


Article Figures & Data
Figures
- Figure 1
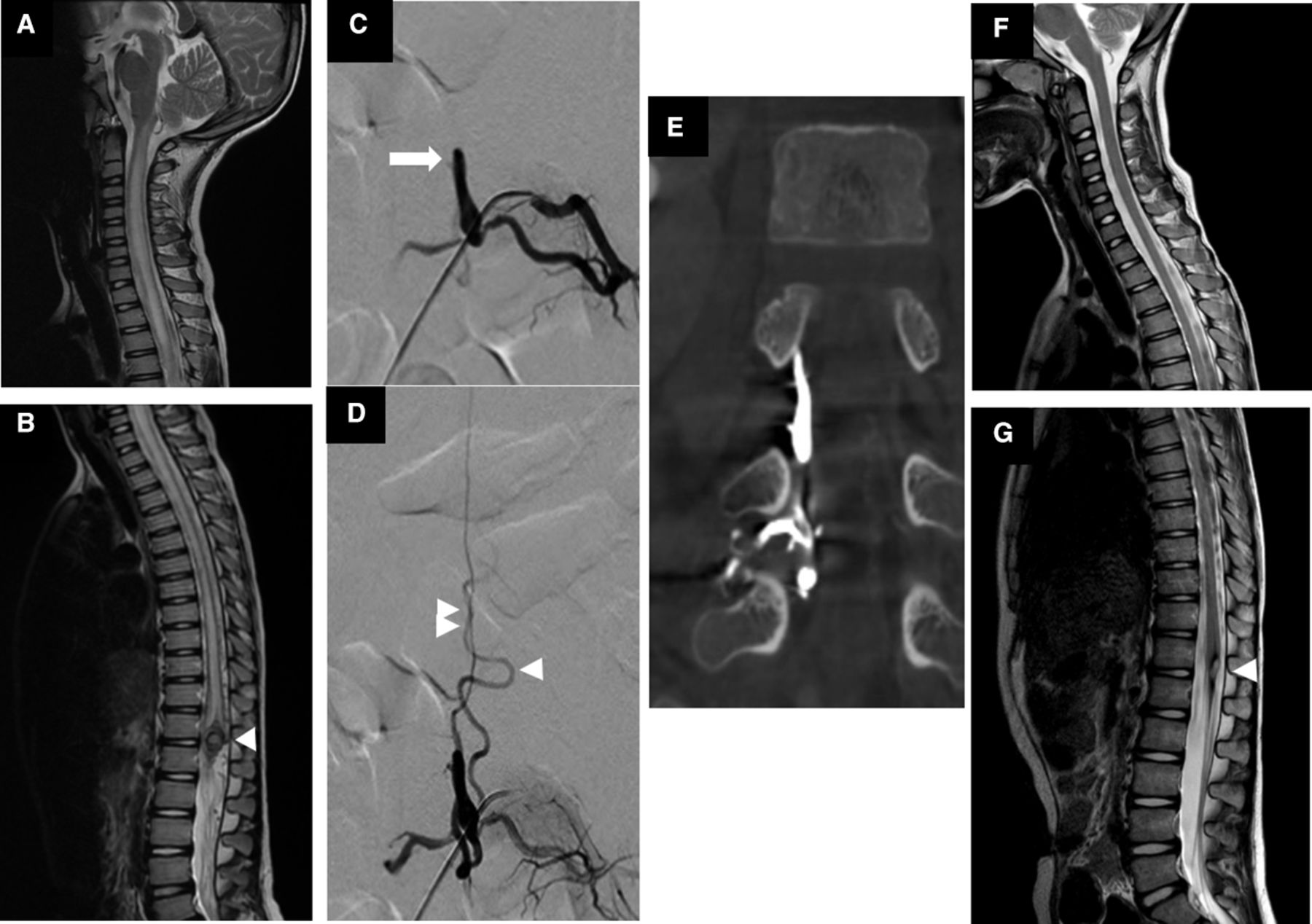
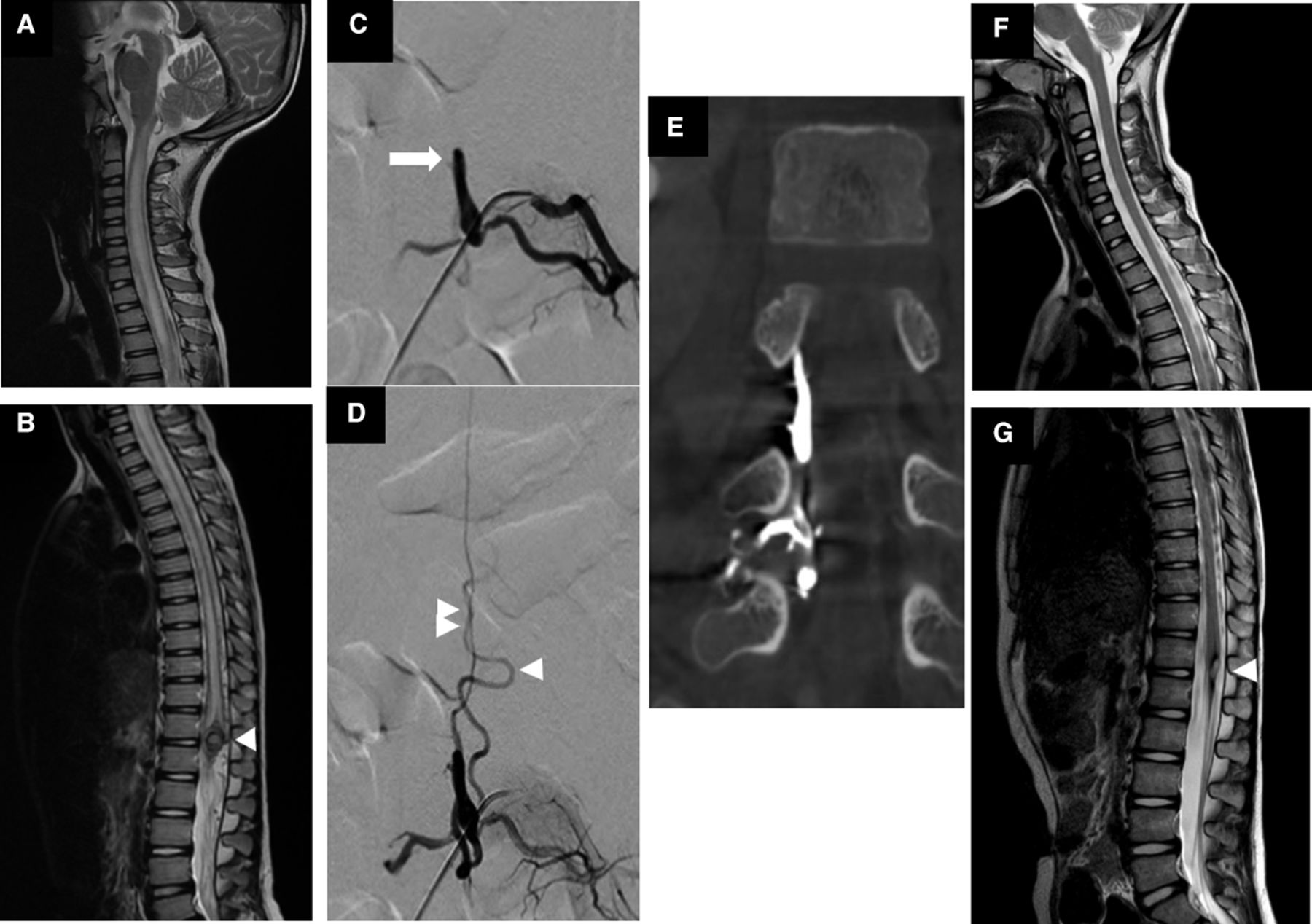
Example of spinal epidural arteriovenous fistula (AVF). (a–b) Pretreatment sagittal T2-weighted magnetic resonance image (MRI) of cervical and thoracolumbar spine shows hyperintense T2 cord signal change from craniocervical junction to conus medullaris with venous pouch at T12/L1 level (white arrowhead). (c) Early epidural venous pouch is fed by left L4 segmental artery (white arrow). (d) Epidural venous pouch drains into 2 radicular veins (white arrowhead). (e) Coronal reformatted image of flat panel computed tomography after transarterial glue embolization shows glue cast in venous pouch, confirming the position of venous pouch is in the epidural space. (f–g) Posttreatment sagittal T2-weighted MRI of cervical and thoracolumbar spine shows resolution of hyperintense T2 change of the spinal cord with hemosiderin deposit at the previously seen venous pouch (white arrowhead).
- Figure 2
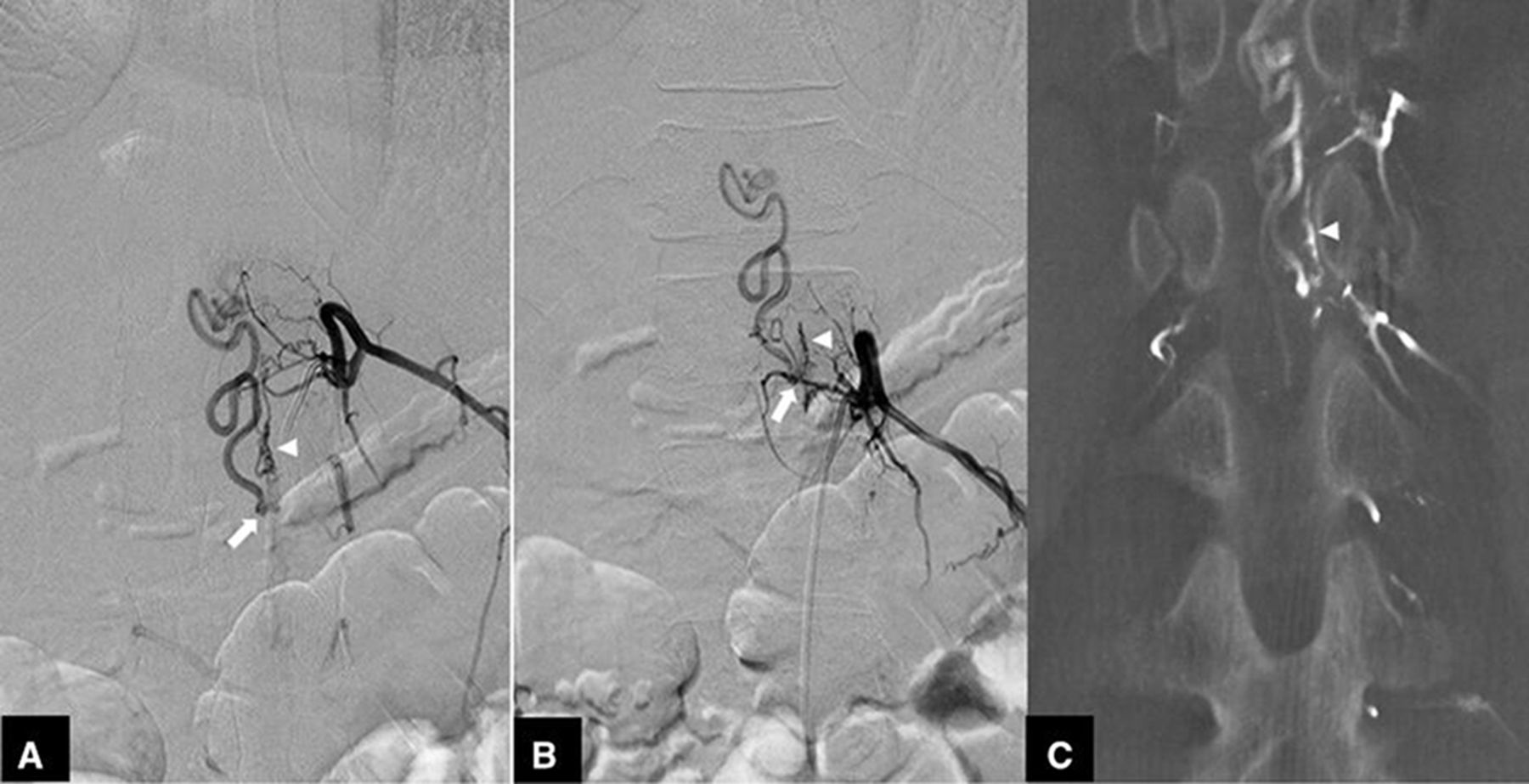
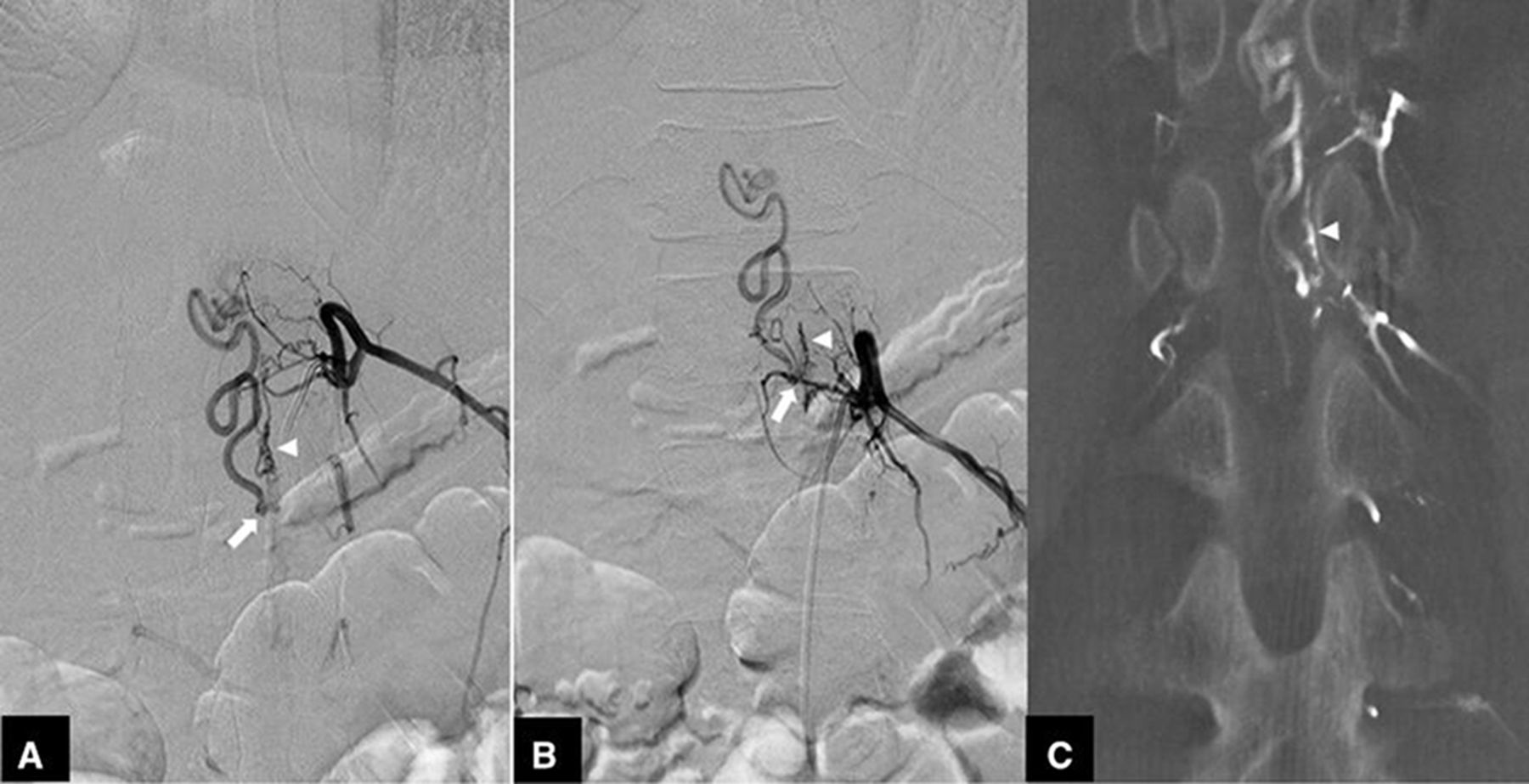
Example of a spinal dural arteriovenous fistula (AVF) at the T12 spinal level that is fed by 2 segmental arteries. (a) Left T11 segmental arterial injection shows the radiculomeningeal artery that runs along the dura (white arrowhead) before opening into the AVF (white arrow). (b) Left T12 segmental arterial injection shows the radiculomeningeal artery feeding the AVF (white arrow). (c) Coronal reformatted view of 3-dimensional rotational angiography before embolization shows the radiculomeningeal artery that runs along the dura.
- Figure 3
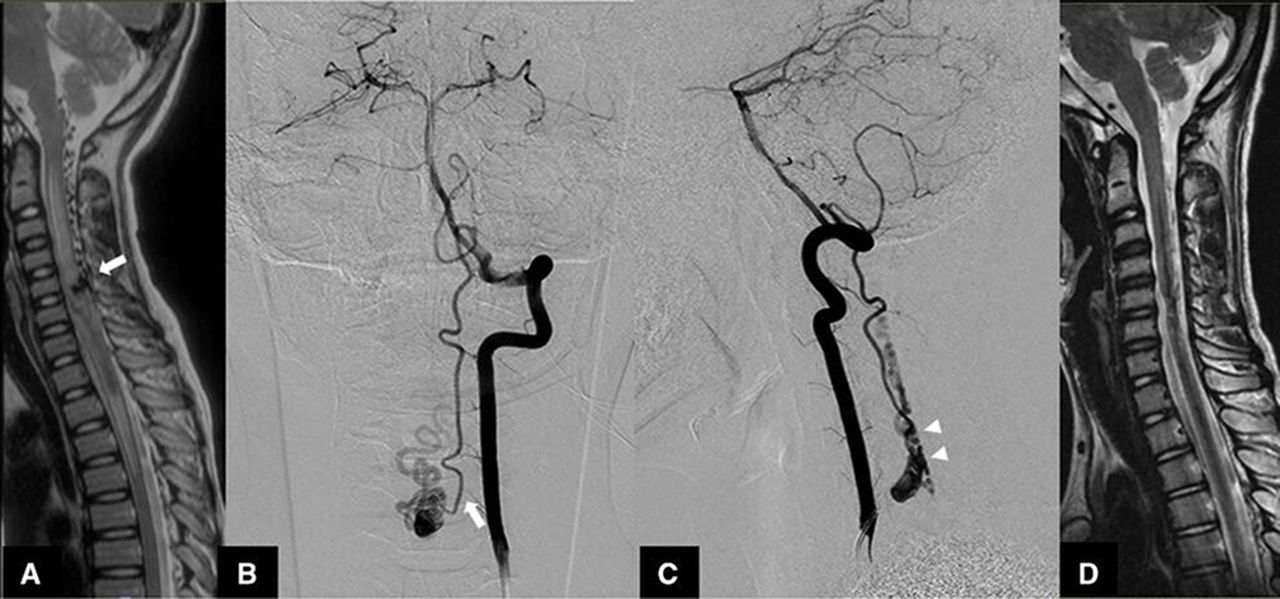
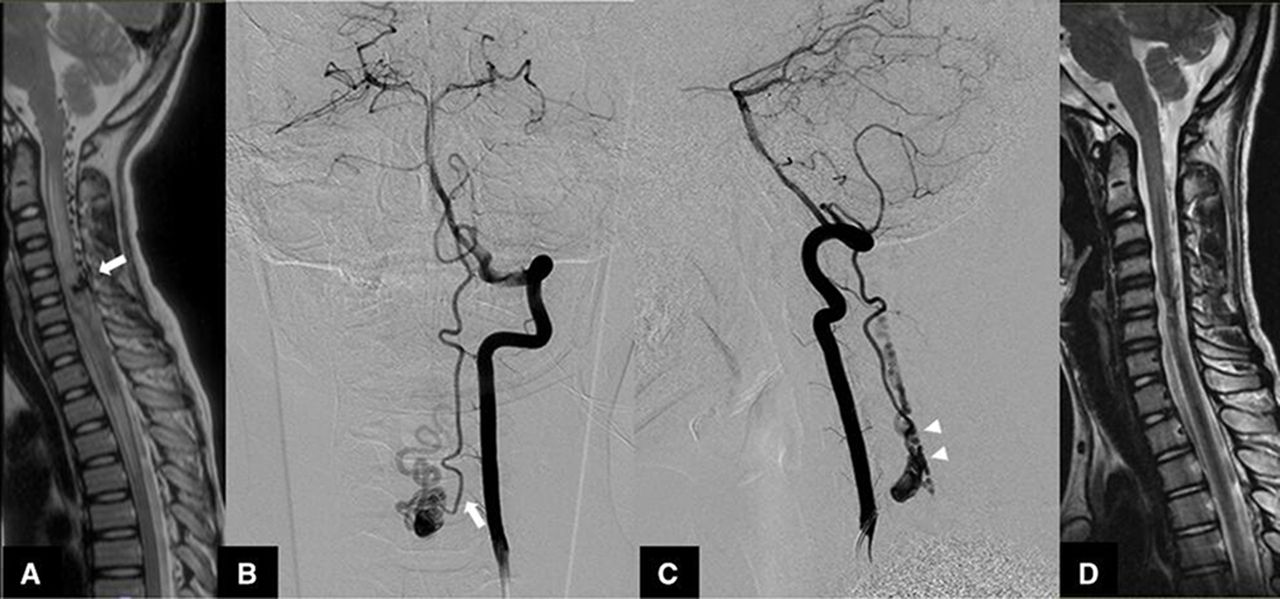
Example of perimedullary arteriovenous fistula (AVF) at the C5 spinal level. (a) Pretreatment sagittal T2-weighted magnetic resonance image (MRI) of the cervical spine shows a hyperintense T2 cord signal change from the craniocervical junction to the T4 level with a venous pouch at the C5 level (white arrow). (b) Anterior-posterior view of left vertebral artery injection shows an AVF that is fed by the left lateral spinal artery (white arrow). (c) Lateral view of the left vertebral artery injection shows an AVF draining into the posterior perimedullary vein (white arrowhead). (d) Posttreatment sagittal T2-weighted MRI of the cervical spine shows resolution of the hyperintense T2 cord signal change with hemosiderin deposition along the spinal cord at C2 to the T4 levels.
- Figure 4
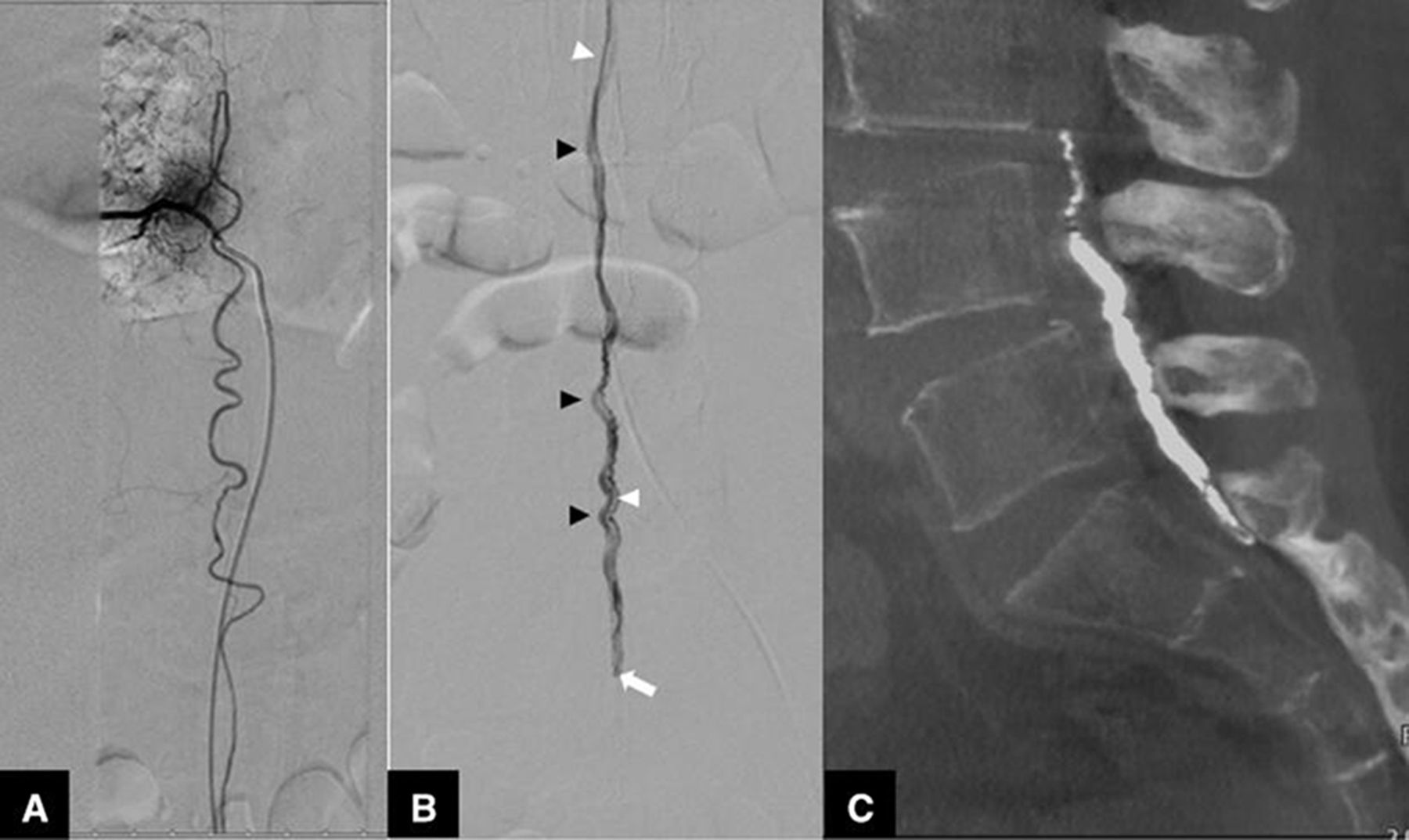
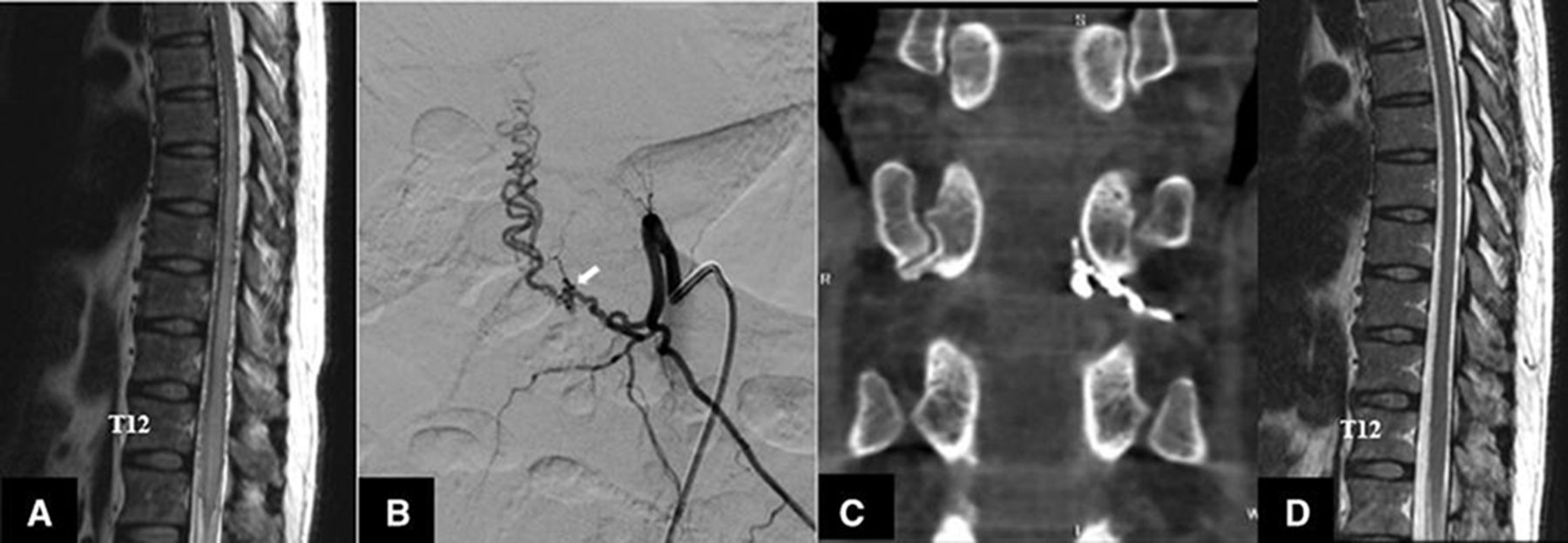
Example of radicular arteriovenous fistula (AVF) at the T11 spinal level. (a) Pretreatment sagittal T2-weighted magnetic resonance image (MRI) of the thoracolumbar spine shows hyperintense T2 cord signal change from T7 to the conus medullaris levels with dilated perimedullary veins. (b) Left T11 segmental arterial injection shows the AVF being fed by the radicular artery (white arrow). (c) Coronal reformatted image of flat panel computed tomography after transarterial glue embolization shows glue cast along the distal segment of left T11 radicular artery and the proximal segment of the radicular vein. (d) Posttreatment sagittal T2-weighted MRI of the thoracolumbar spine shows complete resolution of the hyperintense T2 cord signal change without visualization of the dilated perimedullar veins.
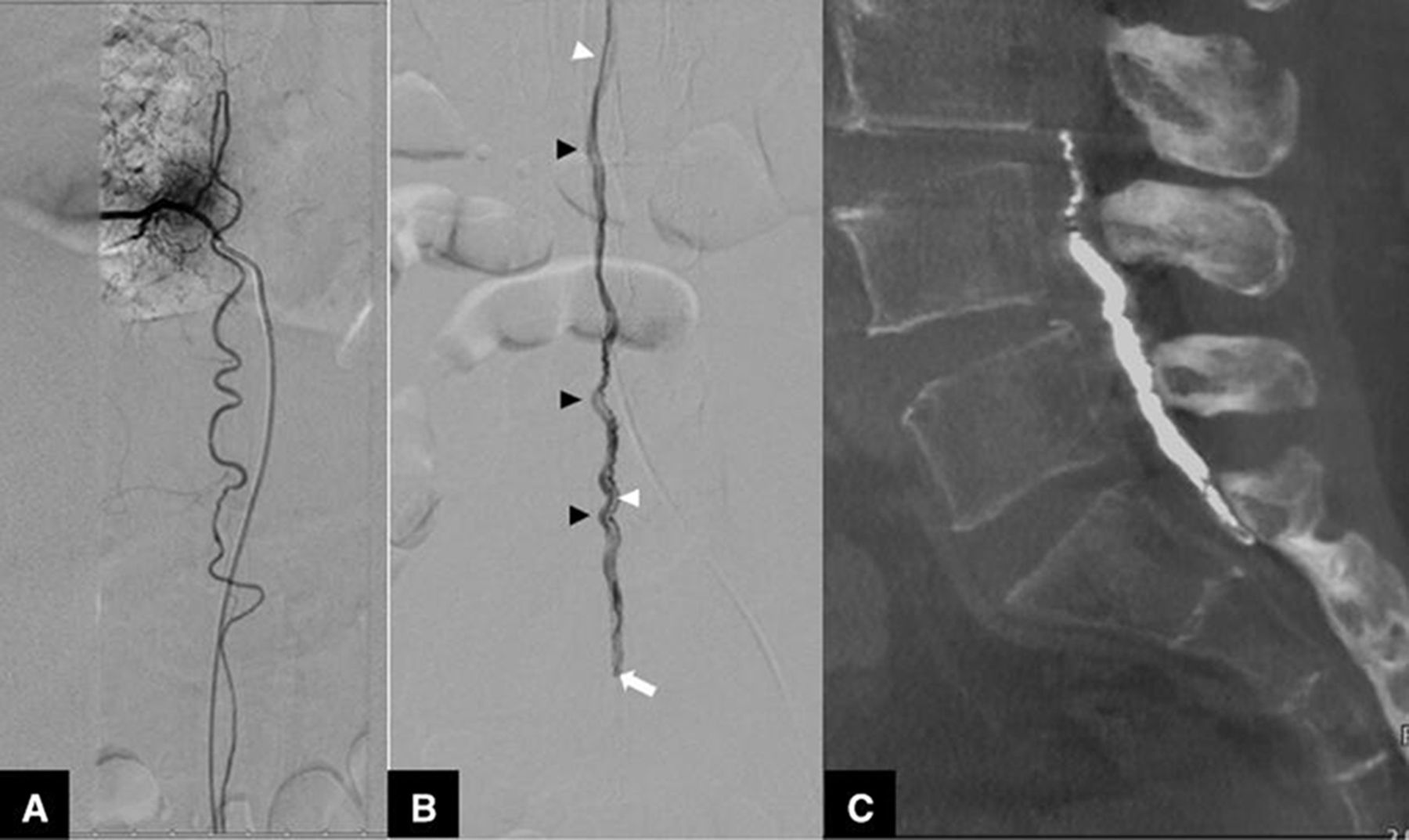
- Figure 5
Example of filum terminale arteriovenous fistula (AVF). (a) Right T9 segmental arterial injection shows the radiculomedullary artery and contributing anterior spinal artery, which runs downward to the conus medullaris. (b) Filum terminale artery (white arrowhead) that is a caudal continuation of the anterior spinal artery feeding the AVF (white arrow), and the filum terminale vein runs upward along the filum terminale (black arrowhead). (c) Sagittal reformatted image of flat panel computed tomography after transarterial glue embolization shows glue cast in the filum terminale vein.

Tables
Inclusion Criteria Exclusion Criteria Diagnosis of the paraspinal AVF, spinal epidural AVF, spinal dural AVF, perimedullary AVF, radicular AVF, or filum terminale AVF
Diagnosis of the intramedullary spinal cord AVM, SAMS, or VVF
Incomplete or absent spinal angiographic imaging
AVF, arteriovenous fistula; AVM, arteriovenous malformation; SAMS, spinal arteriovenous metameric syndrome; VVF, vertebro-vertebral fistula.
Demographic Total (N = 68) Diagnosis Spinal Epidural AVF (n = 16) Spinal Dural AVF (n = 31) Perimedullary AVF (n = 17) Radicular AVF (n = 3) Filum Terminale AVF (n = 1) Age, y, mean (range) 57 (43, 68) 65.5 (56.5, 73.5) 61 (54, 68) 27 (12, 43) 53 (40, 70) 53 Sex, n (%) Female 20 (29.4) 4 (25) 6 (19.4) 10 (58.8) 0 0 Male 48 (70.6) 12 (75) 25 (80.6) 7 (41.2) 3 (100) 1 (100) AVF, arteriovenous fistula.
Presenting Symptom Total (N = 68) Diagnosis Spinal Epidural AVF (n = 16) Spinal Dural AVF (n = 31) Perimedullary AVF (n = 17) Radicular AVF (n = 3) Filum Terminale AVF (n = 1) Weakness 48 (70.6) 11 (68.8) 23 (74.2) 11 (64.7) 2 (66.7) 1 (100) Numbness 46 (67.6) 11 (68.8) 20 (64.5) 12 (70.6) 2 (66.7) 1 (100) Bowel and bladder involvement 39 (57.4) 6 (37.5) 21 (67.7) 11 (64.7) 1 (33.3) 0 Back pain 12 (17.6) 6 (37.5) 4 (12.9) 1 (5.9) 0 1 (100) Radicular pain 13 (19.1) 5 (31.3) 6 (19.4) 2 (11.8) 0 0 Duration, mo, mean (range) 6 (1, 12) 6 (1, 12) 8.5 (3, 12) 0.75 (0.25, 7) 4 (1, 24) 0.25 Note: Data presented as n (%) unless otherwise specified.
AVF, arteriovenous fistula.
MRI Finding Total (N = 68) Diagnosis, n (%) Spinal Epidural AVF (n = 16) Spinal Dural AVF (n = 31) Perimedullary AVF (n = 17) Radicular AVF (n = 3) Filum Terminale AVF (n = 1) Spinal cord edema 64 (94.1) 15 (93.8) 30 (96.8) 16 (94.1) 2 (66.7) 1 (100) Hemorrhage 2 (2.9) 0 0 1 (5.9) 0 1 (100) AVF, arteriovenous fistula; MRI, magnetic resonance imaging.
AVF Characteristic Total (N = 68) Diagnosis, n (%) Spinal Epidural AVF (n = 16) Spinal Dural AVF (n = 31) Perimedullary AVF (n = 17) Radicular AVF (n = 3) Filum Terminale AVF (n = 1) Location Cervical 7 (10.3) 1 (6.3) 2 (6.5) 4 (23.5) 0 0 Thoracic 30 (44.1) 1 (6.3) 20 (64.5) 7 (41.2) 2 (66.7) 0 Lumbosacral 31 (45.6) 14 (87.5) 9 (29) 6 (35.3) 1 (33.3) 1 (100) Number of shunts Single 60 (88.2) 14 (87.5) 30 (96.8) 12 (70.6) 3 (100) 1 (100) Multiple 8 (11.8) 2 (12.5) 1 (3.2) 5 (29.4) 0 0 Arterial feeder Single 39 (57.4) 10 (62.5) 21 (67.7) 5 (29.4) 3 (100) 0 Multiple 29 (42.6) 6 (37.5) 10 (32.3) 12 (70.6) 0 1 (100) AVFs and spinal cord supplies Different segmental artery 43 (63.2) 15 (93.8) 25 (80.6) 0 3 (100) 0 Same segmental artery 25 (36.8) 1 (6.3) 6 (19.4) 17 (100) 0 1 (100) Pial venous reflux No 0 0 0 0 0 0 Yes 68 (100) 16 (100) 31 (100) 17 (100) 3 (100) 1 (100) Venous pouch No 55 (80.9) 15 (93.8) 31 (100) 5 (29.4) 3 (100) 1 (100) Yes 13 (19.1) 1 (6.3) 0 12 (70.6) 0 0 Fistula Micro 59 (86.8) 16 (100) 31 (100) 8 (47.1) 3 (100) 1 (100) Macro 9 (13.2) 0 0 9 (52.9) 0 0 AVF, arteriovenous fistula.
Treatment Total (N = 68) Diagnosis, n (%) Spinal Epidural AVF (n = 16) Spinal Dural AVF (n = 31) Perimedullary AVF (n = 17) Radicular AVF (n = 3) Filum Terminale AVF (n = 1) Endovascular, first treatment 64 (94.1) 16 (100) 28 (90.3) 16 (94.1) 3 (100) 1 (100) Treatment failure 3 (4.7) 0 1 (3.6) 2 (11.8) 0 0 Complete obliteration in first session Yes 48 (75) 14 (87.5) 24 (85.7) 6 (35.3) 3 (100) 1 (100) No 13 (20.3) 2 (12.5) 3 (10.7) 8 (47.1) 0 0 Complication 6 (9.4) 0 3 (10.7) 3 (17.6) 0 0 Surgery, first treatment 3 (4.4) 0 2 (6.5) 1 (5.9) 0 0 Surgery, total treatments n = 6 n = 2 n = 2 n = 2 n = 0 n = 0 Complete cure (%) 5 (83.3) 2 (100) 2 (100) 1 (50) 0 0 No treatment 1 (1.5) 0 1 (3.2) 0 0 0 AVF, arteriovenous fistula.
Follow-up Total Diagnosis, n (%) Spinal Epidural AVF Spinal Dural AVF Perimedullary AVF Radicular AVF Filum Terminale AVF Imaging modality (N = 68) (n = 16) (n = 31) (n = 17) (n = 3) (n = 1) MRA 40 (58.8) 13 (81.3) 17 (54.8) 9 (52.9) 1 (33.3) 0 Spinal angiogram 17 (25) 2 (12.5) 6 (19.4) 7 (41.2) 1 (33.3) 1 (100) NA 11 (16.2) 1 (6.3) 8 (25.8) 1 (5.9) 1 (33.3) 0 Imaging result (n = 57) (n = 15) (n = 23) (n = 16) (n = 2) (n = 1) Cure 50 (87.7) 14 (93.3) 22 (95.7) 11 (68.8) 2 (100) 1 (100) Improvement 6 (10.5) 1 (6.7) 1 (4.3) 4 (25) 0 0 Stability 1 (1.8) 0 0 1 (6.3) 0 0 Clinical result (n = 68) (n = 16) (n = 31) (n = 17) (n = 3) (n = 1) Complete recovery 1 (1.5) 0 0 1 (5.9) 0 0 Improvement 38 (55.9) 7 (43.8) 17 (54.8) 12 (70.6) 2 (66.7) 0 Stability 6 (8.8) 3 (18.8) 2 (6.5) 1 (5.9) 0 0 Worsening 1 (1.5) 0 0 0 0 1 (100) NA 22 (32.4) 6 (37.5) 12 (38.7) 3 (17.6) 1 (33.3) 0 AVF, arteriovenous fistula; MRA, magnetic resonance angiography; NA, not available.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.