


Abstract
Background Percutaneous pedicle screw (PPS) placement has become a pivotal technique in spinal surgery, increasing surgical efficiency and limiting the invasiveness of surgical procedures. The aim of this study was to analyze the accuracy of computer-assisted PPS placement with a standardized technique in the lateral decubitus position.
Methods A retrospective review of prospectively collected data was performed on 44 consecutive patients treated between 2021 and 2023 with lateral decubitus single-position surgery. PPS placement was assessed by computed tomography scans, and breaches were graded based on the magnitude and direction of the breach. Facet joint violations were assessed. Variables collected included patient demographics, indication, intraoperative complications, operative time, fluoroscopy time, estimated blood loss, and length of stay.
Results Forty-four patients, with 220 PPSs were identified. About 79.5% of all patients underwent anterior lumbar interbody fusion only, 13.6% underwent lateral lumbar interbody fusion only, and 6.8% received a combination of both anterior lumbar interbody fusion and lateral lumbar interbody fusion. Eleven screw breaches (5%) were identified: 10 were Grade II breaches (<2 mm), and 1 was a Grade IV breach (>4 mm). All breaches were lateral. About 63.6% involved down-side screws indicating a trend toward the laterality of breaches for down-side pedicles. When analyzing breaches by level, 1.2% of screws at L5, 13% at L4, and 11.1% at L3 demonstrated Grade II breaches. No facet joint violations were noted.
Conclusion PPS placement utilizing computer-assisted navigation in lateral decubitus single-position surgery is both safe and accurate. An overall breach rate of 5% was found; considering a safe zone of 2 mm, only 1 screw (0.5%) demonstrated a relevant breach.
Clinical Relevance PPS placement is both safe and accurate. Breaches are rare, and when breaches do occur, they are lateral.
Level of Evidence 3.
Introduction
Percutaneous pedicle screw (PPS) placement has become a pivotal technique in spinal surgery, especially for addressing thoracolumbar pathologies. The precision of PPS insertion is crucial because inaccuracies can lead to severe neurological complications and adversely affect patient outcomes.1,2 Screw malpositioning not only is the most frequent complication but also entails significant biomechanical disadvantages.3 While initially placed using fluoroscopy,4–7 recent advances in enabling technologies have led to the integration of 3-dimensional (3D) computer-assisted navigation systems, aiming to improve accuracy and safety.
With the aim of increasing surgical efficiency and limiting the invasiveness of surgical procedures, lateral decubitus single-position surgery (L-SPS), which combines both anterior and posterior column support through anterior lumbar interbody fusion (ALIF) and/or lateral lumbar interbody fusion (LLIF) with PPS placement performed in the lateral decubitus position, has gained popularity and evidence base.8 L-SPS eliminates the need for time-consuming operating room setup changes and patient repositioning when moving from supine or lateral to prone positioning.9 In addition, when PPS is placed through small incisions, the posterior tension band is not compromised, and paraspinal muscles are not detached, which results in shorter hospital stays, less blood loss/postoperative pain, and accelerated recovery times.10
However, despite these advantages, reports on the accuracy of PPS placement in the L-SPS, particularly when evaluated using postoperative computed tomography (CT), are limited. In addition, the laterality of breaches is rarely reported, and facet joint violations have not been evaluated. Minimally invasive L-SPS is a relatively new technique, and more evidence from different sites is needed to support the use of navigation in L-SPS. Therefore, the aim of this study was to analyze the accuracy of computer-assisted PPS placement with a standardized technique in the lateral decubitus position.
Materials and Methods
A retrospective review of prospectively collected data was performed on patients undergoing 1- to 3-level L-SPS via LLIF, ALIF, or combined LLIF/ALIF with PPS placement between L1 and S1. Twenty-six patients (59.1%) underwent a single-level fusion, 15 patients underwent 2-level fusion (34.1%), and 3 patients (6.8%) underwent 3-level fusion. All surgeries were performed by the senior author. Patient data were reviewed from an institutional review board–approved prospective single-surgeon registry. Inclusion criteria included PPS placement in L-SPS in skeletally mature patients (radiographically closed growth plates, eg, femoral physes, triradiate cartilage, and Risser Stage V) undergoing fusion for degenerative pathologies, with the exception of 1 patient undergoing fusion for spondylosis. CT was performed at 1-year follow-up as per standard of care. Patients who presented before their 1-year follow-up were included if they had undergone intraoperative CT to assess instrumentation or required CT postoperatively for the purpose of assessing instrumentation if patient symptoms warranted. Seventeen patients (36.6%) had underwent CT prior to the 1-year follow-up. Of these 17 patients, 14 were scanned intraoperatively. Three patients complained of persistent leg pain postoperatively and underwent CT. Pedicle screw malposition could be excluded, and the pain was classified as radiculitis. This was treated with oral cortisone, and the symptoms resolved over time. Patients who had screws placed prone, open, or without navigation were excluded, as were patients treated for infection, revision, or tumor. The primary endpoint was the assessment of pedicle screw placement accuracy. Accuracy was evaluated using the Ravi grading system based on a 2-mm increment scale.11 The presence or absence of facet joint breaches by screws was also evaluated. Measurements were performed in a blinded fashion by an independent fellowship-trained orthopedic surgeon unaware of the clinical outcome.
Variables collected included patient demographics, indication for surgery, intraoperative complications, operative time, fluoroscopy time, estimated blood loss, and length of stay.
Surgical Technique
Setup and Patient Positioning
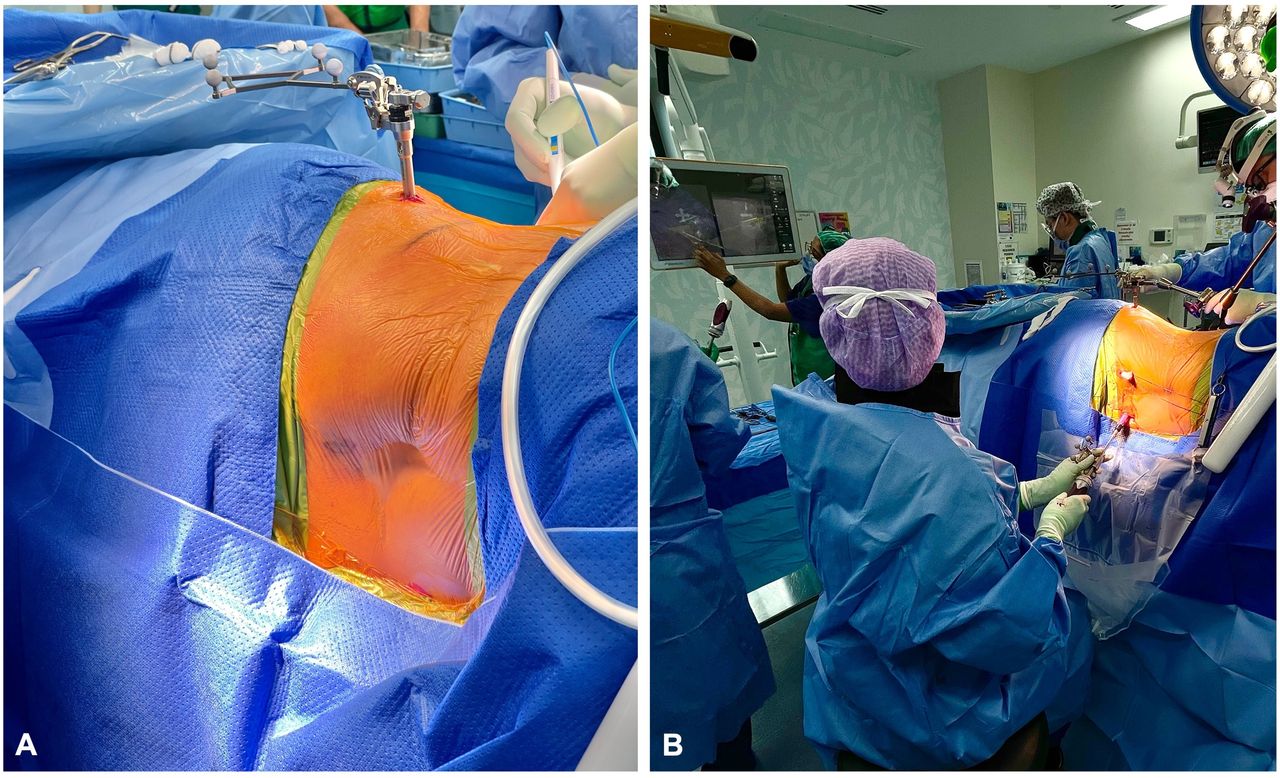
Patients were positioned in the lateral decubitus position on a radiolucent flat table and secured with silk tape with relevant pressure area care and axillary roll placement. The surgeon determined the side for positioning based on optimal factors related to patient pathology and side of symptoms, psoas anatomy, and vascular anatomy.9 To avoid restricting the surgeon’s ability to medialize the down-side screw, patients were positioned with their backs near the edge of the operating table. Electromyography leads were placed, and the patient was prepped and draped to allow simultaneous access to both the abdomen and posterior lumbar spine. PPSs were inserted utilizing computer-assisted navigation (Brainlab) registered with intraoperative 3D fluoroscopy. A patient reference array was attached to the iliac crest on the lateral margin to allow a line of site for instruments for anterior, lateral, and posterior procedures (Figure 1A). The tracking camera was placed at the foot of the operating table and oriented to allow line of sight of the instrument and patient arrays. Subsequently, a 3D fluoroscopic spin was performed, and data were transferred to the navigation system.

Intraoperative clinical photographs. (A) Lateral decubitus patient positioning with reference frame attached to the iliac crest. (B) Use of 3-dimensional computer-assisted navigation for placement of a percutaneous pedicle screw starting with the most proximal vertebra to be instrumented.
Navigated Wire Placement
Bilateral para-midline “Wiltse” incisions were marked using the navigation pointer. Following the skin incisions, fascial incisions were made in line with the skin incisions bilaterally. We assume that manipulation of the patient may cause slight movement of the vertebrae relative to the patient array in the iliac crest due to intervertebral motion. The susceptibility to error, therefore, increases with increasing time and increasing distance from the navigation frame. For this reason, we started with the placement of nitinol wires at the vertebra furthest from the navigation frame (most cephalad vertebra to be instrumented) to minimize potential inaccuracies with the navigation and proceeded in a caudal direction for all vertebral bodies to be instrumented (Figure 1B). Bilateral wires were placed in the cephalad vertebra prior to proceeding to the adjacent caudal vertebra. All wires were placed into the pedicles and vertebral bodies bilaterally prior to the use of a tap or screw insertion to allow for more accurate wire placement and ensure that if inaccuracies developed throughout the procedure, the accuracy would be maintained by “rail-roading” over the nitinol wires.
Jamshidi needles were positioned at a starting point located at the junction of the transverse process and lateral facet. The Jamshidi needle was placed via optimal trajectory through the pedicle to a depth of 30 mm. In certain cases, a navigated drill replaced the Jamshidi needle, especially in small pedicles (upper lumbar spine), sclerotic pedicles, or hypertrophic facet joints (Weishaupt grading ≥ 212) whereby skiving is more likely with a Jamshidi needle. Guidewires were inserted through the Jamshidi needles or navigated drill guide, which were then removed, leaving the wires in place. The wires were secured to the drapes on the cephalad side to prevent interference with the line of sight with the navigated instruments. Sequential dilators were placed over the guidewires, followed by tapping of the screw tracts and placement of cannulated screws over the wires, again starting with the most cephalad screws bilaterally and progressing caudally, similar to the sequence of wire placement. To prevent wire migration when passing instruments over the wires, the wires were always secured with the other free hand. Screw placement was confirmed via fluoroscopy, and thresholds were checked via triggered electromyography stimulation to assess for pedicle wall breaches.
Anterior Column Exposure
If ALIF was being performed, an anterior retroperitoneal approach through a paramedian incision was performed by a vascular surgeon concurrently with PPS placement, aiming to minimize operative time (Figure 2). Conversely, if LLIFs were utilized, they were placed via a standard lateral retroperitoneal approach13 following the placement of pedicle screws due to the requirement to drape in fluoroscopy. The screws were placed prior to any interbody work being performed to prevent unnecessary intervertebral motion or changes in alignment that would create inaccuracy in screw navigation. Following interbody cage placement, rods were percutaneously inserted on each side and secured to the screw heads with torque-limiting set screws.

Intraoperative clinical photograph demonstrating the operating room setup. The anterior exposure of the disc space is performed by the vascular surgeon on the right side. Simultaneously, the spine surgeon performs the percutaneous pedicle screw placement with 3-dimensional computer-assisted navigation, seen in the background. Each surgeon has their own scrub nurse.
Statistical Analysis
Statistical analysis was performed in a descriptive fashion. Numeric variables were expressed as mean (SD) or median (range) according to data distribution, and discrete outcomes were expressed as absolute and relative (%) frequencies. Normality was assessed with the Shapiro-Wilk test. The alpha risk was set to 5% (α = 0.05). Fisher’s exact test was used to compare breach rates between levels. Statistical analysis was performed with EasyMedStat (version 3.30; www.easymedstat.com) and GraphPad Prism (version 10.0.3).
Results
A total of 44 patients underwent L-SPS. The median age was 64.1 years, and there were 28 women and 16 men. Additional demographic details are provided in Table 1.
Demographics of study participants (N = 44).
Degenerative spondylolisthesis was the primary diagnosis in 54.5% of cases. Table 2 lists the indications for fusion, operative time, estimated blood loss, and LOS. Among the patients, 79.5% underwent ALIF only, 13.6% underwent LLIF only, and 6.8% received a combination of both ALIF and LLIF (Table 2). The most commonly treated level was L5/S1 (46.2%) followed by L4/5 (36.9%), L3/4 (10.8%), and L2/3 (6.2%; Table 2).
Treatment and procedural outcome measures (N = 44).
There were no intraoperative complications associated with pedicle screw insertion.
Pedicle Screw Assessment
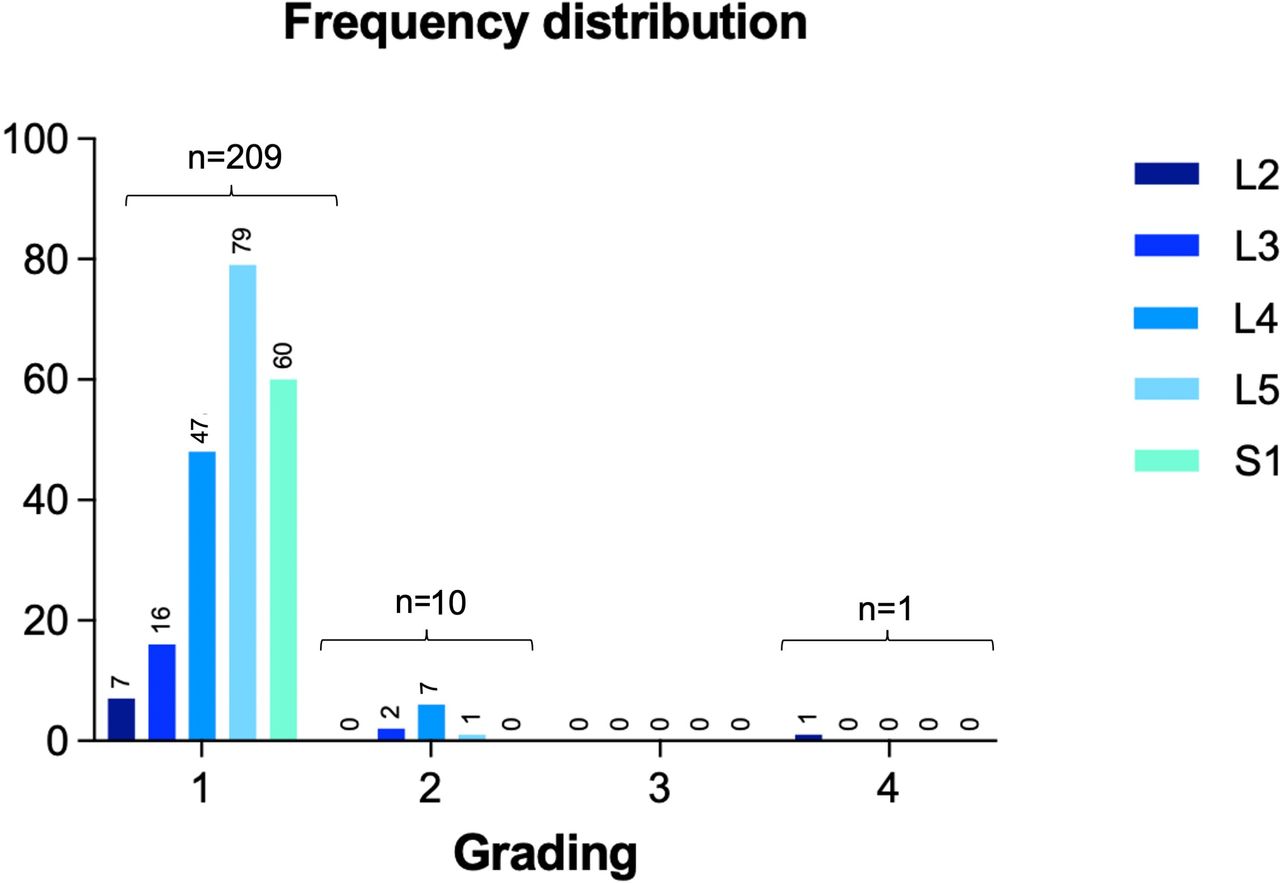
Eleven screw breaches were identified among 220 screws, accounting for 5%: 10 were Grade II breaches (<2 mm), and 1 was a Grade IV breach (>4 mm; Figure 3). These breaches were identified in 5 patients: 3 breaches were identified in 1 patient (3 of 6 pedicle screws) and 2 breaches were identified in another patient (2 of 4 pedicle screws). Taking into account a safe zone of 2 mm,14,15 only 1 screw (0.5%) exhibited a breach exceeding this threshold. All breaches were lateral. Of all breaches, 7/11 involved down-side screws indicating a trend toward the laterality of breaches for down-side pedicles (Table 3).

Frequency distribution of pedicle screws according to grading (Grades I–IV).
Lateral breach location as a function of pedicle orientation during instrumentation.
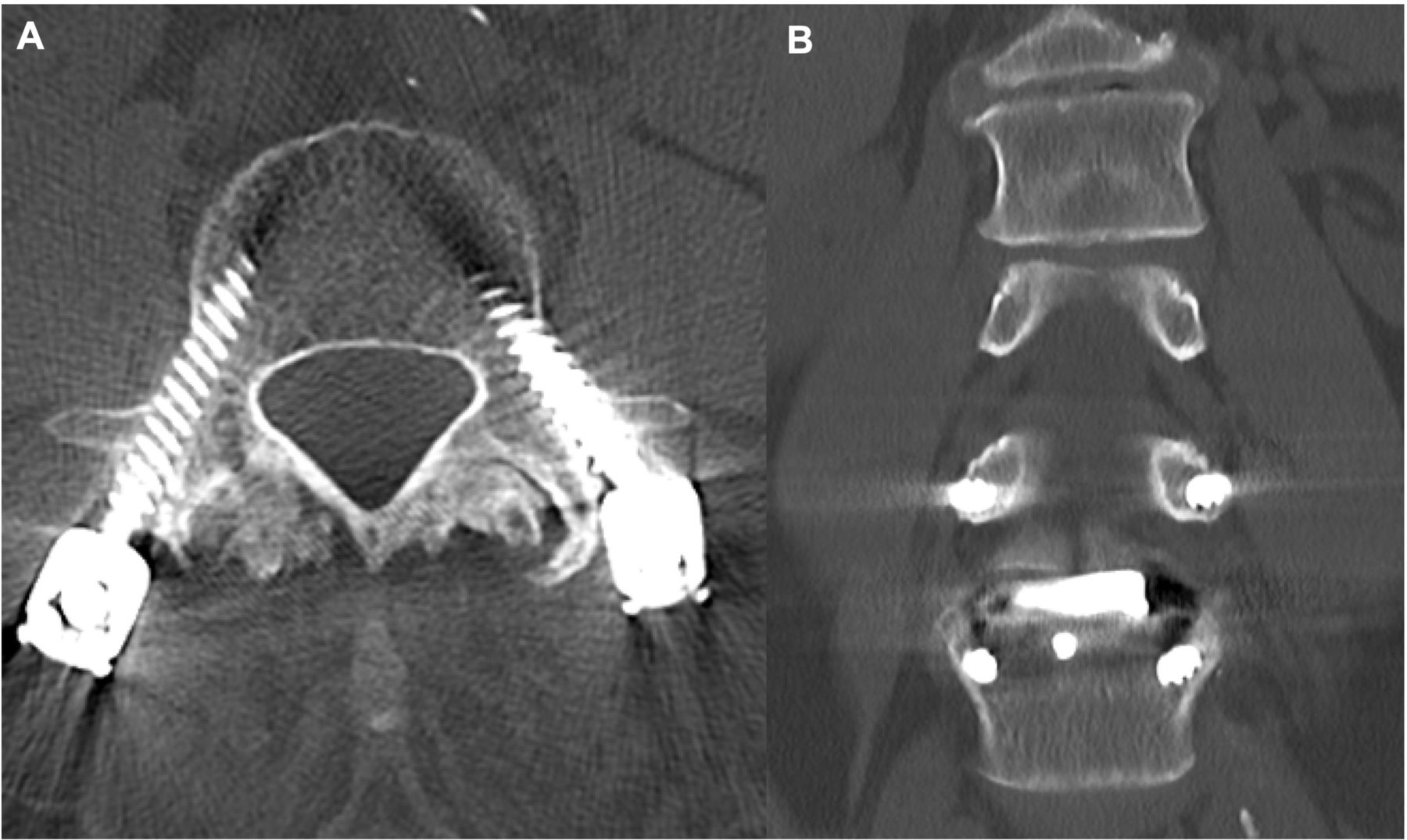
The Grade IV breach involved an up-side screw (1 of 4 up-side breaches). The Grade IV lateral breach involved an L2 pedicle and was due to a narrow “V-shaped” pedicle. The Grade IV breach was an intentional “in-out-in” technique given that the “perfect” pedicle trajectory would have resulted in facet joint violation (Figure 4: blue line).

Illustrative case with axial (A) and coronal (B) postoperative computed tomography images demonstrating a Grade IV lateral breach (orange line: 4.8 mm) of the left L2 pedicle due to pedicle orientation. Had the “perfect” pedicle trajectory been followed (blue line), facet joint violation would have been inevitable. The coronal view (B) demonstrates a narrow “V-shaped” pedicle on the left side.
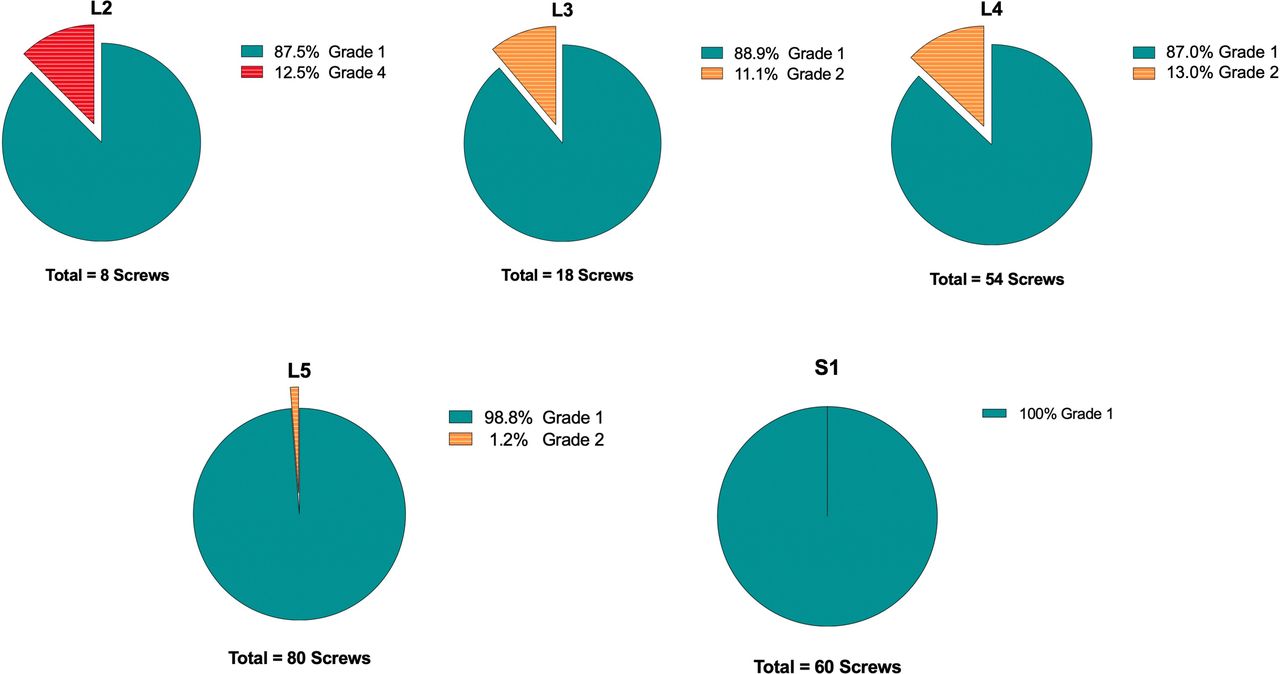
When analyzing breaches by level, 1.2% of screws at L5 exhibited a Grade II breach, 13.0% at L4, and 11.1% at L3 demonstrated Grade II breaches (Figure 5).

Pedicle screw breaches according to level.
A comparison of breach rates between levels showed significantly higher breach rates at L4 compared with L5 and S1 (P = 0.0043 and P = 0. 0073, respectively). No differences were found when comparing the other levels.
Hypertrophic facet joints were present in 6 of 10 screws with a Grade II breach, resulting in lateral screw deviation (Figure 6). No facet joint violations were noted.

Illustrative case with axial (A) and coronal (B) postoperative computed tomography images demonstrating a Grade II lateral breach of both L4 pedicles with hypertrophic facet joints at L3/4.
Discussion
This study demonstrates that PPS placement utilizing computer-assisted navigation in the L-SPS is both safe and accurate; breaches are rare, and when breaches do occur, they are lateral. An overall breach rate of 5% was found; considering a safe zone of 2 mm, only 1 screw (0.5%) demonstrated a relevant breach.
L-SPS has proven to increase surgical efficiency with improved perioperative metrics and reduced complications.9 Radiological outcomes, sagittal alignment parameters, and fusion rates of L-SPS have been extensively evaluated and compared with prone and “flip” techniques,8 but limited data exist on the accuracy of PPS placement using computer-assisted navigation in L-SPS. Posterior instrumentation remains a relevant barrier to the adoption of this novel technique.
In evaluating the published literature, a notable heterogeneity is observed in terms of grading schemes interpretation (eg, Grade I is defined as no breach in one study16 and as a breach in others),6,17 imaging methods, and screw insertion techniques used to evaluate pedicle screw accuracy. Ouchida et al16 reported a 1.8% misplacement rate for PPS in 228 screws undergoing L-SPS. In this study, only pedicle screws with a breach greater than 2 mm were considered malpositioned, which puts their results in a more favorable light. The present study demonstrated a 0.5% rate of breach by >2 mm, compared with 1.8% reported by Ouchida et al.16
The overall reported pedicle screw breach rate, considering different screw insertion techniques and different imaging methods reported in the literature, ranges from 1.5% to 14.3%.4,6,18–23 However, so far, only 3 other studies16,17,24 have analyzed pedicle screw positions on CT images after computer-assisted PPS placement in L-SPS (Table 4). Okuda et al17 analyzed two patient cohorts based on intraoperative positioning and reported pedicle wall breach rates of 4.6% in the lateral decubitus position and 4% in the prone position, which is comparable to the current study. In our study, hypertrophic facet joints were present in 6/10 screws with a Grade II breach, resulting in lateral screw deviation (Figure 5). In one case in the current series, a Grade II breach was intentionally chosen due to the small size of the pedicles. An in-out-in technique was used to obtain a satisfactory screw purchase. Although neural structures are situated within 2 mm of the pedicle,25 clinically relevant issues tend to arise with larger breaches and medial or caudal breaches. We did not identify any medial or caudal breaches in our study, whereas Okuda et al17 reported 3 (14.3%) medial breaches. Focusing on the cases of significant breaches (Grades III and IV), Okuda et al17 reported a rate of 2.2% compared with 0.5% in our study. Possible reasons, such as facet hypertrophy or pedicle dimensions for these breaches, were not evaluated in their study.
Published rates of percutaneous pedicle screw accuracy in lateral decubitus single-position anterior-posterior surgery assessed by computed tomography.
Hiyama et al24 analyzed 728 pedicle screws and reported a breach rate of 1.9%, which is lower than in the present study. However, their rate of significant breaches was higher (1.2% vs 0.5%), and the breach laterality, which is of great interest, was not assessed.
The current study further examined the laterality of breaches in relation to the pedicle’s position relative to the floor during instrumentation. A tendency for breaches to occur on the down-side pedicles was observed. This observation aligns with the findings of Okuda et al,17 who similarly observed a trend toward lateralization of down-side screws, attributing it to the patient’s orientation relative to the operating table. This problem can be considered one of the technical challenges with SPS and should be anticipated. Patients should be positioned with the posterior aspect of the lumbar spine approximately 2 inches from the edge of the operating table to avoid interference with instruments when performing the down-side PPS placement trajectory.8,26 Interestingly, body habitus does not seem to play a role in screw deviation, as no significant differences in body mass index were found between patients with and without a breach.
No clear pattern was discernible in the frequency of breaches per level in relation to the distance from the navigation frame: S1: 0%, L5: 1.2%, L4: 13%, L3: 11.1%, and L2: 12.5%. It is possible that the low number of screws in more cephalad levels and smaller pedicle diameters may contribute to these differences in accuracy rates; however, due to our current sample size, we only found statistically significant differences between L4 and S1 and between L4 and L5. Accuracy was excellent at S1 and L5, most likely due to the limited motion between the navigation frame and the screw, which seems to improve accuracy. However, no screws required revision at any vertebral levels, nor were there any neurological complications or pedicle fractures observed.
In one case, a Grade IV breach was noted referring to an intentional in-out-in trajectory in an L2 pedicle with a narrow “V-shaped” pedicle (Figure 4). Had the “perfect” pedicle trajectory been followed, facet joint violation would have been inevitable, potentially accelerating adjacent segment degeneration and increasing the likelihood of revision. Furthermore, from a biomechanical point of view, we believe that the decision to use an in-out-in trajectory was better than instrumenting pedicles unilaterally in this construct. While this was graded as an inaccuracy, given the surgeon’s intention to treat, the authors believe that this inaccuracy should not be considered a result of the navigation technology.
Overall, the accuracy rate of the PPS technique in L-SPS is consistent with the existing literature, but the precision of the technique described here appears to be higher. The authors believe that wire placement, and the sequence of doing so, is the reason for better precision due to reducing intersegmental motion and providing a safe “rail-road” for the tap and screw later in the procedure where inaccuracies may be magnified.
There are several potential limitations to this study resulting from its retrospective, single-cohort design and constrained duration of postoperative follow-up. The study assumes accuracy purely by the amount of pedicle breach; however, given anatomical constraints, surgeons may choose a trajectory with a small breach to account for hypertrophic facets, to avoid facet joint violation, or to optimize screw length. The only true way to truly assess accuracy would be to assess the final screw position compared with the planned screw orientation, which was beyond the scope of this study. Owing to the study’s design focusing on a single cohort and a single-surgeon practice external validity is not necessarily implied. However, it does allow for a standardized technique to reference.
Conclusion
PPS placement utilizing computer-assisted navigation in L-SPS is both safe and accurate. An overall breach rate of 5% was found; considering a safe zone of 2 mm, only 1 screw (0.5%) demonstrated a clinically relevant pedicle breach.
Footnotes
Funding No funding was received for the present study.
Disclosures Aaron James Buckland has received royalties or licenses from NuVasive, Evolution Spine, and Altus Spine and consulting fees from NuVasive. The remaining authors have nothing to disclose.
Disclaimer The authors, their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.