


Abstract
Background Cervical diffuse idiopathic skeletal hyperostosis (DISH) fractures are frequently unstable and carry significant risk of neurologic injury and death. Most patients with DISH fractures are elderly (>70 years) with significant comorbidities. We assessed factors that contribute to outcomes in elderly patients with cervical DISH fractures.
Methods Elderly patients with cervical DISH fractures from 2008 to 2017 were included in this retrospective multi-institutional cohort study. Predictor variables included injury level, surgical approach, preinjury comorbidities, American Society of Anesthesiologists (ASA) score, American Spinal Injury Association (ASIA) impairment scale grade, preoperative anticoagulation status, and the subaxial cervical spine injury classification system (SLIC) score. Univariate and multivariate analyses were utilized to identify factors associated with 30-day mortality and ambulatory status at discharge.
Results A total of 48 patients, mean age 74.7 years old (range 60–96), underwent cervical fixation for DISH fractures. Average SLIC score was 6.30 ± 1.2 (range 5–8), and most frequent fracture level was at C6 to -C7 (31.3%) followed by C7–T1 (25.0%). Forty (83.3%) patients underwent posterior fixation, 7 (14.6%) with anterior fixation, and 1 (2.1%) had combined approach. Ten (20.4%) patients died within 30 days of surgery. Multivariate analysis demonstrated that poorer preoperative ASIA grade (OR 2.35, P = 0.003, CI = 1.33–4.14) and ASA score >3 (P = 0.027) had increased risk of being nonambulatory at discharge. Higher SLIC score was associated with increased 30-day mortality (P = 0.021, CI = 1.20–9.60).
Conclusions Cervical DISH fractures can be highly unstable, for which instrumentation and fixation are indicated. Surgical decision-making should focus on preoperative ASIA grade, SLIC score, and ASA score.
Clinical Relevance The study is relevant due to an aging poulation predisposed to cervical DISH fractures.
Level of Evidence 4.
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is an ankylosing spinal disorder highly associated with male sex and age over 50 years.1,2 As the general population continues to age, the prevalence of DISH is increasing. It is a noninflammatory systemic condition characterized by osseous fusion of the anterolateral aspect of at least 4 vertebral bodies with relative preservation of vertebral disc height in the involved segments without degenerative disc disease.3,4 The Resnick criteria is used to classify each vertebral level with DISH based on the amount of ossification and degree of disc space bridging.4,5 While the outcomes are often similar to ankylosing spondylitis, the underlying pathophysiology of DISH is distinct.
Ossification in DISH predominantly occurs in the anterior longitudinal ligament with minimal paravertebral connective tissue involvement.6 In the cervicothoracic spine, involvement of the posterior longitudinal ligament may result in spinal stenosis.7,8 The resulting ankylosis dramatically changes the biomechanics of the spine. The fused spinal segments act as a long lever arm with increased rigidity that results in decreased impact resistance and susceptibility to complex injuries, even with low impact trauma.9,10 DISH fractures tend to be highly unstable. Given the risk of sudden neurological deterioration, operative management is often considered.
There are currently limited data assessing cervical spine fractures in DISH patients regarding surgical outcomes and survival. Advanced age, an increased number of comorbidities, and low energy mechanism of injury are associated with higher morbidity and mortality.5 In one study, Bransford et al found that only 22% of patients with operative cervical DISH fractures had neurological improvement.11 Given the high rate of medical comorbidities and surgical complications in these patients, there is a critical need for data demonstrating which preoperative risk factors and pre-existing comorbidities best identify patients’ morbidity and mortality from surgery. We present the largest operative cohort study describing morbidity and mortality in association with preoperative risk factors in elderly patients diagnosed with cervical and cervicothoracic DISH fractures.
Methods
Study Design
This is a multicenter retrospective cohort study from 2008 to 2017. All data were collected under the approval of the Institutional Review Boards of each institution. Patients were eligible for study inclusion if they were >60 years old, had DISH as defined by the Resnick criteria, had a fracture in the cervical and/or cervicothoracic spine demonstrated on computed tomographic image, and were treated operatively via anterior, posterior, or anterior/posterior approach. All patients were treated as soon as medically safe. Patients with a diagnosis of ankylosing spondylosis (AS) were excluded. Forty-eight patients met the above criteria. Informed consent was obtained for each patient or from the legal authorized representative for proxy consent. All data in the current study were deidentified in the analysis and are presented as such. The study did not need approval by the local Institutional Review Board.
Evaluation of Patient Characteristics
Descriptive characteristics included patient age, preinjury medical comorbidities, Charlson Comorbidity Index (CCI), level of injury, injury severity, American Society of Anesthesiologists (ASA) score, preoperative anticoagulation status, pre- and postoperative American Spinal Injury Association (ASIA) impairment scale grade, and surgical approach. Fracture characteristics were assessed by level of fracture, levels of DISH pathology above and below the fracture, and subaxial cervical spine injury classification system (SLIC) score. Outcome measures consisted of ambulation at discharge and 30-day mortality.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics (SPSS Inc., Chicago, Illinois). Univariate statistics were calculated using χ 2 tests for categorical variables, and independent sample t tests were used for continuous variables. Multivariate logistic regression was utilized to identify factors independently associated with 30-day mortality and ambulatory status at discharge. Statistical significance was accepted at a P value of <0.05.
Results
Patient Demographics and Fracture Characteristics
Patient demographics and comorbidities were summarized in Table 1. A total of 48 patients (42 men, 87.8%; 6 women, 12.2%) with operative DISH fractures at the cervical and cervicothoracic spine were identified. The mean age was 74.7 ± 9.18 (range 60–96) with a mean body mass index (BMI) of 31.9 ± 8.33 (range 19–58.5). The most common comorbidity was hypertension (n = 40; 87.5%), followed by diabetes mellitus (DM) (n = 22; 45.8%), coronary artery disease (n = 20; 41.6%), congestive heart failure (N = 7; 14.6%), and chronic obstructive pulmonary disease (n = 5; 10.4%). Fifteen (31.3%) patients were being treated with anticoagulation therapy at the time of presentation. The number of comorbidities per patient was distributed as follows: 5 patients (10.4%) had no included comorbidities; 16 patients (33.3%) had 1 comorbidity; 11 patients (22.9%) had 2 comorbidities; 9 patients (18.8%) had 3 comorbidities; and 3 patients (6.3%) each had 4 and 5 comorbidities. The mean preoperative CCI was 5.14 ± 1.71 (range 2–10).
Patient characteristics (N = 48).
The average number of ossified disc spaces was 5.2 ± 1.9 (range 3–8). The average number of ossified disc spaces above the fracture was 2.2 ± 1.4 (range 1–5) and below was 2.4 ± 1.3 (range 1–4). Regarding level of fracture, 5 patients (10.4%) fractured C3-C4, 10 patients (20.8%) fractured C4-C5, 6 patients (12.5%) fractured C5-C6, 15 patients (31.3%) fractured C6-C7, and 12 patients (25.0%) fractured C7–T1. The average SLIC score was 6.30 ± 1.2 (range 5–8).
Treatment Data and Complications
All patients in the study were treated operatively with either anterior or posterior fixation or a combination of both (Table 2). The majority of patients (N = 40; 83.3%) had posterior fixation, 7 (14.6%) had anterior fixation, and 1 (2.1%) patient had anterior and posterior approach. Fifteen (31.3%) patients had procedures isolated to the cervical level, while 33 (68.7%) were fused at the cervicothoracic level. Twenty-three patients (48%) had a complication of either a surgical or a medical nature during their hospitalization. A total of 4 (8.3%) patients suffered intraoperative surgical complication, and 4 (8.3%) had postoperative wound infection requiring reoperation. Two (4.2%) patients required reoperation due to hardware failure. Both of these patients had an anterior cervical discectomy and fusion as their index surgery at the time of injury and required a posterior decompression and fixation within 3 months postoperatively. Two patients suffered pulmonary embolism (4.1%). Pneumonia was the most common complication (N = 12; 25%), and patients with DM and hypertension were significantly more likely to develop pneumonia (P = 0.019 and P = 0.012, respectively).
Description of surgical characteristics, ASIA grade, complications, and outcomes.
Functional and Neurological Status
At the time of presentation, 27 (56.3%) patients were classified as ASIA grade E, 11 (22.9%) as ASIA D, 3 (6.3%) as ASIA C, 1 (2.1%) as ASIA B, and 6 (12.5%) as ASIA A (Table 2). The mean time to follow-up was 12.5 ± 7.0 (range 2–24) months. At the time of follow-up, 13 (27.1%) patients had an improved ASIA grade, 34 (70.8%) had a stable grade, and 1 (2.1%) patient worsened. Of the 13 with improved an improved grade, 10 (71.4%) improved from ASIA D to E, 3 (21.4%) improved from C to D, and 1 (7.1%) improved from A to B (Figure).
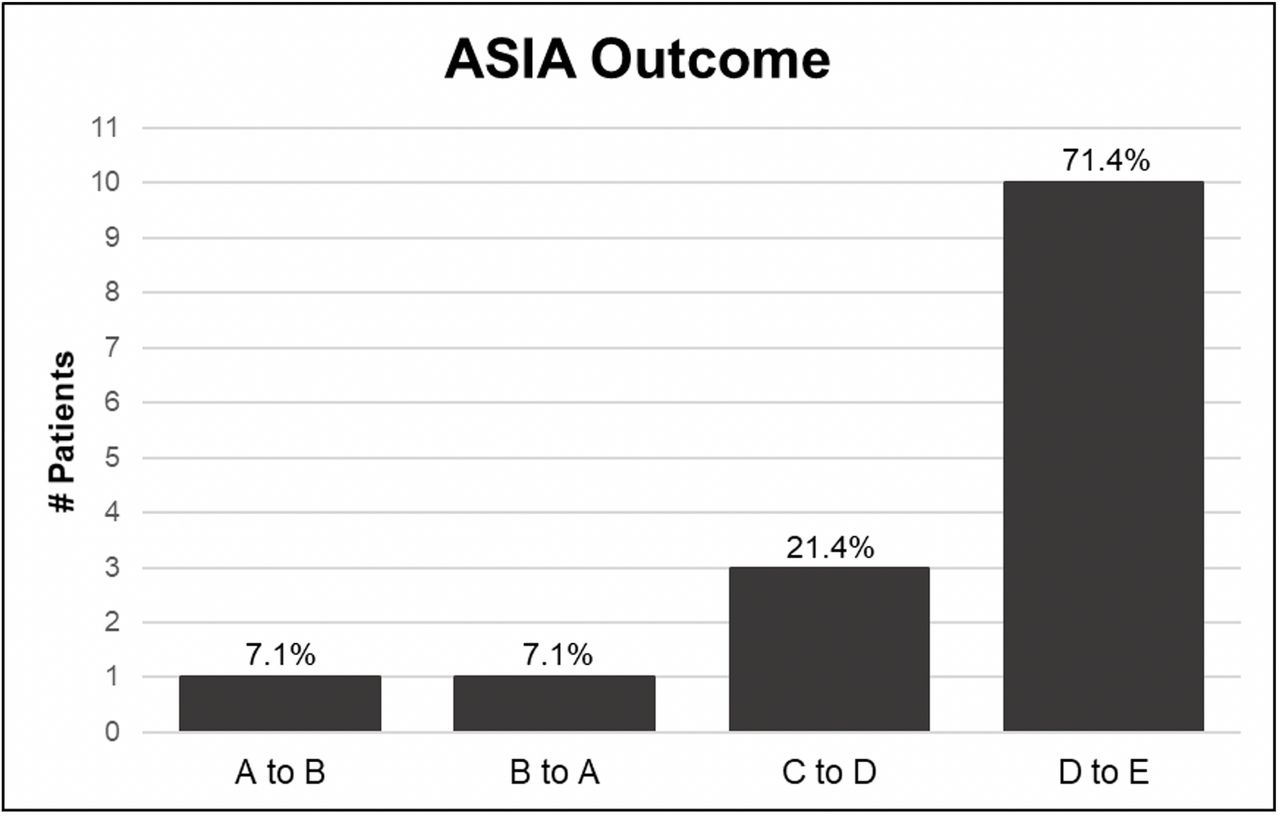
American Spinal Injury Association (ASIA) impairment scale grade outcomes for 14 patients whose score changed postoperatively. For all 14 patients, the score only changed by 1 increment. Percentages represent percent of total patients with changed scores.
Factors Affecting Ambulation and Mortality
At the time of discharge, 33 (68.8%) patients were ambulatory (Table 2). On univariate analysis, an ASA score of >3 (P = 0.048), poorer preoperative ASIA grade (P = 0.010), and history of a prior spine surgery (P = 0.045) were significantly associated with being nonambulatory at discharge (Tables 3 and 4).
Univariate analysis of outcome dependence on preoperative variables.
Univariate analysis of outcome dependence on preoperative and postoperative ASIA grade.
Multivariate logistic regression was performed using the variables: age, preoperative ASIA grade, anticoagulation, BMI, SLIC score, and ASA score >3 (Table 5). On multivariate analysis, ASA score >3 (P = 0.027), poorer preoperative ASIA grade (P = 0.003), and higher SLIC score (P = 0.018) remained independent predictors of being nonambulatory at discharge (Table 5). Per 1-letter increase in ASIA grade, there was a 2.35 increase chance of being nonambulatory at discharge (P = 0.003, 95% CI = 1.33–4.14) and 3.61 increased chance of 30-day mortality. Per 1-point increase in SLIC, there was a 2.9 increased chance of being nonambulatory at discharge (P = 0.018, 95% CI = 1.20–7.07). Per 1-point increase in SLIC score, there was a 3.4 increased chance of 30-day mortality (P = 0.021, 95% CI = 1.20–9.60). CCI was not significantly associated with ambulation at discharge (P = 0.881, 95% CI = 0.72–1.47) or 30-day mortality (P = 0.790, 95% CI = 0.59–1.49).
Multivariate analysis demonstrating independent association of preoperative variable on outcomes.
Ten (20.4%) patients died within 30 days of surgery (mean 20.9 ± 11.1 days; range 2 to 30), 5 of whom were neurologically intact at presentation. For the cases in which cause of death could be identified, respiratory failure (N = 4) and cardiac arrest (N = 3) were the most common causes of death. Six (46.2%) patients with a respiratory complication from surgery died within 30 days. The patient’s BMI, pre-existing comorbidities, and anticoagulation therapy had no significant association with ambulation at discharge or 30-day mortality.
Discussion
Cervical spine injuries that occur in the context of DISH represent a particularly difficult patient population to treat. These patients are typically older, have multiple comorbidities, and experience poorer outcomes. Current data assessing DISH fractures of the cervical and cervicothoracic junction remain limited. Furthermore, most analyses of DISH fractures are often categorized into the same subset as AS patients, which does not allow for the particular nuances of this group to be appreciated. In this study we provided the largest cohort of patients and most comprehensive analysis of preoperative risk factors predicting morbidity and mortality in patients with cervical or thoracic DISH fractures. In the present study, we determined that preoperative ASA score, SLIC score, and ASIA grade correlated with poorer outcomes. Choice of surgical approach for fusion was not correlated with postoperative outcomes.
Preoperative Comorbidities
Consistent with previous studies, the majority of patients in the current study were men (87.9%), elderly (mean age, 74.7 years), and had at least 1 comorbidity at presentation (89.6%; Table 1). Previous studies have reported a mortality rate of 10% to 27% in patients with operative surgical DISH fractures.11,12 Similarly, we found that 20.4% of patients died within 30 days of surgery. Furthermore, the postoperative complication rate in cervical DISH fractures has been reported to be as high as 61% to 75%.13 In the current study, 48% of patients experienced postoperative complications. Furthermore, our data showed that CCI was not associated with worse outcomes (Table 5). Several studies have been published in support of the reduction of morbidity associated with earlier time to surgery.14–17 In our cohort, our time to surgery ranged from 3 to 72 hours. Tsujui et al found that patients are more likely to have neurological improvement if operated on within 8 hours of injury.13 Furthermore, treatment delay has also been shown to result in worsening neurological function in 20% to 80% of patients.3
In this study, we evaluated preoperative comorbidities to determine whether any of these factors put patients at a higher risk for postoperative complications and mortality. We found that poor preoperative ASIA grade, an ASA score >3, and SLIC scores were the only significant independent predictors of being nonambulatory at discharge and 30-day mortality. Age, BMI, preoperative anticoagulation, and other preoperative comorbidities (DM, hypertension, coronary artery disease, congestive heart failure, and chronic obstructive pulmonary disease) were not related. Current literature regarding prognostic factors in cervical DISH fractures has been highly discordant. Here we found no association between age and morbidity or mortality in univariate or multivariate analysis.
The ASA physical status classification is a risk stratification tool using a patient’s general health and comorbid medical conditions, and has recently been shown to be as a useful risk stratification tool for spine surgeries.18 In a survey of 22,857 patients with a documented ASA score who underwent spinal surgery, patients with higher ASA grades had higher complication and mortality rates, a trend that also held true when patients with adult spinal deformities were analyzed as a subgroup.19,20 Consistent with these data, we found that a higher ASA score (>3) predicted inability to ambulate at discharge and 30-day mortality.
It is common to encounter elderly patients with comorbidities requiring anticoagulation therapy. However, there is significant variability in practice patterns among spine surgeons regarding the safety of surgical repair of traumatic spine fractures in patients on anticoagulation therapy due to the feared complication of postoperative bleeding complications.21,22 To our knowledge, no previous studies have investigated anticoagulation therapy as a predictor of morbidity and mortality in DISH fractures. In the present study, we found that anticoagulation status had no effect on outcomes. This finding is consistent with data within the orthopedic surgery literature, which state that preoperative anticoagulation therapy had no increased risk of postoperative bleeding complications in patients with operative traumatic spine fractures.23,24
Spinal Cord Injury
Elderly patients, particularly those with ankylosing spinal disease, have significantly higher risk of spinal cord injury (SCI) than those with fractures in a mobile spine.25,26 Poor preoperative neurological examination findings have been consistently shown to predict worse outcomes in patients with cervical DISH fractures. In fact, mortality rates have been reported to be 26% to 100%, and complete SCI carries 5 times greater risk for mortality compared with patients with incomplete SCI.27,28 Furthermore, Tsuiji et al, found that all the deaths in their series were due to severe pulmonary disorders related to complete cervical SCI.13 In another study, adverse events and mortality were significantly higher in patients who suffered an SCI regardless of fracture location in the spine.29 Similarly, 3 of the 4 patients in our study who presented with a complete SCI injury died by 30 days, and poor preoperative ASIA grade predicted 30-day mortality in the absence of other factors. Therefore, we found that morbidity and mortality in DISH-associated cervical and cervicothoracic fractures appear to occur primarily as a result of the injury severity and the inability to recover from this injury rather than an exacerbation of any prior medical comorbidity.
Surgical Management
Cervical fractures in DISH tend to be highly unstable, and surgical management involving anterior and/or posterior fixation is typically indicated to avoid neurologic sequelae. While posterior long segment fusion has been traditionally acknowledged as the treatment of choice for thoracic and lumbar fractures, superiority of surgical approach at the cervical and cervicothoracic in DISH is a topic of discussion. Anterior approaches can be associated with dysphagia and worsening of pathologic kyphosis. In studies of patients with AS and DISH, the biomechanical inferiority of the anterior approach has been characterized by postoperative hardware failures requiring early surgical revision.29–33 In fact, the 2 patients who required reoperation in our study were originally anterior approach surgeries that developed postoperative kyphosis requiring revision with posterior instrumentation. Alternatively, posterior surgical approach is not without associated risks.34 Prone positioning can predispose the patient to a greater risk of cardiopulmonary complications.35 Overall, our data showed no significant difference between surgical approach and postoperative complications.
Patients with cervical fractures in the context of DISH are typically poor surgical candidates with multiple comorbidities, resulting in higher rates of medical and surgical complications. However, patients who were managed conservatively can have a higher risk of complications and mortality compared to patients treated operatively.3,36 The SLIC categorizes injury severity for prognostication and management, with a patient score greater than 4 being considered an indication for surgery.34 The pathologic biomechanics of DISH make fractures highly unstable. Despite the high morbidity and mortality associated with surgery in patients with DISH, operative management remains superior to conservative management and should be considered as a first-line intervention for all patients that can tolerate surgery.
Limitations
This study sought to advance the current literature aimed at predicting which elderly patients are at the greatest risk for morbidity and mortality following surgical management of cervical and cervicothoracic DISH-associated fractures. However, it is important to acknowledge the limitations. This is a retrospective review of outcomes, resulting in inherent limitations, including the possibility of referral bias. Additionally, although this is the largest cohort study of its kind to date, it is still limited by a relatively small sample size. Despite these limitations, we believe the results can be reasonably generalized to populations with similar presentations.
Conclusion
In this study, age and preinjury comorbidities were not predictive of ambulation at discharge and 30-day mortality. Surgical decision-making should focus on preoperative neurological examination, SLIC, and ASA score as opposed to the patient’s preinjury comorbidities. Despite high rates of complications and mortality, operative management remains superior to conservative management of patients with cervical DISH fractures.
Footnotes
↵AO and JLP are joint first authors.
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This study was exempt as it contains no identifiable patient data.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.