


Abstract
Objective Both under- and overcorrection are risk factors for junctional failure after deformity correction. This study investigates which factors determine the segmental radiographic outcome in mini-open lateral deformity surgery.
Methods A single-center operative database was searched for patients undergoing multilevel mini-open lateral corrective surgery of degenerative spinal deformities. Preoperative and postoperative whole spine x-rays and computed tomography scans were compared for change in global and segmental alignment parameters. Linear regression analyses were performed to study the impact of surgical level, preoperative segmental sagittal Cobb angle, presence of bridging osteophytes, disc height, ankylosis of facet joints, and implantation site of the interbody device on postoperative increase in segmental lordosis, foraminal height, and foraminal width.
Results A total of 49 patients were identified with a mean age of 68.7 years. At a mean, 4.2 segments were fused using a lateral approach, while the posterior stage comprised either minimally invasive surgery or open instrumentation. Upper instrumented vertebra was L2 (range T4-L3), and lower instrumented vertebra was L5 (range L4-pelvis) in most cases. Mean radiographic values pre- and postoperatively were as follows: C7 sagittal vertical axis +79.6 mm, +60 mm; lumbar lordosis 32.9°, 41.6°; pelvic tilt 21.1°, 21.8°; global coronal Cobb 16.3°, 10.8°; increase in segmental sagittal Cobb angle was significantly and inversely correlated with preoperative sagittal Cobb and positively correlated with preoperative coronal Cobb angle. No other variable showed significant correlations. Preoperative foraminal width and height showed significant and inverse correlation with change in postoperative foraminal width and height.
Conclusion Segmental sagittal correction is significantly influenced by preoperative loss of lordosis and coronal Cobb angle. Neither presence of osteophytes nor ankylosed facet joints, disc height, or implantation site of the interbody device had an influence on sagittal alignment goals. Only preoperative foraminal dimensions impact inversely the degree of foraminal decompression; no other factor investigated showed significant impact.
Clinical Relevance Only preoperative lordosis and coronal Cobb angle influence sagittal correction.
Level of Evidence 4.
Introduction
Mini-open retroperitoneal fusion techniques, comprising the direct lateral and oblique lateral approach,1,2 can be applied to a subset of patients with adult spinal deformities to realign the spine in the coronal and sagittal planes. In addition to improving sagittal and coronal alignment of the spine, indirect decompression of neural structures is another benefit of these approaches, which can be particularly useful in patients with degenerative scoliosis.3 Significant coronal and sagittal correction, as well as indirect decompression of the foramina and spinal canal, can be achieved solely by the implantation of a lordotic interbody device that spans the apophyseal ring. This maneuver reconstructs physiologic segmental alignment of the disc space. In a subset of patients with degenerative spinal deformities, this minimally invasive approach has been shown to offer advantages over open posterior only correction techniques, including reduced blood loss.4
Compared to posterior or transforaminal interbody fusion, significantly less soft tissue disruption is necessary to access the disc space, since the approach utilizes a muscle splitting technique, rather than a subperiosteal dissection. Furthermore, larger footprint cages, which rest on the apophyseal ring rather than cancellous bone underlying the vertebral body endplate, allow for a more pronounced correction of segmental sagittal and coronal alignment. Significant disc space restoration leads to widening of the segmental neuroforamen, as well as increased cross-sectional area of the spinal canal occupied by the thecal sac. If the lateral approach is utilized over several segments, significant correction of both coronal and sagittal parameters may be achieved. Since under- and overcorrection are risk factors for junctional failure in deformity surgery, it is important to predict the radiographic outcome in mini-open lateral deformity surgery and to understand which factors have an impact.5
Factors that determine the degree of sagittal correction and neuroforaminal decompression in mini-open lateral spine surgery have not been studied in detail. This retrospective study aims to investigate the correlation between radiographic baseline characteristics and final radiographic outcomes after mini-open lateral spinal deformity surgery. The results should help clinicians predict the radiographic outcomes in minimally invasive retroperitoneal fusion techniques, thus optimizing outcomes.
Methods
After approval of the study by the institutional review board (IRB 20-0444), the procedural database was searched for patients undergoing at least 3-level lateral mini-open lumbar surgery between 1 January 2015 and 28 February 2020. Inclusion criteria were as follows: (1) age 18 years or older and (2) degenerative etiology of spinal deformity. Exclusion criteria were incomplete imaging data (pre- and postoperative computed tomography [CT] images and pre- and postoperative whole spine standing x-rays images) and incomplete clinical data.
Details of Surgery
Surgeries were performed by board-certified neurosurgeons. Electrophysiologic monitoring was utilized as well as intraoperative fluoroscopy. The lateral stage of the procedure was usually performed in a right lateral decubitus position. To access multiple disc spaces, a vertical skin incision was performed followed by sharp dissection of the subcutaneous tissue. Muscle layers of the abdominal wall were bluntly split and retracted. After the retroperitoneal space was entered, finger dissection and palpation were used to identify and expose the lateral surface of the psoas muscle. For each level, the desired annulotomy site was located under lateral fluoroscopy, followed by placement of a retractor system. Direct neurostimulation was used to verify correct positioning of the dilatator in relation to the lumbar plexus fibers. Under anterior-posterior and lateral fluoroscopy, a thorough discectomy including contralateral annular release was performed. The endplates were prepared with curettes. The best-fitting titanium cage with either 20 or 22 mm width and 45 to 60 mm length was packed with recombinant human bone-morphogenic protein and morselized allograft. Lateral plating was not performed. After completion of the lateral stage of surgery, the incision was closed in a layered fashion. The posterior stage has been performed either as part of the same operating session or as part of a second procedure with an interval of up to 1 week. The posterior stage of the surgery has been performed either open or minimally invasively using percutaneous instrumentation. Generally, open posterior stage surgery was performed after several days, whereas MIS posterior surgery was performed at the same session. In cases undergoing open posterior surgery, only direct decompressions were performed such as laminectomies, no osteotomies were performed.
Radiographic Analysis
The following radiographic measurements were obtained on pre- and immediate postoperatively performed whole spine standing x-ray imaging: pelvic incidence (PI), pelvic tilt (PT), L1-S1 lumbar lordosis (LL), segmental sagittal Cobb angle for each segment undergoing lateral interbody fusion, thoracic kyphosis (TK), C7 sagittal vertical axis (C7SVA), apex of the degenerative scoliotic curve, and coronal Cobb angle. PreoperativeCT images were used to obtain the following measurements for each motion segment undergoing lateral interbody fusion: (1) central disc space height, (2) grading of osteophytes spanning the disc space (grade I: osteophytes visible but not spanning the entire disc space; grade II: osteophytes spanning the whole disc space but not bridging the disc space; grade III: bridging osteophytes), (3) grading of facet joint degeneration (grade I: visible facet joint osteophytes; grade II: facet joint osteophytes spanning the joint space; grade III: facet joint ankylosed). Postoperative CT images were used to obtain central disc space height and implant position (position of the center of the interbody device in relation to the disc space, analog to Meyerding’s grading system) for each motion segment undergoing lateral interbody fusion. Standing whole spine x-ray and CT images were all obtained within 14 days of the index surgery.
Statistical Analysis
Analysis of variance linear regression analyses was performed using PSPP (GNU PSPP (2015), Free Software Foundation Boston, MA, USA). For each outcome variable (change in postoperative segmental sagittal Cobb angle, change in postoperative foraminal height, and postoperative change in foraminal width), a linear regression analysis was performed with the following variables: preoperative segmental sagittal Cobb angle, preoperative disc space height, preoperative osteophyte grade, preoperative facet joint degeneration grade, anatomic level, preoperative segmental coronal Cobb angle, preoperative foraminal height, preoperative foraminal width, and implant position.
Results
Details of Surgery
A total of 49 patients were identified. Mean age was 68.7 years, and 63% of the cohort was female (Table 1). Degenerative scoliosis was observed to have a left convexity of 63% with apex level at L2 in 25% of cases, at L4 in 6%, at L3/4 in 6%, L2/3 in 4%, and L1 at 1% of cases. The lateral stage of the surgery comprised mini-open transpsoas interbody fusion in 96% of cases and mini-open prepsoas interbody fusion in 4% of cases. Upper instrumented vertebra was L2 in 60% of cases, L1 in 11%, L3 in 10%, T10 in 6%, T4 in 2%, T11 in 2%, and T12 in 2% of cases. Mean number of levels fused was 4.3 (SD 2.3, range 3–15). L5/S1 level was fused in 50% of cases; posterior spinal fusions (PSF) without interbody device was performed in 8% of cases, transforaminal lumbar interbody fusion/posterior lumbar interbody fusion in 40%, and lateral anterior lumbar interbody fusion in 2% of cases. One patient (4%) underwent L4/5 transforaminal lumbar interbody fusion after no safe docking spot for the discectomy could be found during the lateral stage of the surgery. Regarding the L5/S1 levels, the following interventions have been performed in the whole cohort: not fused in 50%, PSF in 8%, transforaminal lumbar interbody fusion/posterior lumbar interbody fusion in 40%, and lateral ALIF in 2%. An illustrative patient example is given in Figure 1.
Patient demographics and overview of surgical details (N = 49).

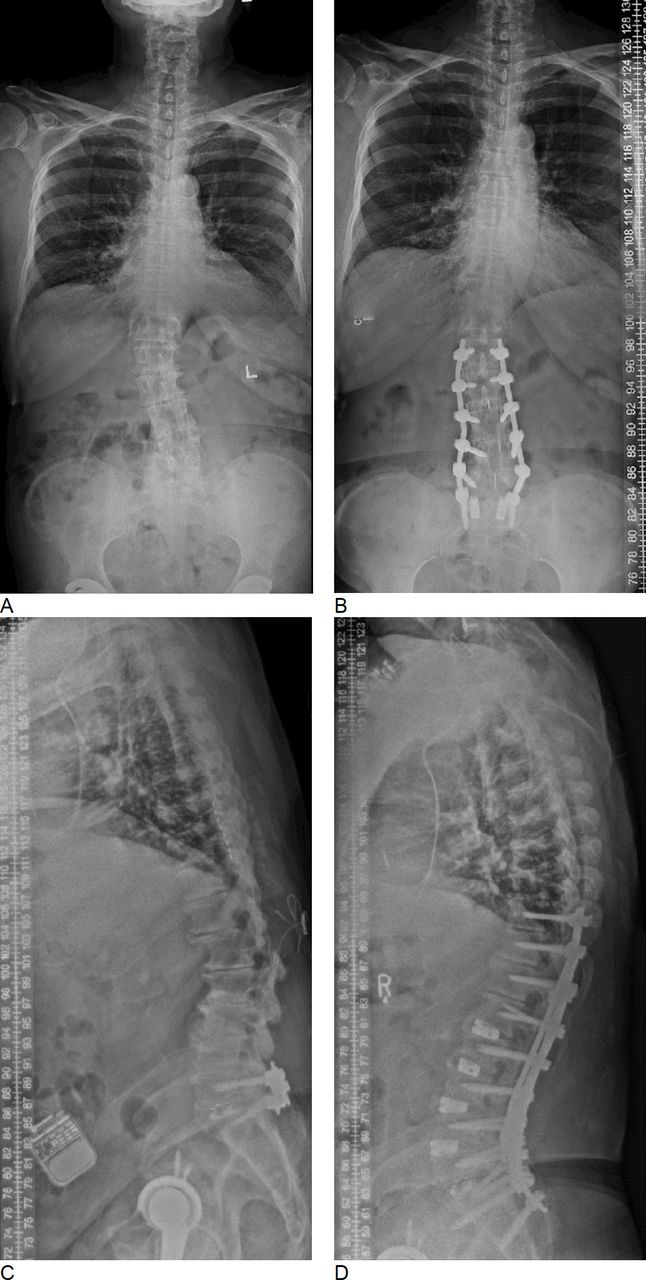
(A and B) Pre- and postoperative whole spine x-ray images. The correction of coronal deformity can be appreciated. (C and D) Pre- and postoperative whole spine x-ray images in a patient with marked correction of sagittal alignment.
Radiographic Analysis
Mean radiographic measurements were as follows: C7SVA +79.6 mm preop, +60 mm postop (∆ −33.6 mm); TK 36.1° preop, 43.8° postop (∆ +4.2°); LL 32.9° preop, 41.6° postop (∆ +9.3°), T10-L2 sagittal Cobb angle 3° preop, 2.3°postop (∆ −1°); PI 49°; PT 21.1° preop, 21.8° postop (∆ +0.1°); degenerative scoliosis was left convex in 63% of cases with the apex at L2 in 25% of cases; coronal Cobb 16.3° preop, 10.8° postop (∆ −4.8°). Postoperative mean change of C7SVA was −33.6 mm, of TK -4.2°, of LL +9.3°, of T10-L2 sagittal Cobb angle −0.7°, of PT −0.7°, see Table 2.
Radiographic measurements on whole spine standing x-rays before and after surgery.
Table 3 outlines radiographic measurement before and after surgery for each anatomic level from L1/2 to L4/5.
Radiographic measurements before and after surgery for each anatomic level.
Statistical Analysis
One linear regression analysis investigated possible impact factors on postoperative change of segmental sagittal Cobb angle. Statistically significant correlations between preoperative segmental sagittal Cobb angle (−0.54, P = 0.01) as well as preoperative coronal Cobb (0.18, P = 0.023) were found, as shown in Table 4. There was in addition a statistical trend toward significance for the variable: anatomic level (0.18, P = 0.063). The other factors investigated, namely preoperative disc space height, preoperative disc space osteophyte grade, and preoperative facet joint degeneration did not show a significant correlation with the amount of perioperative change in segmental sagittal Cobb angle. Two further linear regression models investigated the possible impact of baseline radiographic measurements on the postoperative change in foraminal width and height. Preoperative foramen height was shown to be inversely correlated with postoperative change in foraminal height (−0.25, P = 0.008, Table 5). The same finding was made for foraminal width, as shown in Table 6. No other factor investigated showed statistically significant correlations (preoperative disc space height, preoperative osteophyte grade, preoperative facet joint degeneration grade, anatomic level, implant position, and preoperative foraminal width/height).
Correlation between baseline radiographic measurements and perioperative change in segmental sagittal Cobb angle.
Correlation between baseline radiographic measurements and perioperative change in neuroforaminal height.
Correlation between baseline radiographic measurements and perioperative change in neuroforaminal width.
Discussion
In this cohort of 49 patients, correction of segmental sagittal Cobb angle was greater in segments with greater preoperative segmental coronal Cobb angle and higher loss of segmental lordosis. There was a trend toward significant correlation between sagittal correction and anatomic level, in the sense that correction of segmental sagittal Cobb angle was greater in the more caudal motion segments. No other preoperative radiographic finding had a significant impact on change of segmental sagittal Cobb angle, including degree of disc space and facet joint ankylosis. Postoperative increase of foraminal height and width was only (inversely) correlated to preoperative foraminal dimensions.
Adult spinal deformity is a major burden to health systems with an estimated prevalence of 68% among elderly populations.6 A strong correlation has been well established between C7SVA deviation, the primary surrogate marker for global thoracolumbar misalignment, and disability.7–9 In degenerative deformity, the driving force for pathologic C7SVA deviation is loss of LL, which is caused by multifocal disc and facet degeneration.10,11 In later stages, loss of coronal alignment, laterolisthesis, and anterolisthesis further contribute to the deformity in the coronal and sagittal plane. Loss of coronal alignment, another hallmark of degenerative deformities, not only causes spinal and foraminal stenosis but also attributes to further loss of global LL.9 A primary goal of deformity surgery in this setting is the restoration of LL, which improves C7SVA alignment in the sagittal and coronal plane.7,12 However, surgeons have historically not been able to predict the adequacy of postoperative correction before surgery, in as many as one-third of cases,13 which might lead to under- or overcorrection. Preoperative measures predictive of the postoperative radiographic outcome in the case of mini-open lateral deformity surgery will be useful in preventing under- and overcorrection of the deformity. In a subset of patients with adult spinal deformity less invasive, mini-open lateral surgery is a valid treatment option. The MISDEF2 algorithm has been used to select patients with ASD suitable for MIS correction technique, highlighting an sagittal vertical axis of less than 6 cm, or if more than that with flexible curves, as well as a LL-PI mismatch of no more than 30°, and TK no more than 60°.14 In this study, the postoperative increase in segmental lordosis ranged from 1.6° to 4°, which is consistent with the findings of a recent meta-analysis of 13,260 patients with an average segmental correction of 2° to 3°.15 We found that the change of segmental sagittal lordotic angle was highest in the L1/2 segment (4°) followed by a decrease in the L4/5 segment (1.6°). The degree of absolute postoperative segmental lordosis was unsurprisingly higher in the lower lumbar segments.
The degree of LL, TK, and cervical lordosis is determined by the pelvic morphology,16,17 while normal sagittal alignment of the lumbar spine is also influenced by other factors, as been described by Roussouly et al.18 The group introduced 4 different sagittal alignment types of the lumbar spine. These 4 groups differ by the absolute amount of whole lumbar alignment, location of the sagittal lordotic apex as well as sagittal curvature proximal, and distal to the lumbar apex. In a recent study on 210 asymptomatic individuals of all age groups,19 it was shown that a mismatch between LL and PI increases during aging from +9° at age 20 to 30 years to −13.5° at age 80 to 90 years. For asymptomatic individuals, for example, TK will be roughly 75% of LL.20 It has been shown, however, that TK increases across the lifespan from 24° to 35°, contributing to an increase in T1 slope angle from 23° to 36°.19 Because of these age-related changes, the normative value of C7SVA increases from 1.7 mm at age 20 to 30 years to 52.5 mm at age 80 to 90 years.
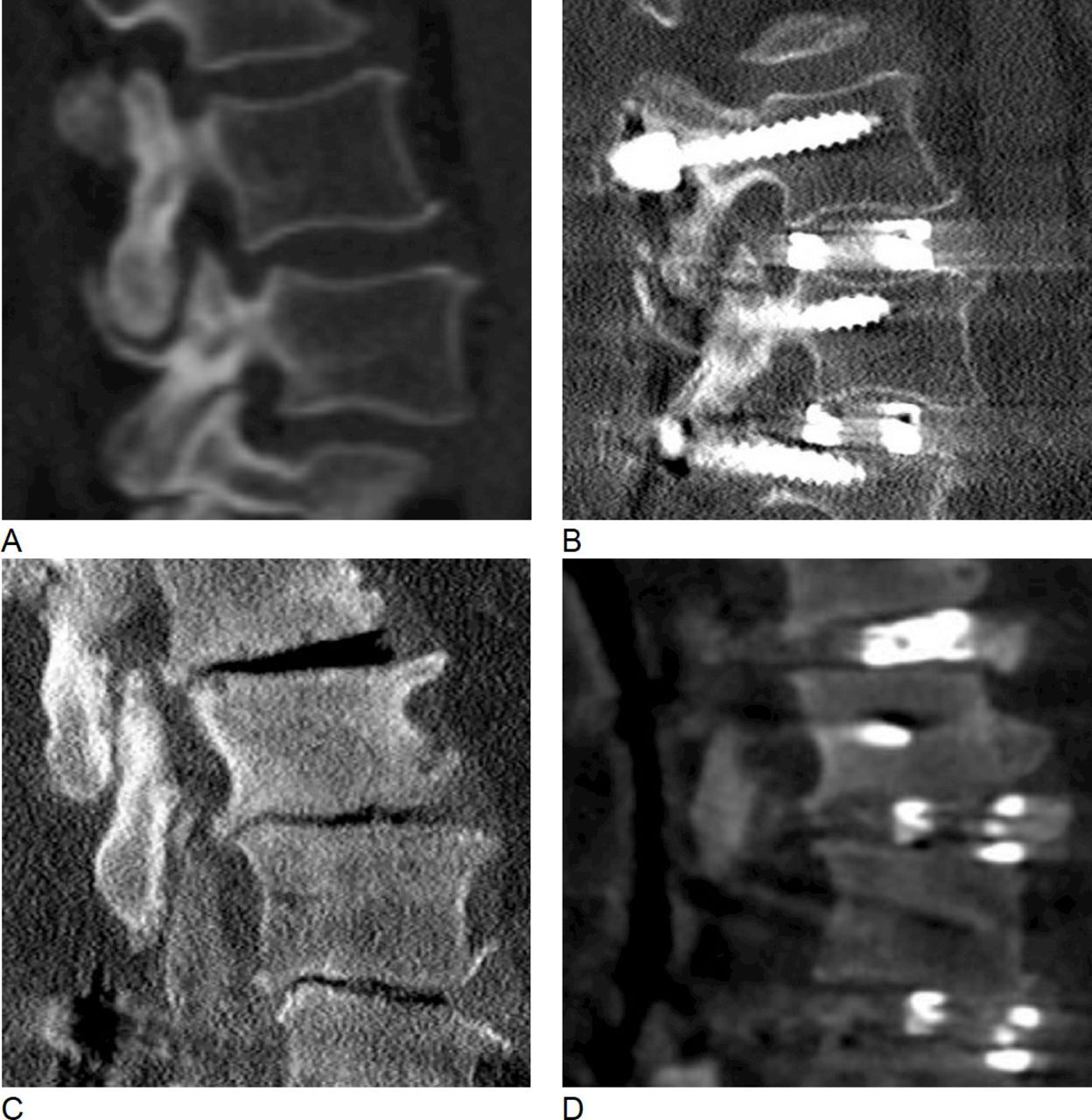
Notably neither disc space spanning osteophytes nor ankylosed faced joints had a negative impact on the correction of sagittal segmental alignment. The trend for a positive correlation between segmental sagittal correction and anatomic level is explained by the fact that segmental lordosis physiologically increases from L1/2 to L4/5. Interestingly, there was also a significant positive correlation between preoperative segmental coronal Cobb angle and postoperative segmental sagittal Cobb angle indicating that coronal deformity negatively impacts sagittal alignment. The lack of significant correlation between preoperative disc space height and sagittal correction shows that even with maintained disc space height correction can be obtained. Figure 2a/b shows an example of high preoperative segmental sagittal Cobb angle with consequently lack of significant increase postoperatively, while Figure 2c/d shows the opposite. As shown in this figure, increase in segmental lordosis is not influenced by disc space height; however, there is an inverse correlation between preoperative segmental lordosis and postoperative increase in segmental lordosis. The fact that disc space osteophytes did not influence the amount of sagittal correction is explained by the fact that in most cases the lateral osteophytes are directly resected upon approach to the disc space. Even severely degenerated facet joint with bridging osteophytes did not interfere with the ability to restore segmental lordosis. This study further shows that the more distal the anatomic level treated is located, the more lordosis is restored postoperatively. Even though this finding only showed a trend toward significance, it is plausible given the fact that lordosis steadily increases from L1/2 to L5/S1.

Restoration of segmental sagittal profile. (A and B) Pre- and postoperative sagittal computed tomography (CT) images of the L3/4 disc space. Preoperatively, there was little loss of disc space height. The perioperative change of segmental sagittal Cobb angle was +3°. (C and D) Pre- and postoperative sagittal CT images of the L3/4 disc space in a patient with marked loss of disc space height. In this case, the perioperative gain in segmental lordosis was 5°.
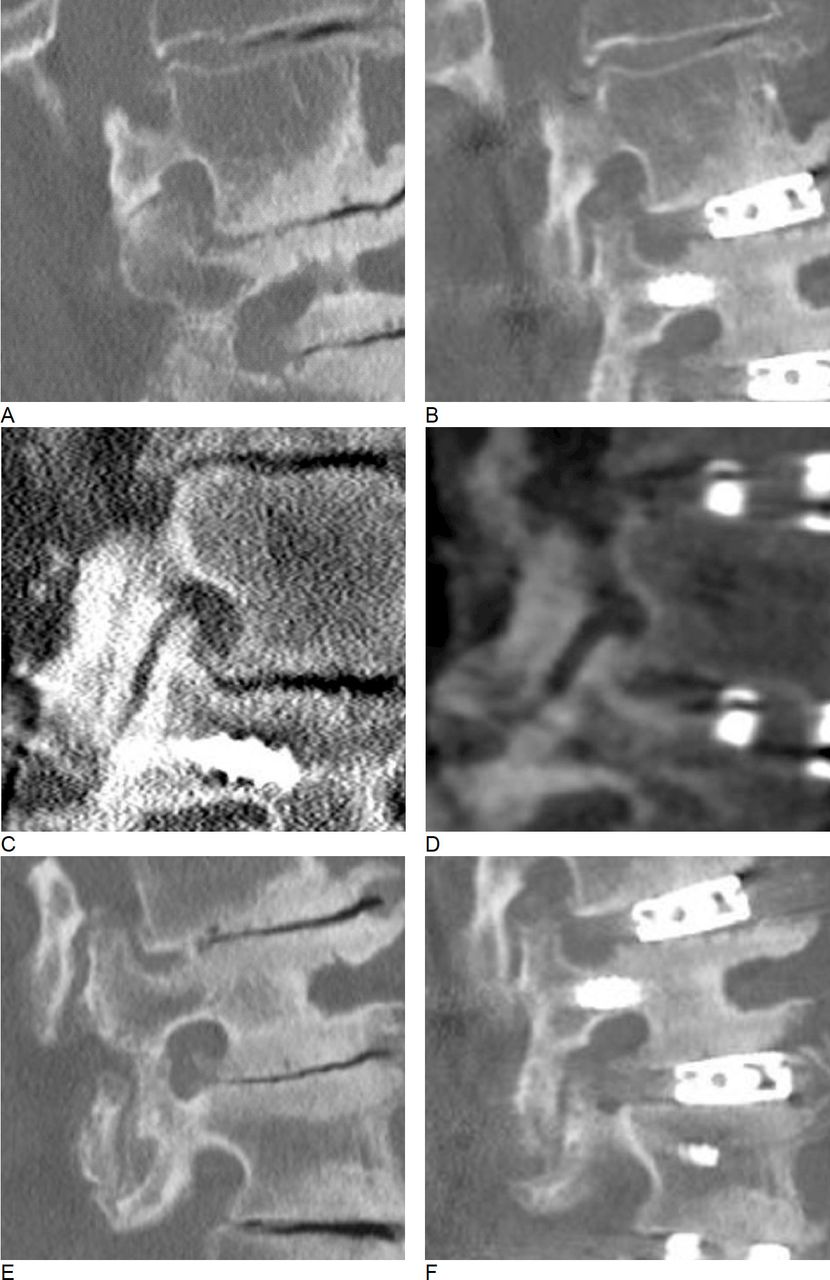
Lateral approaches with interbody fusion in ASD surgery have been shown to indirectly reduce compression of the neuroforamen through restoration of disc height, stretching of the facet joint capsules and ligamentum flavum as well as reducing subluxations of the facet joints.21 In the present study, we find that postoperative neuroforaminal height and width for ASD surgery could not be predicted by preoperative radiographic measures, including disc height, orthogonal neuroforamen measure, preoperative coronal Cobb angle, implant position, osteophyte, or degeneration grade. Indirect decompression of the neuroforamen was achieved through expansion of disc height with the superior articulating process being displaced caudally and laterally, yet not in a predictable manner (Figure 3). While low grade osteophytes are known to prevent sufficient decompression of the neuroforamen and nerve root, osteophyte and autofused facet segments did not influence the degree of correction in our study.

Foraminal decompression. (A and B) Pre- and postoperative sagittal views of the L2/3 neuroforamen. The superior articulating process causes significant foraminal stenosis preoperatively. Postoperatively, the SAP is displaced caudally, which leads to foraminal decompression. (C and D) Similarly, Pre- and postoperative views of a left-sided L4/5 foramen. Again, postoperative displacement of the SAP decompresses the neuroforamen. (E and F) Failure of indirect decompression. Even though the craniocaudal dimension of the neuroforamen significantly increases postoperatively, an osteophyte causes persistent nerve root compression.
The main limitation of this study lies in the rather small sample size. Further longer clinical and radiographic follow-up would add relevant insight into mechanisms implied in maintenance of the immediate postoperative radiographic outcome. Furthermore, measurements on radiological images are always dependent on the investigator and may underlay a variability if repetitively performed. We tried to minimize intra- and interobserver variability by measuring all images through a single investigator who measured all values at least twice. Lastly, the presented series comprises patients operated by several surgeons. Intraoperative decisions as, that is, at which extend to stop a decompression or the amount of correction of the sagittal balance are to some extend subjective and may vary between surgeons. This should be taken into account when extrapolating these data to other series.
Conclusion
Preoperative sagittal and coronal Cobb angles were inversely correlated with postoperative degree of sagittal alignment restoration; Bridging osteophytes, ankylosed facet joints, disc space height, and position of the interbody device did not affect radiographic outcome. Indirect neuroforaminal decompression could not be reliably predicted based on preoperative imaging findings.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.