


Abstract
Background Metastatic spine tumor surgery (MSTS) is an important treatment modality of metastatic spinal disease (MSD). Open spine surgery (OSS) was previously the gold standard of treatment till the early 2010s. However, advancements in MSTS in recent years have led to the advent of minimally invasive spinal surgery (MISS) techniques for the treatment of MSD. The clear benefits of MISS have resulted in a current paradigm shift toward today’s gold standard of MISS and early adjuvant radiotherapy in treating MSD patients. Nonetheless, despite improvements in surgical techniques and the rise of literature supporting MISS for MSD, there are still certain situations whereby MISS is not desirable or even suitable. There has also yet to be any literature describing the considerations of not using MISS in MSD in today’s clinical context.
Methods A narrative review was conducted for this manuscript. All studies related to OSS and MISS in MSTS were included.
Results A total of 54 studies were included in this review. These studies discussed various advantages of MISS for MSD in today’s clinical context, including the patient profile, location of vertebrae involved with metastasis requiring treatment, tumor characteristics, as well as equipment availability.
Conclusion This study establishes situations in which MISS can be less applicable despite the advantages it may confer over traditional OSS. MSTS should be individualized, depending on the experience of the surgeon. OSS is a time-tested approach that still holds weight in MSTS and should be readily utilized depending on the clinical situation.
Level of Evidence 4.
Introduction
Surgery has been an established modality of treatment for metastatic spinal disease (MSD), with open spine surgery (OSS) the gold standard till around the early 2010s.1 The indications for surgery are cord compression, spinal instability, pathological fractures, and intractable pain.1,2 These have been constant since the early 1980s when treatment of metastatic spine disease evolved and established surgery as a dependable treatment option.1,3,4 However, OSS is usually associated with extensive soft tissue dissection, which leads to excessive blood loss, increased hospital length of stay, and complication rates.5–8
In recent years, advancements in metastatic spine tumor surgery (MSTS) have led to the advent of minimally invasive spinal surgery (MISS) techniques for the treatment of MSD. MISS has shown benefits in reducing mortality, morbidity, and hospital length of stay, as well as allowing earlier introduction of adjuvant radiotherapy (RT) and chemotherapy.6,9,10 The clear benefits of MISS have resulted in a current paradigm shift toward today’s “gold standard” of MISS followed by early adjuvant RT in treating MSD patients.1 Nonetheless, even with the advantages of MISS as described above, the functional and neurological outcomes of patients undergoing MISS as compared with OSS have been showed in several studies to be similar.11–14 Hence, it still remains to be seen if the advantages accorded by MISS do translate to clinical improvements in MSD patients in the long run.
The aim of MISS in MSD is to achieve the same surgical goals of decompression of neural structures for improvement of neurological function, stabilization of the spine, and allowing for postoperative safe adjuvant RT and local tumor control with the minimization of surgical approach related morbidity.15 This effectively translates to less blood loss, operative time, and postoperative morbidity.12,16,17 MISS includes the use of percutaneous pedicle screw fixation as well as mini-open techniques to perform tumor decompression and corpectomy to achieve the outcomes mentioned above. The recently described separation surgery also allows the creation of separation between tumor tissue and the neural structures to allow safe adjuvant RT and local tumor control.18 Patients who undergo MISS have a shorter length of hospital stay than those of OSS, likely due to the lower invasiveness of surgery.19,20 Hence, they are able to ambulate faster and be discharged earlier. MISS also negates the risk of potential dead space or tissue necrosis formation due to extensive dissection in OSS,21,22 allowing for faster wound healing times due to smaller incisions. This enables earlier initiation of adjuvant therapy for these patients,10,11 overall improving the management of MSD for them.
Despite the improvements in surgical techniques and the rise of literature supporting MISS for MSD,6,11,15 there are still certain situations whereby MISS is not desirable or even suitable. There has also yet to be any literature describing the considerations for not using MISS in MSD in today’s clinical context. In this manuscript, we aim to review the literature and highlight personal experiences from our senior authors, regarding the various situations whereby MISS may not be suitable in MSD.
Methods
This narrative review was conducted using PubMed, Medical Literature Analysis and Retrieval System Online (MEDLINE), The Cochrane Library, and Scopus databases through 31 July 2024. The keywords used were (minimally invasive surgery OR MIS OR MISS OR mini-open spine surgery OR open spine surgery) AND (spine OR vertebra OR vertebrae OR spinal) AND (metastasis OR bone neoplasm OR bone tumor OR spine neoplasm OR spine tumor OR metastatic epidural spinal cord compression).
The inclusion criteria for the review were studies with a discussion on the type of surgery in MSTS. All studies that had no description regarding the surgical procedure performed were excluded. The articles were selected in 2 stages (Figure 1). First, the abstracts identified by the above searches were downloaded, and the list was screened using the relevant inclusion and exclusion criterias (non-human studies, no full text, not in English and duplicates). Next, the full texts of this shortlisted list were downloaded and assessed for eligibility. All articles that did not have any surgical procedure described were excluded at this stage. The reference lists of the publications were then hand-searched for additional relevant studies. This process was repeated twice by our senior authors independently.

Flow diagram of the review and selection of cases.
Results
MISS for MSD has recently gained traction and demonstrated its ability in various studies to treat MSD patients of varying severity. Kumar et al18 demonstrated the utility of MISS techniques in treating patients with spinal instability secondary to spinal metastases and metastatic spinal cord compression, with significantly decreased blood loss and length of stay. In a meta-analysis by Pranata et al23 which compared MISS with instrumented fusion with conventional OSS instrumented fusion for the treatment of MSD, MISS was associated with decreased blood loss and lower blood transfusion rates, as well as lower rate of complications and duration of stay. There were also comparable rates of neurological improvement and duration of surgery. Similar findings of decreased blood loss, transfusion rates, complication rates, and duration of hospital stay have also been found in meta-analyses done by Lu et al, Perna et al, and Pennington et al.16,24,25 Despite this, OSS has also shown potential benefits to be kept in the MSTS armamentarium. Colangeli et al26 showed in their retrospective review that OSS was more a more suitable treatment choice when tumor debulking was central to the local control plan. Studies have also shown that patients with substantial posterior involvement of spinal elements, such as the facet joints, are unlikely to get pain relief from minimally invasive procedures alone.27,28 Thus, it is important to consider the various situations in which MISS is less suitable. In situations where MISS is unable to access the area of the lesion, OSS is an important fallback to allow access and stabilization.
Situations Where Miss May Not Be As Suitable
Tumor Characteristics
The type of tumor is an important decision-making factor for MSTS surgeons. In patients with hypersclerotic lesions such as those with prostate and certain breast metastases,29 the vertebrae can be very difficult to cannulate with MIS probes. The introduction of the guide wire into the vertebrae body can also be difficult in patients with hypersclerotic tumors, and bending or breaking of the wire has been reported when the wire is inserted.30 As such, they are best operated by open technique to allow for adequate dissection and location of entry point for pedicle screw insertion. In our experience, intraoperative image intensifier-guided delineation of vertebrae landmarks is also not easy in hypersclerotic tumors.
MISS is also less feasible in patients with hypervascular tumors, such as renal cell, thyroid, and hepatocellular carcinoma,31 due to reduced ability to control intraoperative bleeding. An open technique will confer easier control of bleeding intraoperatively. In the same vein, hypervascular tumors where preoperative embolization has failed will logically require open techniques to allow for adequate intraoperative control of bleeding.
Extent of Surgery
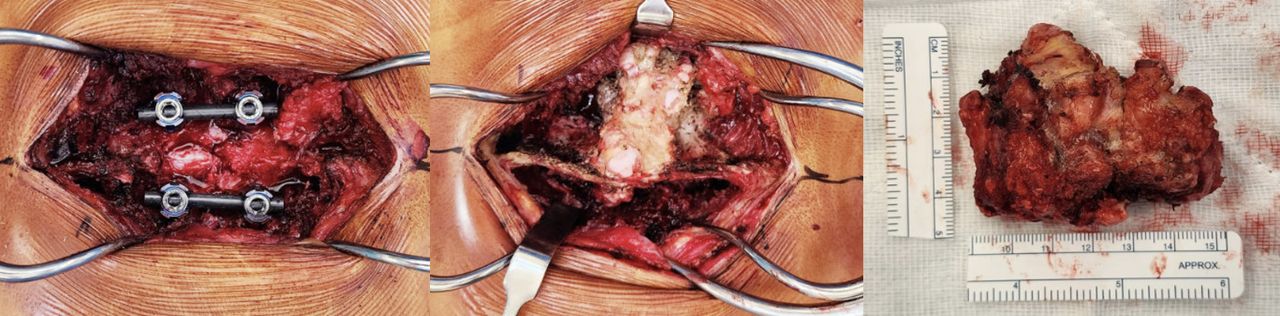
In order to decide whether to elect MISS or OSS, the extent of planned surgery must also be taken into account. Indications for undertaking MSTS are disease-related cord compression, spinal instability, pathological fractures, and intractable pain.1,2,32 In certain scenarios, surgical resection of the tumor or decompression of the spine can involve total en-bloc corpectomy (Figure 2). This is usually considered in isolated metastatic lesions of slow-growing malignancy (ie, oligometastatic breast cancer), patients with an expected survival of more than 2 years, and an acceptable functional status of the patient due to the high surgical morbidity.10,33 Barzilai et al also noted the relative indication for en-bloc resection of spinal metastasis where stereotactic RT may not be available.34 In the cases above where reconstruction of the anterior column is required33 after undertaking extensive decompression surgery, it can be technically challenging to achieve the reconstruction and fusion with an MIS technique. Likewise in young patients where extensive decompression has been done (eg, corpectomy and hemivertebrectomy) and reconstruction of the spine is required, it will be easier to perform fusion through an open technique. This allows for direct visualization of the fusion bed and control of any potential bleeding, as these patients undergoing corpectomy are also known to have increased intraoperative bleeding and total transfusion requirement.35
In cases where there is significant posterior column involvement with the tumor and decompression of that level is required, MISS may not be as suitable (Figure 3). Tan et al36 showed in their study that posterior facet visualization is more challenging with MISS as compared with OSS. The ability of OSS to provide visualization during decompression is important and also allows instrumentation if required. This is an important consideration in MSTS where stabilization of the spine in the most efficient manner is important.

Example of patient with oligometastasis undergoing metastectomy and requiring open spine surgery.

Exampled of open spine surgery having good access to posterior elements allowing thorough decompression and metastectomy.
Previous Operation at the Level of Surgery
In cases where previous surgery at the affected level has been done, there may be extensive scarring, and landmarks may not be easily identified, making MISS a more daunting undertaking. This is an important consideration in cases of MSD where patients may have various comorbidities;29,30 hence, surgical duration should be kept to the minimum to avoid potential complications from prolonged surgery or anesthesia. The development of computer-guided navigation techniques in recent years has also allowed for more accurate localization of levels and screw positioning.31,32 Morgan et al showed in their single-center randomized controlled trial that MISS was associated with a significantly longer operating time compared with OSS.37 It is notable that navigation techniques can potentially be more technically demanding and thus result in increased operating times or not be available beyond tertiary centers. In our experience, if navigation systems are not available or prior surgery at the affected level has been done, OSS should be considered for MSD patients.
Location of Tumor
The most common location for spinal metastasis in the vertebrae is in the thoracic spine (60%–80%), followed by the lumbar spine (15%–30%), and lastly the cervical spine (<10%).38,39 MISS is currently well developed for the thoracic, thoracolumbar, and lumbar spine due to the ease of imaging in these areas with a gentler change in the sagittal profile of patients. In cases where the site of metastasis is in the occipitocervical or cervicothoracic region, MISS may not be as suitable since intraoperative localization of levels with imaging intensifier may be difficult.38 In these cases, intraoperative navigation with the O-arm or robot-assisted pedicle screw placement has been described,32,40,41 but this specialized equipment involves significant costs42,43 and training that may not be available in less specialized centers.44 In our opinion, for locations such as the occipitocervical and cervicothoracic regions, MISS may be less suitable due to inherent challenges with imaging these regions.
Profile of MSD Patients
The profile of MSD patients also plays an important role in deciding whether MISS is a feasible treatment plan for MSD. In the pediatric group, MISS instruments have not been well developed for use in this group of patients. Recent use of MISS in the pediatric population has been limited to small case series for scoliosis and discectomy.36,45,46 Likewise, small-statured patients similar to the pediatric population would require open technique as the landmarks of 2 continuous vertebrae will be very close to each other, which limits the use of multiple small incisions for pedicle screw insertion.
Miscellaneous
MISS is commonly augmented with specialized equipment intraoperatively such as navigation and robotic systems to increase the accuracy of instrumentation.47–50 Hence, a trained team adept in using such equipment is needed, which leads to a further increase in overhead. More often than not, MISS is incorporated with early stereotactic RT postoperatively, which results in the requirement for such facilities to be present to maximize the advantages of MISS.34 The relative novelty of MISS technique also poses a high barrier of entry toward incorporating MISS in one’s practice. This can be significant especially for less developed countries or for young surgeons who are just starting out in their own clinical practice.
The Role of Miss in MSTS Today
Notwithstanding the previously discussed points, MISS techniques should still be considered for the appropriate MSTS patient. Clinical studies of MISS done in thoracolumbar MSTS have shown benefits in reducing blood loss and overall hospital length of stay.14,18 MISS has also shown benefits to be utilized as part of “separation surgery,”15,18 where the surgical goal is not for metastasectomy but rather to achieve circumferential tumor debulking and decompression and facilitate improved adjuvant RT postoperatively.
The development of Enhanced Recovery After Surgery pathways51 around the world, coupled with the increase in patient blood management strategies,52,53 has also reduced the invasiveness in MSTS and positively impacted the outcomes of patients undergoing MSTS. With the trend toward MISS, together with robotic and navigation technology in recent years, it is ever so important to understand when MISS or OSS should be utilized, depending on the surgical goal (Table).
Considerations in which MISS/OSS may be more feasible for MSD patients.
Limitations
To our knowledge, this study is the first to highlight the utility of OSS in today’s clinical practice, but it also faces some limitations. First, this study is conducted as a narrative review, and there is currently a lack of established guidelines and opinion on this topic. The varying types of MSD in patients also result in heterogeneity in the review, and the multitude of different surgical techniques in MSTS precludes the conduct of a direct comparative study between the 2 surgical approaches. Our team recognizes the clinical benefit of MISS over OSS shown in literature, but as discussed above, either technique should not be a universal fit for all MSTS patients. The rapid advancement of MISS has also seen the introduction of robotic and navigation techniques to further enhance the potential of MISS. These are viewed as adjuncts for improving the execution of MISS and are not explicitly discussed in our manuscript.
Our manuscript thus provides clarity into the direct utility of OSS vs MISS in MSTS and allows MSTS surgeons to have more deliberate surgical planning considering the factors listed above to benefit patients undergoing MSTS. With the publication of this manuscript, higher-powered comparative studies can be performed between the 2 approaches to further highlight the benefits of either approach in clinical practice.
Conclusion
MISS is becoming increasingly prevalent in the treatment of MSD, and surgical techniques are constantly evolving to benefit patients. However, it is important to understand the limitations of MISS in various clinical context as highlighted in this manuscript. MSTS should be individualized to the patient, depending also on the experience of the surgeon. OSS is still a time-tested approach that holds weight in MSTS and should be readily utilized depending on the clinical situation. This highlights the importance of keeping OSS in the armamentarium despite the trend toward MISS in recent years.
Acknowledgments
1. We acknowledge the AO Technological Commission Spine Expert Group for the discussions of Metastatic Spine Tumour Surgery management which have led to the formulation and submission of this manuscript.
2. We also acknowledge Dr Aye Sander Zaw for her help in proofreading the manuscript and submission of the manuscript for publication.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.