


Abstract
Background Despite the known association between increased estimated blood loss (EBL) and suboptimal perioperative outcomes, the exact threshold of EBL that impacts outcomes following elective spine surgery remains unknown. In a cohort of patients undergoing elective 1-level open posterior lumbar fusion, we sought to identify EBL thresholds associated with: (1) prolonged length of stay (LOS), (2) postoperative complications, and (3) patient-reported outcomes (PROs).
Methods A retrospective, single-center study was performed of patients undergoing elective, 1-level open posterior lumbar fusion with and without interbody fusion between October 2010 and April 2021. The primary exposure variable was EBL. Primary outcomes included: (1) LOS, (2) 30-day complications, and (3) 3-month PROs. Minimum clinically important difference was set at 30% improvement from baseline. For purposes of receiver-operating characteristic curves, LOS was dichotomized as 1 vs ≥2 days.
Results Of the 2028 patients undergoing posterior lumbar fusion surgery, 1183 underwent 1-level fusions, 763 (64.5%) with interbody fusion and 420 (35.5%) without. With interbody fusion: Median (interquartile range [IQR]) EBL was 350 mL (200–600), and median (IQR) LOS was 2 days (2–3). A positive linear association was found between EBL and LOS (P < 0.001) but not with PROs. EBL above 275 mL was associated with LOS beyond postoperative day 1 (POD1) (area under the curve [AUC] = 0.73, 95% CI 0.68–0.78, P < 0.001), with no significant association with overall complications or PROs. Without interbody fusion: Median EBL (IQR) was 300 mL (150–500), and median (IQR) LOS was 3 days (2–4). A positive linear association was found between EBL and LOS (P < 0.001) but not with PROs. EBL above 238 mL was associated with LOS beyond POD1 (AUC = 0.78, 95% CI 0.71–0.85, P < 0.001), with no impact on overall complications or PROs.
Conclusions In patients undergoing 1-level posterior lumbar fusion, EBL volumes greater than 275 and 238 mL in patients with and without interbody fusion, respectively, were associated with increased LOS beyond POD1. No effect was found regarding 30-day complications and 3-month PROs. Although EBL did not directly impact complications or PROs, surgeons may expect longer LOS when higher EBL is reported.
Clinical Relevance EBL above 275 mL with an interbody and 238 mL without an interbody were associated with prolonged LOS beyond POD1 in 1-level open lumbar fusion.
Level of Evidence 3.
Introduction
Lumbar fusions are commonly performed throughout the United States and have increased by approximately 180% from 2004 to 2015, reaching almost 200,000 procedures per year, totaling approximately $10.2 billion annually.1,2 Though elective lumbar fusions have been shown to improve patient-reported outcomes (PROs) at 2 years, the risk of complications persists. Rates of postoperative complications following degenerative lumbar fusion surgery range from 19% to 29%.3,4 An important intraoperative factor under the surgeon’s control that has been associated with perioperative outcomes is estimated blood loss (EBL).
Prior studies have shown that EBL is associated with increased morbidity following spine surgery.5 Recent studies have found that EBL exceeding 500 mL was associated with an increased risk of postoperative complications and prolonged length of stay (LOS) following lumbar fusion surgery of varying levels.6,7 Blood loss can provoke physiologic fluid shifts, which can affect cardiac, pulmonary, and renal status in the immediate postoperative period. Moreover, greater blood loss increases the need for transfusions, which places the patient at risk for transfusion reactions8 and immune system impairments that further raise the infection rate after surgery.9
Although higher EBL is a well-established risk factor for increased postoperative complications and LOS following lumbar fusion surgery,6,7 the exact amount of EBL that modifies outcomes remains elusive. In patients undergoing elective, 1-level posterior lumbar fusion with and without interbody, we sought to identify EBL thresholds associated with: (1) prolonged LOS, (2) postoperative complications, and (3) PROs.
Methods
Study Design
A retrospective cohort study was conducted from our institution’s prospective spine outcomes registry. The prospective registry includes all patients who underwent elective spine surgery and has been in existence since 2011. The registry enlists 3 full-time employees who prospectively call patients to obtain preoperative and postoperative data points and PROs. In the registry’s existence, approximately 12 fellowship-trained neurosurgery and orthopedic spine surgeons have contributed cases. Institutional review board approval was obtained for this study (institutional review board #211290).
Patient Population
Registry data were obtained for patients who underwent elective, 1-level, open posterior lumbar fusion with or without interbody fusion from October 2010 to April 2021 for degenerative reasons. Inclusion criteria were age ≥18 years and a signed consent for participation. Any lumbar fusion more than 1 level was excluded. Of note, 21 (2.7%) patients underwent a tubular minimally invasive surgery (MIS) approach and were also excluded from analysis. Postoperative care was standardized for all patients who were admitted to similar spine floors mostly in 1 location. Postoperative pain management was similar, which consisted of multimodal pain management.
Independent Variables
EBL measured in milliliters was the primary independent variable of interest. EBL was collected retrospectively from the operative report and was determined jointly by both the attending surgeon and anesthesiologist using intraoperative blood draws, intraoperative lab values, and blood in the suction canister postoperatively. Other independent variables included chief symptomatology, patient demographics, comorbidities, and perioperative data. These variables included age, gender, body mass index (BMI), employment status, intent to return to work, ambulatory status, symptom duration, diagnosis, revision vs primary surgery, indication for revision, preoperative antiplatelet use, and smoking status. Operative and perioperative variables included primary pathology, operation performed, operative time (minutes), and discharge disposition (home vs facility).
Since the placement of interbody device has been shown to increase EBL and operative time, analyses were separated into 1-level fusions with and without interbody placement.10 Interbodies were placed consistent with a transforaminal lumbar interbody fusion approach or a posterior lumbar interbody fusion approach. No anterior or lateral fusions were included.
Outcomes
The 3 primary outcomes of interest consisted of (1) LOS (days), (2) 30-day complications, and (3) 3-month PROs. LOS was treated as both a continuous variable and a dichotomized variable at 1 vs ≥2 days. Complications were defined as any complication within 30 days. PROs were taken at 3 months and included: (1) Numerical Rating Scale (NRS) back pain, (2) NRS leg pain, and (3) Oswestry Disability Index (ODI). In addition to mean PRO values, minimum clinically important difference (MCID) defined as an increase of 30% from baseline was calculated.11 PROs were prospectively collected over the phone or via email before surgery and 3 months postoperatively. Patients with NRS back pain/leg pain values of 0 preoperative and postoperative were excluded from the MCID analysis.
Statistical Analysis
Descriptive statistics were compiled for all demographic, preoperative, and postoperative characteristics. Means and SDs for continuous variables and frequency for categorical variables were computed. Continuous data were compared using Student t tests. MCID was defined as a 30% improvement over baseline PROs at 3 months following surgery.12 Univariate and multivariate linear and logistic regression were performed, controlling for age, BMI, and revisions. Receiver-operating characteristic (ROC) curve analysis was performed to determine whether EBL was a good binary classifier of outcomes. Sensitivity, specificity, area under the curve (AUC), and Youden’s Index were also analyzed. Any AUC that was <0.60 was determined to be poor, and for these, no Youden’s Index was calculated due to lack of clinical meaning. A P value <0.05 was considered statistically significant. The analysis was performed using SPSS version 22 (IBM Inc., Chicago, Illinois) and R Statistical Software version 4.0.3 (https://www.r-project.org/).
Results
Part I: 1-Level Posterior Fusion With Interbody Placement
Perioperative Patient Demographics
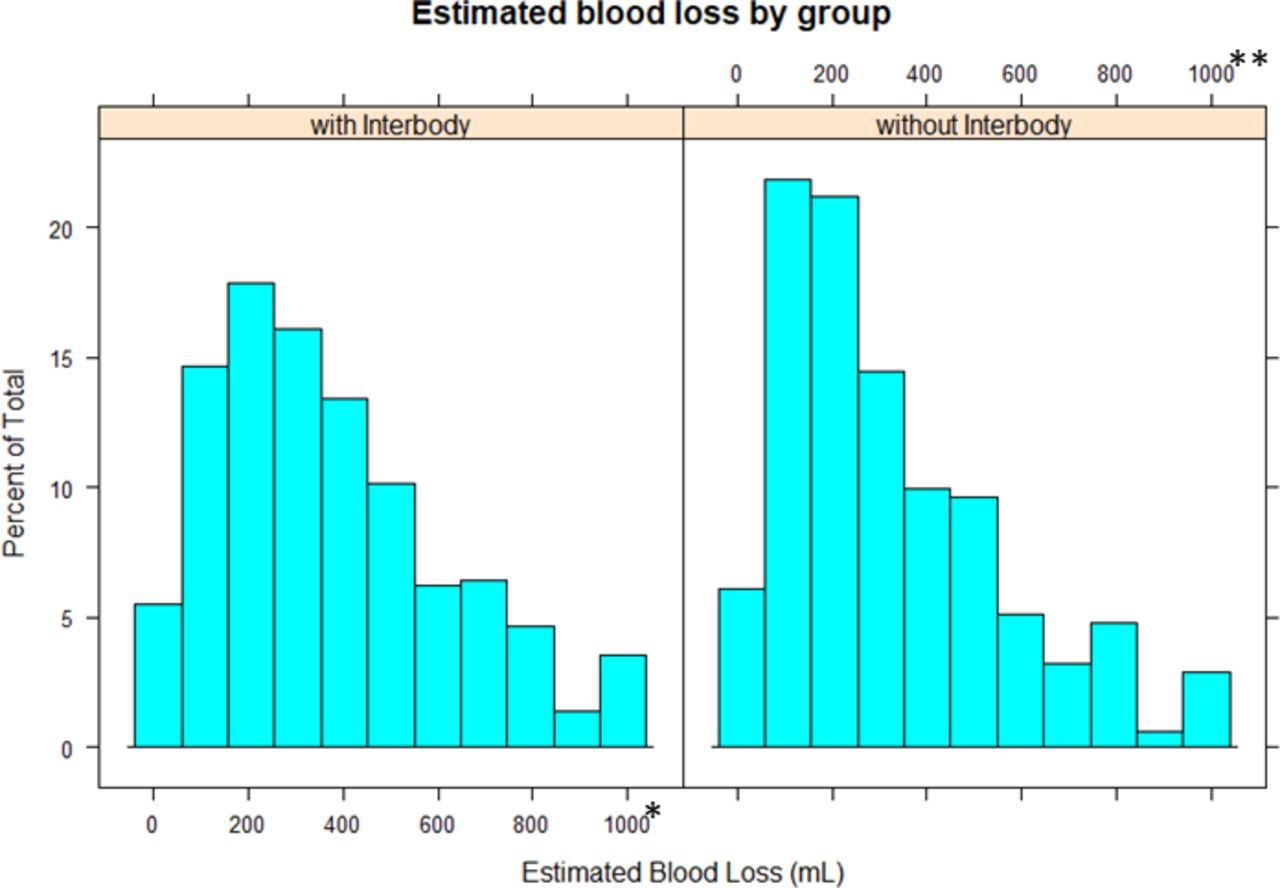
Of the 1183 patients undergoing elective, 1-level open posterior lumbar fusion, 763 also underwent interbody fusion. Mean age was 59.2 ± 11.6 years, and 43.8% were men. A total of 2.0% were on antiplatelet/anticoagulant therapy preoperatively. Median (interquartile range [IQR]) EBL was 350 mL (200–600), and median (IQR) operative time was 204 minutes (166–246). Detailed patient demographics, comorbidities, and preoperative characteristics are summarized in Tables 1 and 2. EBL distribution is shown in Figure 1A.
Demographic characteristics of patients receiving 1-level posterior lumbar fusion.
Operative and perioperative variables of patients receiving 1-level posterior lumbar fusion.

Histogram showing the distribution of estimated blood loss (EBL) in patients with 1-level open posterior lumbar fusion, with and without interbody fusion. *33 patients had EBL >1000, **17 patients had EBL >1000.
EBL Association With LOS
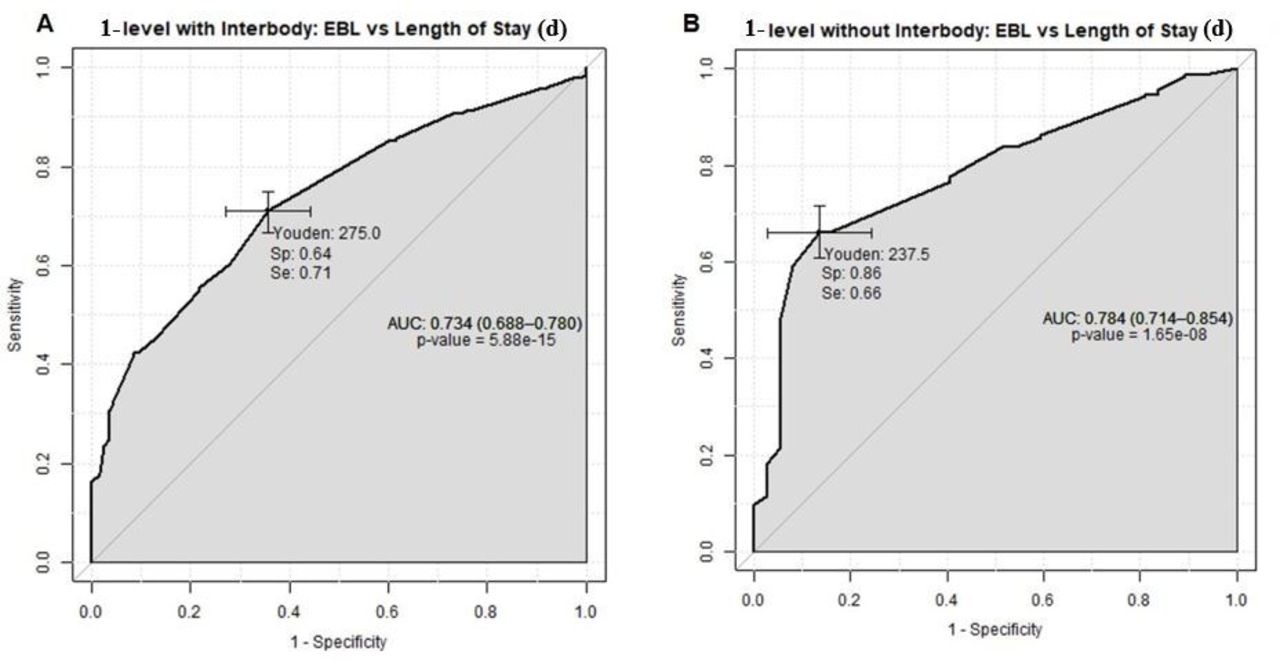
Median (IQR) LOS was 2 days (2–3). Univariate and multivariate linear regression demonstrated a significant but weak correlation between increased EBL and prolonged LOS (r = 0.243, P < 0.001), controlling for age, BMI, and revisions (Figure 2A, Table 3). ROC analysis of EBL as a predictor of LOS beyond POD1 demonstrated strong predictive value (AUC = 0.73, 95% CI 0.68–0.78, P < 0.001), and Youden’s Index calculation optimally differentiated EBL at 275 mL (Figure 3A).
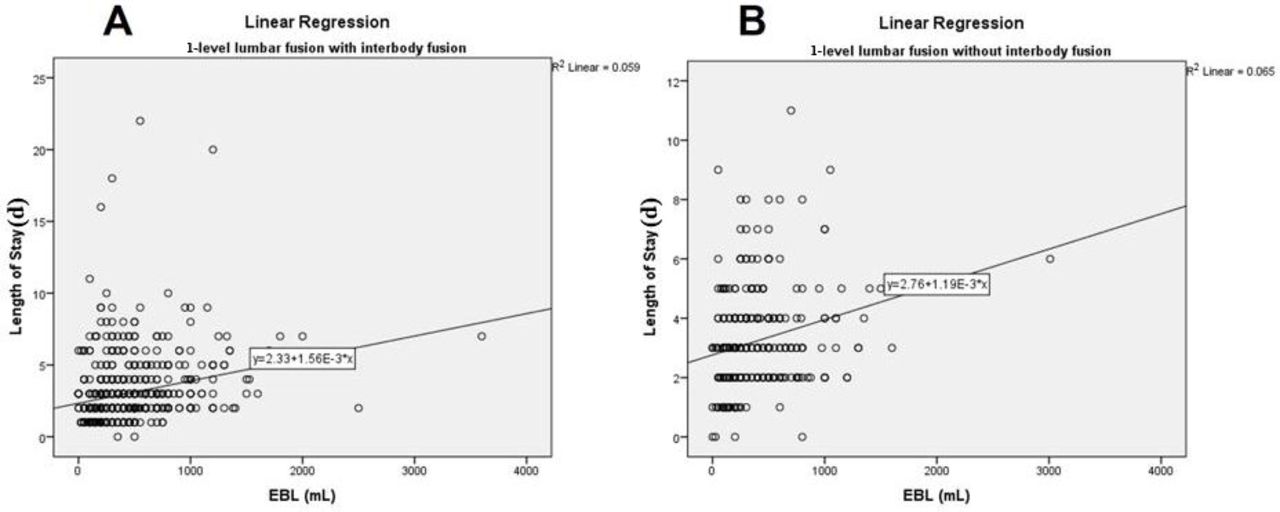
Regression graphs demonstrating the linear relationship between estimated blood loss (EBL) and length of stay: 1-level posterior lumbar fusion with interbody fusion (A), 1-level posterior lumbar fusion without interbody fusion (B).
Univariate/multivariate logistic and linear regression showing the association between estimated blood loss and outcomes, controlling for age, body mass index, and revision.
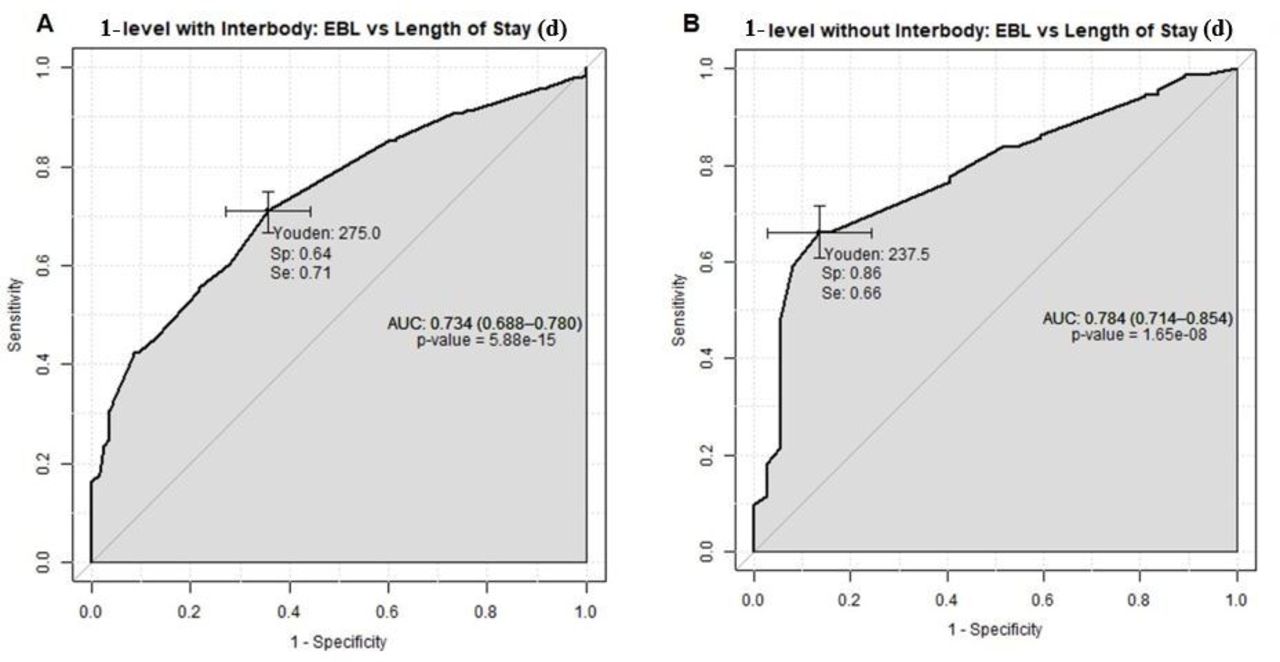
Receiver-operating characteristic curves (ROC) of estimated blood loss (EBL) vs length of stay of 1 d or more. Patients undergoing 1-level posterior lumbar fusion with interbody fusion (A) and patients undergoing 1-level posterior lumbar fusion without interbody fusion (B). AUC, area under the curve; Se, sensitivity; Sp, specificity.
EBL Association With 30-Day Complications
All medical and surgical complications were summarized in Table 4. There were a total of 41 (5.4%) patients with at least 1 complication, the most common being surgical site infection (SSI) with 18 patients (2.4%), followed by 13 (1.7%) urinary tract infections, 7 (0.9%) pneumonia, 2 (0.3%) neurological deficits, 2 (0.3%) deep vein thrombosis, and 1 (0.1%) hematoma. The majority of SSI resolved with a course of oral antibiotics (12, 1.6%), 2 (0.3%) required intravenous antibiotics, and 4 (0.5%) required surgical incision and drainage. A total of 34 (4.5%) patients were readmitted, and 18 (2.4%) required reoperation. Univariate and multivariate logistic regression showed no association between EBL and 30-day complications (OR = 1.00, 95% CI 0.99–1.00, P = 0.789) when controlling for the aforementioned variables (Table 3). AUC value for EBL as a predictor of complications was low and similar to random chance (AUC = 0.47, 95% CI 0.37–0.57, P = 0.624); therefore, no Youden’s Index was calculated (Table 5).
Medical/surgical complications of diabetic patients within 30 d after lumbar spine surgery.
Receiver-operating characteristic curve analysis of 1-level posterior lumbar fusion with patient-reported outcomes.
EBL Association With PROs
Average NRS back pain score was 6.8 ± 2.3 preoperative and 3.4 ± 2.7 at 3 months postoperative (P < 0.001). A total of 432 (56.6%) had achieved MCID 30 of NRS back pain scores at 3 months. The mean NRS leg pain score was 6.8 ± 2.4 preoperative and 2.5 ± 3.0 postoperative (P < 0.001). A total of 470 (75.3%) achieved 30% reduction of NRS leg pain scores at 3 months. The mean ODI score was 46.2 ± 13.9 preoperative and 27.5 ± 17.4 postoperative (P < 0.001). There were 400 (52.4%) patients who achieved 30% reduction of scores. Table 6 provides a tabulated form of these findings. No association was found between EBL and MCID PROs on univariate and multivariate logistic regression (Table 3). ROC analysis failed to demonstrate a correlation between EBL and MCID NRS back pain (AUC = 0.43, 95% CI 0.38–0.48, P = 0.016), MCID NRS leg pain (AUC = 0.48, 95% CI 0.42–0.53, P = 0.551) and MCID ODI (AUC = 0.48, 95% CI 0.43–0.53, P = 0.625) (Table 5). Given the poor ROC analysis, Youden’s Index was also not calculated.
Preoperative and 3-mo PROs in patients undergoing elective 1-level open posterior lumbar fusion.
Part II: 1-Level Posterior Fusion Without Interbody Placement
Demographic and Perioperative Variables
A total of 420 patients had 1-level spinal fusion without interbody fusion. Mean age was 61.6 ± 13.2, and 46.4% were men. Only 2.1% were on antiplatelet/anticoagulant therapy preoperatively. Median EBL (IQR) was 300 mL (150–500), and median (IQR) operative time was 202 minutes (160–248). Detailed patient demographics, comorbidities, and preoperative characteristics are summarized in Tables 1 and 2. EBL distribution is shown in Figure 1B. A total of 3 (0.7%) patients underwent a tubular MIS approach and were excluded from analysis.
EBL Association With LOS
Median (IQR) LOS was 3 days (2–4). Univariate and multivariate linear regression analysis demonstrated a significant but weak positive relationship between increased EBL and prolonged LOS (r = 0.25, P < 0.001) (Figure 2B, Table 3). ROC analysis of EBL as a predictor of LOS beyond POD1 is shown in Figure 3B. EBL higher than 238 mL was significantly correlated with prolonged LOS (AUC = 0.78, 95% CI 0.71–0.85, P < 0.001).
EBL Association With 30-Day Complications
Medical and surgical complications are summarized in Table 4. There were a total of 27 (6.4%) patients with at least 1 complication, the most common being urinary tract infections with 17 patients (4.0%), followed by 7 (1.7%) surgical site infections, 2 (0.5%) neurological deficits, 1 (0.2%) pneumonia, 1 (0.2%) deep vein thrombosis, and 1 (0.2%) hematoma. Of the 7 patients with SSI, 4 (1.0%) resolved with a course of oral antibiotics, 2 (0.5%) required intravenous antibiotics, and 1 (0.2%) required surgical incision and drainage. A total of 25 (6.0%) patients were readmitted, and 12 (2.9%) required reoperation. Univariate and multivariate logistic regression showed no association between EBL and 30-day complications (OR = 1.00, 95% CI 0.99–1.00, P = 0.989) (Table 3). ROC analysis shown in Table 5 did not demonstrate a significant correlation between higher EBL and the occurrence of medical and surgical complications (AUC = 0.55, 95% CI 0.43–0.66, P = 0.389).
EBL Association With PROs
Mean NRS back pain score was 6.7 ± 2.7 preoperative and 3.3 ± 2.7 at 3 months postoperative (P < 0.001). A total of 258 (61.4%) had achieved MCID 30 of NRS back pain scores at 3 months. The mean NRS leg pain score was 6.6 ± 2.8 preoperative and 2.8 ± 3.0 postoperative (P < 0.001). A total of 241 (75.3%) achieved MCID 30 of NRS leg pain scores at 3 months. The mean ODI score was 47.1 ± 15.1 preoperative and 28.9 ± 18.5 postoperative (P < 0.001). There were 375 (53.3%) patients who achieved MCID 30 of ODI. No association was found between EBL and MCID PROs on univariate and multivariate logistic regression (Table 3). Pre- and postoperative PROs are summarized in Table 6. ROC analysis showed poor association between EBL and MCID NRS back pain (AUC = 0.44, 95% CI 0.36–0.51, P = 0.122), MCID NRS back pain (AUC = 0.53, 95% CI 0.46–0.61, P = 0.328) and MCID ODI (AUC = 0.44, 95% CI 0.37–0.51, P = 0.101) (Table 5). Given the poor AUC values, no Youden’s Index was calculated.
Discussion
Spine surgeons seek to accomplish the goals of surgery as efficiently as possible while minimizing operative time and blood loss. Recent data have shown that in lumbar fusion surgery, increased EBL is a risk factor for suboptimal perioperative outcomes.6,7 In a study of 1183 patients undergoing elective, 1-level open posterior lumbar fusion, we showed that EBL above 275 mL with an interbody and 238 mL without an interbody were associated with prolonged LOS beyond POD1. In contrast, EBL had no effect on overall complications or PROs.
Addressing EBL in spine surgery is of critical importance and appears to be associated with perioperative outcomes. Studies have shown that blood loss can result in antibiotic dilution, coagulopathy, and an increased need for transfusions.5,13 The latter is known to suppress human T-cell proliferation,9 which can translate into increased risk of postoperative surgical site infections and urinary tract infections following lumbar spine surgery.14,15 Blood transfusion does not only increase operative time but also the cost-related burden.13 A retrospective study involving 3262 patients who received blood transfusions following elective spine surgery found that even a single unit was associated with increased LOS and postoperative morbidity, regardless of the preoperative hematocrit or patients’ comorbidities.16 Although in a 1-level lumbar fusion blood clots are unlikely to occur, attempting to make every surgery as safe as possible with minimal blood loss is of utmost importance. Moreover, when operating on patients with multiple comorbidities, little room for error and a lower threshold of significant EBL exist.
Although a clear definition for significant EBL in spine surgery is still missing, several studies have tried to determine the precise volume of EBL that might affect patients’ outcomes following lumbar spine surgery. Kobayashi et al7 involved 1168 patients undergoing either open or MIS transforaminal lumbar interbody fusions of varying levels and found that EBL ≥500 mL was associated with prolonged LOS (OR = 1.71, 95% CI 1.07–2.75) defined as LOS ≥75th percentile. They reported a mean LOS of 20.8 ± 9.8 days, which was much longer than our study (2.8 ± 2.4 days with interbody fusion, 3.0 ± 1.7 days without interbody fusion), and found that open surgery, fused levels ≥3 and operative time ≥300 minutes also correlated with prolonged LOS. In addition, increased age, greater number of comorbidities, drain use, and fluid administered were all considered risk factors for increased LOS.17–19 A randomized controlled trial conducted by Challier et al20 demonstrated a mean EBL of 364 and 271 mL in 1-level posterior lumbar fusion with and without interbody fusion, respectively. Another study by Huang et al6 included 199 patients who underwent lumbar fusion surgery for degenerative reasons. Significant EBL was defined as >500 mL (107 patients) and <500 mL (92 patients). The former was associated with a high complication rate (P = 0.002), defined as wound-related complications, delirium, pneumonia, urinary tract infection, transfusions, and systemic inflammatory response syndrome. Significant blood loss was also associated with prolonged LOS (P = 0.045), which was 9.8 and 8.6 days in patients with significant and nonsignificant EBL, respectively. Similarly, their study was not limited to 1-level fusion, which can explain the higher LOS compared with our study.
In this study, EBL was associated with prolonged LOS after POD1, but no effect was related to increased complications or 3-month PROs. LOS has been associated with increased hospital-acquired infections and higher risk for deep vein thrombosis.21,22 Moreover, increased LOS after spine surgery was associated with increased risk of 90-day postoperative complication and increased health care cost.23,24 Though EBL was not associated with complications or PROs, exploring the association of EBL with LOS can lead to better estimation of LOS by the hospital administrators as well as to implement early measures to minimize unwanted complications. That said, it is equally useful for surgeons and patients to know that EBL, even if higher than expected, was not associated with an increased risk of complications or poor 3-month PROs.
Future studies are needed to delineate the amount of EBL that influences patients’ outcome in multilevel spine surgeries and spinal deformity surgeries. Risk factors for EBL have long been explored in spinal deformity surgery and different ways to prevent them,25–28 yet the effect of EBL on LOS and patients’ outcome is still understudied. Preoperative estimation of EBL should be based on the magnitude and duration of surgery, along with the surgeon’s expertise and risk factors assessment. An accurate estimation of LOS based on EBL and other preoperative and intraoperative factors should focus on improving patients’ outcomes and increased cost-effectiveness.
This study has several potential limitations. First, errors can be present in reporting EBL by the surgeon and/or the anesthesiologist. EBL measurement is inherently inaccurate, and by definition, it is an estimation, as blood volume can be lost in gauze or other forms of hemostasis. Furthermore, it is sometimes poorly estimated how much irrigation is used in a case. Among general surgery procedures, frequent under and overestimation of EBL were demonstrated by Thomas et al29 when compared with measured blood loss as depicted by the actual hemoglobin levels, which we did not report. Second, there were wide SD ranges in EBL for both interbody and noninterbody cohort, which may be due to some cases being revision fusions and others being primary fusions. The wide ranges may also be due to the high number of surgeons who participated in the registry over the 10-year registry existence and major variation in technique and experience. Third, from a statistical perspective, we dichotomized our exposure variable (EBL), which was originally a continuous measure. However, a recent statistical review drawing from the cardiology literature30 argued against the credibility of certain thresholds such as exercise peak oxygen uptake, ejection fraction, and brain natriuretic peptide, as prognostic factors in heart failure. Though at times an apparent cutoff is easily discernible, it can be misleading, as the authors demonstrated that dichotomized physiological variables are often limited and statistically biased due to an intrinsic heterogeneity of the populations being dealt with. Overall, this study concluded that physicians should be vigilant when making decisions based on thresholds extrapolated from average measurements in a certain population, and these thresholds can be especially useful when applied toward high-risk individuals in clinical settings. Despite the information lost when dichotomizing a continuous variable, we still believe that EBL threshold might be of benefit for spine surgeons due to its potential implication in prolonged LOS. Fourth, we did not collect details regarding transfusions or cell-salvage devices, nor the amount of fluid administered. Fifth, in some cases, prolonged LOS might be attributed to unavailable transportation, administrative issues, and unsuitability of patient’s home, among other reasons.31 Sixth, this study suffers from the inherent limitations of retrospective cohort studies of pre-existing data, where information may be incomplete as compared with prospectively performed studies. Lastly, these data were received from a single-center study; hence, the result may not reflect the experience of other institutes.
Conclusion
In a cohort of patients undergoing 1-level posterior lumbar fusion with and without interbody fusion, EBL volumes above 275 mL with an interbody and 238 mL without an interbody were associated with increased LOS beyond POD1. However, no effect was found on overall complications and PROs. Thus, meticulous surgical technique to reduce EBL may lead to a reduction in LOS and healthcare costs.
Footnotes
Funding The authors did not receive any funding related to this study.
Disclosures Byron F. Stephens reports consulting fees from Dupuy-Synthes and Stryker Spine. The remaining authors have nothing to disclose.
Ethics Approval Institutional review board (IRB) approval was obtained for this study (IRB#211290).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.