


Article Figures & Data
Figures
- Figure 1
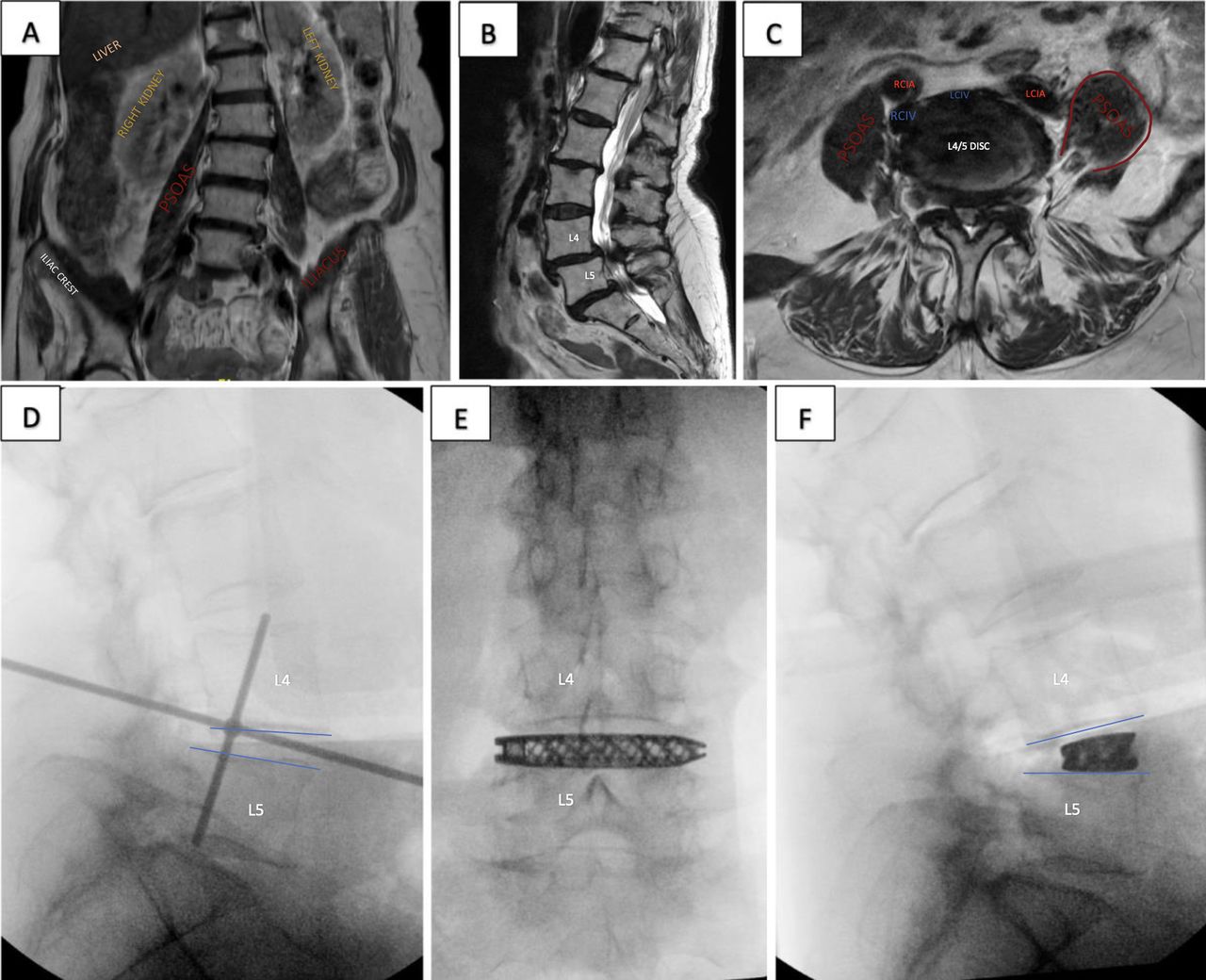
Case Example 1: A 72-year-old woman presented with neurogenic claudication symptoms and bilateral lower limb symptoms. Preoperative magnetic resonance imaging coronal (A) illustrates coronal deformity and asymmetry of iliac crests, with ease of access likely through the right. Preoperative sagittal (B) with grade 1 anterolisthesis of L4/5 and L5/S1 and associated canal stenosis. Preoperative axial (C) of L4/5 with severe canal stenosis, asymmetry of psoas—left psoas resembling “Mickey Mouse Ear”—favoring right-sided approach. However, the vascular anatomy—the right common iliac vein trajectory—encroaching on the right anterior disc space is noted. She underwent an uncomplicated right-sided L4/5 prone lateral interbody fusion with a posterior approach for L5/S1 level and L4 to S1 pedicle screws. Intraoperative radiography (D) showing fluoroscopy targeting and final implant position in anteroposterior view (E) and lateral view (F) with a decrease in spondylolisthesis at L4/5 through a right-sided approach. RCIA, right common iliac artery; LCIA, left common iliac artery; RCIV, right common iliac vein; LCIV, left common iliac vein.
- Figure 2
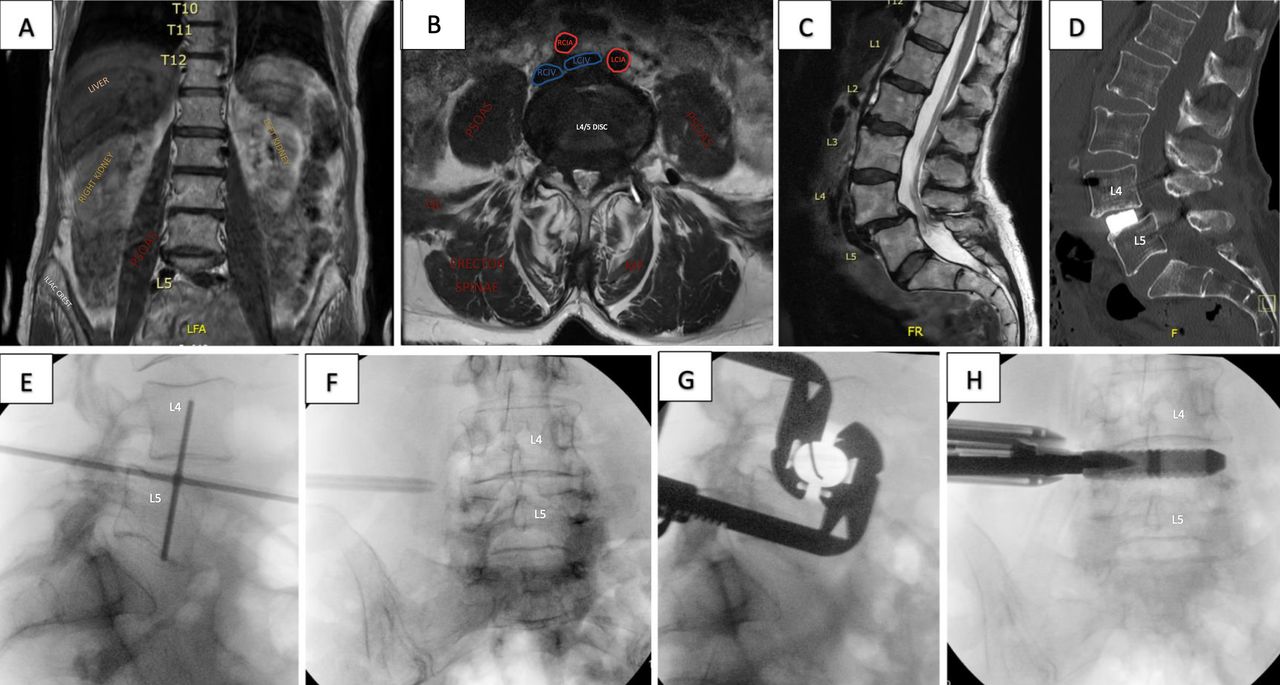
Case Example 2: An 81-year-old woman with a body mass index of 18 presented with severe back pain, neurogenic claudication symptoms, and intermittent bilateral lower limb paresthesia on a background of rheumatoid arthritis. Preoperative magnetic resonance imaging coronal (A) with visceral structures, axial (B) with canal stenosis, psoas and vascular anatomy, and sagittal (C) with grade 1 anterolisthesis of L4/5 highlights approachability from either side of the spine. She underwent an uncomplicated right-sided L4/5 prone lateral interbody fusion with posterior percutaneous pedicle screws. Postoperative sagittal (D) with realignment at L4/5 and final implant position. Intraoperative radiography (E–H) showing fluoroscopy targeting, through 2-blade retractor system. RCIA, right common iliac artery; LCIA, left common iliac artery; RCIV, right common iliac vein; LCIV, left common iliac vein; MF, multifidus; QL, quadratus lumborum.
- Figure 3
Case Example 3: A 78-year-old woman presented with severe back pain limiting mobility, neurogenic claudication symptoms, and L4 radiculopathy with imaging findings of degenerative scoliosis. EOS images preoperatively (A) with sagittal vertical axis (SVA) of 55 mm, lumbar lordosis of 31°, and postoperatively (B) with SVA of 8 mm, lumbar lordosis of 63°. Preoperative axial images at L1/2 (C), L2/3 (D), L3/4 (3), and L4/5 (F) with relevant vascular and visceral anatomy. A right-sided approach at the side of the concavity was selected, and she underwent an uncomplicated L1/2, L2/3, L3/4, and L4/5 prone lateral interbody fusion with L1 to L5 posterior percutaneous pedicle screws and L2 to L4 decompression. IVC, inferior vena cava; AA, abdominal aorta.
- Figure 4
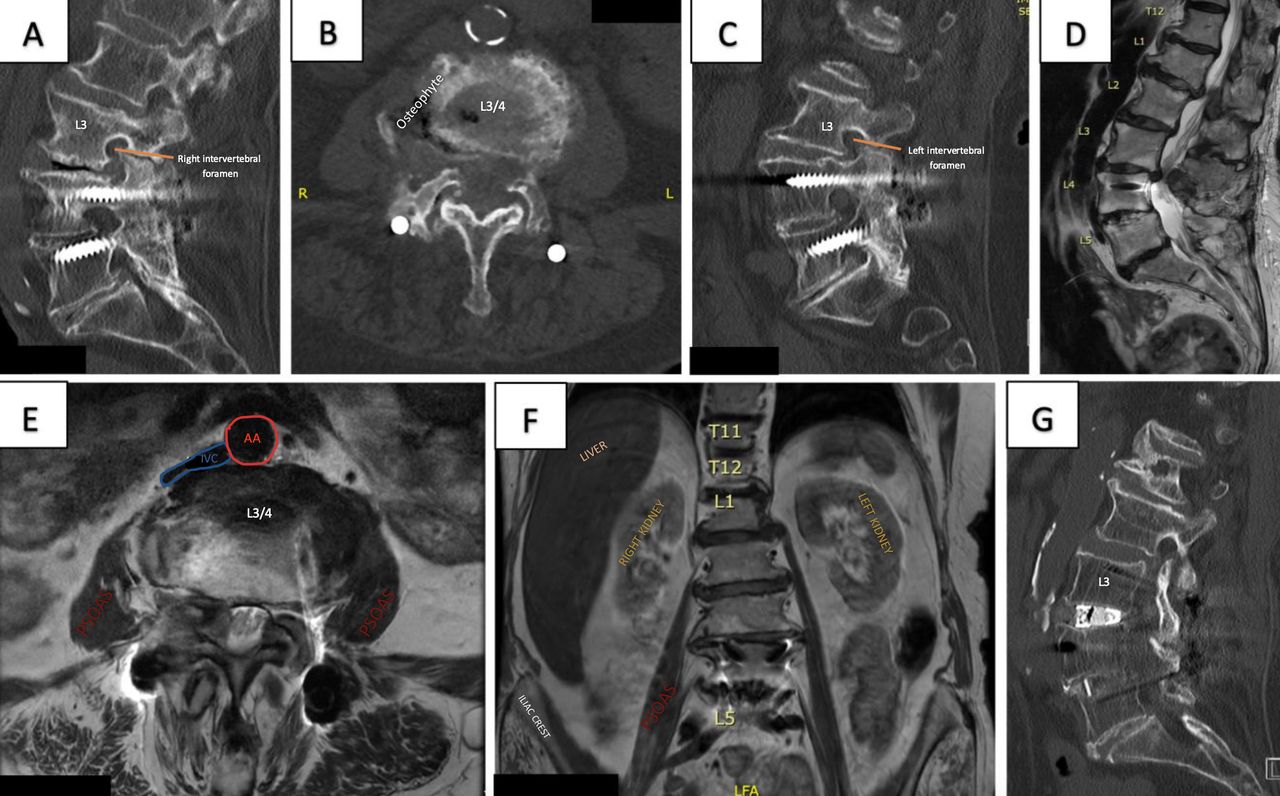
Case Example 4: An 86-year-old woman presented with severe lower limb pain and claudication due to spinal stenosis at L3/4 and adjacent segment disease on the background of an L4/5 posterior lumbar interbody fusion. Preoperative computed tomography L-spine sagittal (A) of vacuum phenomena of L3/4 disc space and right intervertebral foramen, axial (B) at L3/4 with a right-sided osteophyte complex, and sagittal (C) left intervertebral foramen. Preoperative magnetic resonance images are sagittal (D), axial at L3/4 disc and right-sided unilateral stenosis (E), and coronal (F). A left-sided approach was chosen, contralateral to the osteophyte, for ease of access and hepatomegaly evident on the right. She underwent an uncomplicated left L3/4 prone lateral interbody fusion with the extension of L4/5 posterior fusion and L3/4 laminectomy. IVC, inferior vena cava; AA, abdominal aorta.
- Figure 5
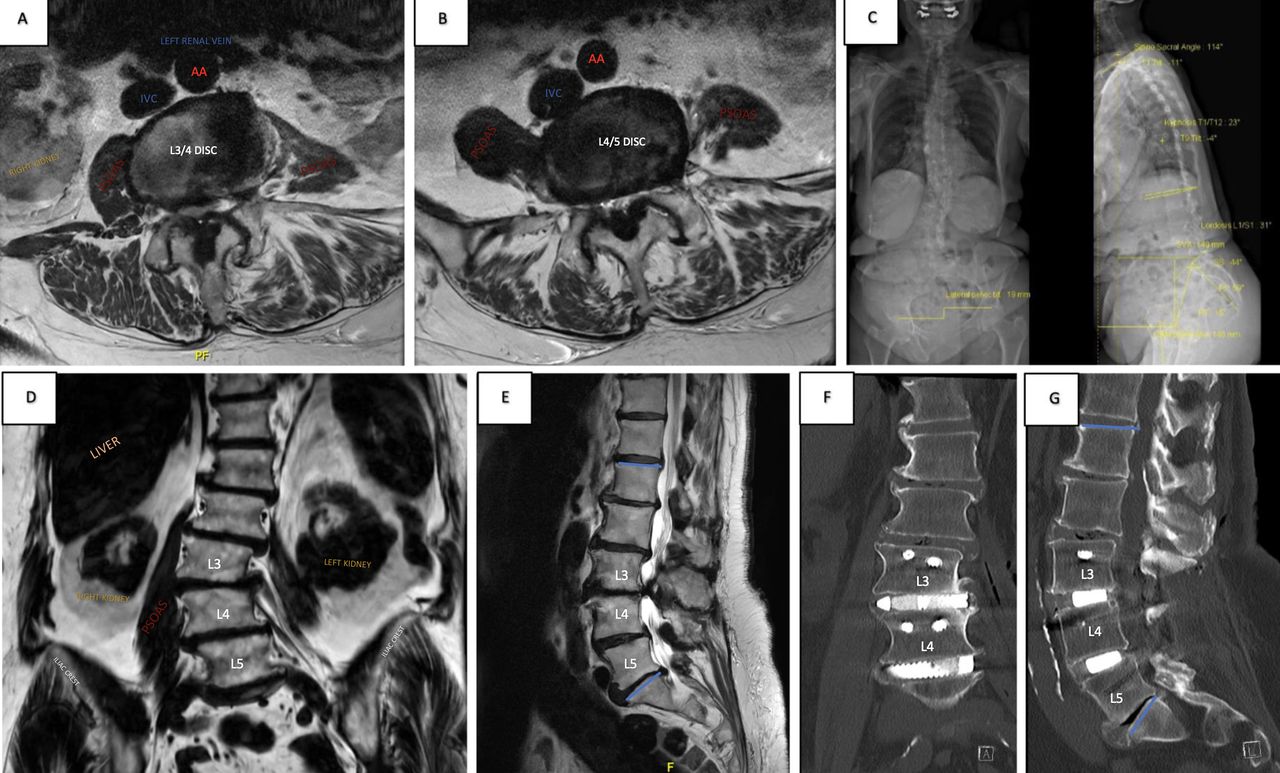
Case Example 5: An 83-year-old woman presented with neurogenic claudication, bilateral lower limb paresthesia, and difficulty walking in an upright posture. Preoperative magnetic resonance imaging axial L3/4 (A) with severe canal stenosis and axial L4/5 (B), coronal (D) with asymmetry of psoas and scoliosis convex right and sagittal (E). EOS (C) with sagittal vertical axis 149 mm. A left-sided approach was selected due to concavity to the left, plus the right psoas location is more anterior to the disc space at L4/5. She underwent a left-sided L3/4 and L4/5 prone lateral interbody fusion with L3 to L5 posterior percutaneous pedicle screws and L3 to L5 laminectomy. Postoperative computed tomography L-spine of coronal (F) and sagittal (G) with final implant positions. IVC, inferior vena cava: AA, abdominal aorta.
- Figure 6
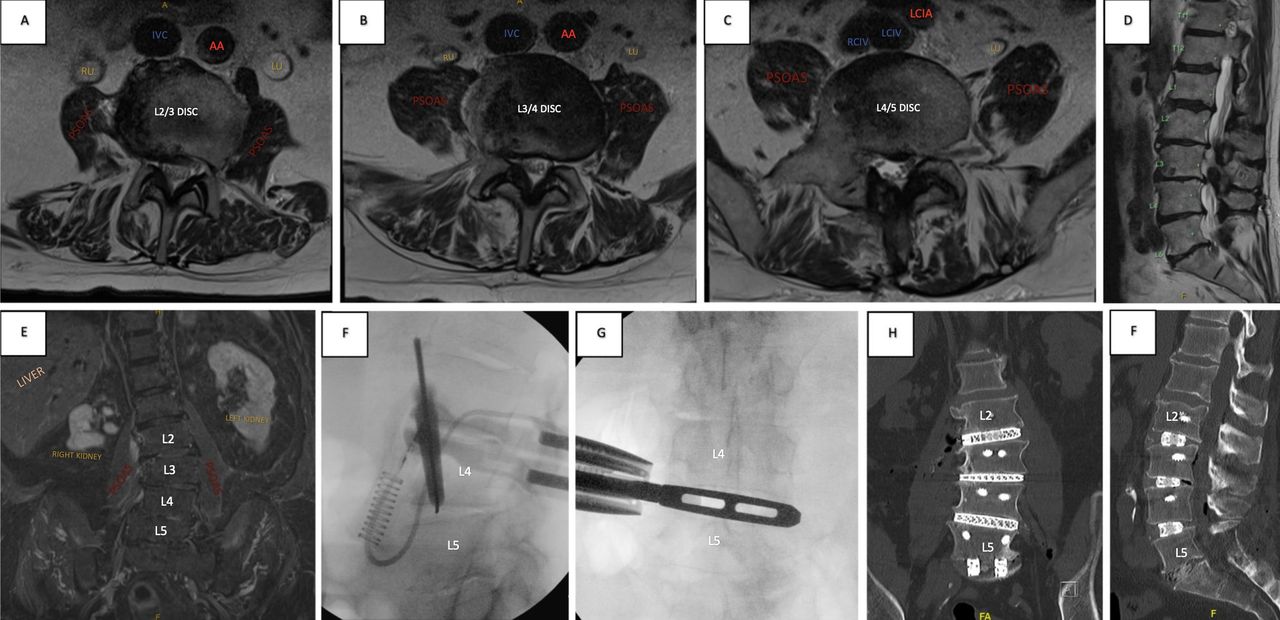
Case Example 6: A 74-year-old man presented with significant lower back pain, limiting mobility on a background of renal impairment and cardiac issues. His imaging showed degenerative scoliosis and loss of lumbar lordosis. Preoperative axial L2/3 (A), L3/4 (B), L4/5 (C), sagittal (D), and coronal (E) with scoliosis convex left and kidney abnormalities. After medical work-up and preoperative optimization, a right-sided approach was chosen due to coronal concavity to the right. He underwent a right-sided L2/3, L3/4, and L4/5 prone lateral interbody fusion plus L5/S1 posterior lumbar interbody fusion with L2 to S1 posterior pedicle screws and S2-iliac screws. Intraoperative radiography shows fluoroscopic targeting of L4/5 (F) and trialing (G) prior to other rostral levels. Postoperative coronal (H) and sagittal (I) with final implant positions through a single incision right-sided approach for L2 to L5 prone lateral fusion. IVC, inferior vena cava; AA, abdominal aorta; RU, right ureter; LU, left ureter; LCIA, left common iliac artery; RCIV, right common iliac vein; LCIV, left common iliac vein.
- Figure 7
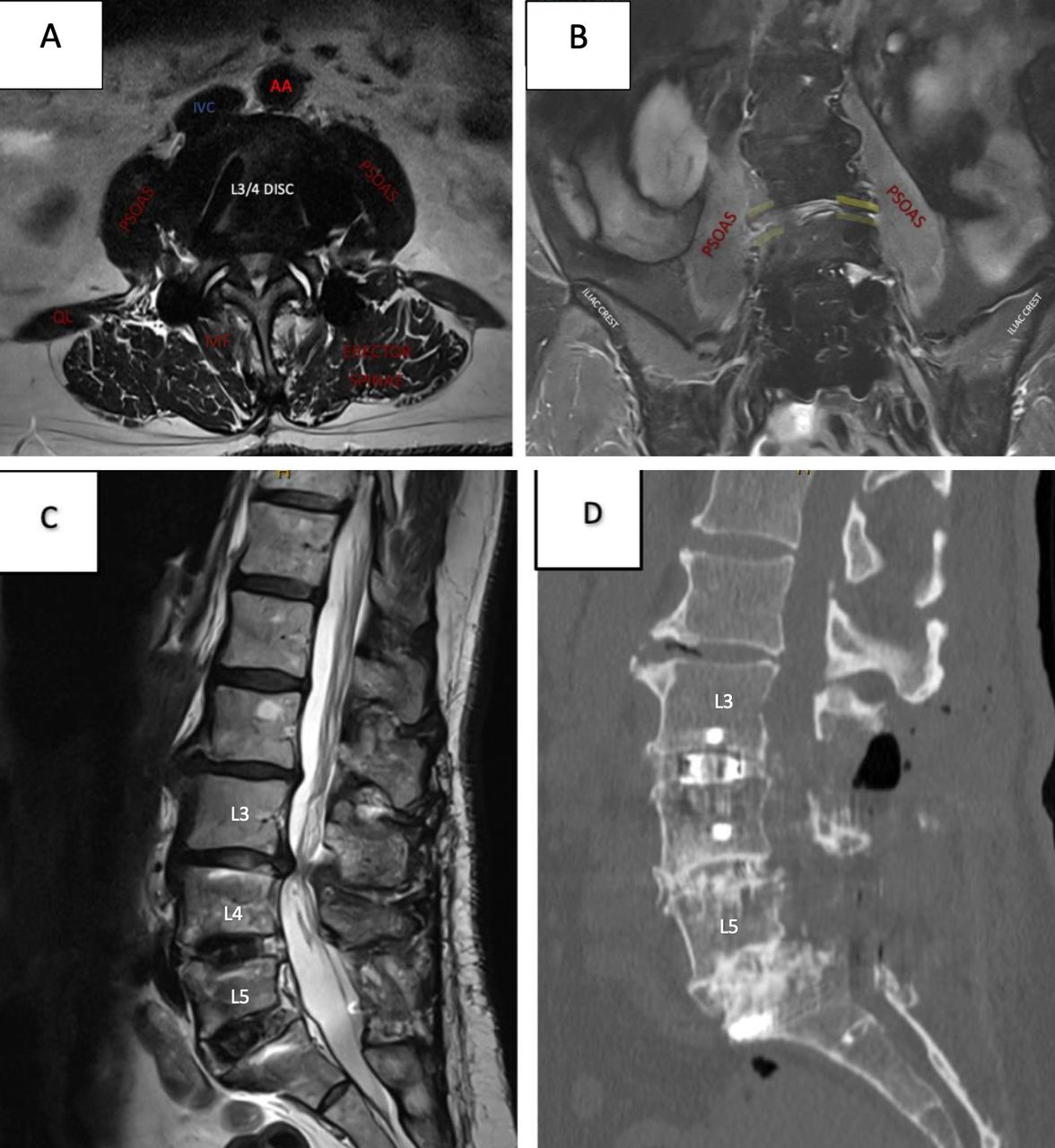
Case Example 7: A 78-year-old woman presented with claudication symptoms secondary to adjacent segment disease on a background of L4/5 and L5/S1 interbody fusion. Preoperative axial at L3/4 (A) with severe canal stenosis and vascular, visceral and psoas anatomy, coronal (B) highlighting left-sided collapse, and sagittal (C) with canal stenosis and previous fusion. A right-sided approach was chosen for ease of access at disc space given overhang and collapse on the left. The patient underwent an uncomplicated right-sided L3/4 prone lateral interbody fusion with lateral plate and L3/4 laminectomy. Postoperative sagittal (D) with final implant position. IVC, inferior vena cava; AA, abdominal aorta; MF, multifidus; QL, quadratus lumborum.







In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.