


Abstract
Background Minimally invasive transforaminal interbody fusion (MIS-TLIF) is an effective procedure for lumbar spine diseases. The procedure can be done using a surgical microscope (SM) or surgical loupes (SL) magnification. However, there are no studies that compared outcomes between using these 2 magnifying devices in the MIS-TLIF procedure. The purpose of this study was to compare clinical outcomes, perioperative complications, and radiographic parameters of MIS-TLIF using SM compared with SL magnification.
Methods We included all patients undergoing 1-level MIS-TLIF between January 2017 and December 2019. Type of magnification (SM vs SL), operative time, blood loss, perioperative complications, cross-sectional area of the spinal canal, and fusion rates were analyzed. Clinical outcomes measurement using the visual analog scale (VAS) and Oswestry Disability Index (ODI) were compared between groups.
Results A total of 100 patients had underwent MIS-TLIF (SM group: 62; SL group: 38). Operative time (SM: 182.7 ± 41.5 vs SL: 165.6 ± 32.6 minutes, P = 0.043) was significantly shorter in the SL group, with a mean difference of 17.2 minutes and a 10.4% increase in operative time between SL and SM. Blood loss (SM: 187.4 ± 176.4 vs SL: 215.6 ± 99.4 mL, P = 0.36) was not different between groups, with a mean difference of 28.2 mL. Both the SM group and SL group demonstrated no significant differences in improvement from baseline in VAS back, VAS legs, ODI score, and cross-sectional area of the spinal canal. There was also no significant difference in complication rates and fusion rates between groups.
Conclusions Our study found no difference between intraoperative use of SL compared with SM in clinical outcomes through the 12-month follow-up timepoint. However, the use of SM resulted in an increased average operative time of 17 minutes compared with the SL group.
Clinical Relevance Intraoperative use of SM and SL magnification in MIS-TLIF provides similar outcomes except prolonged operative time in the SM group.
Level of Evidence 3.
Introduction
Minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) has been reported to result in less trauma to soft tissue and back muscles, decreased blood loss and length of hospital stay, as well as improved functional outcomes compared with an open TLIF procedure.1–6 Visualization is an important factor for success in any surgical procedure and becomes even more critical when operating through a reduced surgical field such as with MIS-TLIF. Some surgeons use the surgical microscope (SM) for magnification and lighting. Some studies reported that surgical site infection rates in patients who underwent lumbar microdiscectomy were not different between the groups that used SM or surgical loupes (SL).7,8 Basques et al found that operative time was slightly increased with using SM during spine surgeries.9 However, this study was a database review that included a heterogenous cervical and lumbar surgeries sample. SL magnification is also used by some surgeons for performing MIS-TLIF with favorable outcomes.4 Nevertheless, some surgeons purport that the use of the intraoperative microscope may allow for a more extensive decompression and potentially improved clinical outcomes and fewer intraoperative complications when performing MIS-TLIF. We hypothesized that there would be no difference in clinical outcomes or complications when comparing MIS-TLIF cases using SM vs SL. Therefore, the purpose of our study was to compare clinical outcomes, complication rates, and radiographic parameters of MIS-TLIF performed by using SM vs SL magnification.
Methods
We performed a retrospective study evaluating the spine registry data at a single institution by a single surgeon (W.S.). We included patients who had undergone 1-level MIS-TLIF for degenerative lumbar spine diseases with SM or SL between January 2017 and July 2019. The first 38 patients underwent MIS-TLIF using SL, and the subsequent 62 patients underwent the procedure with SM because the hospital acquired a new microscope in the middle of the study period. Patients were excluded if completed patient-reported outcomes were not collected (at baseline and at 1-day, 1-month, 3-month, 6-month, and 12-month postoperative periods). Patients with spinal infection, tumor, or prior spinal surgery were also excluded.
Data Collection
Baseline data included patient demographics, symptoms, diagnosis, past medical history, patient comorbidities, and preoperative spinal canal cross-sectional area. Perioperative data included estimated blood loss, operative time (from incision to wound closure), and perioperative complications.
Patient-reported outcomes included measurement of Oswestry Disability Index (ODI) and visual analog scale (VAS) score for back pain and leg pain, and both outcome measures were evaluated at preoperative, immediate postoperative (1 day), 1 month, 3 months, 6 months, and 1 year after surgery.
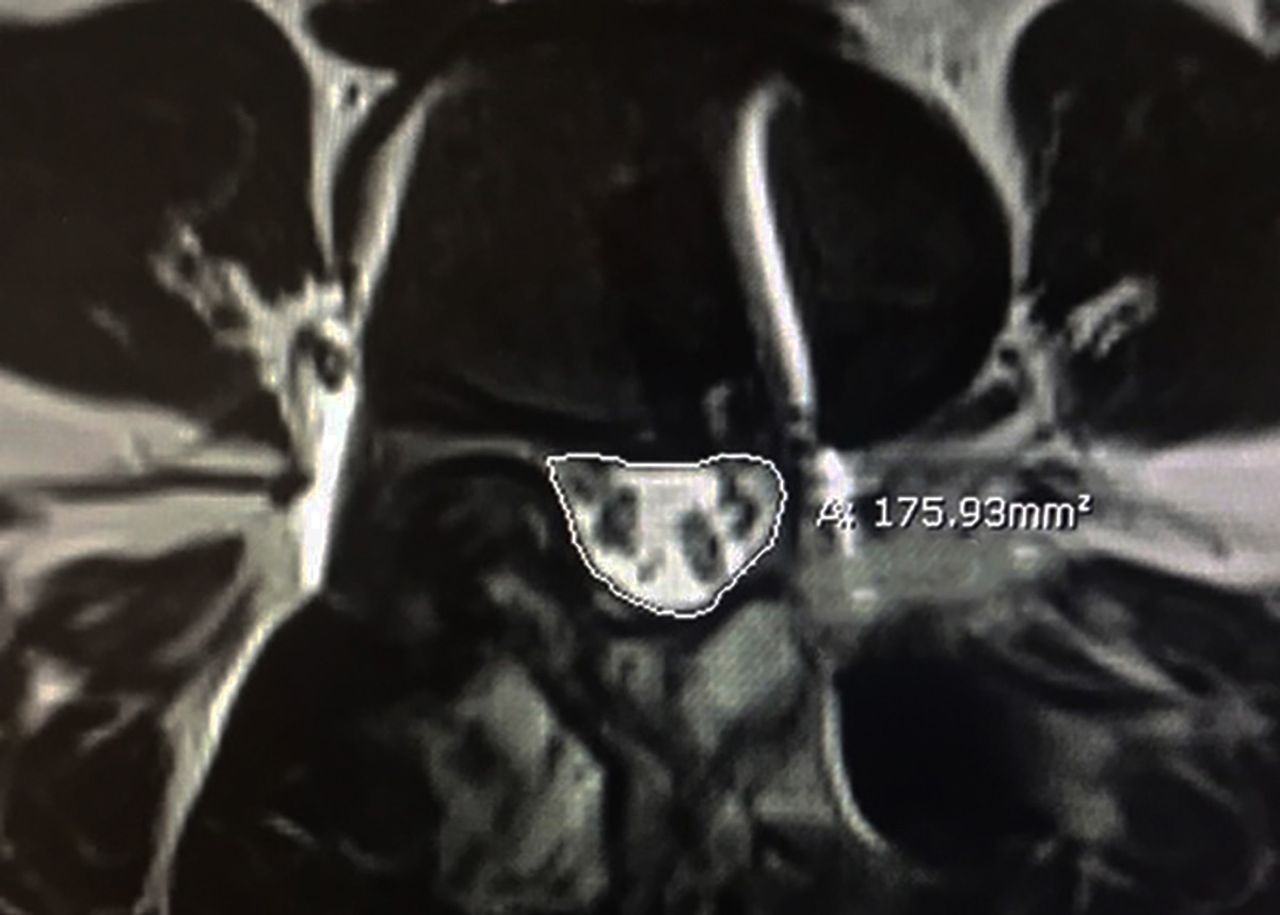
We used picture archiving and communication system program to evaluate the cross-sectional area of the spinal canal on axial view T2-weighed magnetic resonance images at the facet joint level (Figure 1). The area was measured on the preoperative and 3-month postoperative images. The spinal fusion was evaluated by computed tomography images and flexion-extension radiographs 12 months after the operation. Fusion was defined by less than 3-mm translation and 5° angular motion on the flexion-extension radiographs as well as complete bone bridging between the end plates on the computed tomography image.2,10,11

Spinal canal cross-sectional area was measured by drawing the line surrounding spinal canal using digital synapse picture archiving and communication system.
Statistical Analyses
Statistical analyses included descriptive statistics and univariate analysis using Student t test. Statistical significance was defined as P < 0.05. All analyses were performed using SPSS.
Surgical Techniques
The MIS-TLIF procedure was performed with the patient placed in the prone position. Fluoroscopy was then used to identify the starting incision between pedicles of the operative levels. A 2.5-cm skin incision was then made over the interpedicle line and approached through the underlying paraspinal fascia and muscles. A Jamshidi needle was advanced into each pedicle bilaterally using biplanar fluoroscopic guidance. Kirschner guide wires were then placed through the Jamshidi needle, and then the needle was removed over the wire. The Kirschner wires were then bent in cephalad and caudad directions away from the incision site. Sequential dilation was then performed, followed by tubular retractor placement. At this point, the surgeon used either the SM (Carl Zeiss OPMI-Vario700) or the Aculux xenon headlight with 2.5 power SL for magnification and visualization. Hemilaminectomy and facetectomy were performed using high-speed burr and Kerrison rongeur. The ligamentum flavum was removed to identify the thecal sac and nerve root. In the patient with bilateral symptoms, we also decompressed the contralateral side using the “over the top technique.” Discectomy was performed, followed by meticulous end plate preparation. The trial was inserted and sized. Autologous local bone graft plus demineralized bone matrix was used to enhance fusion. Bone graft plus demineralized bone matrix was placed in the anterior portion of disc space, followed by the intervertebral polyetheretherketone cage (CAPSTONE, Medtronic). Percutaneous screws and rods (CD HORIZON SEXTANT II, Medtronic) were then placed on both sides. A drain was placed only on the TLIF side, and the incision was then closed layer by layer.4,12
Results
A total of 100 MIS-TLIF (SM group: 62; SL group: 38) were included in this study. The mean follow-up time was 20.4 months in the SM group and 24.3 months in the SL group. There was no difference between groups in age, body mass index, smoking status, or comorbidities (hypertension, diabetes, and dyslipidemia). Spondylolisthesis was the most common diagnosis in both groups, followed by spinal canal stenosis and degenerative disc disease (Table 1).
Demographic data.
Baseline Patient-Reported Outcome Measures
At baseline, there was no difference in baseline VAS back pain, VAS leg pain, and ODI score. Similarly, we found no difference in mean spinal canal cross-sectional area between groups (SM: 73.5 ± 35.4 vs SL: 68.1 ± 33.9 mm2, P = 0.433).
Intraoperative Outcome Measures
The duration of surgery was significantly different between groups, with the SL group having a shorter mean operative time (SM: 182.7 ± 41.5 vs SL: 165.6 ± 32.6 minutes, P = 0.043). Mean blood loss was not significantly different between groups (SM: 215.6 ± 99.4 vs SL: 187.4 ± 176.4 mL, P = 0.36). There were also no significant differences in operative time between the first 30 and the last 30 cases of the SM group (P = 0.406).
Postoperative Patient-Reported Outcome Measures
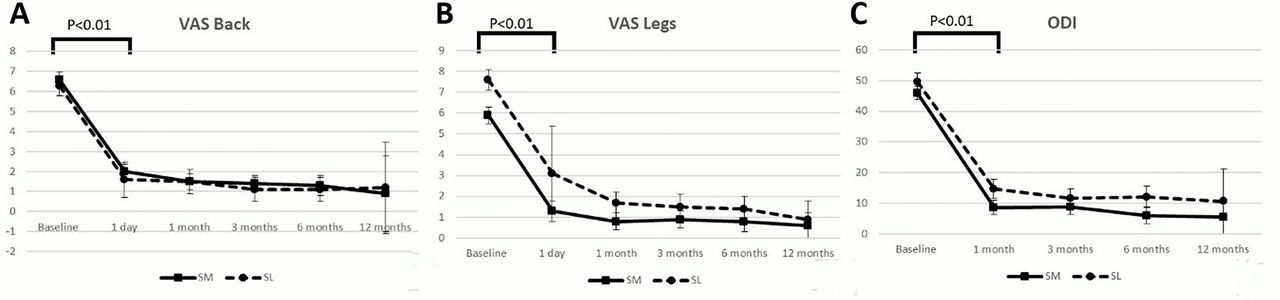
VAS back and leg pain were significantly improved in both groups from baseline to immediate postoperative (P < 0.01). These improvements were sustained through the 12-month follow-up. There was no significant difference in VAS back pain or VAS leg pain between these groups at any follow-up timepoint (Table 2 and Figure 2A and B).
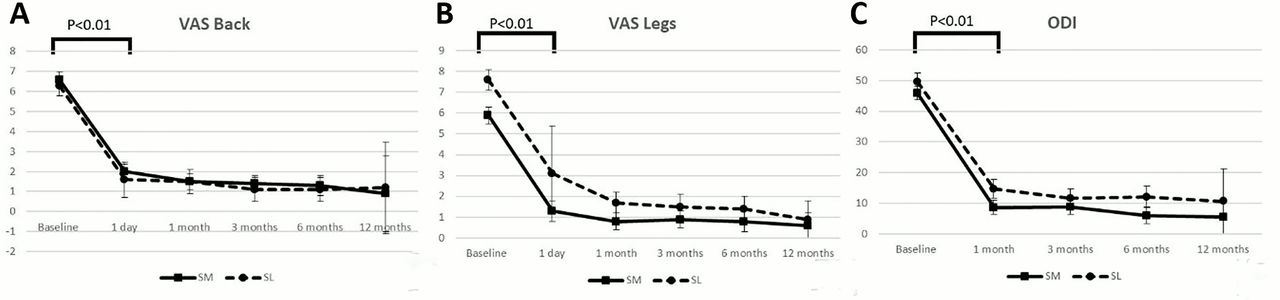
Patient-reported outcome in (A) visual analog scale (VAS) back, (B) VAS legs, and (C) Oswestry Disability Index (ODI).
Patient-reported outcome in back pain (VAS back) and leg pain (VAS legs).
ODI score was also significantly improved in both groups from baseline to immediate postoperative (P < 0.01 in both groups). There was no difference in ODI score between both groups at any follow-up timepoint (Table 3 and Figure 2C).
Patient-reported outcome in back pain (ODI).
There was a significant improvement from baseline to postoperative spinal canal cross-sectional area in both groups. In the SM group, the mean cross-sectional area increased from 73.5 to 161.9 mm2 (120% improvement). In the SL group, the mean cross-sectional area increased from 68.1 to 174.4 mm2 (156% improvement). There was no difference in mean postoperative spinal canal cross-sectional area between these groups (SM: 161.9 ± 45.3 vs SL: 174.4 ± 16.9, P = 0.348).
There was no significant difference in fusion rates at 12 months postoperative between the SM group (91.84%) and the SL group (83.33%) (P = 0.397).
The rate of postoperative complications was not different between these groups. There was no incidental durotomy or infection in both groups. Two patients in the SM group and a single patient in the SL group experienced new postoperative lower extremity sensory changes, and all patients recovered in a month after the operation.
Discussion
The MIS-TLIF procedure has been shown to be a better treatment option compared with traditional open procedures in terms of recovery time and blood loss,1–3 and this procedure can be performed using an SM or SL for better visualization.4 However, to our knowledge, there is no literature to date that compares outcomes between these 2 methods used for performing MIS-TLIF. The theoretical benefits of using SM are greater magnification and a direct light source. These advantages may help surgeons achieve a more extensive and thorough decompression, decreased bleeding due to better identification of bleeding points, more effective in controlling epidural bleeding, and better disc preparation and removal for arthrodesis. Nevertheless, our study did not confirm these theoretical benefits. This study showed no difference in clinical outcomes between the SM and SL groups. Furthermore, the use of SM may be associated with increased operative time.
We performed a retrospective cohort study with at least 1-year follow-up of MIS-TLIF performed with SM vs SL. Our study found no difference in clinical outcomes at 1 year postoperative as well as no difference in complication rates between groups. The duration of surgery was significantly longer in the SM group compared with the SL group, with 17 minutes (10% increase) longer on average in the SM group. The finding may be explained by the preparation period of the microscope, such as sterile draping and positioning. In addition, adjustments are made several times during the use of the SM to maintain appropriate visual fields, lighting, and magnification, whereas these adjustments are not required with the use of SL. Our findings are similar to an investigation of anterior cervical discectomy and fusion (ACDF) procedure by Adogwa et al, who analyzed 140 ACDF patients with and without using an SM. The study found no difference in outcomes except for a significant increase (P = 0.01) in operative time. The average operative time was 71 minutes (73% increase) longer with the use of SM.13 Davidson et al also reported a significant increase (P < 0.001) of average operative time (30 minutes) in thyroidectomy procedure with the use of an intraoperative microscope.14 The SM group had no difference in blood loss when compared with the SL group, which was a similar finding in the current study on MIS-TLIF.
Our study found no difference in baseline demographic parameters or patient-reported outcomes. We demonstrated significant improvement in patient-reported outcomes (VAS back, VAS leg, and ODI) from baseline to all follow-up timepoints in both groups, but no difference in these outcomes at any follow-up timepoint between these groups. The spinal canal cross-sectional area was significantly increased from baseline to the 12-month postoperative time point in each group. However, there was no difference in postoperative cross-sectional area between these groups. Finally, fusion rates were not significantly different between the SM group (91.84%) and the SL group (83.33%).
Our data suggested that both SM and SL are effective for magnification and lighting in the MIS-TLIF procedure performed through a tubular retractor. These 2 visualization methods provided similar clinical outcomes, the extent of decompression, and fusion rates. As previously noted, our results are similar to a study of ACDF procedure in 2016 by Adogwa et al, which found no difference in outcomes.13 More recently, Ehanire et al evaluated free-flap procedures with SM vs SL and also reported no statistical difference in outcomes and safety between 2 methods.15 We did not find any previous study specifically comparing the use of SM and SL when performing MIS-TLIF. The study by Basques et al included both cervical and lumbar surgeries. However, the lumbar procedures in their study contained many procedures such as laminotomy, laminectomy, anterior fusion, and posterior fusion. The multivariate analysis found that the microscopic group was associated with an increase of 13.2 minutes of average operative time when their model was controlled for demographic data, comorbidities, and operative characteristics.10
Regarding the retrospective nature, this study may potentially have selection bias. However, the baseline demographic characteristics were not different between SM and SL groups. In addition, all surgeries were performed by a single surgeon, which may reduce the variation of surgical outcomes. Due to the small sample size, multivariate analysis was not able to perform in our study. A larger sample size with a longer follow-up time may provide additional data in future studies.
Conclusions
Our study found no significant difference in clinical outcomes between intraoperative use of SL compared with SM. During 12-month follow-up period, there was no difference in patient-reported outcomes, the extent of decompression, fusion rates, and complications between groups. However, the average operative time was 17 minutes longer in the SM group, accounting for 10% loonger duration than in the SL group.
Acknowledgments
The authors thank Thanachaporn Kittipibul, MD, and Clinical Research Center, Chulalongkorn University, for their support of this study.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval The Human Investigation Committee of Faculty of Medicine, Chulalongkorn University Institutional Review Board (IRB) approved this study. The approval number is 354/61. The written informed consent was waived.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.