


Abstract
Background Computerized navigation improves the accuracy of spine procedures. However, intraoperative imaging is plagued by ionizing irradiation and its cancer risk. Advanced technologies attempt to optimize the radiation dose. The goal of this study was to compare radiation exposure and screw accuracy of O-arm navigation and the Surgivisio device (SD) in pedicle screw insertion.
Methods All patients operated on by navigated pedicle screw insertion during a 19-month period were prospectively included in 2 spine centers: the first with the O-arm and the second with the SD. Demographic, operative, and irradiation data were collected. The accuracy of the screw positioning was assessed using the Heary and Gertzbein classifications. The effective dose in millisievert (mSv) was calculated.
Results One hundred patients were included, 50 per group. Five hundred and twelve screws were inserted, among them 228 in 120 vertebrae with the O-am and 284 in 145 vertebrae with the SD. Screw accuracy was 99.1% with the O-arm vs 93.3% with the SD (P = 0.07). Operative times were similar, with 145 vs 139 minutes respectively, P = 0.68. The effective dose was significantly higher in the O-arm group, with 5.43 vs 2.70 mSv with the SD (P < 0.01). The effective dose related to 2-dimensional imaging was significantly lower in the O-arm group than in the SD group, with 0.26 vs 1.16 mSv, respectively, P < 0.01, related to a shorter imaging duration (4 vs 109 seconds respectively, P < 0.01).
Conclusions Accuracy of pedicle screws was higher with the O-arm than with the Surgivisio, but the latter showed less radiation exposure. Despite promising results, improvements in technology should be pursued for ergonomics and surgical safety.
Level of Evidence 4.
Introduction
Pedicle screw insertion, first described in 1970 by Roy-Camille et al1 and modified by Steffee2 and Cotrel and Dubousset,3 is a procedure regularly performed in spine surgery in deformity, degenerative, tumorous, inflammatory, infectious, or traumatic conditions when the spine needs posterior stabilization or correction of deformity. Several techniques allow the insertion of pedicle screws, such as the “free-hand” technique, the open or percutaneous technique under 2-dimensional (2D) or 3-dimensional (3D) imaging with computerized navigation, or, more recently, robotic guidance.4 Navigation offers confidence and ergonomics during the surgery, with more accurate procedures5 in comparison with fluoroscopic guidance.6 However, intraoperative imaging devices currently use x-ray technology, with a cumulative associated cancer risk,7 named “stochastic risk.” This risk can be estimated through the effective dose (E) in millisieverts (mSv). New technological advances tend to optimize irradiation related to imaging devices.8 The O-arm imaging system (Medtronic, Minneapolis, MN, USA) has been known since its first use at the University College of San Francisco Medical Center in 2006,9 with numerous publications so far. The Surgivisio device (SD; eCential robotics, Gières, France) was first used to perform spinal procedures in 2017.10 O-arm with navigation11–13 and Surgivisio10,14,15 showed good accuracy during spine procedures and good postoperative results. Besides, a recent comparative study between these 2 devices in percutaneous cementoplasty found that the O-arm delivered higher radiation exposure in comparison with the SD, as well as higher operative time, although image quality and radiological results were better with the O-arm. Thus, the authors highlighted the need to perform further evaluation in other spinal procedures.16
The objective of the present study was to compare the radiological results and irradiation of posterior pedicle screw insertion performed under O-arm navigation or under SD guidance. The hypotheses were that considering the more recent SD, O-arm produces more irradiation but reaches a similar rate of satisfactory screw positioning as the SD, which is expected to be between 89% and 100% according to Gelalis et al.17
Methods
Participants
During a 19-month period, we prospectively included all consecutive cases of pedicle screw insertion procedures performed at 2 locations: at a private clinic with a spine fellowship program with the use of the O-arm (1 senior and 1 junior spine surgeons), and at a university hospital with the use of SD (3 senior and 2 junior spine surgeons). Inclusion criteria were (1) age 18 years or older and (2) presenting with an unstable fracture or a degenerative spine condition that required posterior spondylodesis by pedicle screw insertion. Exclusion criteria were (1) younger than 18 years, (2) refusal to participate, (3) pregnancy patients, and (4) vulnerable patients unable to give consent.
Study Design
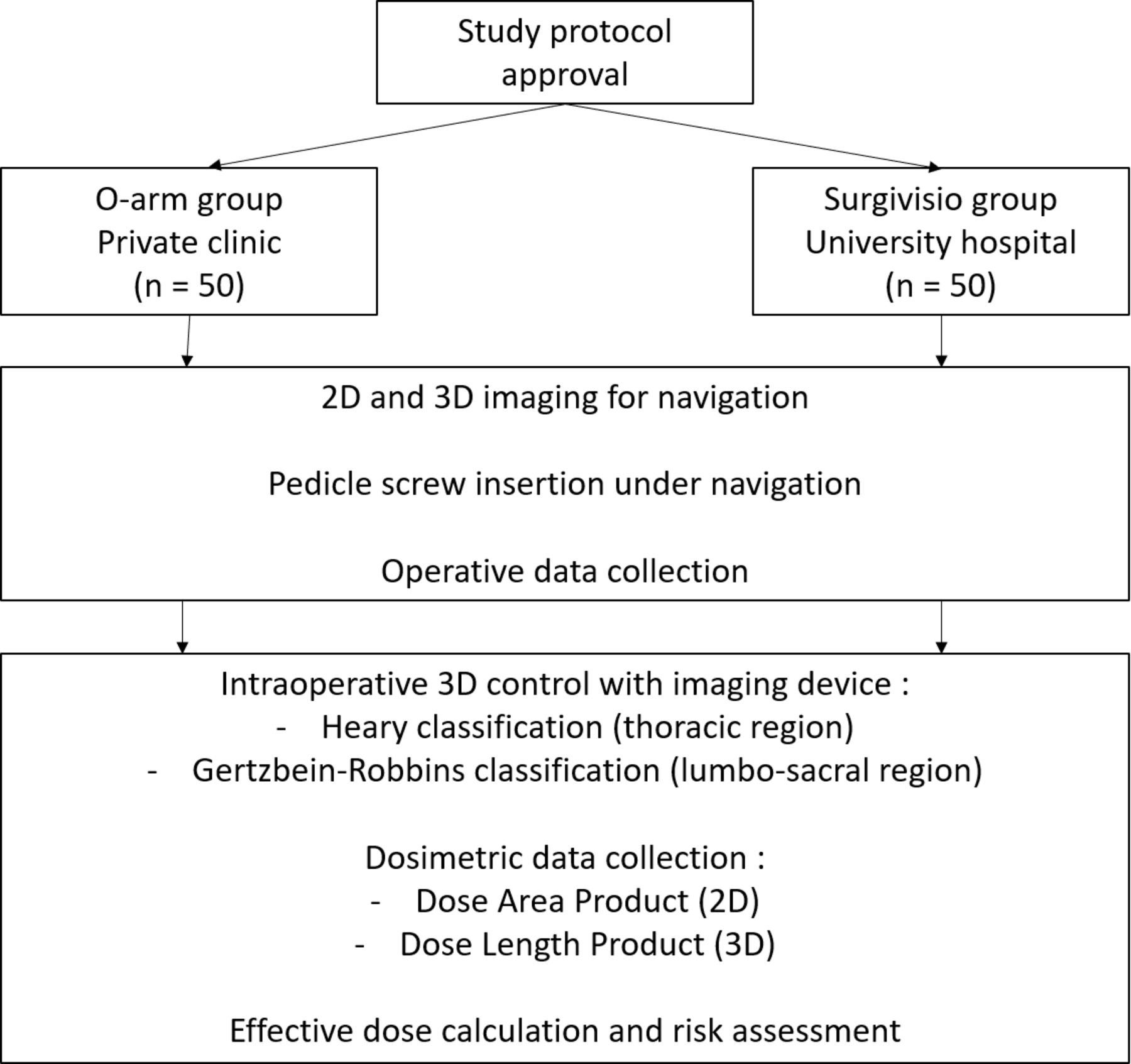
Study design was prospective (Figure 1).

Patient flow diagram. 2D, 2-dimensional; 3D, 3-dimensional.
Ethical Statement
The study was performed in accordance with the Declaration of Helsinki (1964). The ethical commission of the Vaud canton approved the research protocol (No. 2021–00298). All patients provided written consent for participation in the study.
Interventions
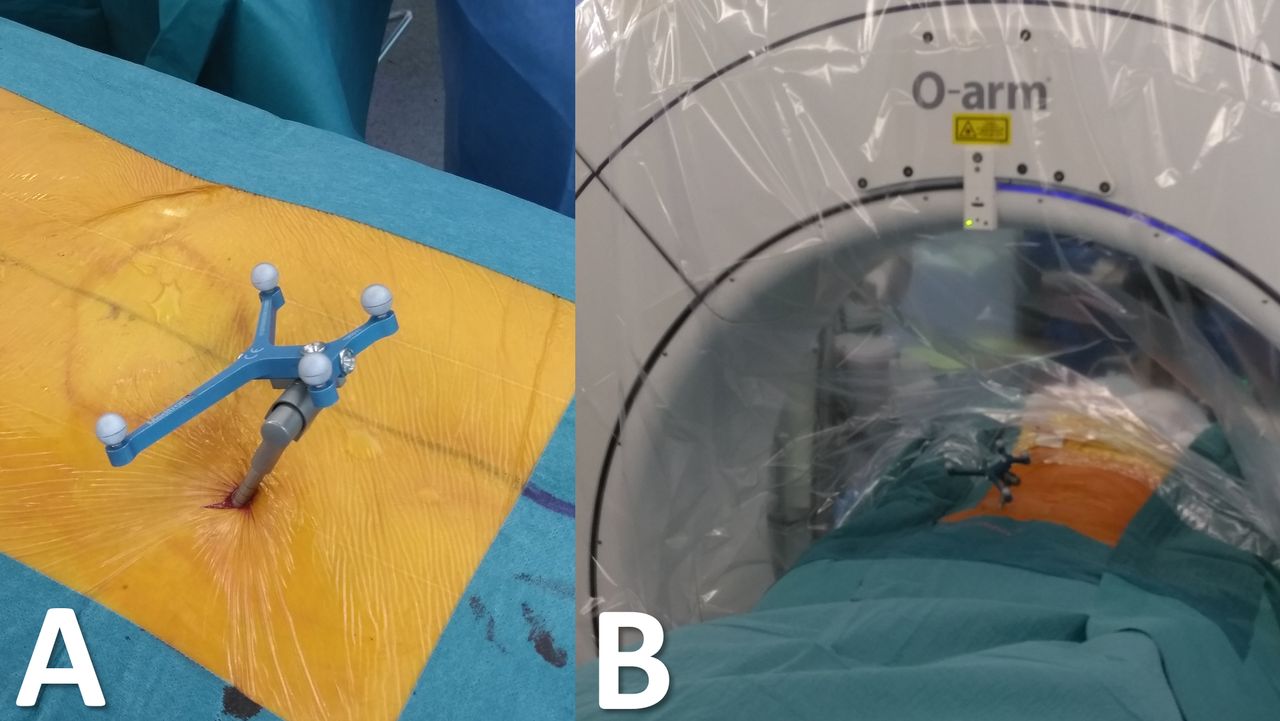
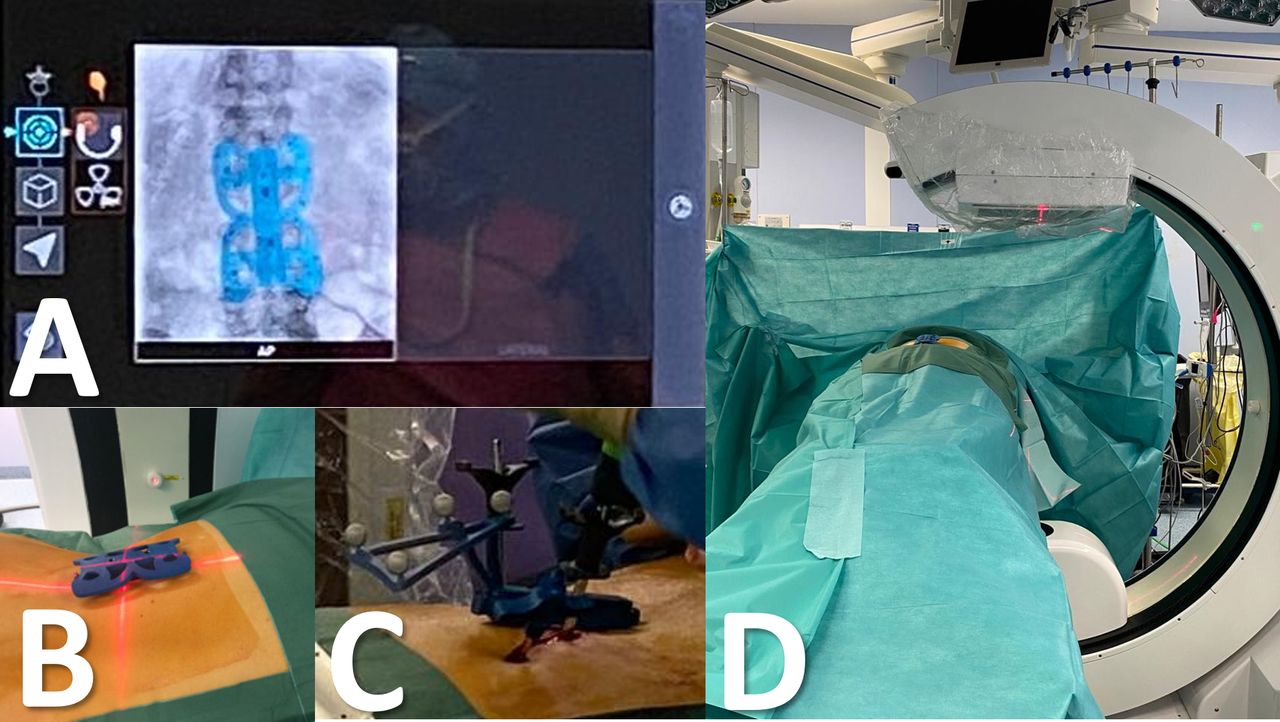
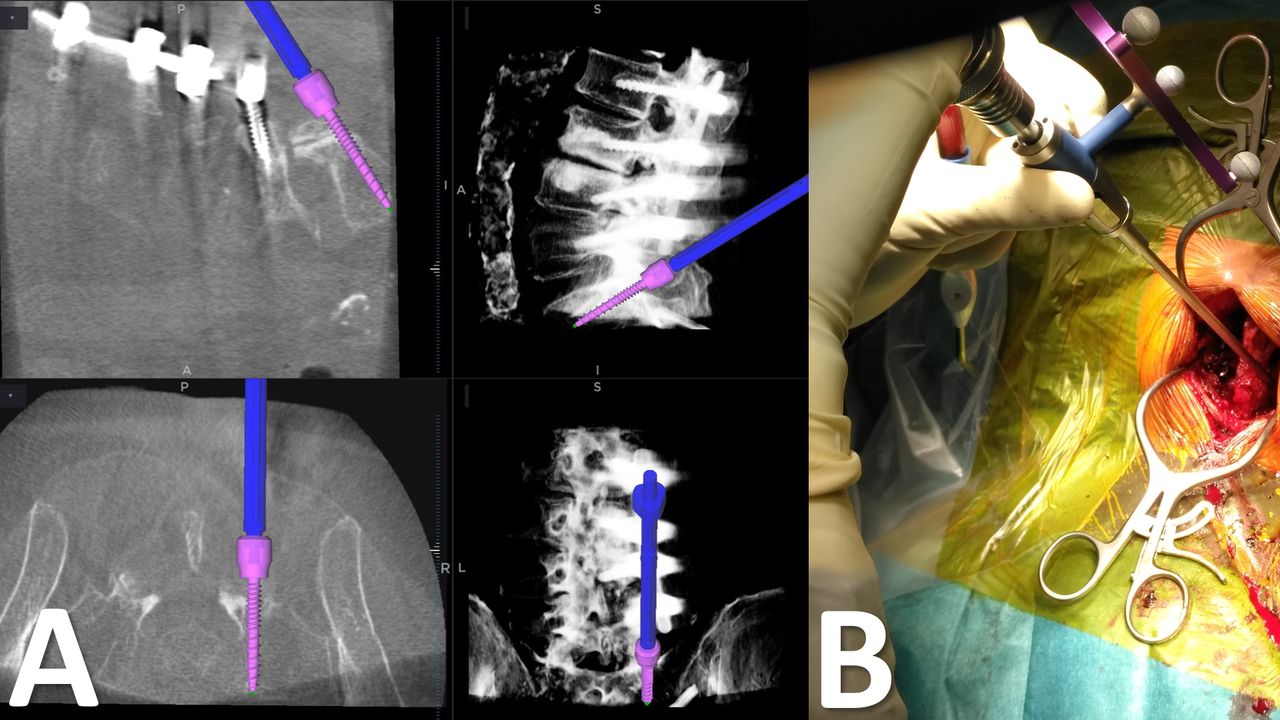
For both groups, patients were operated on in a supine position under general anesthesia and after antibiotic prophylaxis. For the O-arm group (OG),16 a pin was introduced in the posterior iliac crest with the patient frame attached (Figure 2). 2D acquisitions for vertebral level landmarking were performed. Then, while the detection camera could reach the patient frame and detectors on the O-arm machine (Figure 2), a 3D acquisition could be performed under apnea, and the images were transmitted to StealthStation navigation (Medtronic, Minneapolis, MN, USA). For the Surgivisio group (SG), the patient frame was attached using 2 to 4 Kirschner wires introduced in the spinous processes in the area of the vertebrae to be operated.15,16 2D fluoroscopic landmarking was performed (Figure 3). When detection of all detectors inside the patient frame was reached in an anterior-posterior view, a lateral view was performed. After anti-collision rotation of the SD gantry, the 3D acquisition (90 or 180 images) could be performed. For both machines, operating room personnel could leave the operating room during 3D acquisition, avoiding unnecessary irradiation. Then, open approach and pedicle screw insertion under O-arm navigation could be performed (Figure 4) or percutaneous or open navigated screw insertion with the SD using a navigated Jamshidi needle for drilling and transpedicular Kirschner wire insertion (Figure 5). The percutaneous approach was preferably chosen thanks to the use of cannulated screws, but if a vertebral osteotomy was needed,18 an open approach was performed.

Intraoperative views of the O-arm setup. (A) Standard drape with a patient frame inside the posterior iliac crest for navigation. (B) Infrared detectors on the O-arm machine.

Intraoperative views of the Surgivisio setup. (A) Anteroposterior radiograph, which was taken with the detector placed on the patient (B). (C) The detector is replaced by the patient frame, allowing navigation procedures. (D) Setup of the Surgivisio device for imaging acquisitions.

Intraoperative views of an instrumentation extension at the S1 level using the O-arm guidance. (A) Screen of the StealthStation with the 3-dimensional scan of the patient on sagittal and axial views, the navigated tool (in this case the screwdriver) and the screw with its determined length and diameter. (B) Intraoperative view of the navigated screwdriver during pedicle screw insertion.

Intraoperative views of a Surgivisio procedure for pedicle screw insertion. (A) Screen of the Surgivisio, displaying the 3D scan of the patient with the trajectory of the navigated Jamshidi needle. (B) Nitinol threads for percutaneous pedicle screw insertion performed under Surgivisio guidance.
Data Collection
Demographic data, such as age (in years), gender, height (in cm), and weight (in kg), were collected. Surgical data were also recorded, such as the level and number of operated vertebrae and the operative duration from incision to closure (in minutes). We also collected irradiation data from the dosimetric report such as the 2D imaging duration (in seconds), the dose-area product (DAP; in mGy.cm2) of the SD and of the 2D O-arm fluoroscopy, and the dose-length product (DLP; in mGy.cm) from the O-arm in 3D mode at the end of the surgical procedure. Body mass index was calculated using height and weight. Screw accuracy was assessed by 2 independent observers on the postoperative computed tomography or 3D O-arm scan according to the Gertzbein-Robbins classification19 for the lumbar spine and the Heary classification20 for the thoracic spine. A placement was considered acceptable if it corresponded to grades A or B according to Gertzbein-Robbins and grades I or II13 according to Heary.
Radiation Exposure Calculation
E in mSv was calculated using the DAP and the operative field dimensions, with weight and height of the patient, through a Monte Carlo simulation using the PCXMC 2.0 software (STUK, Helsinki, Finland),21 using parameters described in the dosimetric study of Rousseau et al.22 3D-related E (E 3D) was calculated with the DLP according to the European Guidelines for Multislice Computed Tomography23 using the corresponding conversion factor k (in mSv/mGy.cm) related to the irradiated region. For the thoracic region, k was 0.014. For the lumbar region and the whole trunk, k was 0.015. The calculation formula was E 3D = DLP × k. For the approximate calculation of E related to 2D (E 2D) irradiation, we also utilized conversion factors w (in mSv/[Gy.cm2]) according to the European Commission report Nr. 182,24 with w of 0.19 and 0.26 for the thoracic and lumbar spine, respectively, considering a calculation formula of E 2D = DAP × w. We also compared these results with those obtained with PCXMC. The absolute risk of radiation-induced cancer (AR, in %) equivalent to a whole-body acquisition was calculated from E, considering a value of 5% per Sv.25
Outcomes
The main outcomes were the acceptability rate of screw positioning and the overall E. Secondary outcomes included operative and imaging durations, E 3D and E 2D, and AR.
Statistical Methods
Statistical analyses were performed using R software,26 v.3.1.3. Student t test was used for comparison of numerical variables. Fisher’s exact test was used for binomial comparison. A Pearson’s correlation was used to determine the association between quantitative variables. A threshold of ≤0.05 was defined as a statistically significant difference. The number needed to treat was calculated for a power of 90% and an alpha risk of 5% with a mean difference of 1 mSv and found 48 patients per group, for a total minimum of 96 patients.
Results
Demographic Data
One hundred patients were included, 50 in each group. The groups were comparable in terms of gender and body mass index but significantly older in the OG than in the SG (P = 0.02). Summarized data are available in Table 1.
Demographics of patients undergoing pedicle screw insertion.
Operative Data
A total of 512 screws were inserted, among them 228 screws in 120 vertebrae for the OG, and 284 screws in 145 vertebrae for the SG. Operative time was similar between the groups, with a mean of 145 minutes in OG vs 139 minutes in SG (P = 0.68). For the operative time per level and per screw, the duration was significantly higher in the OG than in the SG, with 71 vs 53 minutes (P = 0.02) and 39 vs 27 minutes (P < 0.01), respectively. More procedures were performed by open approach in OG in comparison with SG (P < 0.01). There were also 46% of revision surgeries in OG vs 14% in SG (P < 0.01). The mean number of instrumented vertebrae was 2.4 in the OG and 2.9 in the SG (P = 0.02). Operative data are detailed in Table 2.
Operative data of patients undergoing pedicle screw insertion.
Screw Accuracy
In the OG, 38 screws were placed in the thoracic and 190 in the lumbar spine. For the thoracic spine, according to the Heary classification, 36 were grade I, 1 grade II, 0 grade III, and 1 grade IV; 97.4% were rated as acceptable and 2.6% as poor. For the lumbar spine, according to the Gertzbein classification, 179 were grade A, 10 grade B, 1 grade C, and 0 grades D and E; 99.1% were rated as acceptable and 0.9% as poor.
In the SG, 82 screws were inserted in the thoracic and 202 in the lumbar spine. For the thoracic spine, according to the Heary classification, 58 were grade I, 14 grade II, 4 grade III, and 6 grade IV; 87.8% were rated as acceptable and 12.2% as poor. For the lumbar spine, according to the Gertzbein classification, 170 were grade A, 23 grade B, 3 grade C, 2 grade D, and 4 grade E; 95.6% were rated as acceptable and 4.4% as poor. Five screws were removed intraoperatively because of poor bone purchase. No screw was postoperatively revised in either group, considering the uncompromised stability of the instrumentation and the absence of postoperative neurological complications. The results are detailed in Table 3. Clinical grading for thoracolumbar spine instrumentation showed an overall acceptable rate of screw positioning of 99.1% for the OG vs 93.3% for the SG (P = 0.07). For the thoracic spine, this rate was 97.4% in the OG vs 87.8% in the SG, a significant difference (P = 0.03). For the lumbar spine, the rates were 99.5% and 95.6%, respectively (P = 0.12).
Classifications for thoracolumbar pedicle screw fixations.
Radiation Exposure
Overall E was significantly higher in the OG than in the SG, with a mean of 5.43 vs 2.70 mSv, respectively (P < 0.01). The same trend was found for the E per level: 2.65 vs 1.02 mSv, respectively (P < 0.01). E 3D was significantly higher in the OG, with a mean of 5.17 vs 1.54 mSv in the SG (P < 0.01). The same effect was observed for the E per 3D acquisition: 4.79 vs 0.90 mSv, respectively (P < 0.01). E 2D, on the contrary, showed a significant difference between OG and SG with 0.26 and 1.16 mSv, respectively (P < 0.01). The comparison between E 2D calculated with PCXMC and with the European Commission w conversion factors found similar results: 0.26 vs 0.30 mSv, respectively, for the OG (P = 0.50), and the same trend for the SG, with a mean of 1.16 vs 1.05 mSv, respectively (P = 0.64). In the OG, fewer 3D acquisitions were performed than in the SG: a mean of 1.1 acquisitions per patient vs 1.6, respectively, with a significant difference (P < 0.01). For the 2D fluoroscopic duration, an average of 4 seconds for the OG and 109 seconds for the SG were observed, a significant difference (P < 0.01). Mean AR was 2.7 × 10–4 % in the OG vs 1.4 × 10–4 % in the SG, a significant difference (P < 0.01). Irradiation data are detailed in Table 4.
Radiation exposure for screw implantation.
Correlation Study
In the OG, a strong association was found for E and age, E and imaging duration, E 2D and imaging duration, and for E 2D and E 3D (P < 0.01). In the SG, a strong association was only observed for E 2D and E 3D (P < 0.01). In the whole series, including the 2 groups, a strong association was only found for E and imaging duration (P < 0.01). Pearson’s correlation study findings are summarized in Table 5.
Pearson’s correlation study between radiation exposure and other variables.
Discussion
The most important finding in this study was the superiority of the O-arm in terms of accuracy for pedicle screw insertion and its higher radiation exposure in comparison with the Surgivisio. The hypothesized accuracy of between 89% and 100% was reached for both devices.
The accuracy of pedicle screws using the O-arm was assessed by Farah et al,13 who found a 90.8% rate of acceptable screw placement on 11 patients, less than the results of the current study. Boudissa et al published about percutaneous pedicle screw insertion using the SD15 and found a 95% rate of acceptable screw positioning. This result was higher than the current study for the SG. However, in this study, the authors considered acceptable results for Heary grade ≤III, with a 6% rate of screws rising the overall satisfactory rate, whereas in the current study, a Heary grade ≤II was considered acceptable.13 More recently, Saad et al published a retrospective study on screw accuracy with the SD with 648 screws on 97 patients.27 They found an accuracy rate of 92.4%, which was slightly inferior to the current study for the SG, but with a higher number of screws inserted. The authors concluded that the displacement of the patient frame may be a potential major cause of navigation failure leading to screw misplacement. Tian and Xu published a meta-analysis about 7533 pedicle screws28 and reported a mean 90.8% accuracy rate for the in vivo computed tomography-based navigation group. Several authors showed an accuracy rate of the O-arm between 92% and 97.5%,29–31 which was slightly lower than that in the current study. Besides, Sun et al performed a literature review and meta-analysis32 on 20 studies about O-arm–based navigation vs free-hand technique, with 1422 patients and 9982 pedicle screws, among them 4797 screws inserted with the O-arm. The authors highlighted that navigation was associated with a significantly higher accuracy of pedicle screws (odds ratio of 2.45, P < 0.05) in comparison with the free-hand technique.
The difference between the rate of acceptable screws between O-arm and Surgivisio may be explained by several factors. First, more percutaneous procedures were performed in the SG, leading to less sensory feedback on the hand during screw insertion. Second, more thoracic screws were inserted in the SG, and there was a higher rate of misplaced screws (1 Heary IV in the OG vs 10 Heary ≥III in the SG) as well, significantly higher than the rate of the OG, with a significantly lower operative time per level and per screw in the SG, considering the average greater number of screws inserted per procedure. No difference was observed between the groups in the lumbar region. Users of the Surgivisio raised a technical issue related to the device. The procedure requires the insertion of cannulated screws, with a high risk of toggle leading to potentially misplaced screws and poor bone purchase, especially in the thoracic region where pedicles are shorter and thinner than in the lumbar region. Furthermore, the navigated trocar is bevel-ended, which may cause it to slip against the pedicle, whereas the PAK Needle has a conical extremity. Besides, the software of the StealthStation allows visualization of the trajectory of all navigated instruments as well as the simulation of the screw length, diameter, and shape during its progression through the vertebra (Figure 4). These results may encourage the industry to improve the software and the navigated devices of the SD.
Boudissa et al also published about radiation exposure15 of the Surgivisio during pedicle screw insertion on 29 patients and found a mean E of 1.97 mSv, thus a lesser irradiation level than both groups of the current study. Saad et al27 reported from their series of 648 screws implanted with the Surgivisio a mean E of 1.84 mSv, also slightly less than in both groups of the current study. The study from Farah et al13 comparing the O-arm and the AIRO (Brainlab AG, Germany) devices found a mean E of 3.52 and 15.6 mSv, respectively. They also found an average E per navigated vertebra of 1.04 and 3.9 mSv, respectively. These results were inferior to those of the current study for the O-arm but higher than those of the SD.
Differences in radiation exposure between the O-arm and SD may be explained by technological aspects. The O-arm is a 2D and 3D cone beam computed tomography. The Surgivisio machine is a 2D and 3D C-arm. Both devices use plan detectors as imaging technology. However, the O-arm can create a 3D acquisition with the delivery of 192 images, whereas the Surgivisio could perform 180 or 90 images for a whole 3D acquisition, explaining higher E 3D in the OG. Higher E 2D and imaging duration with the SD can be explained by the fact that the surgeon can navigate the entry point and the trajectory of the screw until the insertion of a nitinol thread. The progression of the screw cannot be navigated, and more fluoroscopic controls were required with the SD. However, significantly higher E 3D with the O-arm may encourage the industry to continue improving imaging technology in favor of dose optimization.
According to the optimization principle of “as low as reasonably achievable,”33 several possibilities remain to decrease the dose. For the O-arm, using the low-dose or standard modes in 3D, the low-dose mode in 2D, limiting the number of 3D/2D acquisitions, and finally using the navigation on the field of view34 may help to decrease the overall dose. For Surgivisio, using the 90-image 3D acquisition mode and limiting the number of 3D and 2D acquisitions may also decrease the overall dose.
Limitations
There were some limitations in the present study. First, the E calculation is an estimation using standard and specific measurements for the Monte Carlo simulation. There was a calculation bias in the dose estimation because we could not intraoperatively measure the exact focus to skin distance in clinical practice, considering this distance being modified during the surgery and even more during the 3D acquisition with the Surgivisio. For reproducibility purposes, we considered the settings of the software described by Rousseau et al.22 Second, differences in the accuracy of pedicle screw insertion with the Surgivisio may also be explained by a learning curve effect, considering the first experience since 2017 in comparison with the O-arm being used since 2012 at the clinic. Indeed, Rivkin and Yocom emphasized the importance of the learning curve in pedicle screw insertion.35 Finally, 2 different locations and teams for 2 different intraoperative imaging use may have biased the accuracy of results.
Conclusion
Technological advances in intraoperative imaging with the Surgivisio showed a clear dose reduction for the patient during 3D-navigated pedicle screw insertion. However, it was associated with a higher rate of misplaced screws than the O-arm, especially in the thoracic region, where more screws were inserted and more percutaneous procedures were performed—even though both devices reached the expected acceptability of screw accuracy. Despite a learning curve with promising results, these findings highlight the need to pursue further improvement of intraoperative imaging technologies.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Maxime Saad reports being a consultant for eCential Robotics in 2022 and receiving payment and travel support for presentations done at SFCR and Eurospine Congresses in 2022. Gaël Kerschbaumer reports consulting fees from eCential Robotics. Additionally, Marc Prod’homme reports receiving a traveling grant from AO Spine for the Global Spine Congress 2023 and accommodation funding from AO Spine for the AO Spine Fellowship 2025. Guillaume Cavalié reports consulting fees from eCential Robotics and support for attending meetings/travel from Sanofi and Depuy Synthes. Jerome Tonetti reports royalties/licenses from Spineart SA, consulting fees from Spinem, support for attending meetings/travel from Leopharma, and stock/stock options from eCential Robotics and Spineart SA. Mehdi Boudissa reports consulting fees from eCential Robotics and Clariance, payment/honoraria from FH Ortho, and support for attending meetings/travel from Stryker. Jean-Loup Gassend reports royalties from a book (Autopsy of a Battle). Maxime Saad, Arun Thangavelu, and Didier Grasset have nothing to disclose.
Ethical Standards The procedures followed were in accordance with the ethical standards of the responsible committees on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. The ethical commission on human research of the Vaud canton approved the research protocol (No. 2021-00298).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.