


Abstract
Background Despite the known association between higher estimated blood loss (EBL) and suboptimal outcomes, the threshold of EBL that negatively impacts outcomes following elective spine surgery remains unknown. In an open 2- and 3-level posterolateral lumbar fusion, we sought to find a threshold of surgeon-reported EBL associated with length of stay (LOS), 30-day complications, and patient-reported outcomes (PROs).
Methods A single-center, retrospective cohort study was performed for 2- and 3-level open posterolateral lumbar fusions between October 2010 and April 2021. Surgeon-reported EBL (milliliters) was the primary independent variable for predicting LOS (days). Secondary outcomes included 30-day complications and PROs as the minimal clinically important difference (MCID). Multivariable regression and receiver operating characteristic curve with Youden’s Index were calculated.
Results 2-Level Fusion: A total of 557 patients underwent 2-level fusions. Multivariable regression found EBL to be a significant risk factor for prolonged LOS. A threshold of 375 mL was associated with LOS beyond postoperative day 2 (POD2) (area under the curve [AUC] = 0.64, 95% CI 0.58–0.70, P < 0.001). 3-Level Fusion: A total of 287 patients underwent 3-level fusions. Similarly, EBL was a significant risk factor for prolonged LOS, with a threshold of 675 mL to predict LOS beyond POD2 (AUC = 0.63, 95% CI 0.54–0.73, P = 0.012). EBL was associated with increased odds of 30-day complications, with a threshold of 538 mL (AUC = 0.63, 95% CI 0.51–0.76, P < 0.001). For both 2- and 3-level fusions, EBL was not significantly associated with MCID for any of the PROs.
Conclusions In patients undergoing open, posterolateral lumbar fusions, surgeon-reported EBL thresholds at 375 mL for 2-level fusions and 675 mL for 3-level fusions were moderately associated with LOS beyond POD2. In 3-level lumbar fusions, EBL above 538 mL showed a potential association with an increased odds of 30-day complications.
Clinical Relevance Surgeons should improve their ability to manage blood loss and implement methods to keep EBL below the provided thresholds to decrease LOS and minimize the risk of complications.
Level of Evidence 3.
Introduction
Spinal fusion procedures have seen a dramatic rise in volume across the world, especially in countries with an aging population.1 From 2002 to 2014, the number of elective lumbar fusions for degenerative spine disease in the United States increased by 276%.2 Intraoperative blood loss can exceed 1 to 2 L in select studies of elective lumbar fusions.3,4 Significant blood loss can trigger disseminated intravascular coagulation or other coagulopathies, which can lead to a postoperative hematoma, hypotension, neurologic deficit, and infection.5,6 In other cardiac and general surgery procedures, intraoperative estimated blood loss (EBL) of greater than 500 mL has been associated with increased postoperative morbidity and mortality.7,8 Prior spine studies have also investigated the association of intraoperative transfusions and increased operative time, with potential subsequent transfusion-related lung injury, volume overload, and hemolytic reactions.9 While a portion of the overall blood loss is at the surgeon’s discretion, many other factors are involved, such as surgical technique, operative time, complexity of surgery, use of hemostatic agents, surgical assistants, mean arterial pressures, temperatures, and anesthetic protocols.
To optimize outcomes after lumbar fusion surgery, a great deal of attention has been given toward reducing blood loss.4,10 Recent studies have cited the use of tranexamic acid to minimize blood loss with good results. Moreover, the introduction of cell salvage that recycles patient’s intraoperative blood has reduced effective blood loss. EBL greater than 500 mL in multilevel lumbar fusion was found to be an independent risk factor associated with prolonged length of stay (LOS) and increased postoperative complications.11,12
Though the association of higher blood loss and worse outcomes after spine surgery has been established, the exact amount of how much blood loss is too much remains unknown. Additionally, the impact of EBL on patient-reported outcomes (PROs) has not been fully investigated. In a cohort of patients undergoing elective, 2- to 3-level, open, posterolateral lumbar fusion, the current objectives were to find EBL threshold associated with the following outcomes: (1) LOS, (2) 30-day complications, and (3) 3-month PROs.
Methods
Study Design
A retrospective cohort study was undertaken using prospectively collected data from our institution’s spine outcomes registry. The registry includes all patients who underwent elective spine surgery and has been in existence since 2011. The registry team includes 3 full-time employees responsible for contacting patients to collect PRO data at scheduled pre- and postoperative timepoints. Approximately, 12 fellowship-trained neurosurgery and orthopedic spine surgeons have contributed patients in the decade of the registry’s existence. Institutional review board approval was obtained for this study (institutional review board no. 211290).
Patient Population
Registry data were obtained for patients who underwent elective, open, 2- or 3-level posterior lumbar fusion between 10 October 2010 and 4 April 2021 for degenerative reasons. Inclusion criteria were age ≥18 years old and a signed consent for participation. All tubular minimally invasive lumbar fusion surgeries were excluded. Anterior and lateral lumbar interbody fusions were also excluded. Postoperative care was standardized for all patients, who were admitted to similar spine floors, with similar postoperative management, consisting of multimodal pain management and daily physical therapy evaluations.
Independent Variables
EBL measured in milliliters was the primary independent variable of interest. In keeping with prior literature,13 the visual estimation method of the postoperative blood volume in the canister was used to assess for blood loss, which was determined after surgery conjointly by the surgeon and the anesthesiologist. Intraoperative blood draws were also accounted for and added to the total EBL. Whenever intraoperative lab values were available, the intraoperative hemoglobin level was compared with preoperative values to aid in the final EBL quantification. Other independent variables included patient demographics, comorbidities, and perioperative data. These variables included age, gender, body mass index, ambulatory status, symptom duration, employment status, intent to return to work, revision vs primary surgery, indication for revision, diagnosis, preoperative antiplatelet use, and smoking status. Operative and perioperative variables included operation performed, operative time (minutes), and discharge disposition (home vs facility).
Outcomes
Outcomes of interest were: (1) LOS, (2) 30-day complications, and (3) 3-month PROs. LOS was treated as both a continuous variable as well as a dichotomized variable beyond the postoperative day (POD) that achieved the highest area under the curve (AUC) when associated with EBL. Complications were defined as any major/minor complications within 30 days.14 PROs included: (1) Numerical Rating Scale (NRS) back pain, (2) NRS leg pain, and (3) Oswestry Disability Index (ODI). PROs were prospectively collected over the phone or via email before surgery and 3 months postoperatively. Patients with preoperative NRS back pain/leg pain values of 0 were excluded from the minimal clinically important difference (MCID) analysis.
Statistical Analysis
Descriptive statistics were compiled for all demographic, preoperative, and postoperative characteristics. Mean and SD for continuous variables and frequency for categorical variables were computed. Continuous data were compared using Student t tests. MCID was defined as a 30% improvement over baseline PROs at 3 months following surgery.15,16 Due to the multifactorial nature of LOS, complications, and PROs, multivariable regressions were performed assessing EBL per 100 mL as the primary independent variable in addition to the following covariates: age at surgery, gender, revision surgery, preoperative ODI, and presence of comorbidities. Multivariable linear regression was performed for EBL as a predictor of LOS, while multivariable logistic regression models were created to assess predictors of 30-day complications and achievement of MCID. Receiver operating characteristic (ROC) curve analysis was performed to determine whether EBL was a good binary classifier of outcomes. Sensitivity, specificity, AUC, and Youden’s Index were also analyzed. AUC values <0.60 were determined to be poor, and for these, no Youden’s Index was calculated due to lack of clinical meaning. The validated 25th centile approach described by Tubach et al17 was used to cross-reference the cutoff value calculated by the Youden’s Index to provide a range of values within our sample. A P value <0.05 was considered statistically significant. The analysis was performed using SPSS version 22 (IBM Inc., Chicago, Illinois) and R Statistical Software version 4.0.3 (https://www.r-project.org/).
Results
Part I: 2-Level Lumbar Fusion
Perioperative Patient Demographics
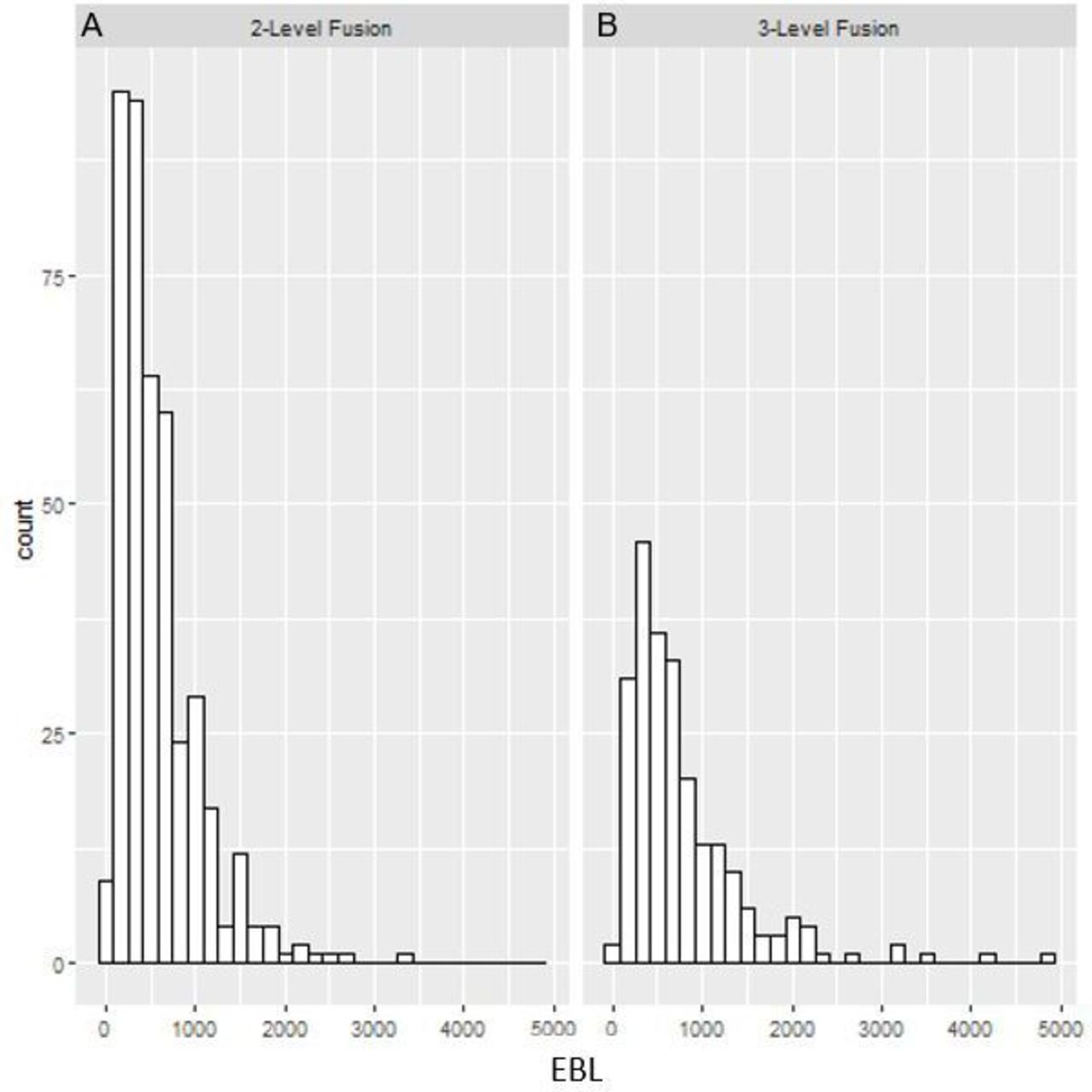
A total of 557 patients underwent elective, open, posterior 2-level lumbar fusion. Mean age was 61.7 ± 12.0 years, and 277 (50%) patients were men. Mean intraoperative EBL was 583.0 ± 447.5 mL. A total of 178 patients had also interbody fusion. Detailed patient demographics, comorbidities, and preoperative characteristics are summarized in Tables 1 and 2. EBL distribution is shown in Figure 1A.
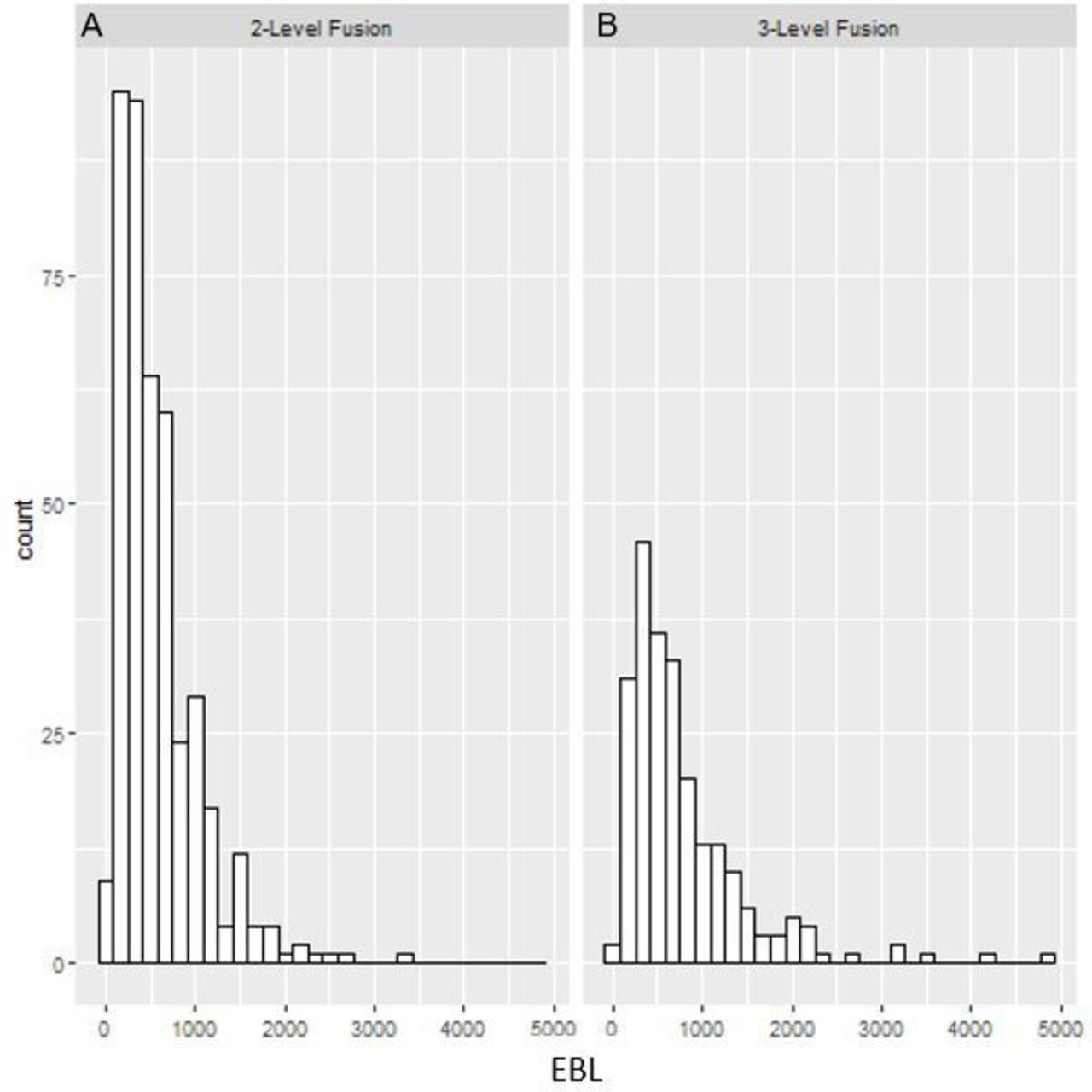
Histogram showing the distribution of estimated blood loss (EBL) in milliliters in patients with 2-level (A) and 3-level (B) posterolateral lumbar fusion, with and without interbody fusion.
Demographic characteristics of patients receiving 2- and 3-level posterolateral lumbar fusion.
Operative and perioperative variables of patients receiving 2- and 3-level posterolateral lumbar fusion.
EBL Association With LOS
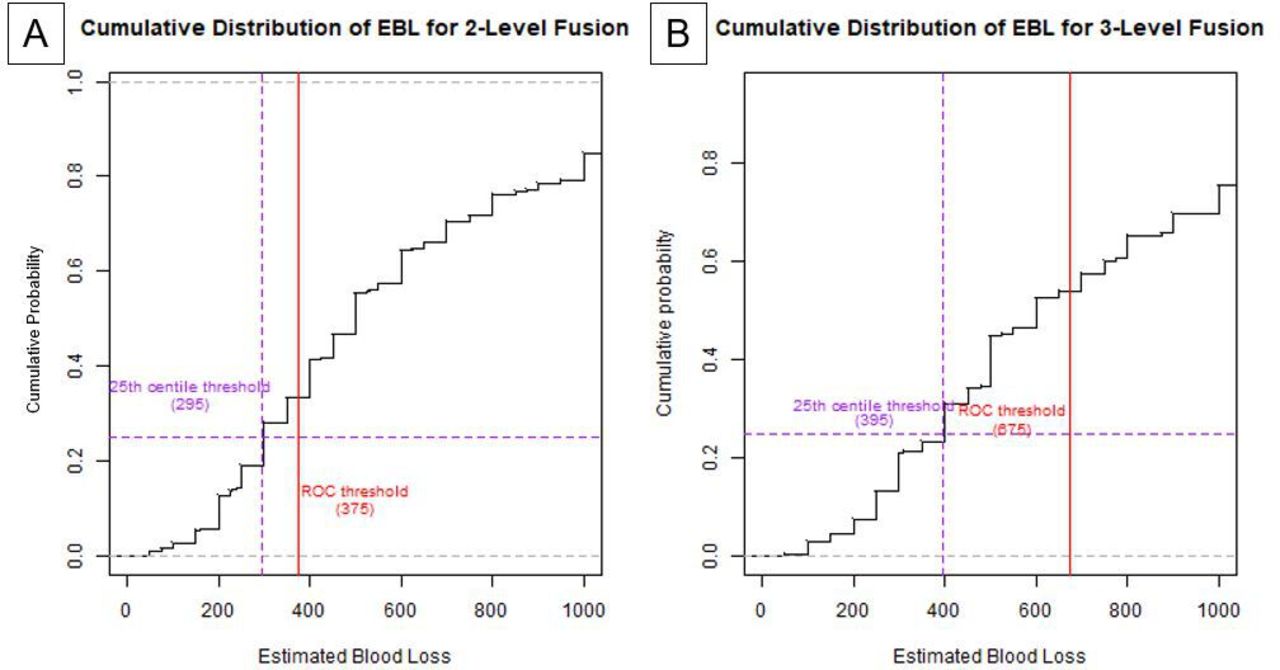
The average LOS for 2-level spinal fusion was 3.4 ± 1.8 days. A multivariable linear regression controlling for age at surgery, gender, revision surgery, preoperative ODI, and presence of comorbidities as covariates showed that EBL was significantly associated with LOS (β = 0.09, 95% CI 0.06–0.13, P < 0.001). ROC analysis of EBL as a predictor of LOS beyond POD2 demonstrated moderate predictive value (AUC = 0.64, 95% CI 0.58–0.70, P < 0.001). The corresponding Youden’s Index calculation optimally differentiated EBL at 375 mL (Figure 2A). Youden’s Index and the 25th centile EBL threshold are compared in the cumulative distribution graph of LOS (Figure 3A).
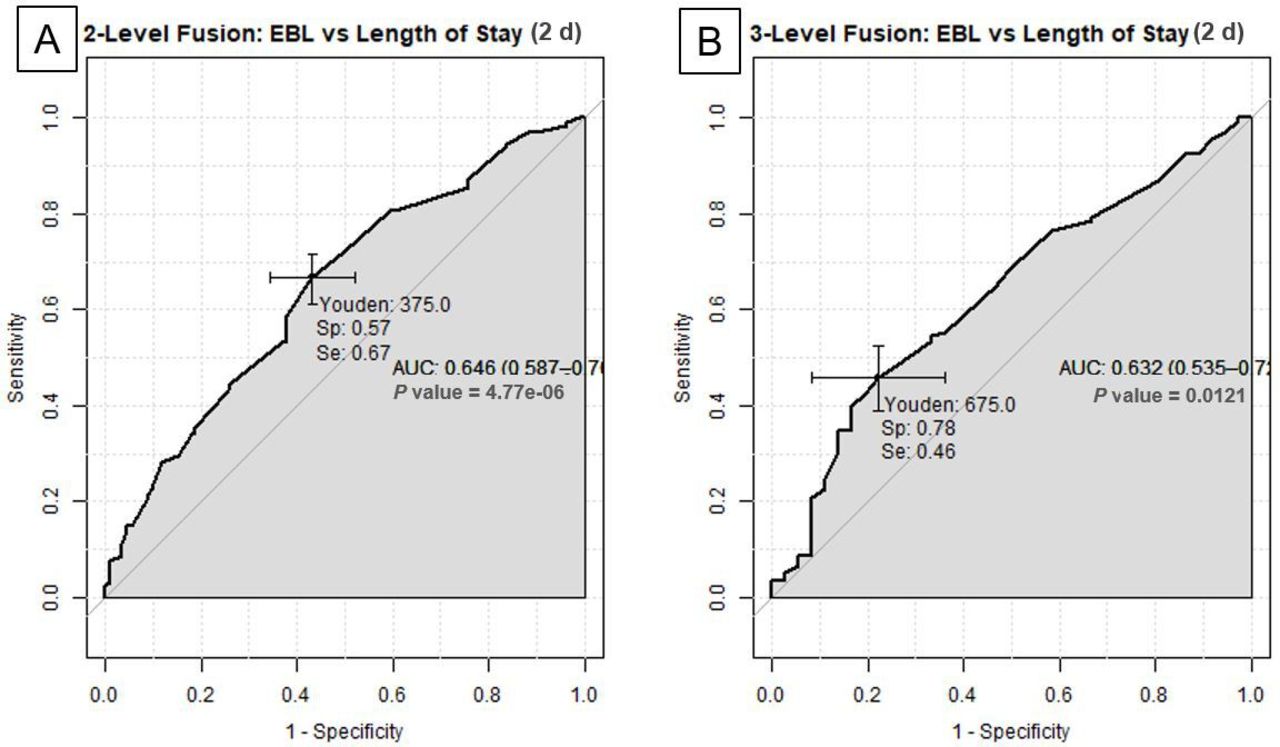
Receiver operating characteristic curves of estimated blood loss (EBL) vs length of stay in 2-level (A) and 3-level (B) posterolateral lumbar fusion. AUC, area under the curve; Se, sensitivity; Sp, specificity.

Comparison of 25th centile and Youden’s Index of patients with prolonged length of stay (LOS) in 2-level (A) and 3-level (B) posterolateral lumbar fusion. The red vertical lines indicate the calculated Youden’s Index. The purple lines show the 25th centile of patients with prolonged LOS. Estimated blood loss is given in milliliters. ROC, receiver operating characteristic curve.
EBL Association With 30-Day Complications
A total of 43 (7.7%) patients had a complication within 30 days. All medical and surgical complications are summarized in Table 3. Multivariable logistic regression did not show a significant association between EBL and 30-day complication (OR = 1.02, 95% CI = 0.95–1.10, P = 0.481). Likewise, ROC analysis found EBL to be poor, no better than a random discriminator (AUC = 0.50, 95% CI = 0.38–0.61, P < 0.001). No Youden’s Index was calculated in this case.
Medical/surgical complications within 30 d after lumbar spine surgery.
EBL Association With PROs
At 3-month follow-up, 303 (62.3%), 294 (64.8%), and 269 (54.0%) achieved MCID for NRS back, NRS leg, and ODI, respectively. Multivariable logistic regression showed that EBL was non-predictive for achieving MCID in any of the 3 outcome variables. Likewise, ROC analysis failed to demonstrate a correlation between EBL and MCID of PROs (Table 4). Table 5 provides a tabulated form of preoperative and 3-month PROs. Given the poor ROC analysis, Youden’s Index was not calculated.
Receiver operating characteristic curve analysis of 2- and 3-level posterolateral lumbar fusion with patient-reported outcomes.
Patient-reported outcomes of 2- and 3-level posterolateral lumbar fusion.
Part II: 3-Level Lumbar Fusion
Perioperative Patient Demographics
There were 287 patients who underwent elective, open, 3-level lumbar spinal fusion, and 70 patients underwent interbody fusion. Mean age was 63.7 ± 11.5 years. Mean EBL was 790.3 ± 682.2 mL. Tables 1 and 2 present detailed demographics, comorbidities, and preoperative characteristics. EBL distribution is shown in Figure 1B.
EBL Association With LOS
The average LOS was 4.4 ± 2.6 days for patients with 3-level lumbar fusions. A multivariable linear regression model showed a significant association between EBL and LOS (β = 0.10, 95% CI 0.06–0.16, P < 0.001). Subsequently, ROC analysis of EBL as a predictor of LOS beyond POD2 found moderate predictive value (AUC = 0.63, 95% CI 0.54–0.73, P = 0.012). The corresponding Youden’s Index calculation optimally differentiated EBL at 675 mL (Figure 2B). The 25th percentile EBL determined by the cumulative distribution function was 395 mL (Figure 3B).
EBL Association With 30-Day Complications
There were 33 (11.5%) 30-day complications in the 3-level fusion cohort (Table 3). Multivariable logistic regression showed that EBL was a significant risk factor for 30-day complications (OR = 1.06, 95% CI 1.02–1.12, P = 0.009). For every 100 mL increase in EBL, there was a 6% increase in the odds of developing complications within 30 days. ROC analysis of EBL and complications demonstrated moderate predictive value (AUC = 0.63, 95% CI 0.51–0.76, P < 0.001), with a corresponding Youden’s Index value of 538 mL (Table 4).
EBL Association With PROs
At 3-month follow-up, 172 (66.7%), 181 (74.2%), and 131 (50.0%) achieved MCID for NRS back, NRS leg, and ODI, respectively. Multivariable logistic regression did not find EBL to be predictive of achieving MCID of PROs. Likewise, ROC analysis failed to show EBL as a predictor of achieving MCID (Table 4). Comparison of preoperative and 3-month outcomes is shown in Table 5.
Discussion
The current study sought to evaluate the impact of surgeon-reported EBL on the perioperative outcomes of LOS, complications, and 3-month PROs in patients undergoing elective posterolateral lumbar fusion. For patients undergoing 2-level open lumbar fusion, higher surgeon-reported EBL showed a potential association with longer LOS, with a threshold EBL of 375 mL for LOS beyond POD2. For 3-level open lumbar fusions, higher EBL was an independent risk factor for longer LOS and 30-day complications. The corresponding calculated thresholds were 675 mL for LOS beyond POD2 and 538 mL for 30-day complications. In both cohorts, EBL was not associated with PROs at 3 months. Despite these thought-provoking results, we are careful not to imply causation because these results convey associations. The reasons for extended LOS are multifactorial, and concluding that higher EBL causes increased LOS would be incorrect. That said, it is our hope these threshold values can provide reasonable estimations for EBL in open 2- to 3-level lumbar fusion surgeries.
It has been consistently shown that with higher EBL in spine surgery, one can expect increased complications and longer hospitalizations. Prior studies have defined high EBL arbitrarily as ≥500 mL.11,12 In a cohort of 1168 patients undergoing 1- to 4-level lumbar fusions, Kobayashi et al12 found that EBL ≥500 mL was an independent risk factor for prolonged LOS, defined as >75th percentile of LOS (OR = 1.71, 95% CI 1.07–2.75). They reported average LOS to be 20.8 ± 9.8 days (range, 7–77 days), much longer than that reported in our study. In a similar study design, Huang et al11 attained similar findings; EBL ≥500 mL had longer hospital LOS (<500 mL: 8.6 ± 3.1 days vs ≥500 mL: 9.8 ± 4.9 days, P = 0.045). Our study reported a mean LOS of 3.4 ± 1.8 days and 4.5 ± 2.7 for 2- and 3-level fusions, respectively. The drastically shorter LOS in our study may be attributed to a multitude of factors, including different cultural, institutional, and health care structures at different institutions and across different countries. Nonetheless, the same association between EBL with LOS and complications was shown.
Aside from LOS, studies have also shown increased complication rates with higher blood loss. Cai et al18 evaluated 687 patients undergoing 1- to 2-level lumbar fusions and found lower postoperative hematocrit was strongly associated with higher levels of complications requiring postoperative intensive care unit stay (P < 0.022) and thus prolonged hospital LOS (P < 0.05). Lower hematocrit levels require transfusions, which in itself have been associated with higher postoperative complications across surgical disciplines.9,19–21 Higher EBL and increased complications have been repeatedly demonstrated,22–24 yet a threshold at which EBL is associated with negative outcomes was still not reported. In this study, we found an EBL threshold of 538 mL to be associated with an increased odds of complication associated with 3-level fusions. Perhaps, complications were associated with 3 levels only due to higher hidden blood loss and lower accuracy in EBL.
Though an association was found between EBL and LOS and complications, no such association existed for PROs. It appears that patients’ outcomes are not impacted by EBL, which is encouraging that these outcomes likely affected only the immediate perioperative period. To our knowledge, there have not been any studies that have sought to address the question of intraoperative EBL on PROs in spine surgery, as presented in this current study. Moreover, as stated earlier, the association of EBL with prolonged LOS does not appear to be causal, as longer-term PROs were not affected.
By providing EBL thresholds for 2- and 3-level lumbar fusions, we believe these results can improve surgeons’ ability to manage blood loss intraoperatively. Most studies have arbitrarily chosen a dichotomized cutoff of 500 mL and found >500 mL to be an independent risk factor for prolonged LOS.11,12 Moreover, most studies of EBL and spine surgery include heterogenous populations. For instance, Kobayashi et al12 included patients with 1- to 4-level fusion, with only 25% representing 2 levels or more. Additionally, minimally invasive and open surgeries are not always analyzed separately.25 On the other hand, studies with reported EBL on specific populations have not included thresholds.26 Given the copious literature suggesting higher EBL increase LOS and the incidence of complications, an EBL threshold remains elusive. Providing such a threshold can guide census planning by hospital staff. When predicting the presumed LOS and resource allocation, payers and hospitals can appropriately arrange for an expected duration of hospitalization.
This study, however, is not without limitations. First, we dichotomized a continuous variable of EBL, which may be oversimplifying a complex association. Association does not imply causation, and we conceded that many factors contributed to LOS, not just EBL; factors such as individual surgeon preferences, hospital policies, and availability of personal transportation all come into play. Second, there may be discrepancies in reporting EBL by the surgeon or the anesthesiologist. Previous studies have utilized postoperative hematocrit, yet this was not utilized in our prospective registry. Third, hidden blood loss emerged as a potential intervening factor when measuring total blood loss27,28; however, intraoperative transfusion, cell salvage, and postoperative drain measurements were not provided in our prospective registry but were most often accounted for postoperatively. Moreover, blood loss in the gauzes was not accounted for, which is usually estimated using the gauze visual analog scale as reported by prior studies.29 While EBL might have been subject to minor inaccuracy, we believe that a few milliliters would unlikely impact our findings. Fourth, this study was conducted from a multisurgeon single-center registry, which may affect generalizability of the results. This registry spans nearly a decade, and the analysis does not factor in changes in technology or perioperative management that may have occurred over the years.
Conclusion
In a cohort of patients undergoing 2- and 3-level posterior lumbar fusion, we found that surgeon-reported EBL was independently associated with prolonged hospital LOS. Though we had mediocre AUCs, EBL may predict LOS beyond POD2 at the following thresholds: 375 mL for 2-level fusions and 675 mL for 3-level fusions. In the 3-level fusion cohort, EBL above 538 mL showed a potential association with a higher 30-day complication risk. EBL showed no association with short-term PROs in either cohort. By providing EBL thresholds, surgeons may improve their ability to manage blood loss and employ methods to keep EBL below these thresholds.
Acknowledgments
We thank the employees of Vanderbilt Spine Outcomes Lab for providing the registry data.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Byron Stephens has received consulting fees from Depuy-Synthes and institutional research support from Stryker Spine. Amir Abtahi received institutional research support from Stryker Spine. For the remaining authors, no conflicts of interest were declared.
Ethics Approval Institutional review board approval was obtained for this study (IRB#211290).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.