


Article Figures & Data
Figures
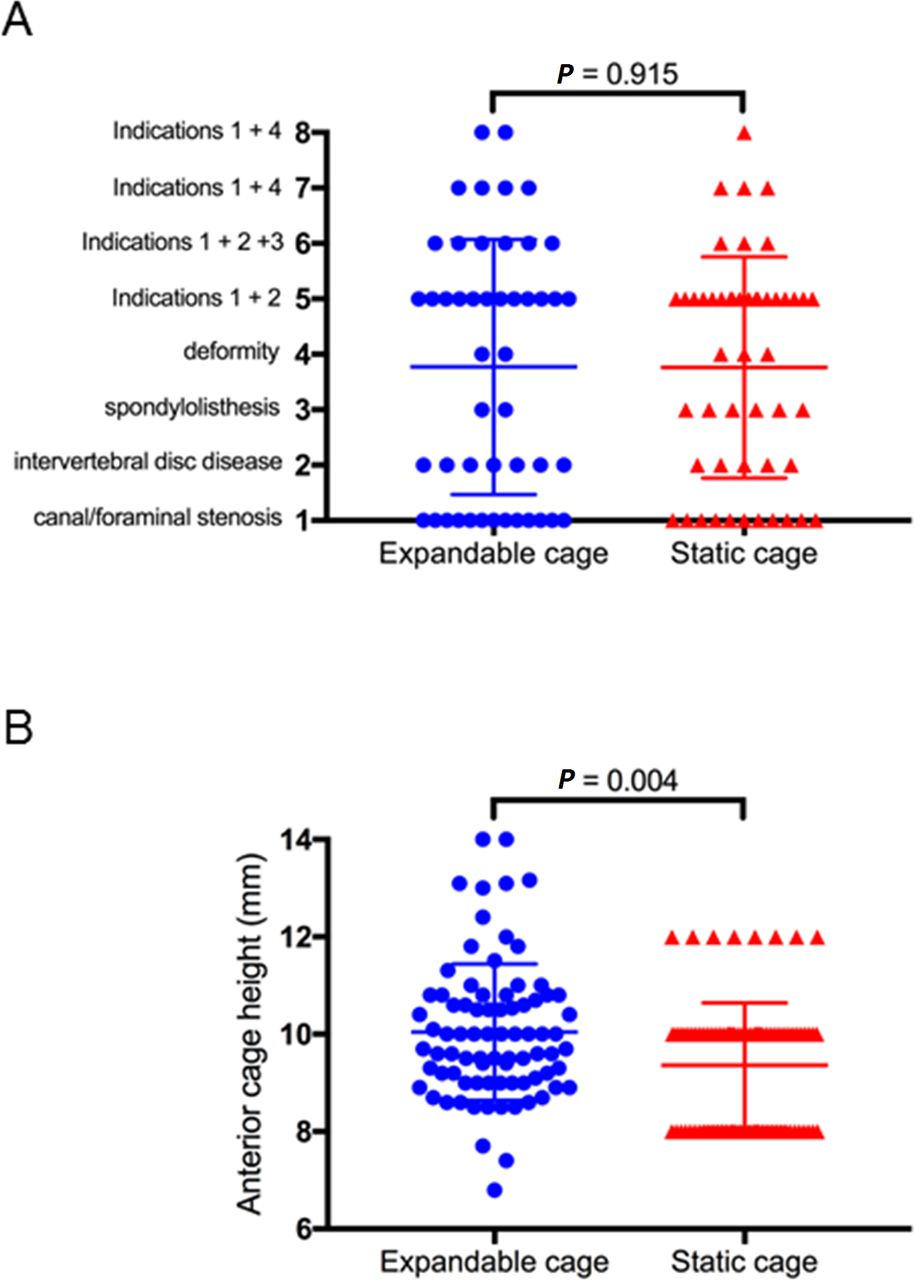
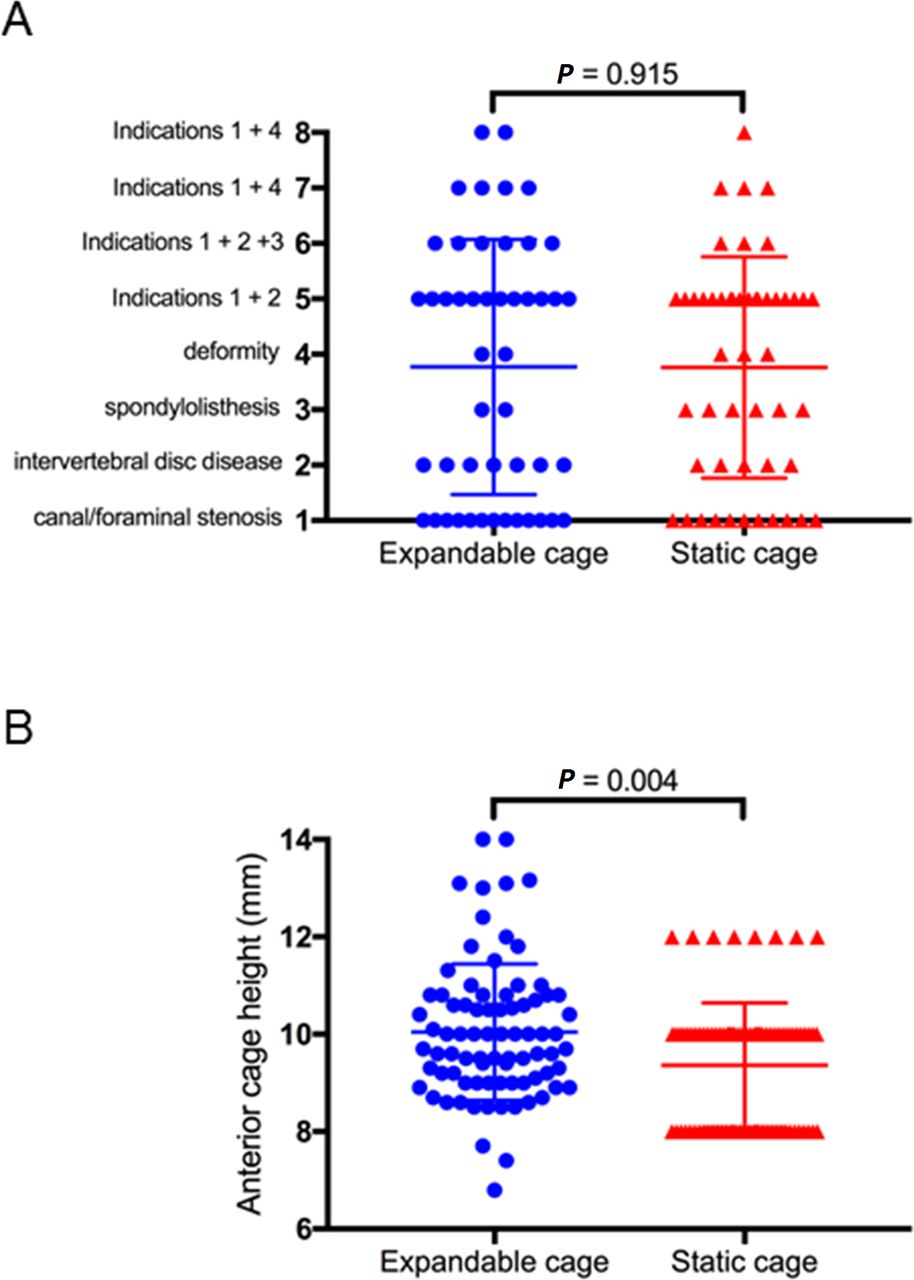
- Figure 1
Surgical indications and cage heights. (A) Numerical numbers were assigned to different pathologies as shown, for which the operations were performed in each study group. (B) Postoperative anterior cage height was measured in millimeters for each study group. Error bar indicates standard error of the mean.
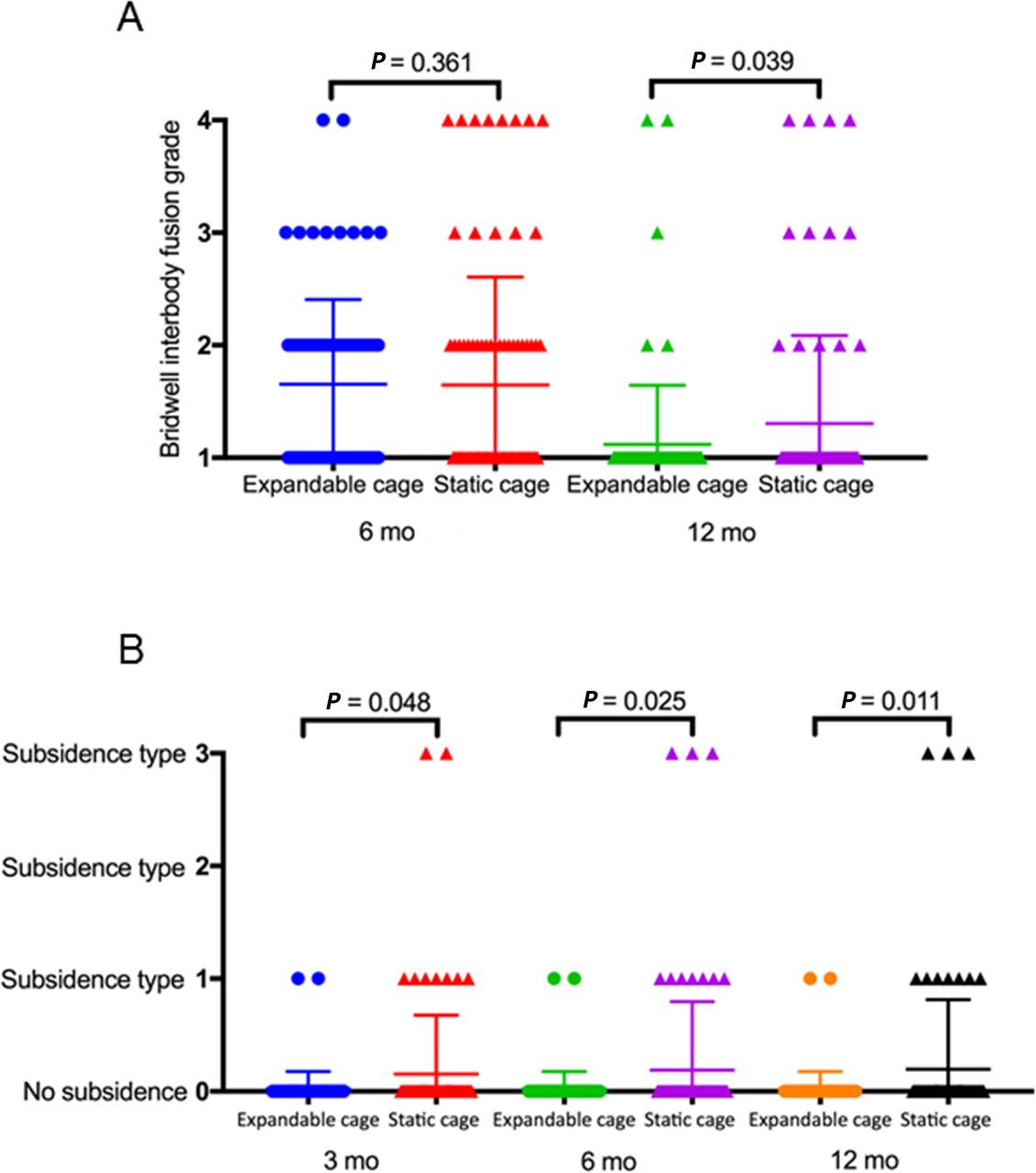
- Figure 2
Fusion and subsidence rates. (A) Fusion grade as assessed by the Bridwell interbody fusion grading system was measured for each study group at 6 and 12 mo postoperatively. (B) The occurrence and type of subsidence were recorded for each study group at 3, 6, and 12 mo postoperatively. Error bar indicates standard error of the mean.

Tables
Inclusion Criteria Exclusion Criteria Adult patients (≥18 y old)
Symptomatic degenerative lumbar spondylolisthesis unresponsive to conservative management for at least 6 mo
Undergoing lateral lumbar interbody fusion
Patients with active infection or malignancy
Significant osteoporosis
Previous lumbar spine surgery
Previous spinal trauma
Drive screw revolutions 0 2 4 6 8 10 12 14 Anterior height, mm 7 8 9 10 11 12 13 14 Posterior height, mm 6.0 6.5 6.9 7.4 7.9 8.3 8.8 9.3 Lordotic angle 3° 4.7° 6.4° 8.1° 9.8° 11.5° 13.2° 15° Source: Globus Medical Inc.
Radiographic Parameters Definition Fusion status The Bridwell interbody fusion grading system:
Grade 1: fused with remodeling and trabeculae present
Grade 2: graft intact, not fully remodeled and incorporated, but no lucency present
Grade 3: graft intact, potential lucency present at top and bottom of the graft
Grade 4: fusion absent with collapse/resorption of graftSubsidence Loss of disc height by >2 mm compared with 6-wk postoperative disc height, as measured from the vertebral endplate to the caudal or cranial margin of the cage Subsidence type Type 1: cage subsidence into the contralateral caudal endplate without anterior cage tilt
Type 2: bilateral cage subsidence into the anterior aspect of the caudal endplate, producing an anterior tilt of the cage
Type 3: cage subsidence into both the caudal and cranial endplates bilaterally without cage tiltIndex-level segmental lordosis The angle between the inferior endplate of the caudal vertebral body to the superior endplate of the cephalad vertebral body of the fusion segment Anterior disc height The distance at the most anterior point of the vertebral body from endplate to endplate Posterior disc height The distance at the most posterior point of the vertebral body from endplate to endplate, as a surrogate marker for foraminal height Characteristic Expandable Cage
(n = 48)Static Cage
(n = 50)P Value Patient Demographics Age, y, mean (range, SD) 71.2 (43–84, 8.5) 67.2 (27–89, 13.2) 0.143 Sex, n (%) 0.838 Men 21 (43.8) 25 (50.0) Women 27 (56.2) 25 (50.0) Body mass index, mean (range, SD) 28.7 (18–39, 4.3) 28.5 (18–46, 5.5) 0.567 Current smoker, n (%) 0.618 Yes 0 3 (6.0) No 45 (93.8) 44 (88.0) Unknown 3 (6.2) 3 (6.0) Operative Characteristics Operated spinal segments n (%) >0.999 Single level 35 (52.0) 34 (56.0) 2 Levels 10 (36.0) 12 (28.0) 3 Levels or more 3 (12.0) 4 (16.0) Treated lumbar segments, n (%) 0.308 L1-L2 7 (9.3) 5 (7.3) L2-L3 18 (27.9) 15 (24.4) L3-L4 28 (41.9) 22 (34.1) L4-L5 13 (20.9) 27 (34.1) Radiographic Parameters Preoperative disc height, mm, mean (range, SD) Anterior 6.0 (1–11.5, 2.5) 6.4 (1–19.2, 3.4) 0.251 Posterior 3.4 (1–5.9, 1.1) 3.3 (1–7.0, 1.5) 0.834 Postoperative disc height, mm, mean (range, SD) Anterior a 10.0 (6.8–14.0, 1.8) 9.4 (8–12, 2.3) 0.004 Posterior 5.8 (3–8.5, 1.1) 5.3 (1.1–9.2, 1.4) 0.121 % Increase in disc height postoperative, mean (range, SD) Anterior disc height 242.8 (99–1180, 178.6) 238.9 (69.5–1130, 230.8) 0.114 Posterior disc height 193.5 (89.7–541.7, 91.06) 203.6 (56.9–650, 140.4) 0.266 Postoperative change in segmental lordosis degrees, mean (range, SD) 3.6 (−3.6 to 19.2, 4.2) 3.3 (−8.4 to 14.6, 4.2) 0.947 ↵a Refers to expanded final height in the expandable cage group, whereas static cages were of 8, 10, or 12 mm in height. Total levels decompressed for the expandable group: 84; for the static group: 85.
Study Arm Changesa in ODI (%): Mean (Range, SD) 3 mo 6 mo 12 mo Expandable cage −14.61 (−48 to 28, 14.5) −19.03 (−58 to 4, 14.6) −20.81 (−60 to 8, 16.6) Static cage −10.41 (−28 to 16, 16.5) −16.21 (−52 to 14, 19.5) −20.24 (−58 to 42, 22.1) P value 0.289 0.541 0.894 Changesa in VAS—Back: Mean (Range, SD) 3 mo 6 mo 12 mo Expandable cage −4.46 (−9 to 2, 2.7) −4.65 (−9 to 0, 3.0) −5.20 (−10 to 6, 3.3) Static cage −2.5 (−9 to 2, 2.8) −3.71 (−9 to 1, 2.7) −3.32 (−9 to 5, 3.4) P value 0.006 0.231 0.062 Changesa in VAS—Both Legs Combined: Mean (Range, SD) 3 mo 6 mo 12 mo Expandable cage −6.70 (−18 to 9, 6.8) −6.22 (−17 to 4, 5.5) −6.76 (−18 to 4, 4.6) Static cage −5.46 (−13 to 1, 3.9) −5.55 (−13 to 2, 4.3) −4.27 (−14 to 9, 5.1) P value 0.447 0.654 0.023 Changes*a in SF-12 (PCS): Mean (Range, SD) 3 mo 6 mo 12 mo Expandable cage 7.46 (−34.2 to 29.3, 10.2) 13.24 (−13.1 to 38.9, 10.0) 10.39 (−27.8 to 37.9, 14.6) Static cage 7.12 (−3.4 to 21.2, 7.0) 5.80 (−25.7 to 22, 12.5) 12.68 (−7.4 to 37, 10.7) P value 0.624 0.035 0.988 Changesa in SF-12 (MCS): Mean (Range, SD) 3 mo 6 mo 12 mo Expandable cage 4.54 (−63.6 to 22.41, 14.1) 4.13 (−47.3 to 28.6, 14.1) 6.24 (−28.9 to 28.6, 13.4) Static cage −0.72 (−26.1 to 22.7, 10.6) 2.75 (−67.1 to 20.0, 20.3) 3.08 (−23 to 38.0, 13.2) P value 0.009 0.026 0.273 ↵a The value of the change is the difference between the score at the targeted follow-up minus preoperative baseline score. ODI (a score of 0–100, with higher scores indicating worse disability); VAS (a score of 0–20 for both legs combined, with higher scores indicating more severe pain); PCS (range of 0–100, with higher scores indicating better physical health functioning); MCS (range of 0–100, with higher scores indicating better mental health functioning).
MCS, mental component score; ODI, Oswestry Disability Index; PCS, physical component score; SF-12, 12-Item short form survey; VAS, visual analog scale.
- Table 6
Patient self-reported outcomes as per fusion outcomes within the static cage group.
Static Cage Group Changesa in ODI (%): Mean (Range, SD) 3 mo 6 mo 12 mo Poor fusion 3.2 (−4 to 16, 7.6) −3.5 (−22 to 14, 15.3) −15.64 (−46 to 16, 22.0) Satisfactory fusion −10.29 (−36 to 18, 15.6) −18 (−44 to 14, 17.6) −23.87 (−58 to 18, 19.6) P value 0.045 0.171 0.256 Changesa in VAS—Back: Mean (Range, SD) 3 mo 6 mo 12 mo Poor fusion −2.2 (−9 to 1, 4.2) −3.5 (−9 to 1, 4.8) −3.7 (−9 to 5, 4.1) Satisfactory fusion −2.58 (−6 to 2, 2.5) −3.5 (−7 to 0, 2.1) −4.24 (−10 to 2, 3.2) P value 0.520 0.983 0.661 Changesa in VAS—Both Legs Combined: Mean (Range, SD) 3 mo 6 mo 12 mo Poor fusion −4 (−7 to 0, 3.3) −3.17 (−8 to 2, 3.9) −1 (−14 to 9, 6.1) Satisfactory fusion −5.83 (−12 to 1, 4.0) −6.28 (−15 to 9, 5.1) −7.11 (−14 to 1, 4.7) P value 0.478 0.091 0.048 Changesa in SF-12 (PCS): Mean (Range, SD) 3 mo 6 mo 12 mo Poor fusion 9.68 (5.4–16, 4.5) 10.65 (5.7–16.1, 5.0) 11.81 (−0.4 to 29, 10.3) Satisfactory fusion 7.44 (−2.7 to 21.2, 7.1) 10.03 (−1 to 22, 6.6) 14.53 (−2.8 to 37, 9.9) P value 0.535 0.790 0.439 Changesa in SF-12 (MCS): Mean (Range, SD) 3 mo 6 mo 12 mo Poor fusion −7.2 (−26.1 to 0.7, 10.9) −6.43 (−17.8 to 9.3, 12.9) 1.97 (−22.9 to 38, 15.2) Satisfactory fusion 0.55 (−13.2 to 12.9, 8.8) 3.21 (−10.8 to 20, 6.7) 5.05 (−23 to 28.2, 12.7) P value 0.142 0.202 0.514 Note: Poor fusion is defined as fusion Bridwell grade 3 or 4, with or without subsidence. Satisfactory fusion is defined as Bridwell fusion grade 1 or 2, with no radiographic evidence of subsidence.
↵a The value of the change is the difference between the score at the targeted follow-up minus preoperative baseline score. It denotes statistical significance. ODI (a score of 0–100, with higher scores indicating worse disability); VAS (a score of 0–20 for both legs combined, with higher scores indicating more severe pain); PCS (range of 0–100, with higher scores indicating better physical health functioning); MCS (range of 0–100, with higher scores indicating better mental health functioning).
MCS, mental component score; ODI, Oswestry Disability Index; PCS, physical component score; SF-12, 12-item short form survey; VAS, visual analog scale.
In this issue





{kind=link}
{kind=link}