


Abstract
Background Differences in lumbar morphology and nerve root positioning between supine and prone decubitus are poorly analyzed. This study aimed to perform a magnetic resonance imaging (MRI) study to describe lumbar morphology, nerve root, and related structures positioning in the prone position, while comparing with conventional supine MRI, in patients with lumbar symptoms. The second aim was to define safe working zones for lumbar surgical procedures.
Methods This study was a prospective, single-center, observational study. Fifty patients with persistent low back and/or radicular pain that was unresponsive to conservative treatment were consecutively selected. Supine and prone 3 Tesla MRIs were performed. Two independent researchers performed an imaging analysis of predefined variables.
Results Lumbar lordosis significantly changed from 49.3° in the supine position to 52.1° in the prone position (P = 0.005), without a statistically significant difference in lower lumbar lordosis. No consistent changes were found regarding foraminal height, root-to-pedicle or root-to-superior articular process distances. The exiting nerve root was found between 42% and 49% of the foraminal height (as measured from the upper border of the lower pedicle). The left retroperitoneal lateral corridor showed no significant size variation from the supine to the prone position (P = 0.196 and P = 0.600, for L3–L4 and L4–L5 levels, respectively).
Conclusion This study suggests prone positioning may increase global lumbar lordosis, without changing the position of other major anatomical structures. The exiting nerve root positioning can be estimated in relation to foraminal height. These finding may help optimizing planning and minimizing iatrogenic lesions.
Level of Evidence 3.
Introduction
Spine surgery is undergoing technological advancements, with a trend to use minimally invasive spine (MIS) techniques and endoscopic procedures and to extend their indications. In fact, several studies suggest that these techniques are associated with reduced soft tissue damage, blood loss, postoperative pain, hospital stay, and recovery time while maintaining efficacy and safety (when compared to conventional open surgery). However, MIS and endoscopic techniques have unique complications related to their steep learning curve and commonly performed technical variations.1–6 Therefore, to minimize the risk of such complications, surgeons need to have deep knowledge of spine anatomy. In fact, the upsurge of MIS and endoscopic procedures has contributed to a renewed interest in spine anatomy.7–9 Moreover, as techniques and approaches become more structured and tailored, preoperative planning becomes increasingly important in preventing unanticipated complications and optimizing outcomes.10–12 For instance, given that positioning variations may potentially interfere with the location and morphological trends of anatomic structures, it is of utmost importance to study and understand these variations.
For lumbar disease, magnetic resonance imaging (MRI) is among the most widely used and valuable imaging techniques. Generally, it is performed in a supine/dorsal decubitus position as opposed to prone/ventral decubitus, the most frequently used surgical positioning. Although it has been used for the diagnosis of tethered cord syndrome, prone MRI is rarely used as a diagnostic tool in degenerative cases.13,14 Previous spinal MRI-based studies on the prone position were mostly performed in small samples, and recent works have tried to evaluate its utility in estimating lumbar nerve root and ganglion position, with variable results.15–17
As the impact of intraoperative prone positioning on lumbar spine anatomy remains unknown, prone MRI studies may provide new data and increase accuracy for spinal procedures. The aim of the present study is to describe lumbar morphology, nerve roots and related structures positioning in the prone position and to find potential relevant changes when compared with the conventional supine position in patients with lumbar symptoms. The secondary aim is to help define safe working zones for MIS and endoscopic procedures to reduce the risk of iatrogenic lesions.
Methods
Study Design, Setting, and Participants
This was an observational cross-sectional study performed in a single center (Unidade Local de Saúde de São João, Porto; the largest tertiary hospital in Northern Portugal). Approval was granted by the Ethics Committee of Centro Hospitalar Universitário de São João/Faculdade de Medicina da Universidade do Porto, in May 2023 (CE 73/2023). The study was conducted between July and December 2023. We included a consecutive sample of patients who attended the outpatient clinics of our center, met eligibility criteria and provided informed consent.
Participants were included if they were adults (aged ≥18 years) with persistent low back and/or radicular pain that was unresponsive to conservative treatment and if they were willing to participate and able to understand the study protocol.
Exclusion criteria included age <18 years; pregnancy; previously known spine deformity (such as high-grade spondylolisthesis, scoliosis, or fracture); previous abdominal, retroperitoneal, or spine surgery; and/or contraindication for MRI (such as the presence of ferromagnetic material).
Variables and Data Sources
Clinical and demographic data were collected from all patients. In particular, we collected data on the following variables during medical consultation: age, gender, height, weight and spine-related symptoms. Additionally, we collected information from MRI to compare results obtained in supine and prone positions.
MRI Acquisition and Patient Positioning
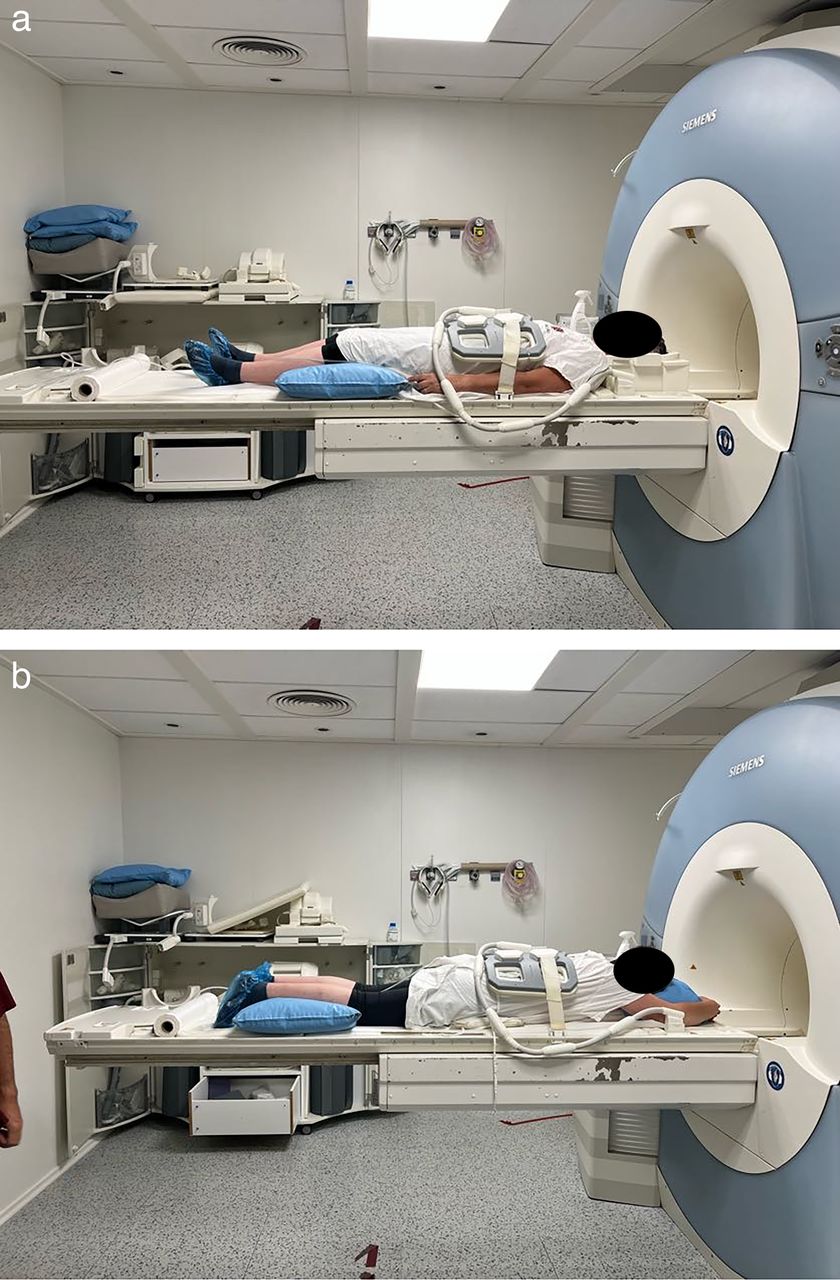
The MRI protocol was defined between orthopedic surgeons and neuroradiologists. Patients were scanned in a 3 Tesla MRI (Magneton TrioTrim, Siemens Healthcare) equipped with multichannel body antennas. A 2D sagittal plane T2-weighted turbo-spin-echo sequence (TR/TE = 3750/84 ms, flip angle = 135, matrix = 384 × 288, echo train length = 19, and slice thickness = 3 mm), along with a axial 2D T2-weighted turbo-spin-echo sequence (TR/TE = 5930/117 ms, flip angle = 130, matrix = 384 × 250, echo train length = 22, and slice thickness = 3 mm) was acquired in supine position and then repeated in prone position. During the latter, support pillows were placed between the table and the patient’s chest and pelvis (Figure 1) to reduce motion artifacts from breathing. Additionally, clinical 2D T1W and short-tau inversion recovery acquisitions were obtained but were not analyzed in this work.

Patient positioning for supine (a) and prone (b) magnetic resonance imaging.
Imaging Analysis
Two researchers independently conducted all measurements described below, using the Sectra IDS7 software. Any significant discrepancies were solved by a third supervising author.
Imaging analysis included median sagittal plane, bilateral sagittal plane (midpedicular), and axial plane (mid-intervertebral disc [IVD]) variables, as described below:
Median sagittal plane analysis and measurements
IVD degeneration and listhesis grading (as classified by Pfirrmann and Meyerding classifications, respectively).
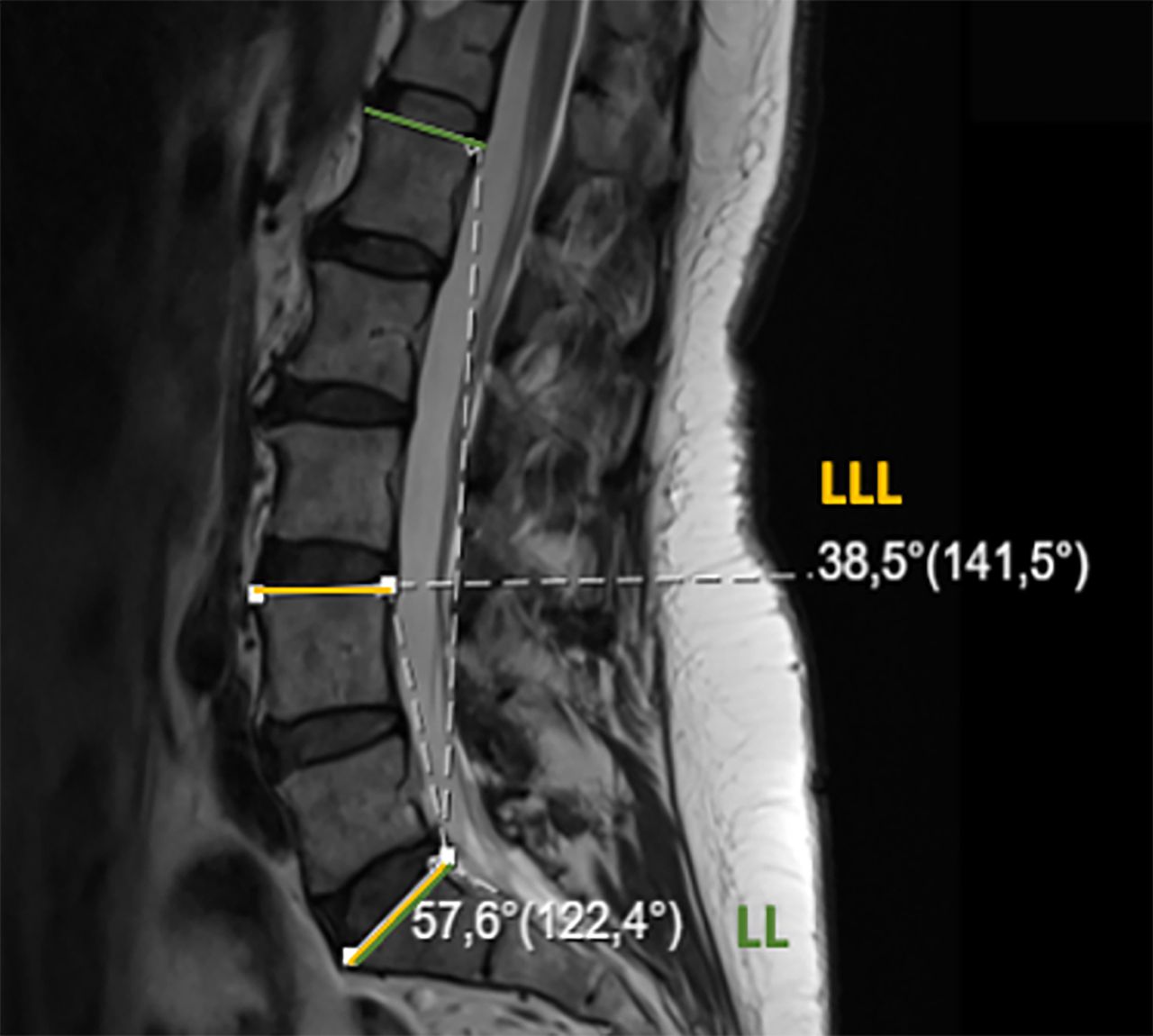
Lumbar lordosis (LL): angle (°) between the upper endplate of L1 and the upper endplate of S1 vertebrae (Figure 2).
Lower lumbar lordosis (LLL): angle (°) between the upper endplate of L4 and the upper endplate of S1 vertebrae (Figure 2).
Anterior, middle, and posterior IVD height for L3 to L4, L4 to L5, and L5 to S1 levels: distance (millimeters) between the upper and lower endplates of each segment at the anterior, middle, and posterior disc locations (Figure 3).

Lumbar lordosis (LL; green) and lower lumbar lordosis (LLL; yellow).

Anterior (a), middle (m), and posterior (p) intervertebral disc height.
Bilateral sagittal plane (midpedicular) analysis and measurements:
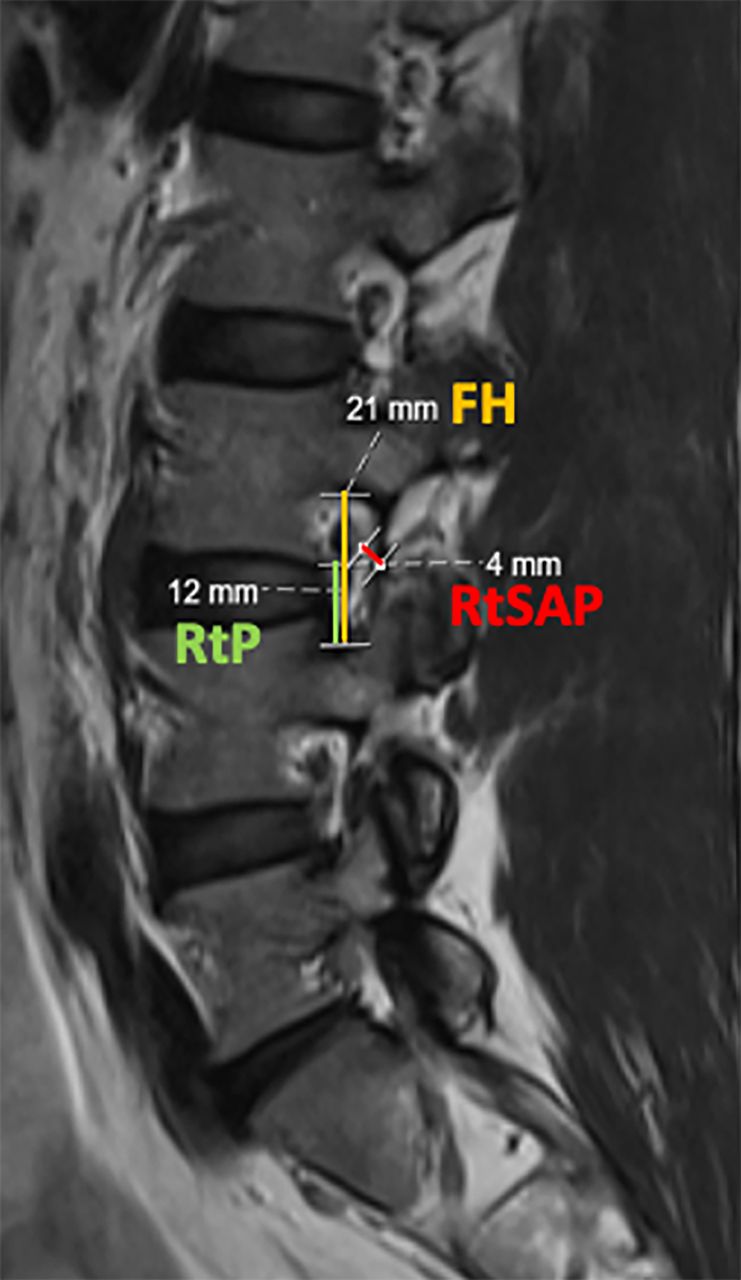
Foraminal height (FH) for L3 to L4, L4 to L5, and L5 to S1 levels: longitudinal distance (millimeters) between the inferior pedicle wall of the upper level and the superior pedicle wall of the level below (Figure 4).
Root-to-pedicle (RtP) distance for L3 to L4, L4 to L5, and L5 to S1 levels: longitudinal distance (millimeters) between the inferior border of the emerging nerve root and the superior pedicle wall of the level below (Figure 4).
Root-to-superior articular process (RtSAP) distance for L3 to L4, L4 to L5, and L5 to S1 levels: distance (millimeters) from the emerging nerve root to the tip of the superior articular process (Figure 4).
Axial plane (mid-IVD) analysis and measurements:
Lumbar stenosis grading (according to the Schizas classification).
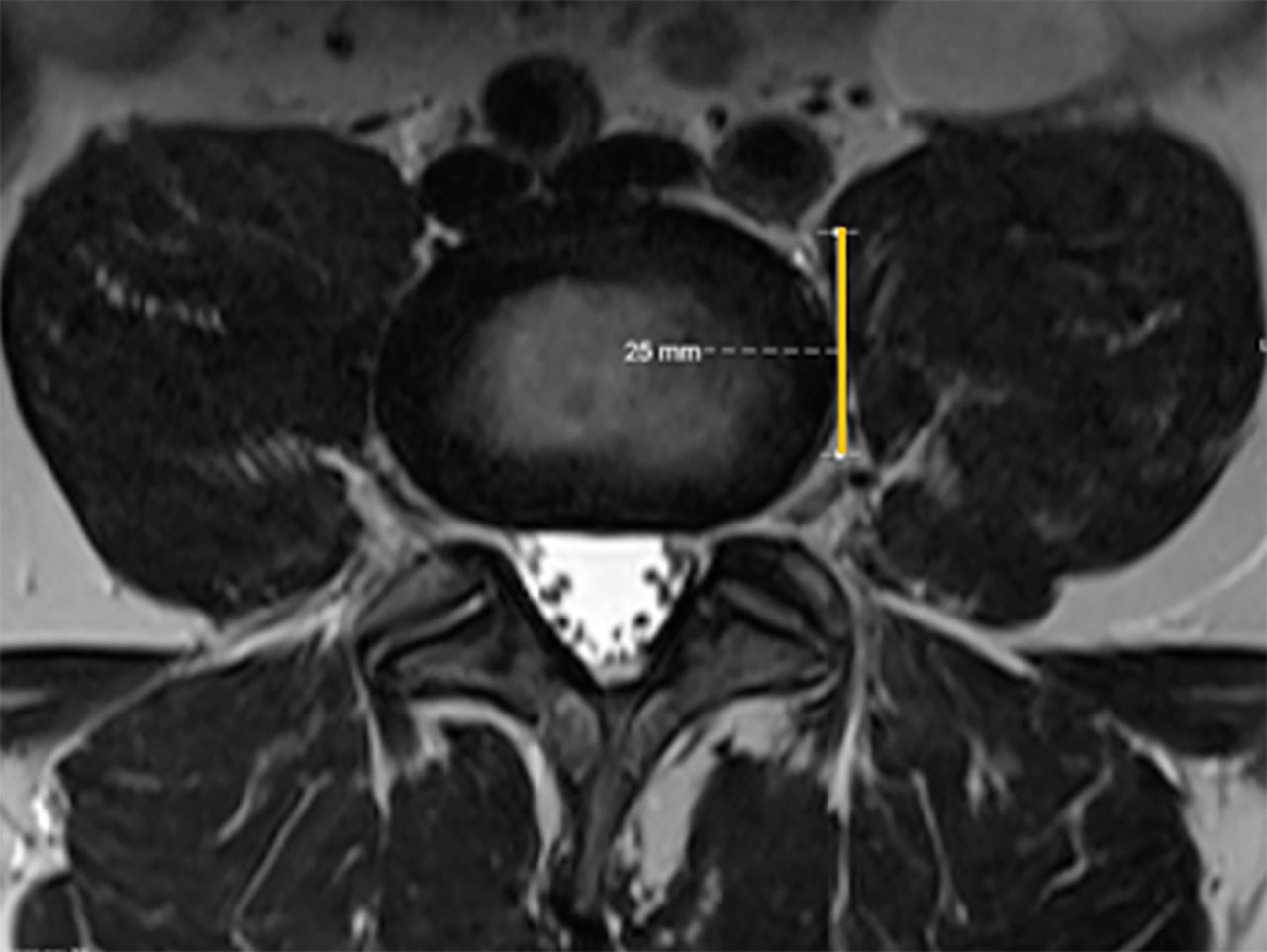
Safe corridor for L3 to L4 and L4 to L5 levels: measurement of the left corridor (mm) for lateral lumbar interbody fusion (LLIF) at the mid-IVD position (Figure 5).
Description of signs of segmental instability.

Foraminal height (FH), root to pedicle (RtP), and root to superior articular process (RtSAP) distances.

Left lateral safe corridor (yellow line) for lateral lumbar interbody fusion approach.
Statistical Analysis
Continuous variables were described using means ± SDs, while categorical variables were described using absolute and relative frequencies. We performed a paired Student t test (for continuous variables) or χ 2/Fisher’s exact test (for categorical variables) to evaluate each parameter between supine and prone positions. In addition, to evaluate interobserver reliability, we computed intraclass correlation coefficients (ICC) and their 95% confidence intervals. ICC estimates were calculated based on a mean rating (k = 2), consistency agreement, and 2-way random-effects model.18
Statistical analysis was performed using SPSS version 27.0 (IBM Corp., USA), and P values less than 0.05 were considered statistically significant.
Results
Fifty patients were included. Four cases were subsequently excluded due to claustrophobia (n = 2) or imaging artifacts precluding adequate analysis (n = 2). Therefore, a total of 46 cases (28 female patients; 61%) were analyzed. Participants’ mean age was 50.3 ± 9.4 years, and the most common complaints were lumbar pain (n = 19), radicular pain (n = 7), or both (n = 20).
Median Sagittal Plane Analysis and Measurements
Based on supine MRI analysis, all patients presented some degree of lumbar IVD degeneration and disc height loss (Pfirrmann grading III–V) was evident in 37%, 59%, and 63% of patients for L3 to L4, L4 to L5, and L5 to S1 levels, respectively. In prone MRI analysis, results were similar, and statistically significant differences were not found.
Regarding olisthesis, grade I spondylolisthesis was identified in 14 supine MRI cases (L3–L4 level: n = 2; L4–L5 level: n = 10; L5–S1 level: n = 2). In prone MRI analysis, 4 additional cases were identified (P = 0.001).
Table 1 summarizes and compares LL, LLL, and IVD heights in both positions. A high degree of interobserver reliability was found between LL and LLL measurements, with an average LL ICC 0.962 (95% CI 0.910, 0.986) and average LLL ICC 0.921 (95% CI 0.857, 0.956); reliability for IVD heights was good, with average ICC always above 0.800. Mean LL was 49.3° in the supine compared to 52.1° in the prone position (P = 0.005), while mean LLL suffered no statistically significant variation (36.9° in supine vs 36.4° in the prone). Moreover, positional differences were evident at L3 to L4 anterior IVD height (paired difference −0.3 mm, 95% CI −0.6, −0.1; P = 0.015) and L5 to S1 posterior IVD height (paired difference −0.3 mm, 95% CI −0.6, 0.0; P = 0.032), with higher values in the prone position.
Lumbar lordosis and IVDh comparison from supine to prone.
Bilateral Sagittal Plane (Midpedicular) Analysis and Measurements
Measurements of both left and right FH at L3 to L4, L4 to L5, and L5 to S1 levels, longitudinal RtP distance, and RtSAP distances are depicted in Table 2. Average ICC ranged from 0.776 to 0.912. No statistically significant differences were found, except for left L5 to S1 FH (paired difference −0.8 mm, 95% CI −1.3, −0.3; P = 0.001), right L4 to L5 FH (paired difference 0.4 mm, 95% CI 0.0, 0.9; P = 0.039), right L4 to L5 (paired difference −0.4 mm, 95% CI −0.6, −0.1; P = 0.003), and right L5 to S1 (paired difference −0.3 mm, 95% CI −0.5, 0.0; P = 0.049) RtSAP distances.
Foraminal height, root-to-pedicle, and RtSAP distances comparison from supine to prone.
To estimate the longitudinal position of the root within the foramen, the relationship between FH and RtP was established, as defined by RtP/FH. Results are presented in Table 3, and no statistically significant differences were found between supine and prone positions. The exiting nerve root was found between 42% and 49% of the FH, as measured from the upper border of the lower pedicle.
Relationship between root-to-pedicle and foraminal height.
Axial Plane (Mid-IVD) Analysis and Measurements
The lateral lumbar working corridor (see Table 4) suffered no statistically significant size variation from the supine to prone position for both L3 to L4 and L4 to L5 levels (P = 0.196 and P = 0.600, respectively; with average ICC ranging from 0.799 to 0.937). Globally, the working window for LLIF was significantly narrower at the L4 to L5 level (P < 0.001 for both supine and prone positions when compared with L3 to L4 space), potentially increasing the risk of complications when performing a prone LLIF at this level.
Lateral lumbar working corridor.
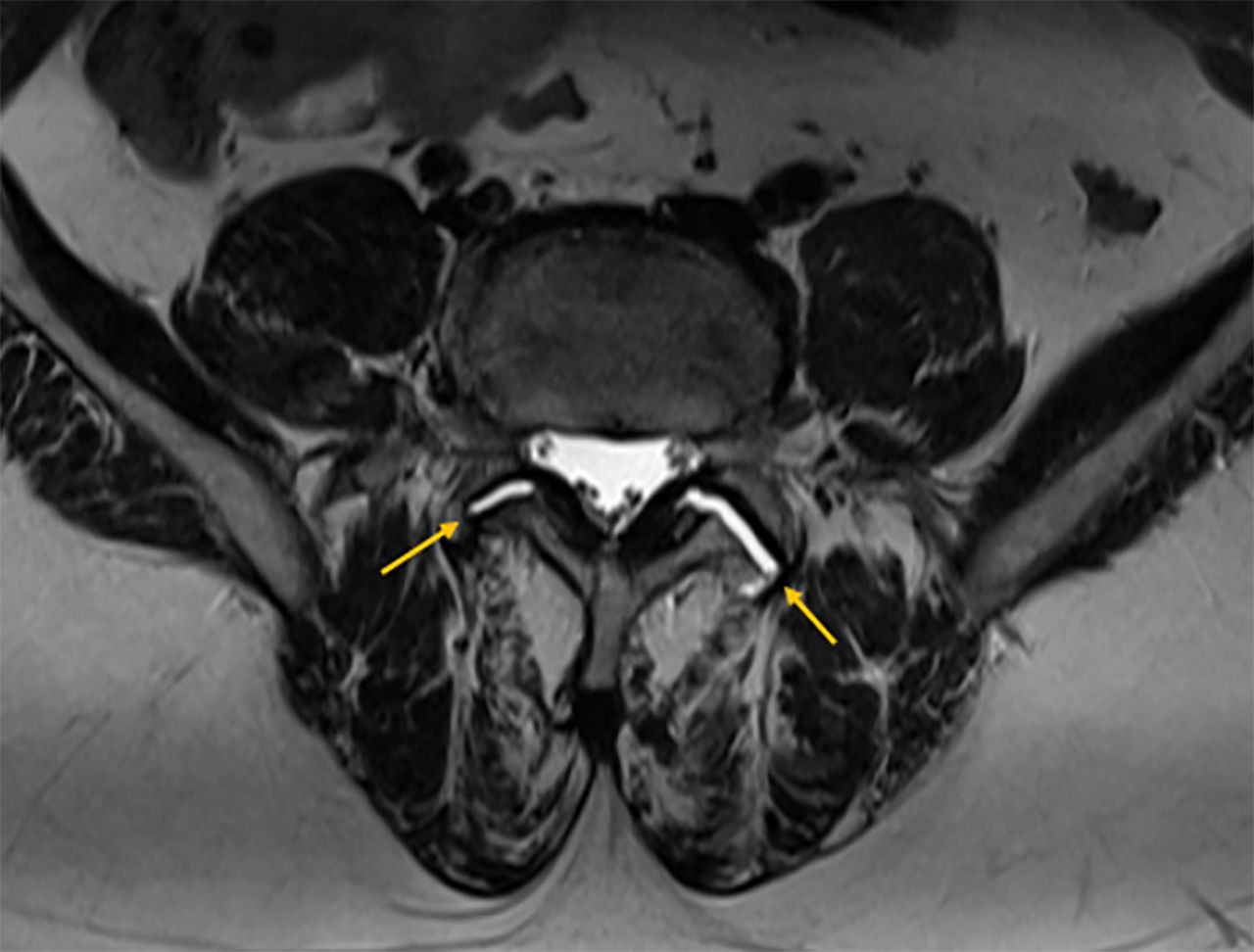
Additional analysis of axial T2-weighted images revealed dispersed facet joint fluid signal changes, suggestive of dynamic lumbar spine instability (Figure 6).

Disperse facet joint fluid signal changes (arrow), suggestive of dynamic lumbar spine instability.
Discussion
This study aimed to assess differences in lumbar morphology and nerve root positioning between supine and prone decubitus, using a 3 Tesla MRI. To the best of our knowledge, this is one of the most extensive quantitative analysis of lumbar positional changes using MRI.
Median Sagittal Plane Analysis and Measurements
The dynamic nature of the spine and its contribution to symptomatic degenerative disease is evident in this study, as prone MRI analysis revealed additional cases of grade I spondylolisthesis (P = 0.001) compared to supine imaging, suggestive of lumbar instability. Positional changes in lumbar parameters have been widely described, mainly using simple radiography.19–21 However, quantitative MRI analysis of LL and IVD height variation from supine to prone is poorly described. Similar to results from Amaral et al15 and Yingsakmongkol et al,17 the current study suggests that prone position may improve global LL, optimizing preoperative conditions in lumbar fusion procedures, where LL correction and sagittal balance reestablishment are paramount features.
Bilateral Sagittal Plane (Midpedicular) Analysis and Measurements
Changes in foraminal measures have become clear while studying cervical and lumbar spine motion, again revealing the dynamic range of effects achievable in the spine.22–24 However, in this study, no consistent changes were found for FH, RtP, or RtSAP distances. We hypothesize that their magnitude might be minimal and consequently could not be detected, as the minimal difference using this software is 1 mm.
Moreover, RtP/FH relation showed that the exiting nerve root can be found between 42% and 49% of the FH. We believe that foraminal ligaments (FLs) might play a role in this finding. Elaborating on this theory, previous anatomical works have demonstrated that FLs connect spinal nerves with the bordering structures such as lumbar vertebral bodies, IVD, ligamentum flavum, articular processes and facet joint capsules.25–27 Therefore, FLs may stabilize the nerve root within the foramen or, in pathological cases, contribute to its compression. Interestingly, Jack et al performed cadaveric dissections in the cervical spine and demonstrated that cutting the FLs results in the detethering of the nerve roots, indirectly suggesting their role as “stabilizers”.28
Axial Plane (Mid-IVD) Analysis and Measurements
Measurement of the left retroperitoneal lateral corridor for LLIF at both L3 to L4 and L4 to L5 levels revealed no significant size variation from the supine to the prone position. This is supported by the work of Yingsakmongkol et al17 who found no major differences in lumbar nerve roots, psoas muscle morphology and great vessels position between supine and prone positions. On the contrary, Amaral et al15 and Munim et al29 suggested posterior psoas muscle retraction in the prone position.
Globally, the working window for instrumentation was significantly narrower at L4 to L5 than at L3 to L4 level, likely increasing the risk of complications at the lower level while performing a prone LLIF, as corroborated by the cadaveric work from Guérin et al.30
Moreover, in a descriptive analysis of axial T2-weighted images, changes in facet joints fluid signals were found in some cases, suggesting dynamic lumbar spine instability, which may contribute to mechanical and/or neurological symptoms.
Limitations and Strengths
Our main limitation concerns the relatively small number of patients included in this pilot study. In addition, patients with previous surgeries or existing metallic hardware were not assessed, which may limit the interpretation of these results to this subgroup that may have a stiffer and more degenerated spine with fibrotic changes. Moreover, the degree of degenerative changes ranged widely among participants. A third issue relates to patient positioning to minimize imaging artifacts in prone MRI, and 2 support pillows were used; the lower one, placed over the abdomen/pelvic area, may have influenced positional changes in lumbar parameters, as IVD height suggests an inflection point approximately at the L4 to L5 level. Therefore, LL might be even higher, and LLL may increase in the prone position.
The present study also has some strengths. First, it is one of the most extensive quantitative analysis of lumbar positional changes using MRI. Second, ICC revealed good to excellent interobserver reliability among measurements. Third, this study may have some implications for clinical practice, such as helping to estimate the lumbar nerve root position within the foramen or providing useful insights of pain generators in patients with minimal changes in supine images, such as signs of segmental instability.
Conclusion
This study shows that the prone position increased global LL, with no other major anatomical variations between supine and prone imaging. Consistently, the exiting nerve root was found around half of the FH. Comparing supine and prone MRI may reveal additional instability levels that may contribute to the mechanical or neurological symptoms.
Footnotes
Funding This study was funded by the Project SSIn - Spine Surgery Innovation (Code: 79701) - Faculty of Medicine of University of Porto.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Centro Hospitalar Universitário de São João/Faculdade de Medicina da Universidade do Porto, in May, 2023 (CE 73/2023).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.