


Abstract
Background Cervical spondylotic myelopathy (CSM) is a very common and devastating spinal disease. Congenital cervical stenosis (CCS) is the most common cause. We aimed to elucidate the security, effectivity, and feasibility of surgery combining laminoplasty with artificial disc replacement (ADR) to treat CSM patients with radiculopathy, especially for preserving the range of motion (ROM) of the cervical spine.
Method Between August 2008 and April 2019, 39 patients with multiple CSM caused by CCS were enrolled in the present study. All patients received laminoplasty first and then ADR. We used a retrospective collection of data for evaluating the functional and radiologic outcomes, especially regarding preservation of ROM.
Results Each patient underwent at least a 2-year postoperative follow-up. The Japanese Orthopedic Association score showed great improvements at 6 months. The ADR index-level ROM was preserved during follow-up. The subaxial Cobb angle could also be retained in the whole cervical spine, and the spinal canal diameter could be expanded by more than 52.6%. There were no severe complications or side effects, and no patients needed secondary surgery.
Conclusions We aimed to treat multiple levels of CSM with adequate decompression without too many intervertebral disc replacements. We were able to expand the spinal canal directly for these patients with CCS and needed only 1- or 2-level ADR to treat them with associated radiculopathy. This combined surgical strategy was secure, effective, and was able to preserve the ROM of the cervical spine.
Level of Evidence 4.
- cervical laminoplasty
- artificial disc
- range of motion
- cervical spondylotic myelopathy
- congenital cervical stenosis
Introduction
Cervical spondylotic myelopathy (CSM) is a common disease of the cervical spine in the general population. One of the major causes is congenital cervical stenosis (CCS). This is defined as a cervical spinal canal diameter of <13 mm or a Pavlov ratio of <0.82.1,2 Some patients have obvious symptoms of myelopathy along with radiculopathy. Magnetic resonance imaging (MRI) investigations typically show multiple-segment stenosis with 1- or 2-level anterior disc pathologies (spurs or discs) caused by compression. CSM caused by CCS can be managed by conservative medication at first, but surgery is the “gold standard” treatment and produces good long-term outcomes.3 However, the optimal surgical treatment is still controversial and has been debated widely for a long time. The options include anterior cervical discectomy and fusion (ACDF), artificial disc replacement (ADR), laminoplasty, and laminectomy with or without fusion.
ACDF and ADR can be used to treat anterior cervical pathologies directly but cannot achieve decompression of the CCS. Moreover, ACDF risks increasing adjacent segment disease (ASD), and ADR is expensive and is not suitable for more than 2 levels of lesions. Laminoplasty can achieve adequate canal decompression and preserve cervical range of motion (ROM), but it is hard to resolve the radiculopathy, causing disc pathology from an anterior aspect. On the other hand, laminectomy with fusion can not only restore the lordotic curvature of the neck, but it can also reduce the final ROM.
We chose to combine surgery with laminoplasty first and to perform ADR after 1 to 2 weeks. Laminoplasty for treating myelopathy is an easy way to extend the spinal canal at multiple levels. Moreover, we use an anterior approach with ADR at the most severe level, which relieves symptoms, especially for those with radiculopathy. Most of all, both approaches can preserve cervical ROM and reduce the chances of developing ASD. This combined surgical strategy to treat patients with CSM caused by CCS with radiculopathy proved feasible, safe, effective, and able to preserve cervical spine ROM.
Materials and Methods
This retrospective study evaluated the functional and radiological outcomes of patients who underwent laminoplasty combined with ADR for the treatment of CSM with radiculopathy.
Inclusion and Exclusion Criteria
Patients were included if they had multiple levels of CSM with radiculopathy, were aged <65 years, and presented with CCS (defined as a spinal canal diameter <13 mm or a Pavlov ratio <0.82).1,2 Patients were excluded if they had ossification of the posterior longitudinal ligament (OPLL), trauma, osteoporosis, neoplasm, active infection, or severe systemic disease (eg, rheumatic arthritis).
Surgical Technique
All patients received laminoplasty first and then underwent ADR. Only 1- or 2-level ADRs were applied. We performed modified open-door laminoplasty using titanium miniplates and screws as described by Park and Hellar in 2004.4 The patient was placed in the prone position with the head slightly flexed using a 3-pin Mayfield. A standard posterior midline approach was used to expose the C2-C7 laminae. The paraspinous muscles were dissected laterally to identify the facet joints on both sides while preserving the facet joint capsules. Two channels were drilled bilaterally at the junction of the lamina and the medial aspect of the facet capsule with a cutting burr or high-speed drill until the ventral cortex of the laminae could be identified. The lamina was elevated from either the right or left side after removing the remaining cortex and yellow ligament using 1 - or 2-mm Kerrison. The choice of the opening side was based on the clinical evidence of radiculopathy or the more stenotic side, according to radiography. After elevation of the posterior element, the yellow ligament, dural adhesion, and bridging vessels were released to achieve satisfactory decompression. After the lamina had been elevated enough for adequate decompression, it was fixed with a titanium miniplate and screws (OsteoMed L.P., Glendale, CA, USA). Straight plates with 4 holes were bent into an “open-Z” fashion to be placed in each lamina.5
Note that we usually performed the cut at the lamina-lateral mass junction with preservation of the capsular tissue over the facets to avoid causing instability of the cervical spine and prevent postoperative neck pain. We always kept the C2 and C7 attachment muscles as much as possible and performed a dome-like laminectomy of C2 and C7 to achieve adequate decompression and avoid postoperative kyphosis.
Anterior cervical discectomy was performed as described.6 The patient was placed in a supine position with the neck extended. For the C5-C6 disc level, the incision was placed at the level of the cricoid cartilage or a few centimeters higher when we operated on regions C4-C5. There was usually a skinfold where we aimed to incise. The anterior and marginal osteophytes were drilled away, and the curved cartilaginous plate surfaces of the upper and lower vertebral bodies were scraped by curettage. Complete osteophyte and posterior longitudinal ligament removal were performed with a drill and Kerrison rongeur to achieve adequate decompression. Then, we chose an artificial disc implant—either Mobi-C, BAGUERA, or Prodisc—as approved by the US Food and Drug Administration as an implantable device that replaces the function of a damaged or diseased disc of the neck region (C3-C7).
Study Measures
Clinical outcomes included Japanese Orthopedic Association (JOA) scores, which were measured before surgery and 6 months postoperatively. The cervical spinal canal area was calculated through a voxel-based median plane or optimal symmetry plane (OSP) to assess the preoperative and postoperative canal area.7 The OSP is the median plane that results in the greatest count of paired voxels on opposing sides of the computed tomography (CT) image. An optimization algorithm was formulated to find the OSP automatically, obviating the need for landmark identification of the reference plane.8 Using this CT-based method, we could precisely calculate the actual expended area before and after laminoplasty.
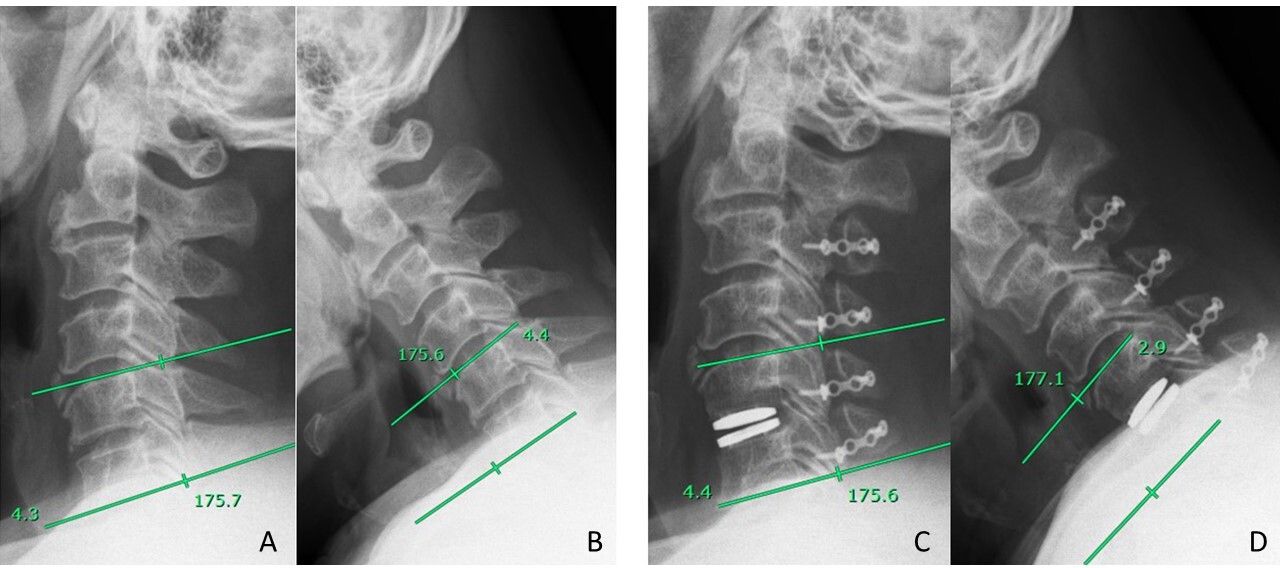
All patients underwent routine preoperative examinations, including dynamic cervical spine x-ray imaging, plain cervical spine x-ray imaging with anterior-posterior and lateral views, cervical spine MRI, and postoperative dynamic x-ray imaging. Radiographs of the patients were taken at the initial examination and at 6 months, 1 year, and 2 years postoperatively in all patients. Measurements were taken for cervical ROM at the index level (treated with an ADR), which was defined as the difference in the Cobb angle between hyperextension and hyperflexion (Figure 1).

(A) Preoperative extension radial graphic, between line means C5 and C6 (index) Cobb angle. (B) Preoperative flexion radial graphic, between line means C5 and C6 (index) Cobb angle; therefore, preoperative range of motion = 4.3° + 4. 4° = 8.7°. (C) Postoperative 6-mo extension radial graphic, C5-C6 (index) Cobb angle. (D) Postoperative 6-mo flexion radial graphic, C5-C6 (index) Cobb angle, postoperative 6-mo range of motion; 4.4° + 2.9° = 7.3°.
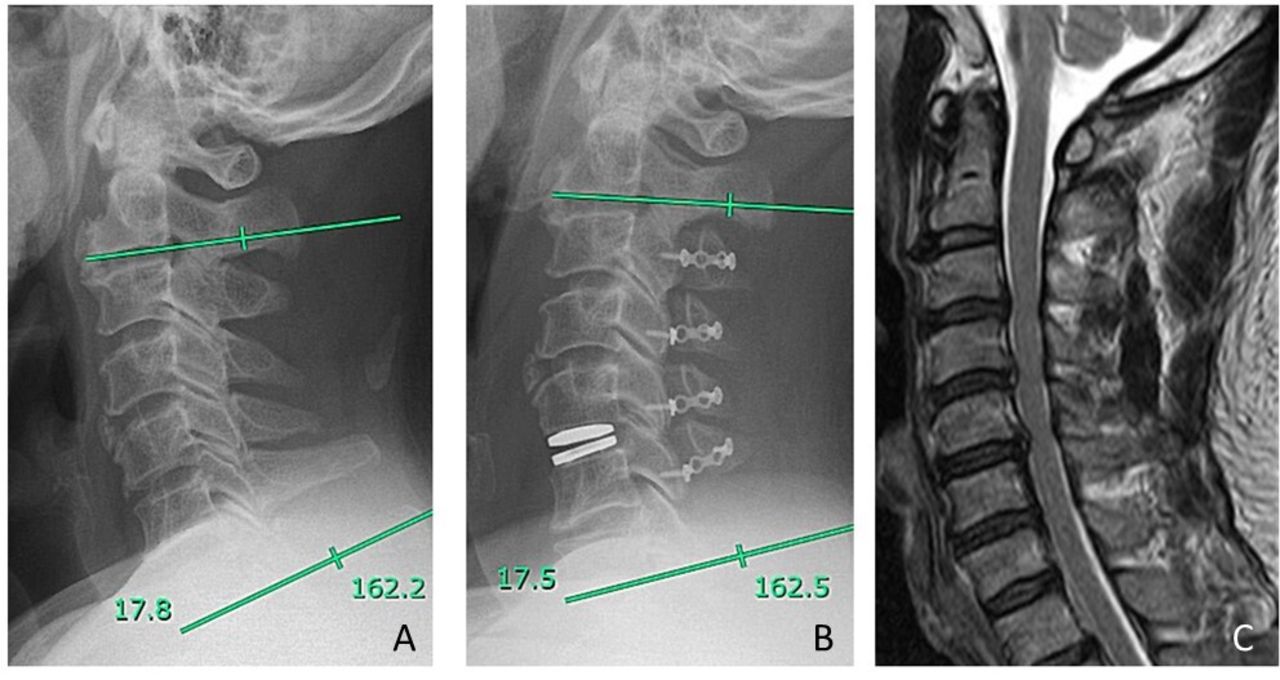
We also checked the subaxial cervical sagittal balance parameters, such as the Cobb angle, before surgery and after 6 months (Figure 2). All radiographic data were obtained by 1 independent nurse specialist under the supervision of the attending physician.

(A) Preoperative lateral graphic, Cobb angle = 17.8°. (B) Postoperative 6-mo neutral lateral graphic, Cobb angle = 17.5°. (C) Preoperative sagittal T2-weighted magnetic resonance image.
Statistical Methods
Statistical calculations were performed using IBM SPSS Statistics (version 25.0; IBM Corp., Armonk, NY, USA) to analyze parameters in all patients. Paired-sample Student t tests were used to compare the means of 2 groups, and P values <0.05 were considered statistically significant.
Results
We enrolled 39 patients with 43 cervical index levels (treated with ADR) with multiple CSM from August 2008 to April 2019. There were 33 male and 6 female patients with a mean age of 49 years (range, 29–65 years). All had a diagnosis of CSM with CCS but not OPLL of the cervical spine. In most patients (35/39), single-level ADR was performed; in the remaining 4 patients, 2-level ADR was performed. In all, 43 index cervical (C) levels were treated with each ADR level as below; C3-C4 (3/43), C4-C5 (16/43), C5-C6 (23/43), and C6-C7 (1/43). The mean body mass index was 26.8 ± 3.0 kg/m2. Patients’ characteristics and surgery levels are listed in the Table.
Patients’ demographics and surgery level.
ADR Index Level
We chose the most severe 1- or 2-level anterior pathologies to perform ADR surgery for CSM caused by CCS. Only 4 patients underwent 2-level ADR (Table). Unless there were obvious T2-weighted signal changes in multiple segments, we selected the most severe segment for ADR surgery and used laminoplasty to get the effect of decompression for other segments. We believe that 1- or 2-level ADR surgical treatment was the most cost-effective choice for CSM caused by CCS. The ADR index level focused on the C4-C5 or C5-C6 segments, which normally allow a maximum ROM in the cervical spine.9
Laminoplasty Level
The most common open-door laminoplasty level was C3-C6 (Table) because the C2 spinous process has a variety of muscle insertions. For some cases, we did not perform C3 laminoplasty because the canal stenosis was not serious at that level. We believed that if we could detach fewer muscles, patients could have fewer adverse axial syndromes. According to a previous study, the incidence of an axial syndrome is estimated at 5.2% to 60%.10 Postoperative C5 palsy is another complication of the posterior approach. The incidence is about 0% to 2.5%, but at the most recent follow-up, most patients reported complete resolution of axial symptoms within 2 months.11
Functional Outcomes
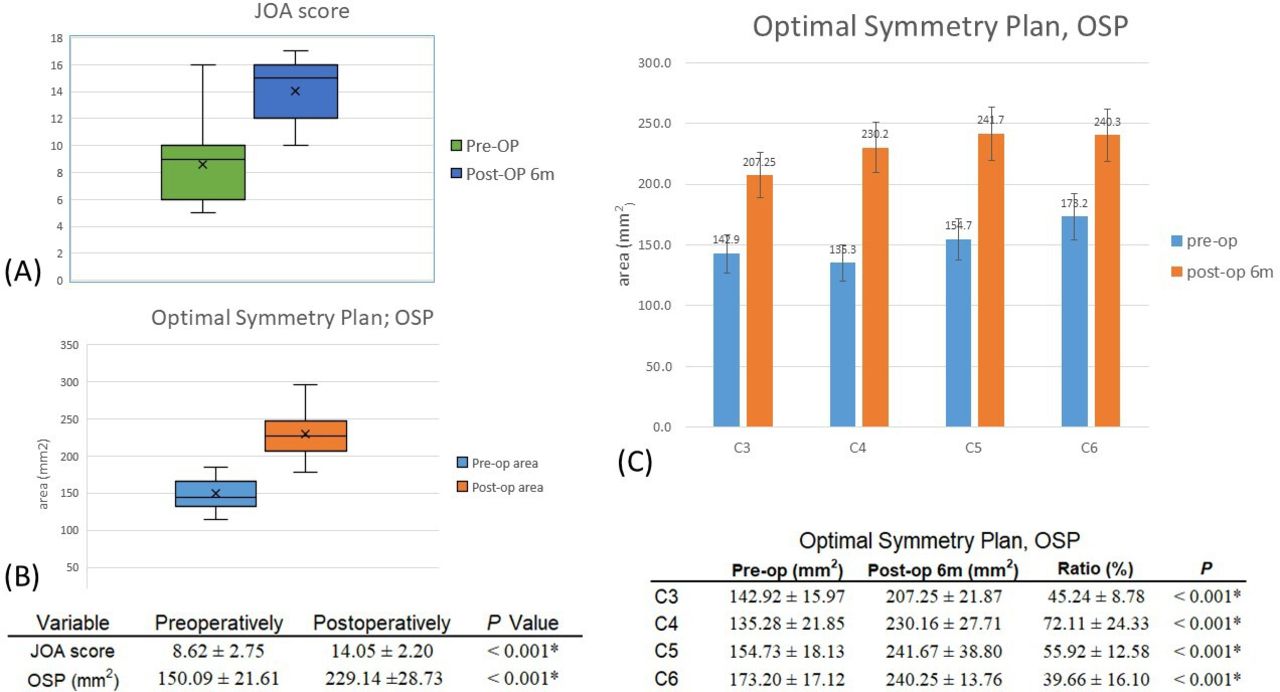
Our results were similar to those reported in most published articles in that JOA scores had improved significantly by 6 months after surgery. The average score ranged from 8.62 ± 2.75 preoperatively to 14.05 ± 2.20 at 6 months (Figure 3). The greatest improvements in JOA of the subgroup were motor function in the lower body and sensory function improvement in the upper body. We posit that the reason behind this finding is that laminoplasty has the ability to augment the spinal canal, thereby mitigating the effects of myelopathy on the lower extremities. No major complications, such as neurological deficits, the need for reoperation, massive bleeding, or prolonged admission time, occurred that required further medical treatment.

(A) The Japanese Orthopedic Association (JOA) score significantly improved after surgery (P < 0.001). (B) The calculated spinal canal diameter significantly expanded after surgery (P < 0.001). (C) Each laminoplasty level canal expansion area. OSP, optimal symmetry plan; post-op, postoperative; pre-op, preoperative. *Statistically significant at P < 0.05.
Twelve of the 39 patients experienced minor postoperative complications such as nuchal pain or soreness. Only 1 patient had nuchal pain that persisted for more than 2 years; pain for the others subsided after discharge. One patient each had symptoms such as C5 palsy and dysphagia, but these problems were resolved after appropriate medical treatment during the admission period.
Canal Expansion
We used images from preoperative and postoperative CT to reconstruct a digital model of the vertebral segment and calculate the OSP, combined with the development of the iterative closest point algorithm for the OSP. The novel technology of superposition for the vertebral segment superposition could help us precisely calculate the degree of expansion of the spinal canal.7 The results are shown in (Figure 3). The mean preoperative area was 150.09 ± 21.61 mm2. The postoperative area was 229.14 ±28.73 mm2 (P < 0.001). Each laminoplasty surgery level had significant enlargement after the 6-month follow-up (Figure 3).
Subaxial Cobb Angle
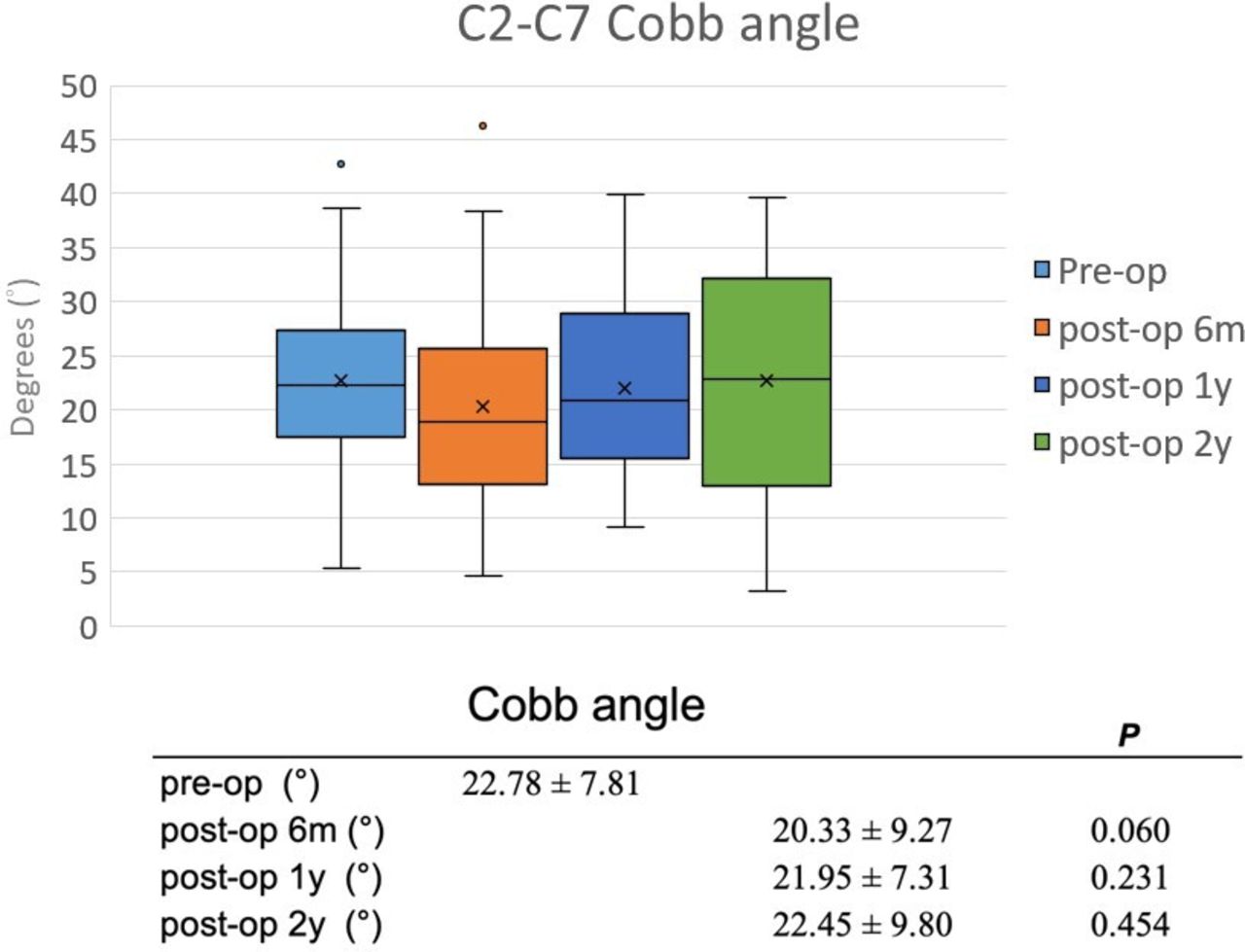
As shown in Figure 4, there were no significant changes in the subaxial Cobb angle between the preoperative stage and at 6 months, 1 year, or 2 years postoperatively. Thus, those patients could maintain lordotic curvature and did not have kyphotic changes. One systematic review study showed cervical laminoplasty significantly reduced the changes in kyphosis during an average follow-up of 39 months.12 We believe that laminoplasty combined with ADR can maintain a patient’s lordotic curvature over a 2-year follow-up.

Cobb angle at preoperative and postoperative 6 mo, 1 y, and 2 y. Each of them had no significant difference.
Range of Motion
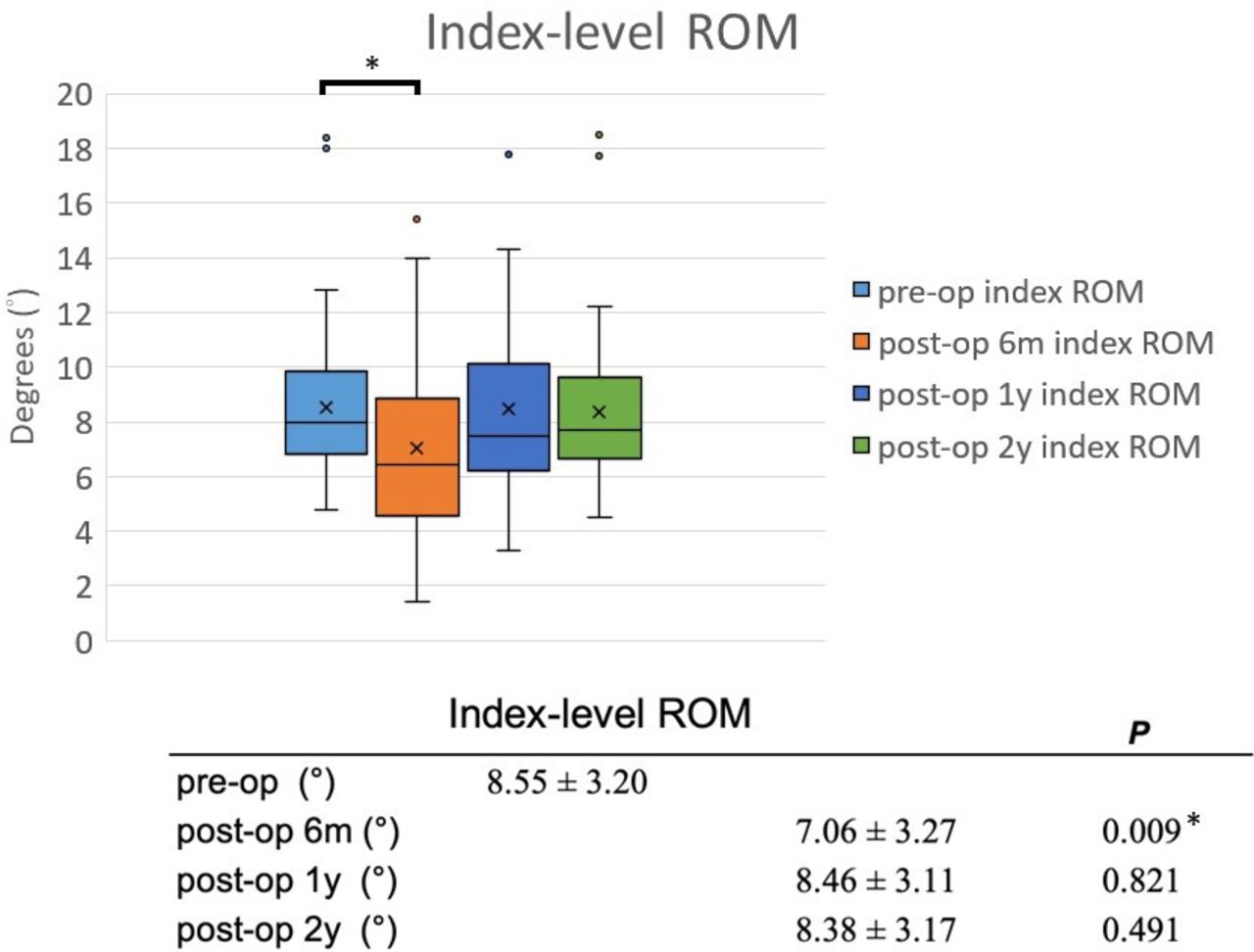
Figure 5 shows that the 39 patients had 43 index levels in all, which decreased from 8.55° (±3.2°) to 7.06° (±3.27°) in the first 6 months. After the 1-year follow-up, the index-level ROM improved to 8.46° (±3.11°), which was close to the baseline. By the 2-year follow-up, the index ROM was 8.38° (±3.17°), but there was no statistically significant difference. Thus, our surgical strategy was able to preserve the index ROM after 2 years of follow-up. Preservation of the ROM is important because it improves functional outcomes and might also, in theory, decrease the incidence of ASD.13

Index-level range of motion (ROM) at preoperative and postoperative 6 mo, 1 y, and 2 y; only postoperative 6 mo had difference than preoperative; After 2-y follow-up, the index-level ROM could preserve as preoperation.
Case Examples
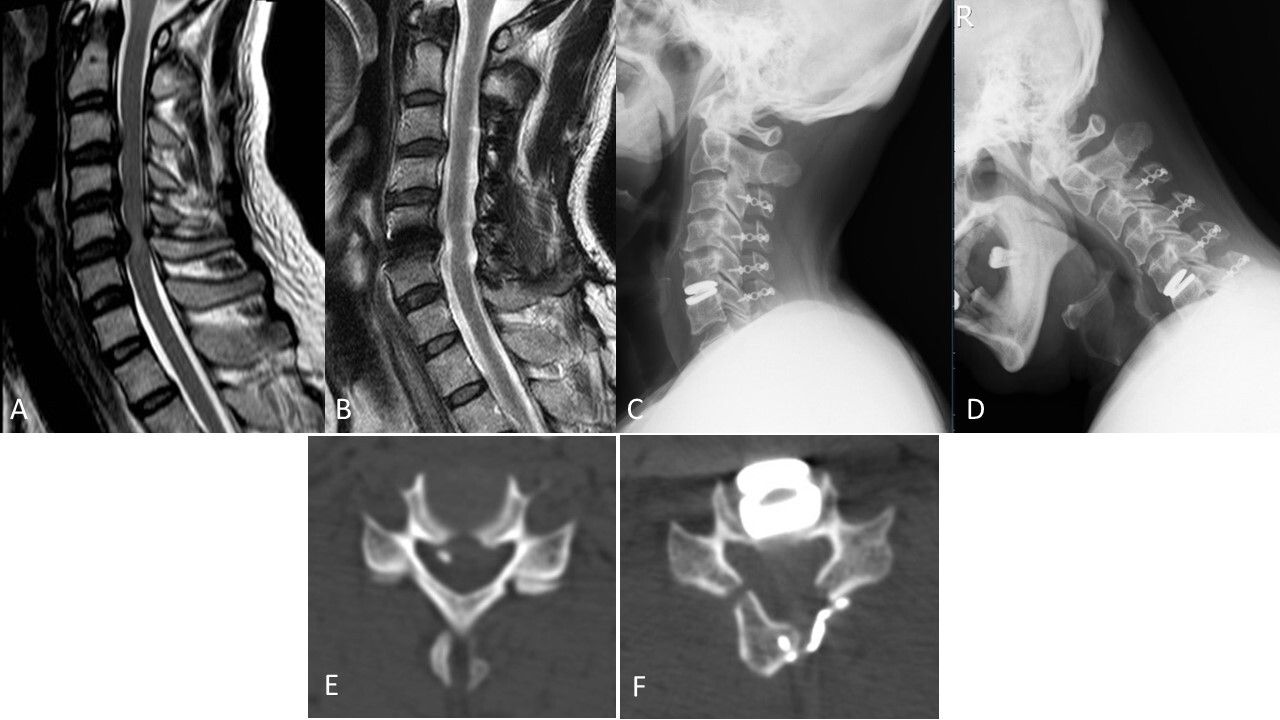
In case 1 (Figure 6), we performed laminoplasty for multiple levels of decompression and then performed ADR at the index level at C5-C6 (because of severe compression from the anterior aspect). Therefore, we could take advantage of both the anterior approach of ADR and the posterior approach of laminoplasty.

Case 1. (A) Preoperative sagittal T2-weighted magnetic resonance image (MRI). (B) Postoperative 2-y sagittal T2-weighted MRI. (C and D) Postoperative 2-y extension and flexion view of cervical spine x-ray image: preservation of range of motion. (E) Preoperative bone window axial view at the C5-C6 level. (F) Postoperative 6-mo bone window axial view at C5-C6 level with an obviously expanded spinal canal.
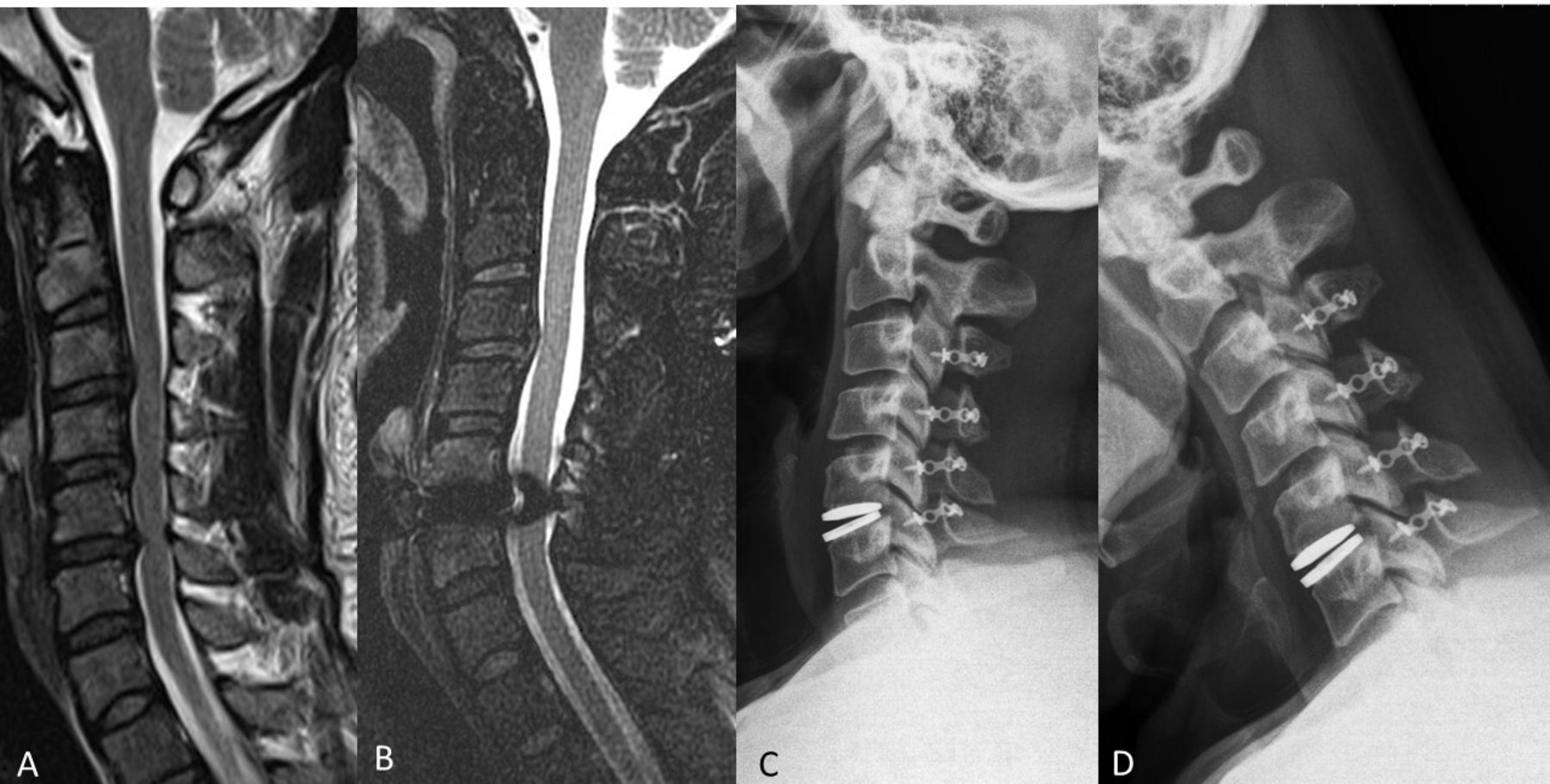
In case 2 (Figure 7), the presence of stenosis in multiple segments, particularly at the C3-C4 and C5-C6 levels, presents a challenge in determining the most appropriate surgical approach. An anterior procedure, such as an ACDF or ADR, may be considered, but it remains unclear whether to perform surgery on just C3-C4 and C5-C6 or to extend it to a 3-level surgery encompassing C3-C4-C5-C6. Both options carry risks, such as limited ROM in the case of an ACDF or increased medical costs with an ADR. Therefore, we decided to arrange C3-C6 laminoplasty for the long multiple-segment spinal stenosis and ADR for severe compression from the anterior aspect at the C5-C6 level.

Case 2. (A) Preoperative sagittal T2-weighted magnetic resonance imaging (MRI), C3-C4 and C5-C6 had anterior disc compression lesion. (B) Postoperative 2-y follow-up T2-weighted MRI, spinal canal expansion. (C and D) Postoperative 2-y extension and flexion x-ray images reveal preserved range of motion.
For case 3, two short videos (Video 1 and Video 2) demonstrate the fluoroscopy of a patient who underwent surgery in 2008 to demonstrate that the ROM of the cervical spine joints was preserved.
Discussion
Optimal surgical intervention for patients with CSM caused by CCS remains uncertain. Spinal cord decompression can be performed via anterior, posterior, or combined approaches, which has been a topic of much debate in spinal surgery.14 There are many surgical treatments, including ACDF, ADR, laminoplasty, and laminectomy with or without fusion, which are widely used in contemporary surgical practice.15 Each of them has its advantages and disadvantages.
Laminoplasty, a technique of reconstructing the vertebral lamina to decompress the spinal cord, is good for spinal cord decompression and direct expansion of the spinal canal, therefore relieving myelopathy.16 Laminoplasty was first described in 1973 in Japan and was initially performed for OPLL. In 1983, Hirayabashi et al described “open-door” laminoplasty for CSM.17 It is suitable for myelopathy and multiple-segment stenosis. The technique of laminoplasty is relatively simple and avoids the prolonged anesthesia time necessary for an anterior approach. The protective function of the lamina is retained, and there is less scarring above the dura than the following laminectomy with or without fusion. However, laminoplasty has some risk of causing kyphotic changes and C5 palsy and occasionally causes postoperative nuchal pain.18
The ACDF and ADR approaches can treat anterior spinal pathologies directly but cannot achieve decompression of the CCS. ACDF can significantly enhance arthrodesis,19 but the elimination of motion can lead to increased stress contributing to ASD.20 ADR was developed to preserve the subaxial cervical spine biomechanics and natural segmental ROM.21 It has been increasing in popularity and is especially suitable for younger patients instead of ACDF.22 ADR has a lower revision rate than ACDF, has less chance of adjacent segment degeneration, and helps preserve the ROM.23 ADR is good for disc pathology decompression from the front, especially for single-level lesions with radiculopathy.24 However, the anterior approach is difficult for long segments and is expensive.12 Moreover, it is difficult and controversial to determine at which level ADR should be performed when dealing with multiple-level stenoses or noncontinuous-segment level stenosis. Some concerns have been raised about multilevel ADR, including the prolonged surgical time, possible heterotopic ossification, and its higher cost.25
Neither laminoplasty nor ADR uses rigid fusion because this is not necessary for those patients with CCS who have CSM because it is not an unstable spine disease. Therefore, the spine can retain neutral stability, and patients can have earlier, more aggressive rehabilitation and return to work as soon as possible. Note that the patients we included were all under the age of 65 years. Preserving the index level of the ROM is important for them to decrease the changes in ASD.26
Our results showed that this surgical strategy could preserve both the subaxial Cobb angle and index-level ROM. Cervical lordosis is very important for neck posture and function. Nuchal pain and instability are usually associated with cervical sagittal unbalance.27 The cervical spine is a remarkably complex region of the skeleton because it not only supports the head but also allows the widest ROM relative to the rest of the spine. Therefore, preserving lordosis and keeping an adequate ROM are very important for successful cervical spine surgery.
In the present article, the affected patients had chronic myelopathy symptoms, and neurologic examinations revealed long-tract signs such as increasing deep tendon reflex in the knee, a positive Babinski’s sign, or even a spastic gait. However, they did not complain of lower limb weakness because these myelopathy symptoms are chronic and do not interfere with daily life. The patients’ chief complaints were usually painful sensations and numbness in the neck, arm, forearm, or hand. They came to seek medical help only if they had radiculopathy signs. Therefore, although an anterior approach to ADR could resolve the radiculopathy, we believe that laminoplasty is still important for treating the true underlying CSM in patients with CCS.
In our opinion, the spinal canal of the CSM in patients with CCS is too narrow, so we chose to expand the canal diameter directly first through laminoplasty and then decompress only the narrowest level from the front, to reduce the pressure on the cord while using a Kerrison rongeur. It is well known that, when performing ADR, you must aim to fit the disc space tightly. If the spinal canal is very narrow at this time, it can cause devastating consequences. Therefore, the expansion of the spinal foramen from the back can avoid this complication, which is why we performed laminoplasty first.
There are some concerns about the surgical indications and timing in this series. The patient selection process for the use of ADR remains a topic of debate among surgeons. The US Food and Drug Administration, which adheres to strict exclusion criteria,28 states that the contraindication for using ADR is an unstable cervical spine and does not include a past history of laminoplasty as a criterion. In Brazil and France, the exclusion criteria also do not include intact posterior elements.28 In our laminoplasty technique, we always preserve the facet joints as much as possible to preserve stability. Moreover, we rarely perform foraminotomy to relieve radiculopathy: if it is present, it is operated on through an anterior approach. In our data, neither instability nor deformity was detected even among repeated surgeries of patients who received this combined procedure. We believe this procedure is safe and effective.
Laminoplasty performed in conjunction with foraminotomy can achieve cord and nerve root decompression in most cases. However, there are a few patients whose anterior pathologies are significantly large or have compressions on both sides. In these cases, decompression must be solved through an anterior approach. Zdeblick et al reported that foraminotomy leads to facet joint damages (because of >50% facetectomy) and increased the kyphosis rate.29 On the other hand, foraminotomy cannot be performed on the hinge side of open-door laminoplasty. Some cases with foraminal stenosis on both sides were more suitable to operate through the anterior side to achieve decompression. Moreover, we have performed laminoplasty for CSM on 430 patients from 2008 to 2019, and only 39 patients received this combined surgery, which highlights that only a small population of patients required this approach.
As for surgical timing, laminoplasty usually caused postoperative wound pain. For the posterior approach, many patients complained of postoperative neck pain, rigidity, tension, and stiffness. These symptoms usually subsided 1 to 2 weeks after the operation, and the anterior approach for ADR could be arranged during this period. Interestingly, some patients felt improved symptoms and signs after receiving laminoplasty and did not continue to be hospitalized for a second surgery. The other possibility is to complete the 2-stage operation at the same time, but the patient needs to be turned over under anesthesia. We have only performed 1 such operation. We need more data and experience to study and confirm whether this method is feasible.
Our inclusion criteria did not cover OPLL, even if it is 1 form of CSM in some studies. Patients with OPLL have the same symptoms and signs, their cervical spine MRIs also have similar characteristics. However, the mainstream surgical treatment for OPLL does not recommend using a frontal approach. It is hard to differentiate between OPLL and CSM among patients with CCS simply through x-ray images and MRI. To avoid diagnostic errors, we will arrange CT images to screen and exclude patients with OPLL.
There are some limitations to this study. First, it was a retrospective study with a relatively small sample size. In addition, the samples were not randomized, which may have resulted in selection bias. Second, each surgical technique was performed by the same surgeon. The skillsets and experience of surgeons could have some impact on the results. In addition, we did not compare our approaches with other surgical methods but have tried to explain the benefits of this method in a straightforward manner. We aim to do further research to determine the exact benefits of this method.
Conclusions
According to the results of our study, we believe this combined strategy allows surgeons to take advantage of laminoplasty and ADR for patients who had canal stenosis and disc pathologies caused by compression from the front. We believe that this method is not only a safe and effective way to solve the patient’s stenosis problem but also a very good way to preserve the ROM of the cervical spine after surgery.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.