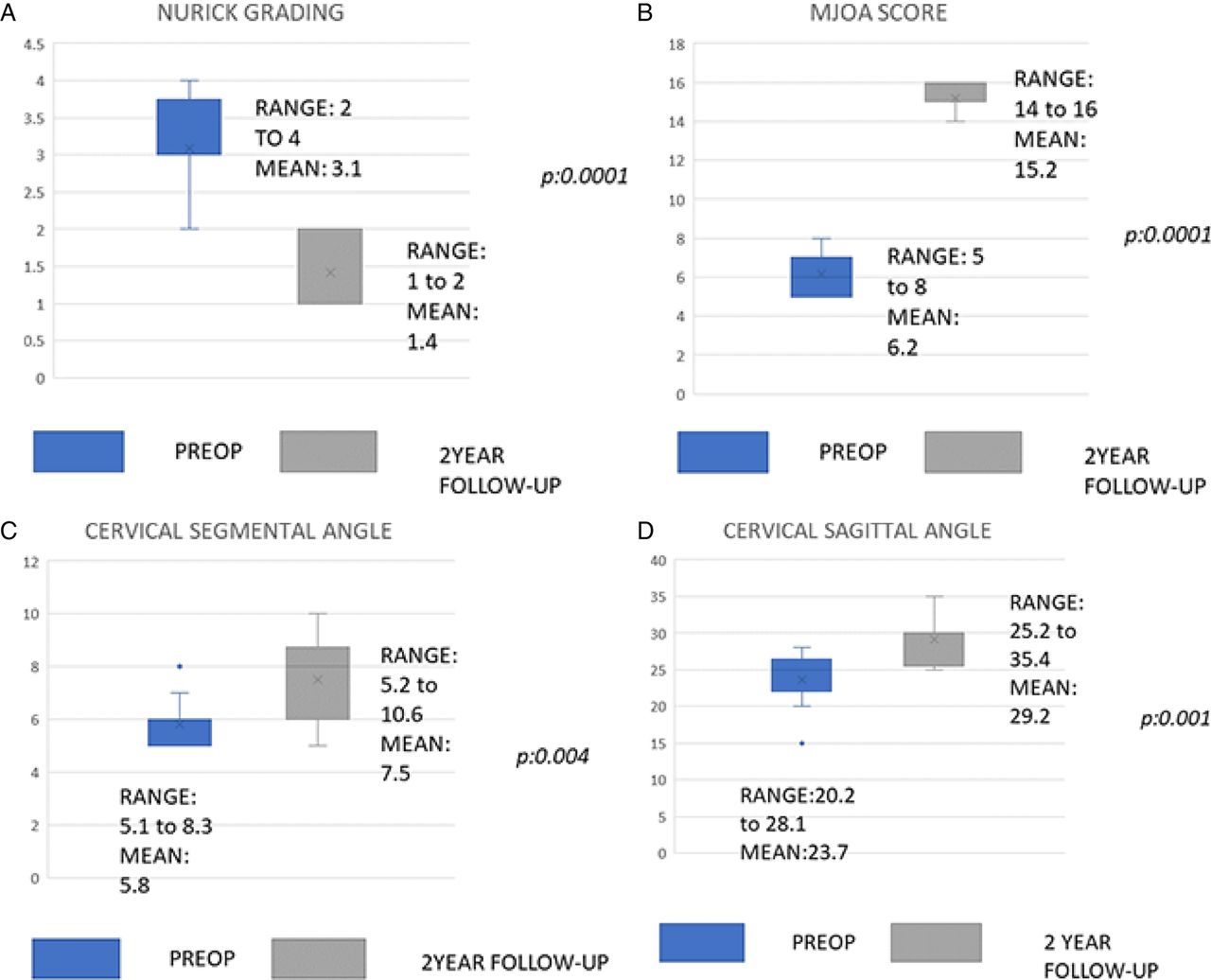
Box and whisker plot of group A patients (autogenous fibular strut graft). (A) Nurick grading, (B) modified Japanese Orthopedic Association (mJOA) score, (C) cervical segmental angle, (D) cervical sagittal angle.

Box and whisker plot of group B patients (titanium mesh cage and rigid cervical plating). (A) Nurick grading, (B) modified Japanese Orthopedic Association (mJOA) score, (C) cervical segmental angle, (D) cervical sagittal angle, (E) graft subsidence and fusion rate.
Mean Difference in Parameters Between the Groups
Our subgroup analysis revealed that there was no statistically significant difference in the baseline functional and radiological parameters between the groups except preoperative mJOA (Table 6). Both groups demonstrated improvement in functional and radiological measures at a 2 year follow-up and the difference in the improvement was not statistically significant. Group B had decreased incidence of graft subsidence, as well as lesser graft subsidence, and this was statistically significant P < .002. Overall fusion rate of the cohort was 89.5% with group B patients demonstrating higher fusion rate (95.8%) compared to group A (83.3%) at 2 years of follow-up and this was statistically significant (P < .001). Comparison of mean difference between the 2 groups is presented in Table 6.
Statistical difference between groups A (autogenous fibular strut graft) and B (titanium mesh cage and rigid cervical plating).
DISCUSSION
Historically, the evolution of graft usage after multilevel cervical corpectomy is of this order: usage of fibula autograft alone, fibula allograft alone, fibula auto or allograft with superadded plate and screws, and titanium mesh cage filled with bone graft with anterior cervical plate and screws. Wang et al6 have proposed a graft displacement rate of 9.9% and 16% following 3- and 4-level corpectomy. The graft displacement usually occurs at the caudal aspect of the graft. In their retrospective series, they had used autogenous fibula alone as long strut graft without an anterior plate. He states that graft migration and displacement are greater when the C7 vertebral body is involved in the inferior end of fusion construct. Macdonald et al7 used fibula allograft alone as strut graft and reports a failure rate of 11% following 3-level corpectomy (16 patients). They proclaim that the graft failure rate proportionately increases with single to 4-level corpectomy. Brezenor et al13 (22 patients) compared fibular allograft with titanium cage and plate fixation and reported titanium cage and plate fixation had a superior outcome to fibular auto- or allograft and dislodgement of graft is less with a titanium cage and plate. In the current series we compared patients who had fibular strut graft or a titanium mesh cage filled with bone chips with superadded cervical plate and screws for anterior reconstruction post multilevel corpectomy and observed no graft extrusion or cage dislodgement with superadded plate construct. Another interesting finding was that in our series, 67% of the corpectomies' reconstructed caudal end was at C7 and none had graft migration or displacement contrary to what has been documented in the literature.
Fusion rates have been found to be higher in long-level corpectomy constructs than in multilevel discectomy and graft constructs as the number of graft host bed surfaces decreases.14 Various authors have reported a fusion rate of 80% in their studies evaluating fibula strut autograft and titanium cage with plate fixation.13,15 In our study we found an overall fusion rate of 89.5% including both groups, with titanium cage and plate fixation group illustrating higher fusion rate (95.8%) than fibular autograft and plate fixation group (83.3%) (Table 7). We also observed less graft subsidence and decreased incidence of graft subsidence in titanium mesh cage and plate construct group. The mean graft subsidence in group A (fibular strut graft) was 3 mm with incidence of 41% (10/24 patients) and in group B (titanium mesh cage) it was 2.0 mm with incidence of 25% (6/24 patients) at 2-year follow-up, indicating decreased incidence of graft subsidence in patients reconstructed with titanium mesh cage group. The cases of subsidence were asymptomatic and required no further intervention.
Fusion characteristics of patients in groups A (autogenous fibular strut graft) and B (titanium mesh cage and rigid cervical plating) at 2-year follow-up.
Our subgroup analysis revealed no difference in the change in radiological measures of cervical segmental and sagittal angle between the groups. However, both groups demonstrated significant improvement in functional measures at 2-year follow-up with mean improvements in Nurick grade and mJOA score in both the groups with grades of 1.9 and 9.1, respectively. An interesting observation is that the higher fusion rate and less graft subsidence noted in the titanium mesh cage and plate reconstruct group does not necessarily translate into superior clinical outcome.
Rajshekhar et al12 documented a rate of 15.2% CSF leak in their series. In our series CSF leak was found to be 8.3%. CSF leaks were managed by following sequential measures: suturing the dural tear if reparable, applying a collagen patch followed by augmentation with a thick layer of fibrin glue, nonsuction of local wound drainage, supine position for 24 hours, intravenous antibiotics for 48 hours, oral acetazolamide medication for 3–5 days and usage of a postoperative lumbar drain in cases where the tear could not be sutured.
In OPLL patients, the senior author always practices the floating-island technique when the ligament is adhered to the dura. A few authors12,15 recommend elective ventilation and steroids for a period of 24–48 hours following multilevel corpectomy as preemptive measure in anticipation of prevertebral swelling–associated respiratory distress due to the prolonged retraction of soft tissues intraoperatively. Sagi et al16 reported the incidence of postoperative airway obstruction requiring reintubation as 6.1% and 1.9%, with risk factors of operative time more than 5 hours, 3 consecutive-level cervical vertebral body exposure; C2, C3, C4 vertebral body exposure; and blood loss more than 300 mL. However, in our center where the study has been undertaken, we have not practiced elective ventilation as a routine and patients are weaned off endotracheal intubation at the end of surgical procedure. In our series we did not encounter any postoperative airway obstruction in the studied patients as two thirds of our patient cohort had undergone C5 to C7 corpectomy. In addition, our shorter operating time, avoiding prolonged soft tissue retraction, and practice of intermittent release of soft tissue retraction whenever not needed might have minimized the tissue trauma, subsequent edema development, and respiratory distress.
There are some debates regarding the use of anterior cervical plates following multilevel anterior cervical corpectomy. A few authors suggest that plate bending, distal screw failure, caudal dislodgement of plate, and subsequent esophageal irritation are of concern with the use of plates.17,18 The number of levels of corpectomy correlate proportionately to the failure of plate.5,19 However, a few authors recommend anterior cervical plate usage as it provides immediate stability, stabilizes the graft, and promotes bony fusion.20–22 A few authors recommend supplemental posterior instrumentation along with 3 or more cervical corpectomy anterior constructs to decrease the stress at the caudal vertebral body and minimize graft- or implant-related failure.9–11 In our series, the majority had standalone anterior reconstruction and our senior author prefer staged supplemental posterior instrumentation following 3 or more anterior cervical corpectomies if the bone stock was felt poor whilst inserting anterior plate screws. In our series, 16.6% of patients underwent posterior instrumentation as a supplemental procedure. We have not observed any graft dislodgement, screw extrusion, or plate failure in our series at 2-year follow-up in standalone anterior reconstruction patients in our series. Our findings support that a superadded cervical plate in anterior reconstruction following multilevel corpectomy stabilizes the graft, provides immediate stability to the construct, and favors higher fusion. We like to stress that the graft carpentry and optimal fusion-bed preparation are other detrimental factors that dictate the success of anterior reconstruction alone following multilevel corpectomy.
Literature documents esophageal injury rate of 7.4% and esophageal perforation rate of 0.02% to 1.49% following anterior cervical spine surgery.23 In our series 2% of the cohort had inadvertent esophageal injury and none of the patients had esophageal perforation. The injury was small serosal tear that was managed conservatively in the immediate postoperative period with naso-gastric tube insertion. The tube was left for a period of 7–10 days and then removed. In our series, 10.4% of the cohort had transient dysphagia for solid foods for a mean period of 9.5 days (range 7–12 days). A meta-analysis by Wang et al24 reports 50% incidence of transient dysphagia on the immediate postoperative week after the anterior cervical procedure and 3% of persistent dysphagia at 1 year after the procedure. In our series, no dysphagia issues were seen at long-term follow-up following multilevel cervical corpectomy and reconstruction.
We had used a right-sided approach with longitudinal incision in all our patients, and observed transient hoarseness of voice in 12.5% of our patients for a mean period of 21.4 days. Jung et al25 reports overall incidence of postoperative recurrent laryngeal nerve palsy as 25%, with 8.3% being clinically symptomatic and 15.9% being clinically unapparent in his series with a left-sided approach.
Nassr et al,26 in their paper on incidence of C5 palsy following multilevel cervical decompression procedures, documented an incidence of 5.1% for a single corpectomy level; it proportionately increased as the number of corpectomies increased beyond 3. They reported spontaneous recovery in the majority of patients within 40 months postsurgery and 15.4% to have persistent residual deficit. We had 12.5% (6/24 patients) of patients developing C5 palsy in our cohort with most of them resolved postsurgery; 6.25% of patients had residual deficit by 2 years of follow-up. All cases of C5 palsy were documented in the immediate postoperative period following anterior cervical reconstruction surgery. Supplemental posterior instrumentation as second stage was done in 8 patients (16.6%) and no new C5 palsy was documented.
The risk of C5 palsies occurring following anterior, posterior, or circumferential spine surgery varies from 0 to 30%. However, similar rates have been documented after anterior and posterior decompression indicating a common pathway in the development of the condition. The inherent nature of decompression at C5, whether anterior or posterior, may have similar effects on the spinal cord or spinal canal which contribute to the development of the palsy.27,28
The presence of preoperative kyphotic sagittal alignment has an adverse biomechanical influence on the standalone anterior cervical construct.29 In our series the mean ± SD preoperative cervical sagittal alignment measured with C2-C7 Cobb angle was 23.2° ± 3.6°, indicating the preserved normal sagittal alignment of our cohort and this had improved to 29.7° ± 3.8° at 2-year follow-up. In this series the majority of the study cohort had maintained normal sagittal alignment preoperatively and had much improved results following multilevel cervical corpectomy and reconstruction procedure.
Maxwell et al,30 in a paper on cervical spondylotic myelopathy (58,115 admissions on the national database), stated that a single-level cervical corpectomy carries a mortality rate of 0.6%, and a single postoperative complication following the procedure increases the mean inpatient stay of the patient to another 4 or more days, and increases the mortality rate 20- fold. Patients aged more than 84 years had a 40-fold rise in adverse outcomes and a 5-fold increase in medical complications, and elective admissions of patients rather than emergency admissions were associated with lower mortality rate. The same authors31 claimed the mortality rate doubles to 1.2%, if a patient undergoes 3 or more cervical corpectomies. They also report a return-to-operating-room rate of 17.9% and a graft or instrumentation failure rate of 5.4% compared to patients who had undergone single-level corpectomy, with rates of 6.2% and 1.8%, respectively. Patients who had returned to the operating room had still-higher mortality of 7%, when compared to the other group. Their analysis identified age, American Society of Anesthesiologists class of more than 3, history of cancer, and presence of diabetes as the determinants of mortality. In our series, we did not have any incident of unplanned returns to the operating room and our mortality rate was nil though 33.3% of patients had multiple comorbidities.
A limitation of this study is its retrospective nature. Our series is one of the largest on the subject and a comparison of our results with existing studies is tabulated in Table 8. Interpretation of our data and the statistical analysis refute the hypothesis that surgical outcome is worse in patients who undergo 3 or more anterior cervical corpectomies with standalone anterior reconstruction for long-segment anterior cervical compression (Figures 3–6).
Comparison of results of other authors with our series.

Preoperative radiograph image of 65-year-old female who had compressive myelopathy due to an ossified posterior longitudinal ligament.
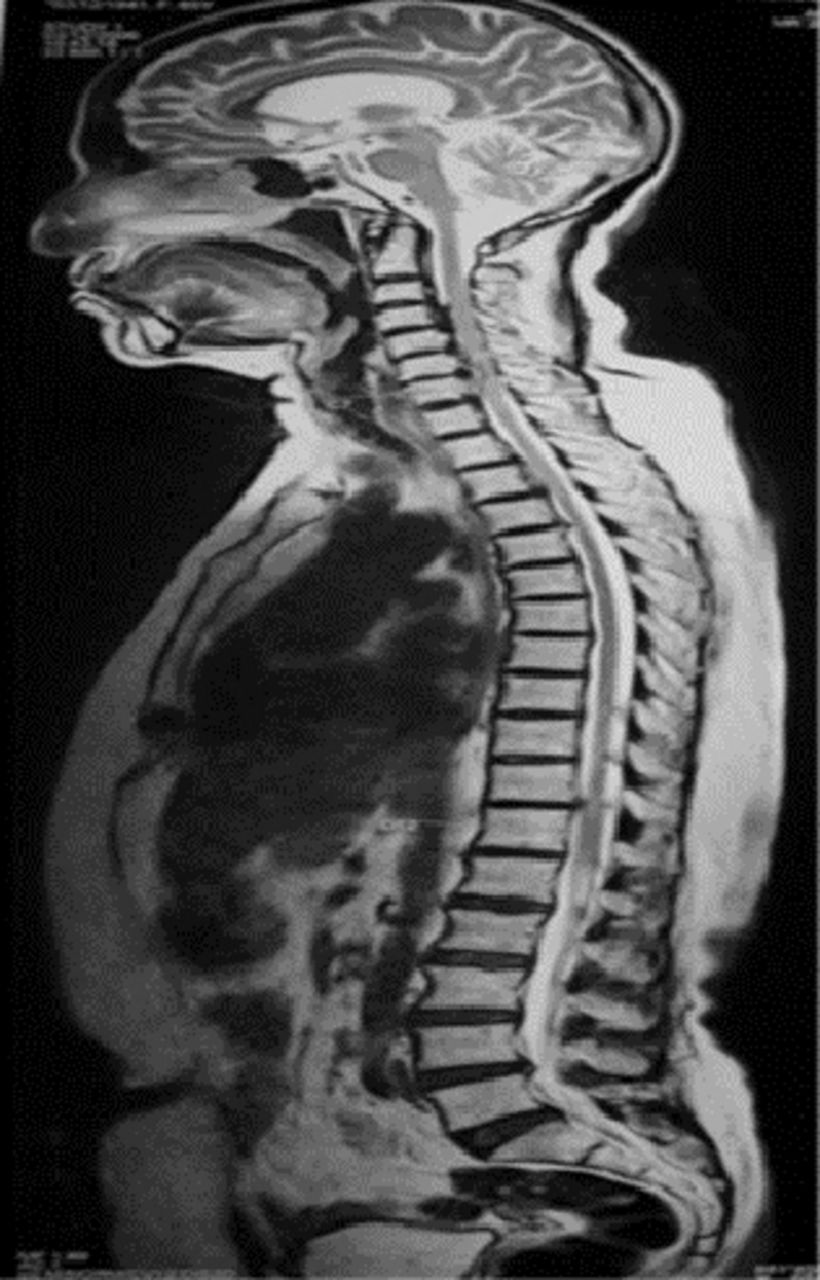
Preoperative magnetic resonance imaging image of 65-year-old female who had compressive myelopathy due to an ossified posterior longitudinal ligament.

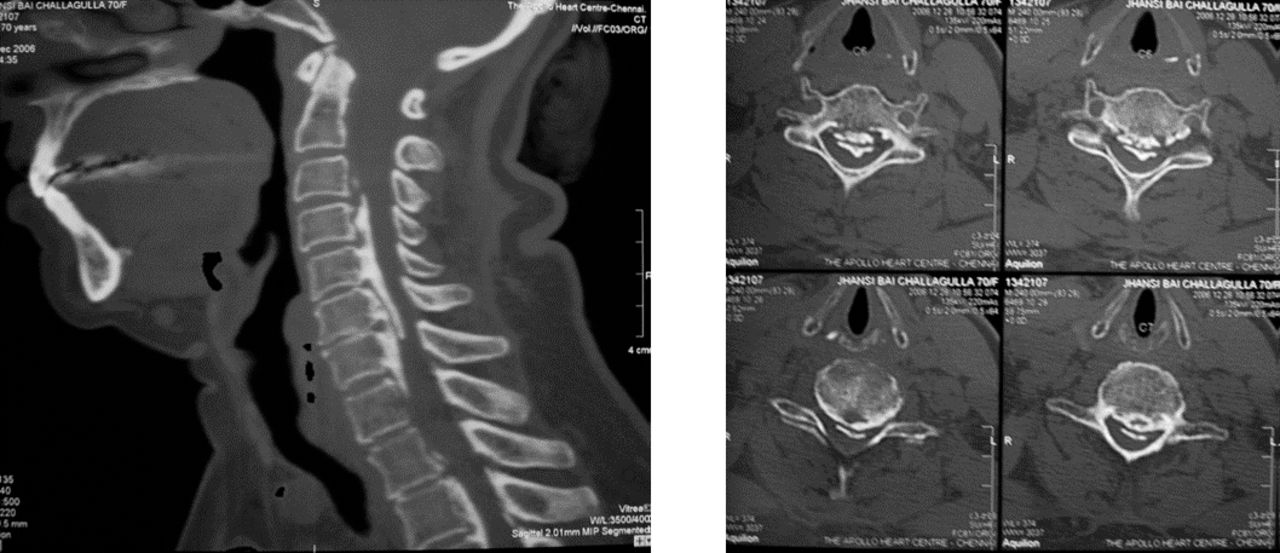
Preoperative computed tomography image of 65-year-old female who had compressive myelopathy due to an ossified posterior longitudinal ligament.

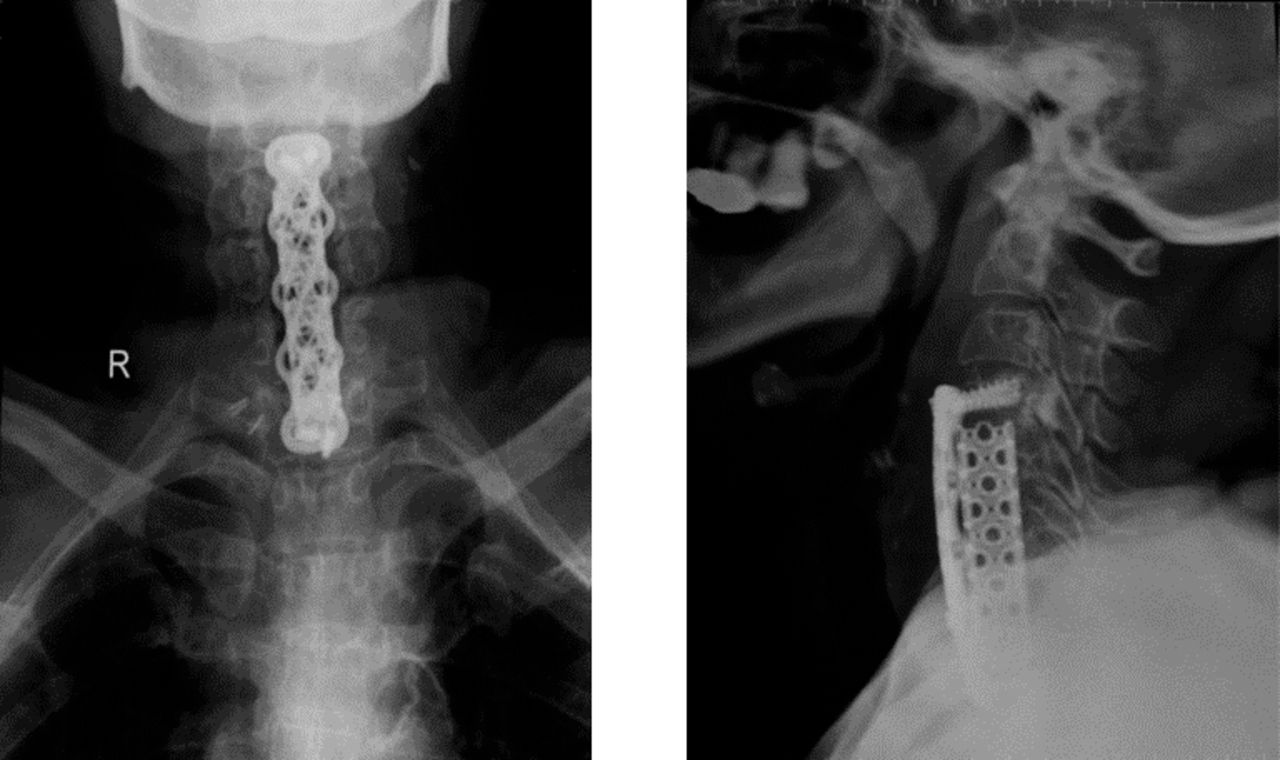
Postoperative radiograph at 2-year follow-up of 65-year-old female after undergoing C5–C7 corpectomy and anterior reconstruction.
CONCLUSION
Multilevel anterior cervical corpectomy and reconstruction is a safe and efficacious procedure. A titanium mesh cage filled with autogenous bone graft with a contoured anterior cervical plate gives best results. Posterior instrumentation should be considered along with a multilevel cervical corpectomy construct in poor bone stock patients.
Footnotes
Disclosures and COI: The authors declare no conflicts of interest. No funding was received from any external agency for undertaking the study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.