


Article Figures & Data
Figures
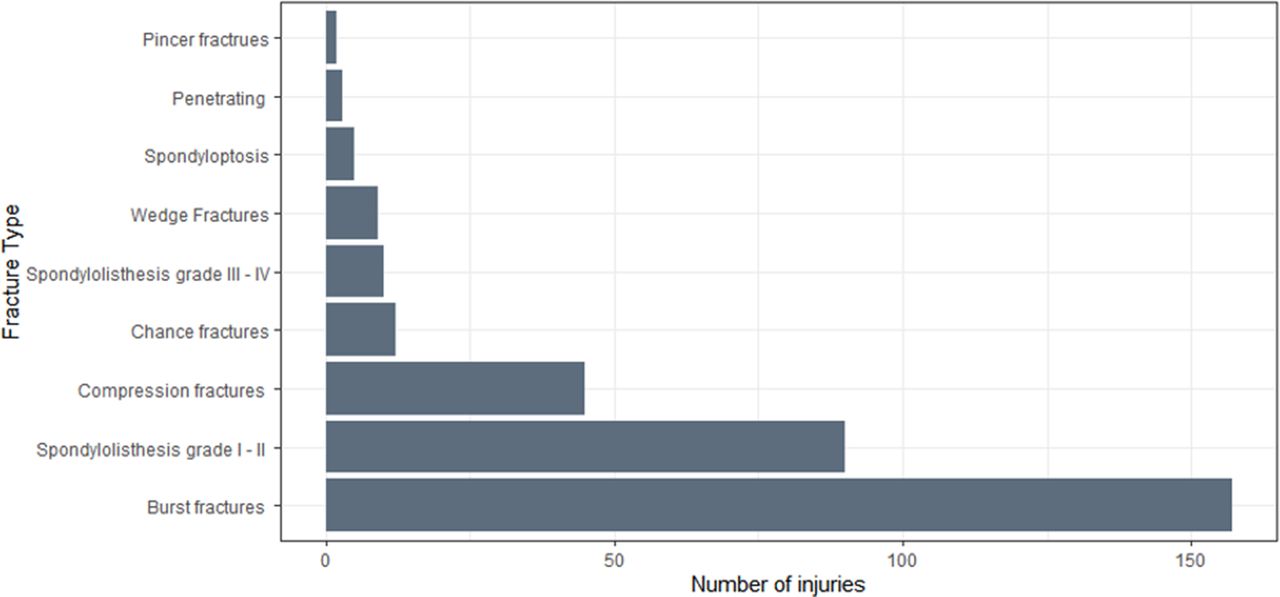
- Figure 1
Fracture types among 257 thoracic, thoracolumbar, and lumbar spine trauma patients (each fracture type counted separately when more than 1 injury was present).
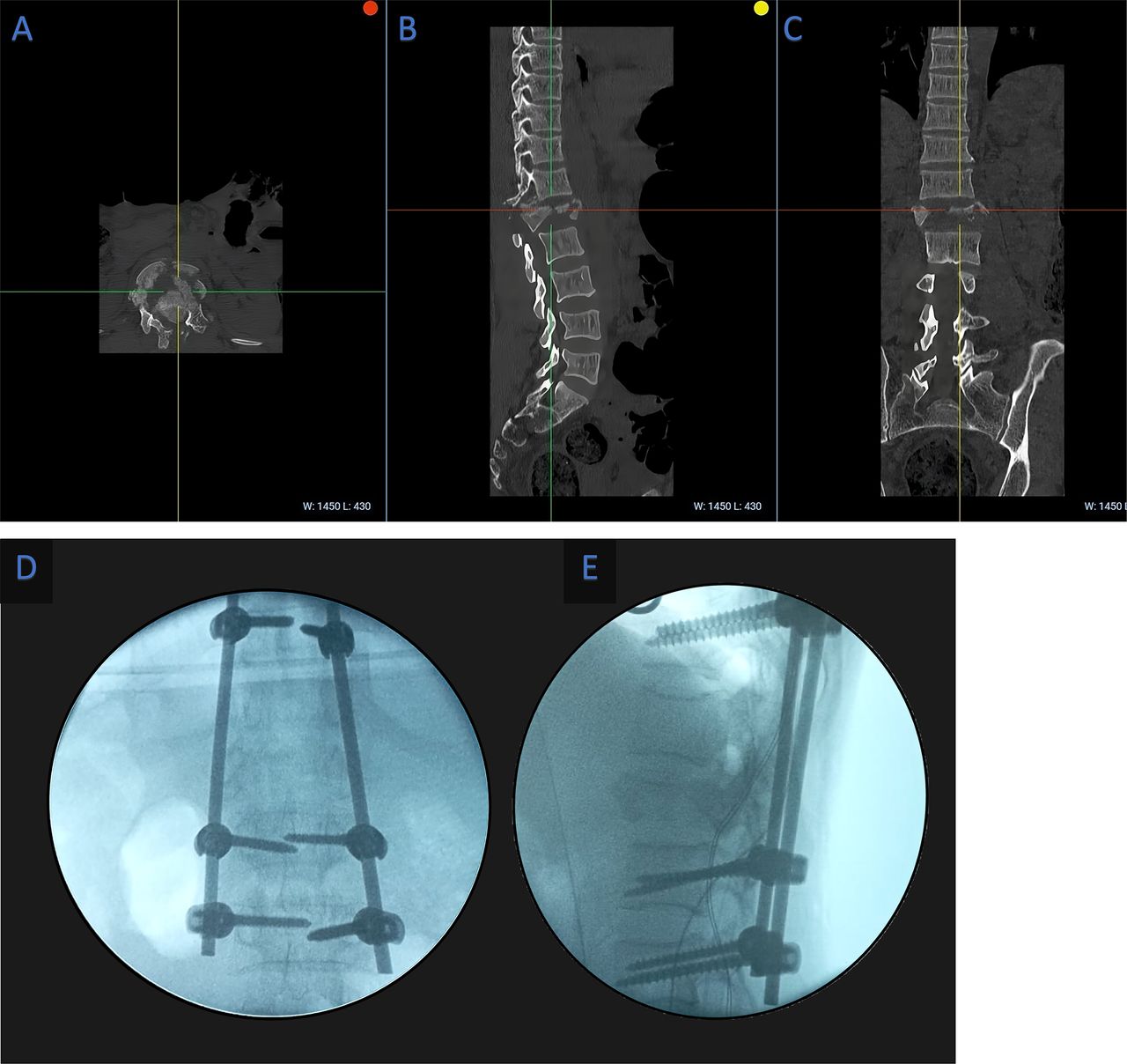
- Figure 2
(A–C) Axial, sagittal, and coronal preoperative computed tomography images of a patient with L1 burst fracture. (D, E) Intraoperative x-ray anteroposterior and lateral views after instrumentation.


Tables
- Table 1
Demographics, injury, and hospitalization information of patients with thoracic, thoracolumbar, and lumbar spine injuries.
Variable Total
N = 257Operative
n = 167Nonoperative
n = 90P Age, mean ± SD, y 35.2 ± 11.3 34.4 ± 11.3 36.8 ± 11.3 0.059 Sex, male, n (%) 215 (83.7) 137 (82) 78 (86.7) 0.435 Insurance, n (%) 0.819 Public 225 (87.5) 145 (86.8) 80 (88.9) Private 32 (12.5) 22 (13.2) 10 (11.1) Mechanism, n (%) 0.439 RTA 112 (43.6) 76 (45.5) 36 (40) Fall 95 (37.0) 57 (34.1) 38 (42.2) Other 50 (19.4) 34 (20.4) 16 (17.8) Admitted to OSH, n (%) 255 (99.2) 166 (99.4) 89 (98.9) 1.000 Location, n (%) Thoracic 52 (20.2) 34 (20.4) 18 (20) 1.000 Thoracolumbar junction (T10–L2) 189 (73.5) 126 (75.4) 63 (70) 0.425 Lumbar 16 (6.2) 7 (4.2) 9 (10) 0.116 Imaging, n (%) X-ray imaging 207 (80.5) 131 (78.4) 76 (84.4) 0.320 CT 80 (31.1) 55 (32.9) 25 (27.8) 0.477 MRI 152 (59.1) 101 (60.4) 51 (56.7) 0.719 Neurologic status, n (%) Complete (ASIA A) 117 (45.5) 80 (47.9) 37 (41.1) 0.362 Incomplete (ASIA B–D) 81 (31.5) 62 (37.1) 19 (21.1) 0.013 Intact (ASIA E) 59 (23) 25 (15.0) 34 (37.8) < 0.001 Indication for surgery, n (%) 232 (90.3) 167 (100) 65 (72.2) < 0.001 Length of stay, median (IQR), d 25 (14–43) 28 (15–45) 22.5 (11.2–41.8) 0.117 Time from injury to admission, median (IQR), d 3 (1–7) 3 (1–6) 3 (1–9.8) 0.755 Pressure ulcer, n (%)a 54 (21) 32 (19.2) 22 (24.4) 0.419 Mortality, n (%) 3 (1.2) 1 (0.6) 2 (2.2) 0.584 Abbreviations: ASIA, American Spinal Injury Association; CT, computed tomography; IQR, interquartile range; MRI, magnetic resonance imaging; OSH, outside hospital; RTA, road traffic accident.
↵a One missing value.
Parameter Value (n = 167) Operation new, n (%)a Posterior fusion thoracic/lumbar 163 (97.6) Decompression only 3 (1.8) Screws, mean ± SD 5.6 ± 1.7 Number of levels fused, mean ± SD 2.7 ± 1.1 Postoperative imaging, n (%) X-ray imaginga 85 (50.9) Computed tomographya 2 (1.2) Magnetic resonancea 2 (1.2) ↵a One missing value.
ASIA on Admission, n (%) ASIA on Discharge, n (%) Total A B C D E A 108 2 3 0 0 113 (44.8) B 2 33 8 3 0 46 (18.3) C 0 0 7 5 1 13 (5.2) D 0 0 0 15 6 21 (8.3) E 0 0 0 0 59 59 (23.4) Total 110 (43.7) 35 (13.9) 18 (7.1) 23 (9.1) 66 (26.2) 252 (100) Abbreviation: ASIA, American Spinal Injury Association.
Operative Status Worsened Stable Improved Operative (n = 163) 1 (0.6) 137 (84.0) 25 (15.3) Nonoperative (n = 89) 1 (1.1) 85 (95.5) 3 (3.4) Total (n = 252) 2 (0.8) 222 (88.1) 28 (11.1) Abbreviation: ASIA, American Spinal Injury Association.
Variable Univariable Logistic Regression Multivariable Logistic Regressiona OR (95% CI) P OR (95% CI) P Age, continuous, y 0.98 (0.96, 1.00) 0.106 - - Age Young, <30 y (n = 91) Reference 0.110 - - Old, ≥30 y (n = 166) 0.64 (0.36, 1.09) - - - Sex Female (n = 42) Reference 0.339 - - Male (n = 215) 0.70 (0.33, 1.42) - - - Injury level Upper thoracic (n = 33) Reference - Lower thoracic (n = 122) 1.22 (0.53, 2.69) 0.634 - - Lumbar (n = 102) 0.92 (0.40, 2.06) 0.847 - - Insurance Private (n = 32) Reference 0.633 ... Public (n = 225) 0.82 (0.35, 1.78) - ... Neurologic Examination Complete: ASIA A (ref) vs B–E; (n = 117) 0.76 (0.45, 1.27) 0.297 ... ... Incomplete: ASIA B–D (ref) vs A/E; (n = 81) 0.45 (0.25, 0.81) 0.009 ... ... Intact: ASIA A–D (ref) vs E; (n = 59) 0.29 (0.16, 0.53) <0.001 0.27 (0.13, 0.54) <0.001 Time from injury to admission, continuous, d 0.97 (0.94, 0.99) 0.048 0.95 (0.92, 0.99) 0.007 Abbreviation: ASIA, American Spinal Injury Association.
↵a Multivariable logistic regression analysis controlled for age, sex, and mechanism of injury.
- Table 6
Predictors of neurologic improvement among all patients and operative patients. Multivariable logistic regression controlling for age, sex, admission neurologic exam, and level of injury.
Variable Univariable Logistic Regression Multivariable Logistic Regression OR (95% CI) P OR (95% CI) P All patients, N = 193a Age 0.432 - Young, <30 y (n = 75) Reference - - - Old, ≥30 y (n = 118) 0.71 (0.29, 163) - - - Sex 0.820 - Female (n = 25) Reference - - - Male (n = 168) 0.88 (0.30, 3.19) - - - Injury level Upper thoracic (ref) vs lower thoracic/lumbar (n = 29)b 5.52 (1.10, 100) 0.100 - - Lower thoracic (ref) vs upper thoracic/lumbar (n = 101) 3.97 (1.67, 10.56) 0.002 0.61 (0.03, 3.96) 0.656 Lumbar (ref) vs thoracic (n = 63) 0.14 (0.05, 0.33) <0.001 0.14 (0.01, 0.83) 0.071 Insurance 0.947 - Private (n = 20) Reference - - - Public (n = 173) 1.04 (0.23, 3.40) - - - Time from injury to admission Continuous, d 0.93 (0.85, 0.99) 0.093 0.93 (0.84, 1.00) 0.113 Operative 0.034 0.067 Nonoperative (n = 55) Reference - Reference - Operative (n = 138) 3.83 (1.27, 16.61) - 3.58 (1.02, 17.07) - Admission neurologic examination <0.001 0.002 Complete: ASIA A (n = 113) Reference - Reference - Incomplete: ASIA B–D (n = 80) 8.71 (3.38, 27.05) - 5.74 (1.94, 18.00) - Operative patients, N = 138 Age 0.299 - Young, <30 y (n = 57) Reference - - - Old, ≥30 y (n = 81) 1.63 (0.66, 4.27) - - - Sex 0.921 Female (n = 23) Reference - - - Male (n = 115) 1.06 (0.35, 3.94) - - - Injury level Upper thoracic (ref) vs lower thoracic/lumbar (n = 20) 4.85 (0.93, 89.30) 0.133 - - Lower thoracic (ref) vs upper thoracic/lumbar (n = 71) 3.36 (1.34, 9.22) 0.012 0.47 (0.02, 2.89) 0.495 Lumbar (ref) vs thoracic (n = 47) 0.17 (0.06, 0.42) < 0.001 0.09 (0.00, 0.51) 0.027 Time from admission to operating room Continuous, d 1.01 (0.99, 1.03) 0.237 - - Variable Univariable Logistic Regression OR (95% CI) P Age Young, <30 y (n = 91) Reference 0.940 Old, ≥30 y (n = 166) 1.10 (0.10, 23.81) - Sex Female (n = 42) Reference 0.995 Male (n = 215) 1.20 (0.00, NA) - Injury level Upper thoracic (n = 33) Reference - Lower thoracic (n = 122) 6.00 (0.00, NA) 0.997 Lumbar (n = 102) 1.00 (0.00, 3.00) >0.999 Insurance Public Reference 0.996 Private 1.15 (0.00, NA) - Time from injury to admission Continuous, d 0.90 (0.53, 1.07) 0.517 Operative status Nonoperative (n = 90) Reference 0.281 Operative (n = 167) 0.27 (0.01, 2.80) - Admission neurologic examination Complete: ASIA B-E (n) Reference 0.994 Incomplete: ASIA A (n) 6.11 (0.00, NA) - Length of stay, continuous, d 0.99 (0.93, 1.02) 0.806 Abbreviation: ASIA, American Spinal Injury Association.
Multivariable logistic regression analyses were not completed because no predictors met the threshold of p < 0.10 after univariable logistic regression analysis.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.