


Article Figures & Data
Figures
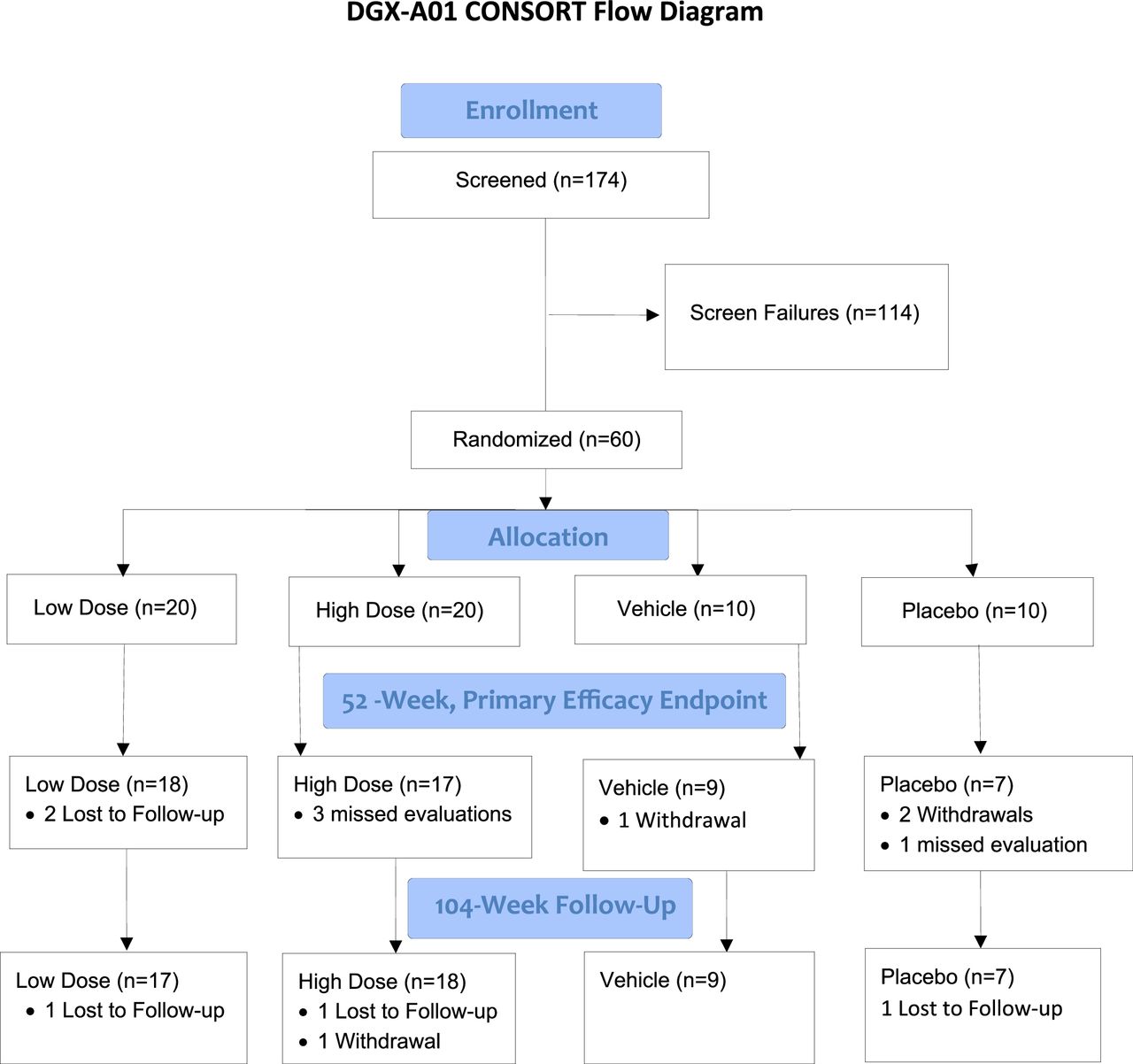
- Figure 1
Study CONSORT (Consolidated Standards of Reporting Trials) flow chart.
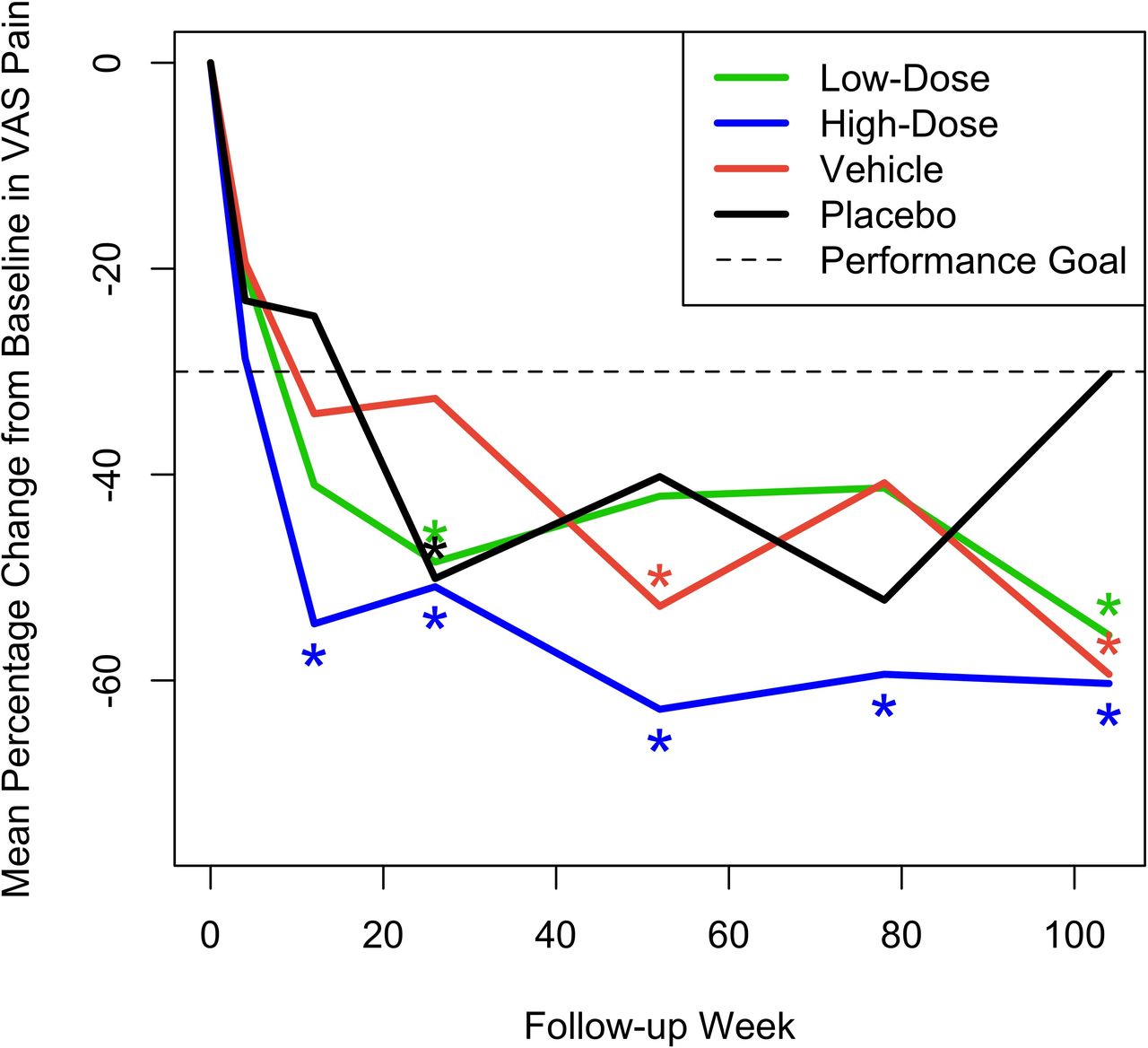
- Figure 2
Mean percent change across time from baseline in visual analog scale (VAS) pain scores for the 4 treatment groups. Asterisks denote statistically significant improvement of greater than 30%.
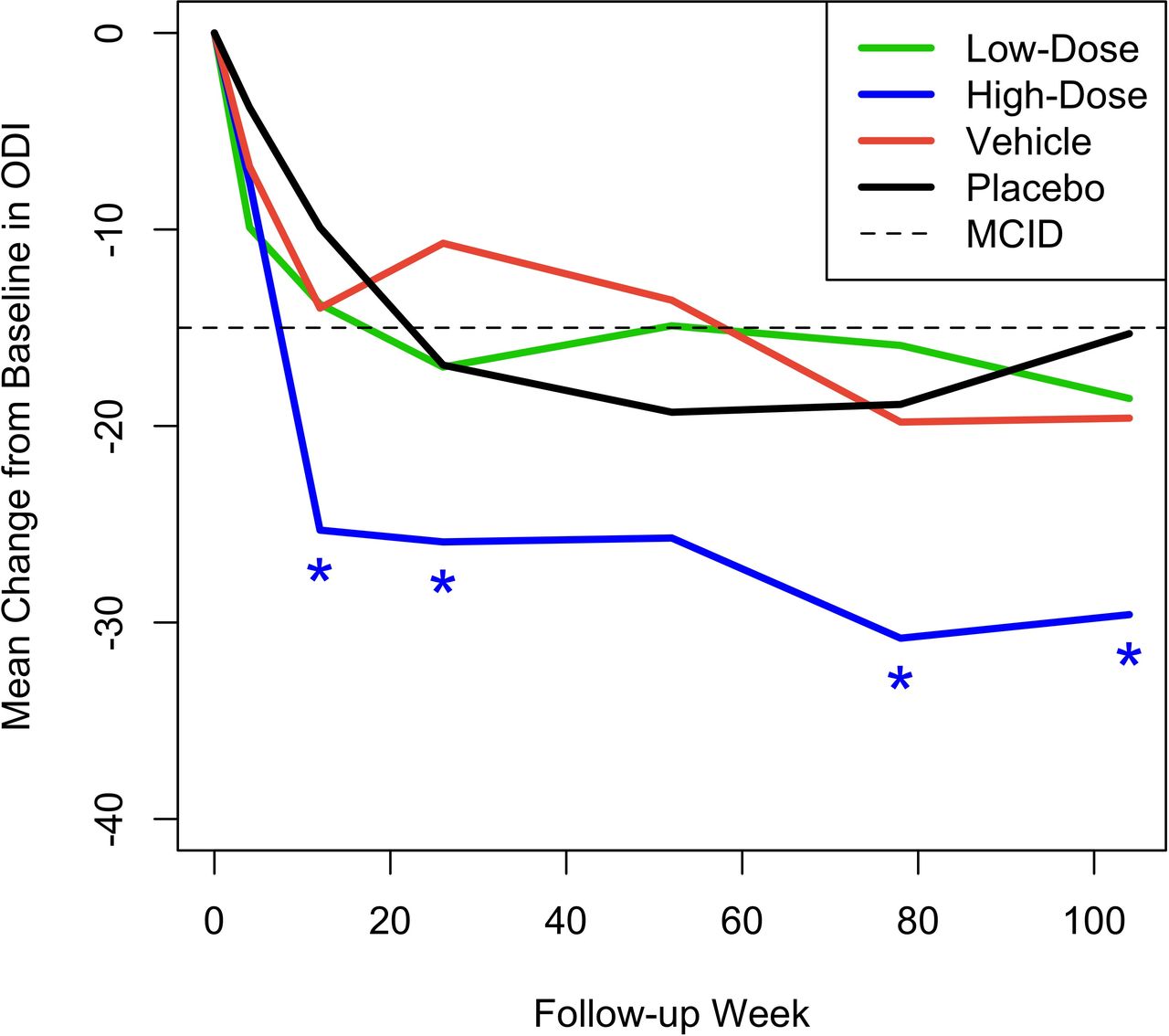
- Figure 3
Mean change from baseline across time in Oswestry Disability Index (ODI) for the 4 treatment groups. Asterisks denote statistically significant improvement compared with a minimal clinically important difference (MCID) of –15.
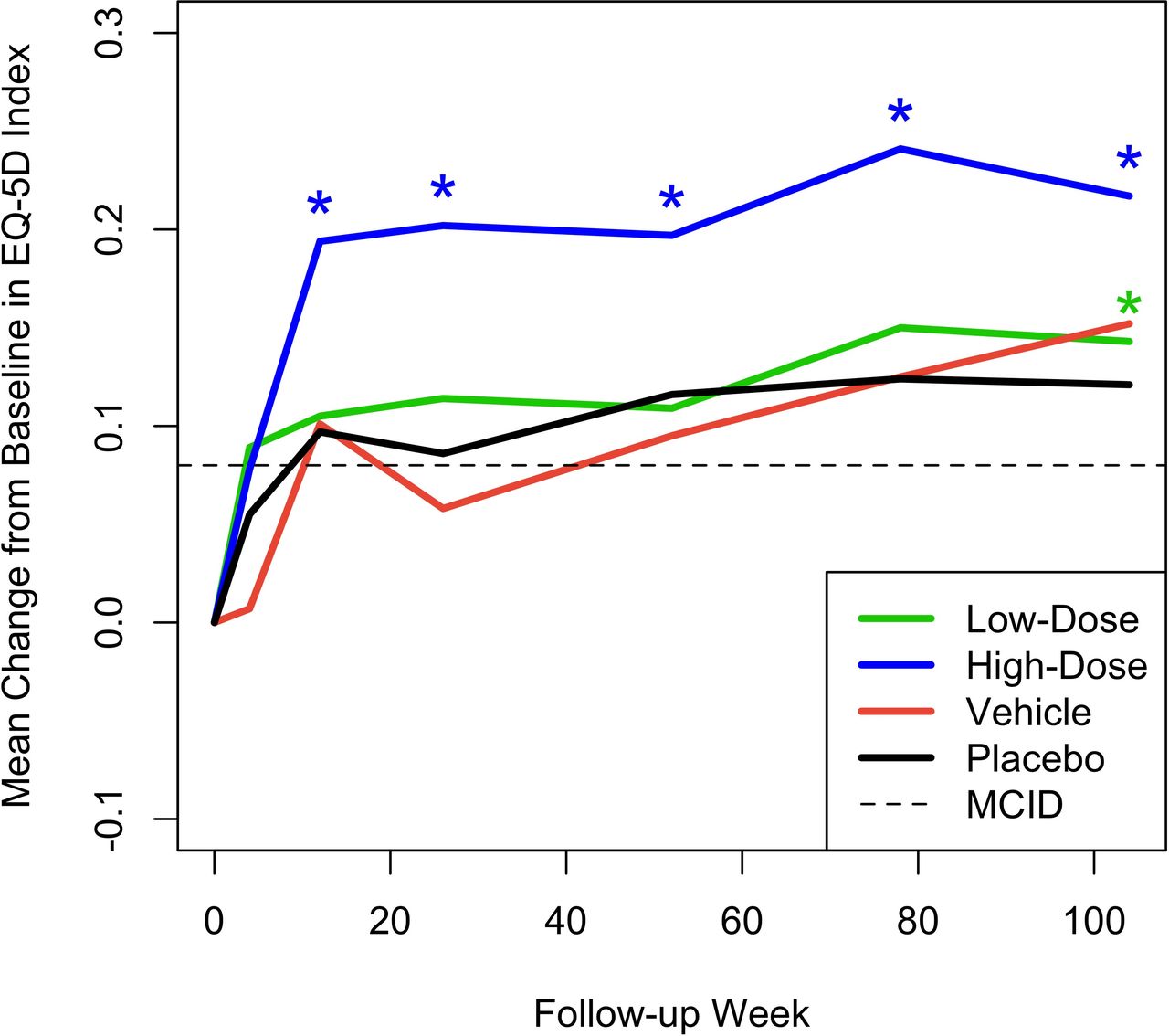
- Figure 4
Mean change from baseline across time in EQ-5D Health Index for the 4 treatment groups. Asterisks denote statistically significant improvement compared with a minimal clinically important difference (MCID) of +0.08.
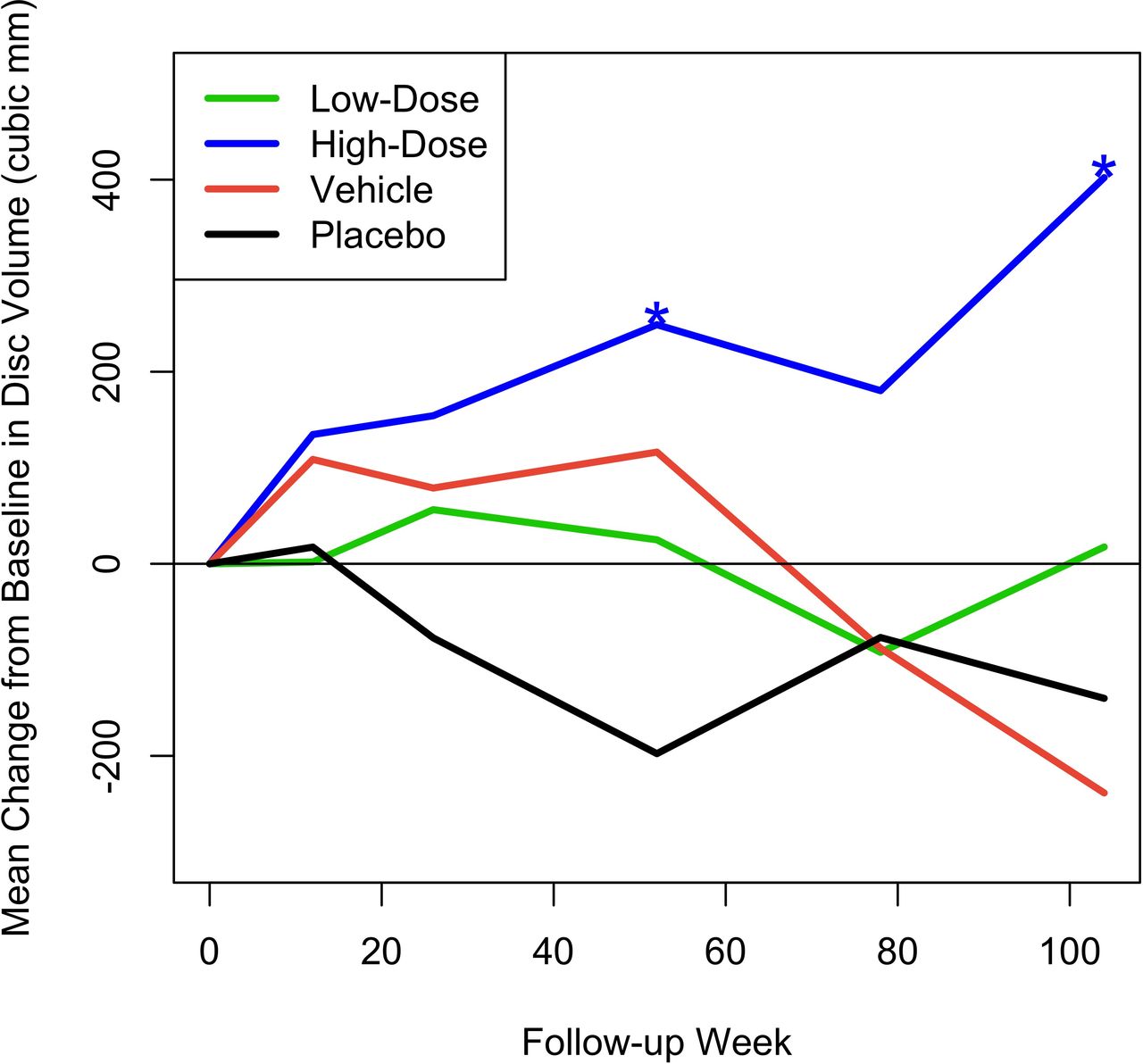
- Figure 5
Mean change from baseline in disc volume (mm3). Asterisks denote statistically significant change.
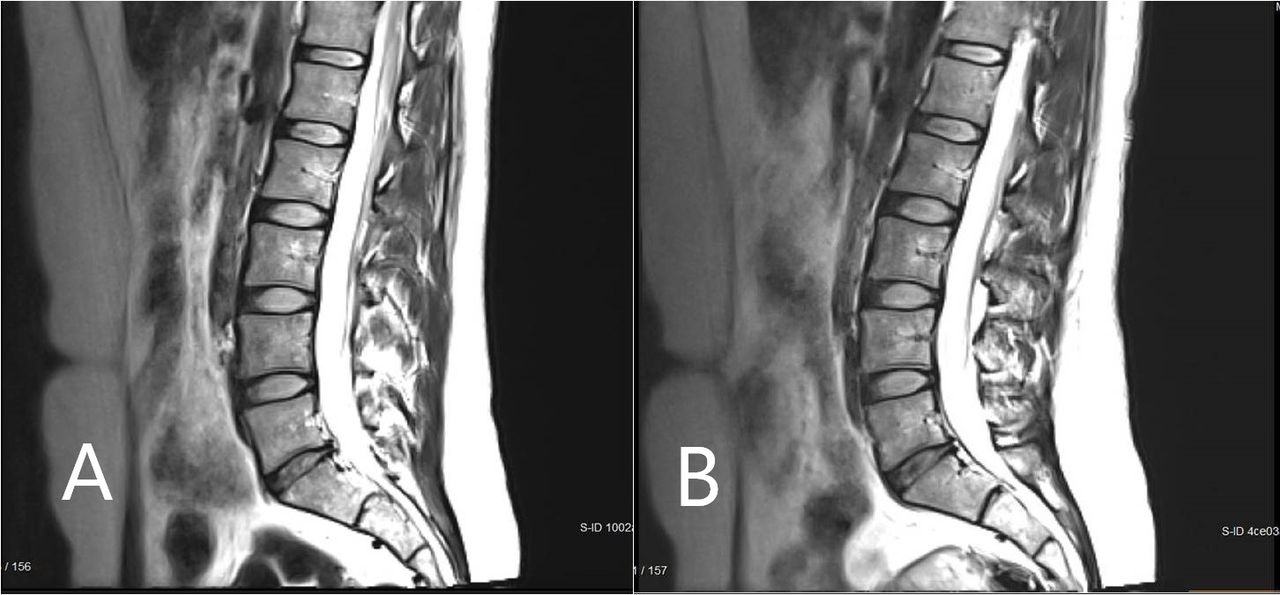
- Figure 6
Magnetic resonance imaging scan of a study participant with single-level disc pathology at L5-S1 at (A) baseline and (B) 6 months after high-dose injectable disc cell therapy. Disc height and volume increased by 6 months.






Tables
Inclusion Criteria 1. Diagnosis of early to moderate, symptomatic, single-level degenerative disc disease from L3–S1. 2. Target disc that met Modified Pfirrmann Grades 3–7. 3. Aged ≥18 and ≤75 years, skeletally mature, with body mass index ≥18 kg/m2 at screening. 4. Chronic low back pain for at least 6 mo prior to screening. 5. Low back pain that was unresponsive to at least 3 mo of conservative care (nonoperative treatment) within the previous year, which may have included physical therapy, as well as bed rest, anti-inflammatory or analgesic medications, chiropractic manipulations, acupuncture, massage, or home-directed lumbar exercise programs. 6. Pretreatment low back pain of 40–90 mm on the VAS at screening and day 1. 7. Pretreatment Oswestry Disability Index score of 30–90 at screening and day 1. 8. Willing to voluntarily sign the informed consent form and agreed to the release of previous medical history for purposes of this study (ie, HIPAA authorization) at screening. 9. Physically and mentally able to comply with the protocol, able to understand and complete the required forms, and willing and able to adhere to the requirements of the protocol in the opinion of the investigator. 10. Female patients of childbearing potential had to agree to and comply with using highly effective methods of birth control for the duration of the study (eg, oral contraceptive, implant, injectable, indwelling intrauterine device, sexual abstinence, condoms, or a vasectomized partner). Exclusion Criteria Physical/medical history exclusion criteria 1. Low back pain that, in the investigator’s opinion, was predominately myofascial in nature. 2. Constant, unchanging low back pain that was not improved in any spinal position. 3. Radiculopathy resulting from nerve compression. 4. Nonradicular unilateral or bilateral leg pain with intensity greater than 50% of the intensity of the low back pain, as measured by VAS. 5. Leg pain that was of radicular origin (ie, due to stimulation of nerve roots or dorsal root ganglion of a spinal nerve by compressive forces). 6. Frequent leg pain that extended below the knee. 7. Severe unilateral or bilateral osteoarthritis of the knee or hip. 8. Cauda equina syndrome. 9. Previous lumbar spine surgery. 10. Previous disc-invasive treatment procedures (ie, intradiscal electrothermal therapy and intradiscal radiofrequency thermocoagulation), intradiscal injections (ie, injection of corticosteroids, methylene blue, dextrose, or glucosamine and chondroitin sulfate), or epidural steroid injections at L3–S1 within the 3 mo prior to screening. (Discography may have been performed, but the procedure must have been done at least 2 wk or more prior to the injection of study medication.) 11. Clinical suspicion of facet pain as a primary pain generator. 12. Current infection at the planned procedure site, active systemic infection, or current or prior history of lumbar spinal infection (ie, discitis, septic arthritis, and epidural abscess) at baseline (day 1). 13. A history of fibromyalgia as diagnosed by a rheumatologist. 14. Tested positive for hepatitis B virus, hepatitis C virus, or HIV. 15. The presence of an active malignancy or tumor, or a prior history of malignancy within the past 5 y (except for basal cell carcinoma of the skin). 16. The presence or prior history of a spinal malignancy. 17. Significant systemic disease, such as unstable angina or autoimmune disease, such as rheumatoid arthritis. 18. A congenital or acquired coagulopathy or thrombocytopenia. 19. Currently taking anticoagulant, antineoplastic, antiplatelet, or thrombocytopenia-inducing medications (except for aspirin or nonsteroidal anti-inflammatory drugs). 20. At higher risk for postsurgical infection (eg, taking immunosuppressants), had a severe infection, or had a history of serious infection. 21. Concomitant conditions requiring daily oral steroid usage for more than 30 d in the preceding 90 d before screening. 22. History of chronic opioid use (greater than 3 mo), unless the patient had been off opioids for 3 mo prior to enrollment. 23. History of unexplained, easy, or persistent bruising or bleeding, bleeding from the gums, or bleeding problems experienced in previous surgical procedures. 24. History of hypersensitivity or anaphylactic reaction to bovine products, sodium hyaluronate/hyaluronan/hyaluronic acid, gentamicin, amphotericin b, dimethyl sulfoxide, crustaceous/shellfish, or porcine products. 25. Uncontrolled psychiatric condition or substance/alcohol abuse that would potentially interfere with the patient’s participation in the study within 2 y prior to screening in the opinion of the investigator. 26. Positive serum pregnancy test or nursing at the time of screening or had plans to become pregnant within the planned length of the study (2 y). 27. A body habitus that precludes adequate fluoroscopic visualization for the procedure, or the procedure was physically impossible. 28. Required an implantable electronic defibrillator, pacemaker, or had other contraindication to MRI scanning or could not tolerate MRI scanning. Patients who were expected to require a defibrillator or pacemaker as determined by the investigator were excluded. 29. Participated in another clinical study within the 6 mo prior to screening. 30. Been a recipient or planned to be a recipient during trial participation of stem cell/progenitor cell therapy or other biologic intervention to repair discs at L3–S1. Other exclusion criteria 31. Pending litigation against a health care professional, except where required by the insurer as a condition of coverage. 32. Prisoner or active military personnel who was not available for the entire planned length of the trial. 33. Active or pending worker’s compensation claims. 34. In the investigator’s opinion, the patient was not suitable for participation in the clinical trial. Imaging exclusion criteria: Modified Pfirrmann exclusion criteria for L3–S1 35. Had 2 discs between L3 and S1 that were Modified Pfirrmann Grades 4–7, and the Modified Pfirrmann Visualization showed that the target disc was the same or better than the nontarget disc. 36. Had 2 discs between L3 and S1 that were Modified Pfirrmann Grades 4–7 and a discogram on the nontarget disc demonstrated symptomatic involvement. 37. All 3 discs had Modified Pfirrmann Grades 4–7. Imaging exclusion criteria: Radiographic exclusion criteria for L3–S1 38. Evidence of prior lumbar vertebral body fracture at L3–S1. 39. An acute fracture of the spine at the time of study enrollment. Clinically compromised vertebral bodies within L3–S1 due to current or past trauma (eg, sustained pathological fracture or multiple fractures of vertebrae). 40. Evidence of dynamic instability on lumbar flexion-extension radiographs as indicated by >4.5 mm of translational motion at L3–S1; >15° of angular motion at L3-L4; >20° of angular motion at L4-L5; or >25° angular motion at L5-S1. 41. Grade 2 or higher spondylolisthesis at L3–S1, as assessed by Meyerding classification. 42. Lumbar spondylitis or other undifferentiated spondyloarthropathy. 43. Evidence of Type III Modic changes at L3–S1. 44. Clinical suspicion of a full-thickness annular tear at L3–S1. 45. Evidence of abnormal disc morphology defined as an extrusion or sequestration according to Fardon classification at L3–S1. Abbreviations: HIPAA, Health Insurance Portability and Accountability Act; MRI, magnetic resonance imaging; VAS, visual analog scale.
- Table 2
Demographics and baseline characteristics for all patients and by treatment group.
Characteristics All
N = 60Low-Dose IDCT
N = 20High-Dose IDCT
N = 20Vehicle
N = 10Placebo
N = 10Age, y, mean (SD) 37.9 (9.7) 36.6 (9.0) 36.9 (8.0) 43.0 (11.0) 37.3 (12.5) Sex, men/women, % 60.0/40.0 70.0/30.0 50.0/50.0 60.0/40.0 60.0/40.0 Body mass index, kg/m2, mean (SD) 27.4 (4.4) 26.3 (4.3) 27.2 (4.3) 28.7 (4.7) 27.4 (4.4) Race, % 85.0 90.0 85.0 80.0 85.0 White 5.0 5.0 10.0 0.0 0.0 Asian 3.3 5.0 0.0 10.0 0.0 Black/African American 1.7 0.0 5.0 0.0 0.0 American Indian/Alaskan Native 5.0 0.0 0.0 10.0 20.0 Other/multiple Modified Pfirrmann Score, % 3 11.7 5.0 25.0 0.0 10.0 4 65.0 75.0 55.0 80.0 50.0 5 1.7 0.0 0.0 0.0 10.0 6 16.7 15.0 15.0 20.0 20.0 7 5.0 5.0 5.0 0.0 10.0 Target treatment level, % L3–L4 5.0 10.0 0.0 10.0 0.0 L4–L5 28.3 10.0 25.0 50.0 50.0 L5–S1 66.7 80.0 75.0 40.0 50.0 Abbreviation: IDCT, injectable disc cell therapy.
- Table 3
Mean (SD) pain visual analog scale scores in mm for the 4 treatment groups across time.
Treatment Group Low-Dose IDCT
N = 20High-Dose IDCT
N = 20Vehicle
N = 10Placebo
N = 10Day 1 60.5 (13.4) 64.9 (14.7) 62.6 (10.0) 63.3 (17.1) Week 4 46.8 (24.2)) 45.2 (27.3) 51.8 (20.9) 45.9 (15.4 Week 12 34.8 (23.3) 30.3 (24.8) 40.4 (23.6) 45.6 (16.7) Week 26 31.5 (19.9) 32.1 (23.7) 41.1 (18.2) 29.6 (8.7) Week 52a 36.6 (23.8) 23.8 (21.2) 30.0 (24.2) 38.6 (23.9) Week 78 37.3 (24.6) 25.9 (26.2) 34.9 (21.5) 31.6 (21.2) Week 104 28.1 (21.9) 26.7 (26.6) 25.2 (17.5) 44.8 (18.8) Abbreviation: IDCT, injectable disc cell therapy.
↵a Primary endpoint (N’s = 18, 17, 9, and 7 for the 4 groups, respectively).
online supplementary file 1.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.