


Article Figures & Data
Figures
- Figure 1
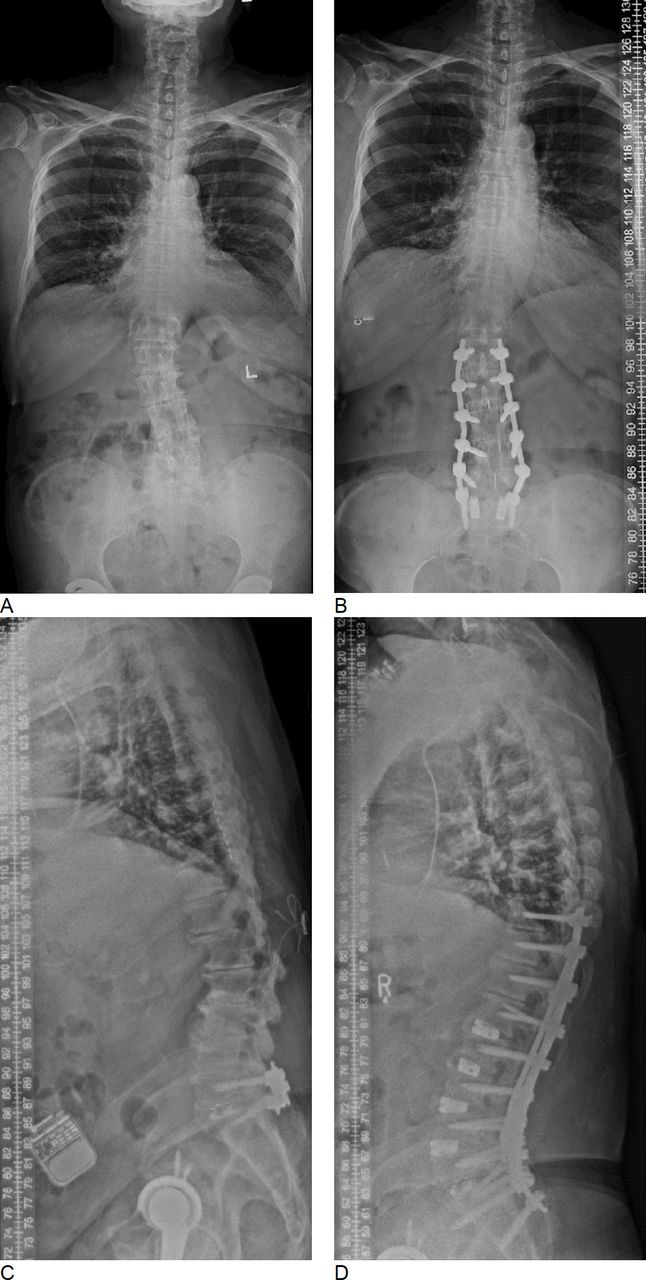
(A and B) Pre- and postoperative whole spine x-ray images. The correction of coronal deformity can be appreciated. (C and D) Pre- and postoperative whole spine x-ray images in a patient with marked correction of sagittal alignment.
- Figure 2
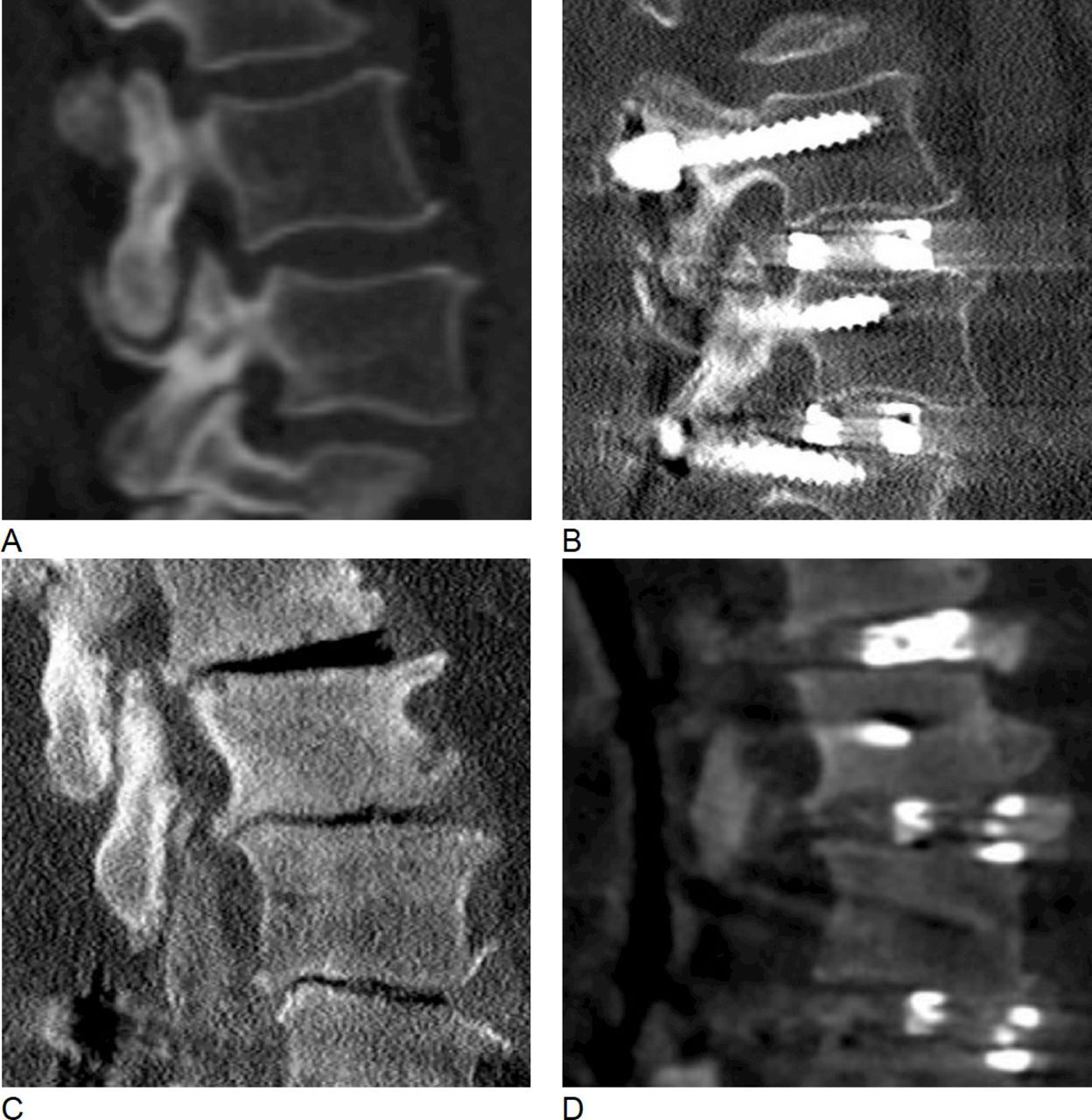
Restoration of segmental sagittal profile. (A and B) Pre- and postoperative sagittal computed tomography (CT) images of the L3/4 disc space. Preoperatively, there was little loss of disc space height. The perioperative change of segmental sagittal Cobb angle was +3°. (C and D) Pre- and postoperative sagittal CT images of the L3/4 disc space in a patient with marked loss of disc space height. In this case, the perioperative gain in segmental lordosis was 5°.
- Figure 3
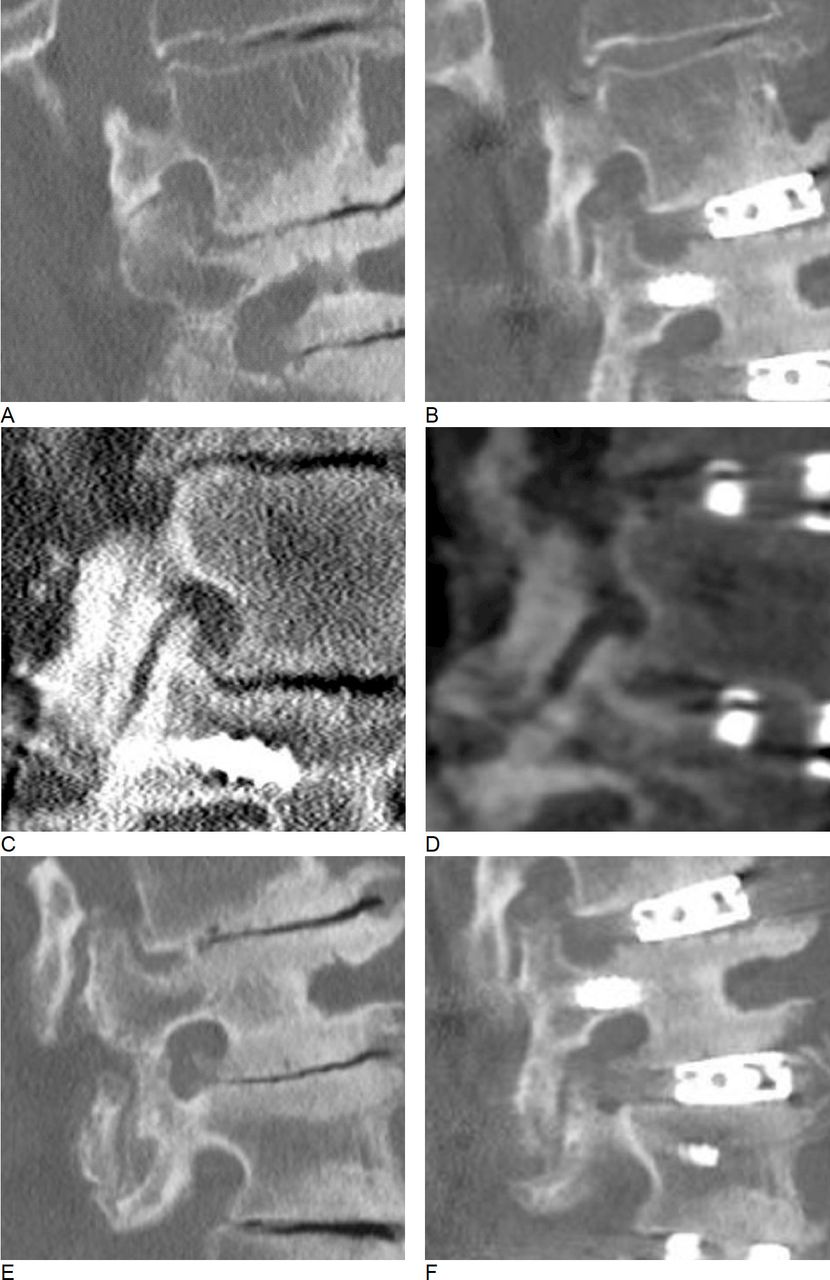
Foraminal decompression. (A and B) Pre- and postoperative sagittal views of the L2/3 neuroforamen. The superior articulating process causes significant foraminal stenosis preoperatively. Postoperatively, the SAP is displaced caudally, which leads to foraminal decompression. (C and D) Similarly, Pre- and postoperative views of a left-sided L4/5 foramen. Again, postoperative displacement of the SAP decompresses the neuroforamen. (E and F) Failure of indirect decompression. Even though the craniocaudal dimension of the neuroforamen significantly increases postoperatively, an osteophyte causes persistent nerve root compression.



Tables
Demographic Data Age, y, mean (SD) (range) 68.7 (8.6) (39.9–84.7) Sex, female/male 63%/37% Fusion construct Distribution of upper instrumented vertebra T4 2% T10 6% T11 2% T12 2% L1 17% L2 60% L3 10% Distribution of lower instrumented vertebra L5a 60% S1 35% Pelvis 15% No. of levels fused, mean (SD) (range) 4.3 (2.3) (3–15) Operative complications Seromab 4% Wound dehiscence 4% Transient dysesthesia 18% Transient hip flexor weakness 6% - Table 2
Radiographic measurements on whole spine standing x-rays before and after surgery.
Measurement Mean (SD) (Range) P value C7SVA, mm 0.1 Preoperative 79.6 (63) (−43−254) Postoperative 60 (51.8) (−26–217) ∆C7SVA −33.6 (57.9) (−166–60) TK, ° 0.01 Preoperative 36.1 (15.4) (5–77) Postoperative 43.8 (15) (21−91) ∆ 4.2 (15.3) (−35–39) LL, ° 0.003 Preoperative 32.9 (15.9) (−14–78) Postoperative 41.6 (12.4) (24–84) ∆ 9.3 (10.5) (−4–46) T10-L2 sag Cobb, ° 0.8 Preoperative 3 (12.7) (−24–30) Postoperative 2.3 (11.2) (−30–32) ∆ −1 (9.4) (-21–32) PI, ° 49 (10.7) (21–77) PT, ° 0.7 Preoperative 21.1 (9.6) (−4–54) Postoperative 21.8 (7.3) (2–34) ∆ 0.1 (10) (−28−26) Degenerative scoliosis Left convex 63% Scoliotic apex level L1 1% L2 25% L2/3 4% L3/4 6% L4 6% Coronal Cobb, ° 0.02 Preoperative 16.3 (12) (0−48) Postoperative 10.8 (10.3) (0–45) ∆ −4.8 (8.4) (−24–30) C7PL, mm 0.6 Preoperative 14.1 (15.1) (0–54) Postoperative 12.9 (9.1) (0–28) ∆ −3.7 (15.3) (−45–26) C7PL, C7 plumb line (coronal); C7SVA, C7 sagittal vertical axis; LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt; TK, thoracic kyphosis.
Mean (SD) (Range) Measurement L1/2 L2/3 L3/4 L4/5 Sagittal Cobb, ° Preoperative −1.8 (5.6) (−11–13) 2.5 (4) (−6-16) 5.6 (4.9) (−5–21) 9.5 (5.7) (1–21) Postoperative 2.2 (4.9) (−5–17) 5.2 (3.8) (0–18) 7.3 (4.4) (0–14) 11 (4.8) (3–24) ∆ 4 (3.2) (0–11) 2.7 (3.4) (−5–10) 1.8 (4.2) (−10–14) 1.6 (4.6) (−7–17) Coronal Cobb, ° Preoperative 5.5 (5.1) (0–16) 7.4 (5.8) (0–26) 5.8 (5.6) (0–23) 4.2 (3.8) (0–15) Postoperative 4.2 (3.5) (0–11) 3.4 (3.8) (0–17) 3.3 (4) (0−20) 2.7 (2.2) (0–9) ∆ −1.3 (6) (−14−11) −4 (4.6) (−14–6) −2.4 (5.5) (−22–18) 4.4 (2.5) (−1–11) Foraminal height, mm Preoperative 15.2 (3.8) (11–23) 16.5 (4) (8−26) 15.7 (3.8) (8–24) 15.5 (3.6) (6–24) Postoperative 18 (5.1) (11–30) 19.6 (4.4) (9–37) 19.3 (4) (8-32) 18.6 (3.5) (9–25) ∆ 2.8 (2.6) (−1–7) 3.1 (3.2) (−2–16) 3.6 (3.5) (−3–14) 2.7 (4.7) (−16–13) Foraminal width, mm Preoperative 7.1 (2) (3-10) 8 (2) (5−13) 8.3 (1.6) (5–12) 8.5 (1.9) (5–14) Postoperative 9.5 (3) (6−15) 9.4 (2.1) (5–14) 9.8 (1.9) (7–14) 9.8 (1.9) (6–13) ∆ 2.4 (2.7) (−1–7) 1.4 (2.2) (−2–8) 1.4 (2.4) (−5–7) 1 (2.5) (−6–7) Disc space height, mm Preoperative 4 (3) (1−11) 5 (2.6) (1–11) 5.8 (2.9) (1–12) 6.5 (3) (2−13) Postoperative 9.2 (2.2) (7–16) 9.8 (2) (7−15) 10.6 (1.5) (8–14) 10.9 (1.7) (8–16) ∆ 5.2 (2.3) (−1–9) 4.8 (2.5) (−1–10) 4.7 (2.9) (0–11) 4.4 (2.5) (−1–11) - Table 4
Correlation between baseline radiographic measurements and perioperative change in segmental sagittal Cobb angle.
Measurement Unstandardized Coefficients Standardized Coefficient P Value B Standard Error Beta t Preoperative segmental sagittal Cobb angle, ° −0.4 0.1 −0.5 −5.7 0.01 Preoperative disc space height, mm −0.2 0.1 −0.2 −1.7 0.09 Preoperative osteophytes gradea −0.3 0.6 −0.05 −0.5 0.59 Preoperative facet joint degeneration gradeb −0.1 0.3 −0.02 −0.2 0.81 Anatomic level 0.8 0.4 0.2 1.9 0.06 Preoperative coronal Cobb angle, ° 0.1 0.1 0.2 2.3 0.02 - Table 5
Correlation between baseline radiographic measurements and perioperative change in neuroforaminal height.
Unstandardized Coefficients Standardized Coefficient Significance B Standard Error Beta t Preoperative disc space height, mm −0.1 .01 −0.04 −0.4 0.71 Preoperative osteophytes gradea 0.7 0.6 0.1 1.3 0.18 Preoperative foraminal height, mm −0.3 0.1 −0.3 −2.7 0.01 Preoperative foraminal width, mm 0.2 0.2 0.1 0.9 0.36 Preoperative facet joint degeneration gradeb −0.1 0.3 −0.02 −0.2 0.81 Preoperative coronal Cobb angle, ° 0.02 0.1 0.03 0.3 0.74 Implant positionc −0.3 0.6 -0.04 −0.5 0.65 Anatomic level 0.2 0.4 0.04 0.4 0.68 ↵a Three grades: I, nonbridging disc space osteophytes; II, small bridging disc space osteophytes; III, ankylosed disc space.
↵b Three grades: I, nonbridging osteophytes of the facet joint; II, small bridging osteophytes of the facet joint; III, ankylosed facet joint.
↵c Location of the center of the interbody device in relation to 4 quadrants, which the disc space has been divided into on sagittal imaging (I anterior to IV posterior).
- Table 6
Correlation between baseline radiographic measurements and perioperative change in neuroforaminal width.
Unstandardized Coefficients Standardized Coefficient Significance B Standard Error Beta t Preoperative disc space height, mm −0.02 0.1 −0.02 −0.2 0.82 Preoperative osteophytes gradea −0.6 0.3 −0.2 −1.8 0.08 Preoperative foraminal width, mm −0.7 0.1 −0.5 −6.8 0.01 Preoperative facet joint degenerationb 0.4 0.2 0.2 1.8 0.08 Preoperative coronal Cobb angle, ° −0.01 0.03 −0.03 −0.4 0.73 Implant positionc −0.3 0.4 −0.1 −0.9 0.37 Anatomic level −0.3 0.2 −0.1 −1.1 0.26 a Three grades: I, nonbridging disc space osteophytes; II, small bridging disc space osteophytes; III, ankylosed disc space.
↵b Three grades: I, nonbridging osteophytes of the facet joint; II, small bridging osteophytes of the facet joint; III, ankylosed facet joint.
↵c Location of the center of the interbody device in relation to 4 quadrants, which the disc space has been divided into on sagittal imaging (I anterior to IV posterior).
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.