


Abstract
Background Body mass index (BMI) serves as a risk factor for complications and poorer outcomes following anterior cervical discectomy and fusion (ACDF). This study investigates the association between BMI and Patient Reported Outcomes Measurement Information System physical function (PROMIS-PF) following ACDF.
Methods A prospectively maintained surgical registry was retrospectively reviewed for cervical spine surgeries between 2015 and 2019. Included patients underwent elective primary, single, or multilevel ACDF and were excluded for missing preoperative PROMIS-PF. Patients were stratified into 4 groups based on BMI score. Associations of demographic and perioperative characteristics with BMI groups were analyzed using either χ2 test or t test. PROMIS-PF was evaluated preoperatively and 6 weeks, 12 weeks, 6 months, 1 year, and 2 years postoperatively using linear regression. Delta improvement in PROMIS-PF was evaluated at all time points.
Results The 128 study cohort had 74 patients the nonobese, 27 in the Obese I, 19 in the Obese II, and 8 in the Obese III groups. The mean age was 50.0 years and 57.0% were male. Gender, diabetic status, and Charlson Comorbidity Index (CCI) significantly differed by BMI groups but did not differ by perioperative characteristics. Preoperative PROMIS-PF did not significantly differ by group. Obese II and III groups had decreased PROMIS-PF compared to Obese I and nonobese groups at 1 year and 2 years. BMI groups had significantly different delta improvement at the 12 weeks (4.1 vs 10.1 vs 1.8 vs 4.3; P = 0.044) and 2 years (9.9 vs 7.1 vs 2.3 vs 3.0; P = 0.048).
Conclusion Among the assessed BMI subgroups, all experienced similar physical function scores during the preoperative and short-term time points. Patients with higher BMI demonstrated diminished physical function at long-term time points. While this study focused on evaluating obesity, longitudinal tracking of high-risk patients during the postoperative period remains important for optimal rehabilitation.
Level of Evidence 4.
Clinical Relevance High BMI may predispose patients to lengthier recovery of physical function following ACDF.
INTRODUCTION
Obesity is a growing health issue within the United States with a reported 42.4% of adults suffering from this epidemic.https://paperpile.com/c/NUwmG6/RFNs5 As compared to 30.5% a decade ago, its prevalence has progressively increased to levels that classify it as an epidemic.https://paperpile.com/c/NUwmG6/xGY9z Defined as a body mass index (BMI) greater than 30 kg/m2, obesity is a major risk factor for chronic diseases, such as diabetes, cardiovascular disease, osteoarthritis, and mortality in children and adults.https://paperpile.com/c/NUwmG6/cDAyj Those who are obese also have an increase in functional abnormalities including musculoskeletal pain and higher rates of spinal degenerative diseases, specifically cervical myelopathy.https://paperpile.com/c/NUwmG6/ZjrGN+rUdaR Left untreated, degenerative diseases of the cervical spine can result in disc herniation, radiculopathy, and myelopathy, all of which can be appropriately treated with procedures, such as anterior cervical discectomy and fusion (ACDF).https://paperpile.com/c/NUwmG6/j0B9K
While ACDF is a common and effective procedure performed for relief of radicular or myelopathic pain, it has been reported that obesity remains a significant risk factor for intraoperative complications not only for spine surgeryhttps://paperpile.com/c/NUwmG6/0glTA but also across multiple surgical specialties.https://paperpile.com/c/NUwmG6/S1aoi+LcTwn+OaZtm In particular, cervical spinal fusion patients with a higher BMI have greater occurrences of deep vein thrombosis wound abnormalities, cardiopulmonary and neurologic complications, and increased mortality.https://paperpile.com/c/NUwmG6/iz0iM+0glTA+bXzDW+raeZN+q4XhJ Additionally, higher BMI was also reported to correlate with impairments in long-term physical function outcomes.https://paperpile.com/c/NUwmG6/iRoQw+i0Eeg+oyVaE Nonetheless, ACDF has been reported to have lower morbidity rates than laminectomies and demonstrates greater cost-effectiveness than cervical disc replacements (CDR) for single-level procedures.https://paperpile.com/c/NUwmG6/j0B9K+3rVXa+0BLau+w1Vj3 More recent studies have indicated that long-term benefits over CDRs may not carry over for multilevel procedures postoperatively;https://paperpile.com/c/NUwmG6/LzRN+AlVZ however, ACDF still remains as effective of an option as CDR.https://paperpile.com/c/NUwmG6/xKQe
With the increased emphasis on use of patient reported outcome measures (PROMs), the use of effective and efficient questionnaires to determine the impact of risk factors such as BMI on outcome measure becomes essential. One such outcome is physical function, which has been shown to negatively correlate with higher BMI and is valued as a predictor of the quality of daily life activities and efficacy of surgery.https://paperpile.com/c/NUwmG6/iRoQw+M3CgQ Although several different PROMs for physical function exist, the Patient Reported Outcome Measurement Information System (PROMIS) questionnaire has been validated against other legacy PROMs and been used to compare preoperative and postoperative shifts in ACDF patients’ outcomes.https://paperpile.com/c/NUwmG6/j31vj+eAlyi+epOjC In one study of ACDF patients, PROMIS-physical function (PF) showed significant improvements from baseline scores at the 12-week and 6-month follow-up timepoints and correlated well with Neck Disability Index (NDI) and Short Form-12 (SF-12).https://paperpile.com/c/NUwmG6/AhgO5
Although studies have considered the correlation of BMI and other postoperative outcomes such as quality of life (EuroQol 5-dimensional), SF-12, and NDI in ACDF patients, the relationship of BMI with physical function outcomes measured by PROMIS-PF has yet to be explored in this patient population.https://paperpile.com/c/NUwmG6/q4XhJ+i0Eeg Therefore, this study aims to detail the association between BMI and postoperative improvement in PROMIS-PF following ACDF.
METHODS
Patient Population
Prior to beginning this study, Internal Review Board approval was obtained (ORA#14051301) and informed consent was granted by patients. For this study, a prospectively maintained surgical database was retrospectively reviewed for eligible cervical spine procedures spanning from May 2015 to September 2019. Eligible patients were reviewed using the following inclusion criteria: elective, primary, single or multilevel ACDF procedures indicated for degenerative cervical spinal pathology. Patients were excluded if their surgery was indicated for infectious, traumatic, or malignant etiologies or if they failed to complete a preoperative PROMIS-PF questionnaire. A single attending physician performed all procedures at a single institution.
Data Collection
Prior to surgery, demographic information, pre-existing medical conditions, and diagnosed spinal pathologies were collected. Both intraoperative and postoperative information was also collected. Demographic information included age, gender, smoking status at time of appointment, diabetic status, CCI, and insurance type. Intraoperative and postoperative variables of interest were number of fusion levels, operative time (skin incision to skin closure, in minutes), estimated blood loss (EBL, in mL), total length of hospital stay (LOS, in hours), hospital discharge day, and postoperative complications. Evaluation of patients’ perceived physical function was conducted using the PROMIS-PF questionnaire, which was collected at preoperative, 6-week, 12-week, 6-month, 1-year and 2-year time points. Higher PROMIS-PF scores indicated more favorable physical function. Delta improvement in PROMIS-PF (postoperative score minus preoperative score) was calculated for all postoperative time points and compared to an established minimum clinically important difference (MCID) of 8.0.https://paperpile.com/c/NUwmG6/qjm2M
Statistical Analysis
Patients meeting inclusion criteria were stratified into 4 groups, based on their BMI, as follows: nonobese (BMI <30 kg/m2), Obese I (BMI ≥30 and <35 kg/m2), Obese II (BMI ≥35 and <40 kg/m2), and Obese III “severe” (BMI ≥40 kg/m2). Significant associations between BMI subgroups and demographic, pre-existing medical conditions, spinal pathologies, number of levels fused, or day of discharge were determined using either χ2 analysis or Fisher exact test where appropriate. Significant differences in mean age, CCI, operative time, EBL, or LOS between BMI subgroups were evaluated using analysis of variance with Tukey post hoc pairwise comparisons. Effects of BMI subgroup on PROMIS-PF scores were analyzed using linear regression followed by post hoc pairwise comparisons to determine specific differences between individual groups. Additionally, significant differences in delta PROMIS-PF by BMI subgroup were also evaluated using linear regression. Any significant correlations between BMI and delta PROMIS-PF were determined by calculating a Pearson correlation coefficient and the strength of relationship rate according to the following categories: weak (0.1 ≤ |r| < 0.3); moderate (0.3 ≤ |r| < 0.5); strong (|r|≥0.5). A significance of P = 0.05 was used for all statistical analyses. All statistical tests were performed using Stata 16.0 (StataCorp, College Station, TX).
RESULTS
Baseline Characteristics
A total of 185 ACDF patients were screened for inclusion in this study. After inclusion and exclusion criteria were applied, 128 patients met inclusion criteria for this study, of which 74 were placed in the nonobese group, 27 in the Obese I group, 19 in the Obese II group, and 8 in the Obese III group (Table 1). A total of 47 patients were excluded from the study due to incomplete preoperative PROMIS-PF questionnaires. The patient cohort had a mean age of 50.0±10.1 years and majority were male (57.0%). A significant difference in distribution of gender (P = 0.014), ageless CCI (P = 0.007), and diabetic status (P = 0.025) by BMI subgroup was observed (Table 1). More specifically, a larger proportion of males were observed in obese groups and a higher proportion of females in the nonobese group. Additionally, further analysis demonstrated patients in the Obese III had a significantly higher ageless CCI (1.85) compared to all other groups (all P < 0.05).
Baseline characteristics by BMI group.
Perioperative Characteristics
Majority of patients across all BMI subgroups had a spinal diagnosis of herniated nucleus pulposus and did not significantly differ in the number of levels fused (Table 2). The patient cohort had a mean operative time of 58.9 ± 16.7 minutes and mean EBL of 30.5 ± 13.3 mL. On average, the patient cohort stayed postoperatively for 13.0 ± 12.1 hours with a majority being discharged on postoperative day 0. No significant differences in perioperative characteristics were observed across all BMI subgroups (Table 2). The overall complication rate for the patient cohort was 4.3% (8/185). The nonobese group had the highest prevalence of complications (n = 5) with 3 patients experiencing postoperative dysphagia, 1 patient with a cervical hematoma, and 1 patient with altered mental status. Obese I patients were associated with a total of 2 postoperative complications, with 1 patient reporting a cervical hematoma and another patient reporting dysphagia. Only 1 patient was reported to have postoperative complications in the Obese II group with dysphagia, and no postoperative complications were reported among the Obese III group. No significant differences in overall rates of complications were demonstrated across all groups (P = 0.913). One patient (0.7%) across the total cohort underwent a reoperation at 1-year status post-ACDF. Data regarding all postoperative complication rates and summaries of each can be found in Tables 3 and 4, respectively.
Perioperative outcomes by BMI group.
Postoperative inpatient complications.
Specific incidences of complications.
Patient-Reported Outcomes
PROMIS-PF did not significantly differ between BMI subgroups at the baseline preoperative time point (P = 0.458; R 2 = 0.021). Similarly, no significant difference in PROMIS-PF by BMI subgroup was observed for the 6-week (P = 0.220; R 2 = 0.048), 12-week (P = 0.109; R 2 = 0.077), and 6-month (P = 0.060; R 2 = 0.114) time points (Table 5). Regression analysis revealed that BMI groups had a significant effect on PROMIS-PF (P = 0.035; R 2 = 0.149) at the 1-year postoperative time point. Further analysis revealed that a significant negative effect on PROMIS-PF scores was associated with Obese II (β = –7.48; P = 0.019) and Obese III (β = −8.3; P = 0.050) groups. Post hoc pairwise comparisons revealed large differences in mean scores between the nonobese group (50.5 ± 7.8) and both Obese II (43.0 ± 6.5; P = 0.087) and Obese III (42.2 ± 6.9; P = 0.207). A similar difference was also established between Obese I (50.8 ± 9.5) and both Obese II (43.0 ± 6.5; P = 0.176) and Obese III (42.2 ± 6.9; P = 0.269). Similarly, at the 2-year time point, BMI demonstrated a significant impact on PROMIS-PF scores (P = 0.014; R 2 = 0.205), with both Obese II (β = −9.7; P = 0.005) and Obese III (β = −8.8; P = 0.028) demonstrating significant negative effects (Table 5). Comparison of means between individual groups demonstrated a significant difference between Obese II and nonobese (41.7 ± 5.0 vs 51.3 ± 7.9; P = 0.026) and a large difference between Obese III and nonobese groups (42.5 ± 13.1 vs 51.3 ± 7.9; P = 0.119).
Patient-reported outcome comparisons by BMI group.
Delta improvement in PROMIS-PF did not significantly vary between BMI subgroups at the 6-week (P = 0.476; R 2 = 0.027), 6month (P = 0.331; R 2 = 0.053), or 1 year (P = 0.388; R 2 = 0.055) time point. However, a significant effect by BMI subgroups on delta PROMIS-PF was demonstrated at the 12week (P = 0.044; R 2 = 0.101) and 2year (P = 0.048; R 2 = 0.156) postoperative time point (Table 5). Further analysis revealed that at the 12-week time point, a large difference in delta PROMIS-PF was demonstrated between Obese I (10.1 ± 10.4) and both Obese II (1.8 ± 7.3; P = 0.043) and Obese III (4.3 ± 7.3; P = 0.587). At the 2-year time point, post hoc comparisons demonstrated large differences between nonobese (9.9 ± 7.0) and both Obese II (2.3 ± 5.5; P = 0.068) and Obese III (7.1 ± 8.5; P = 0.210) as well as Obese I (7.1 ± 8.5) and both Obese II (2.3 ± 5.5; P = 0.539) and Obese III (7.1 ± 8.5; P = 0.731); however, mean differences did not reach significance (Table 5).
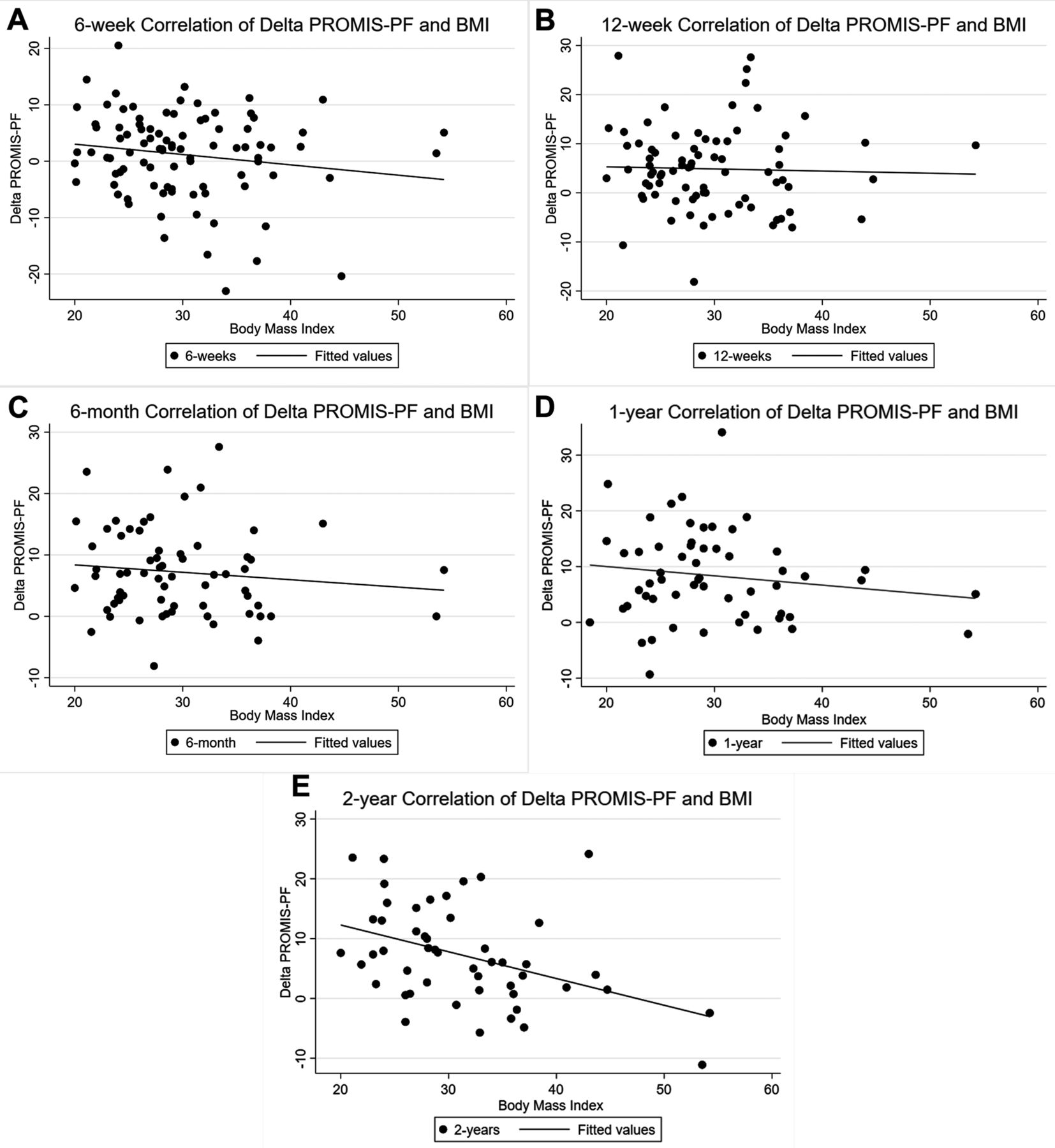
Pearson coefficients demonstrated a weak nonsignificant relationship between delta PROMIS-PF and BMI at the 6-week (|r| = 0.162; P = 0.123), 12-week (|r| = 0.032; P = 0.777), 6-month (|r| = 0.115; P = 0.357), and 1-year (|r| = 0.150; P = 0.265) time point. However, a significant moderate correlation was demonstrated at the 2-year time point (|r| = 0.419; P = 0.003) (Table 5). Overall effect of BMI on PROMIS-PF improvement at each time point can be found in Figure.
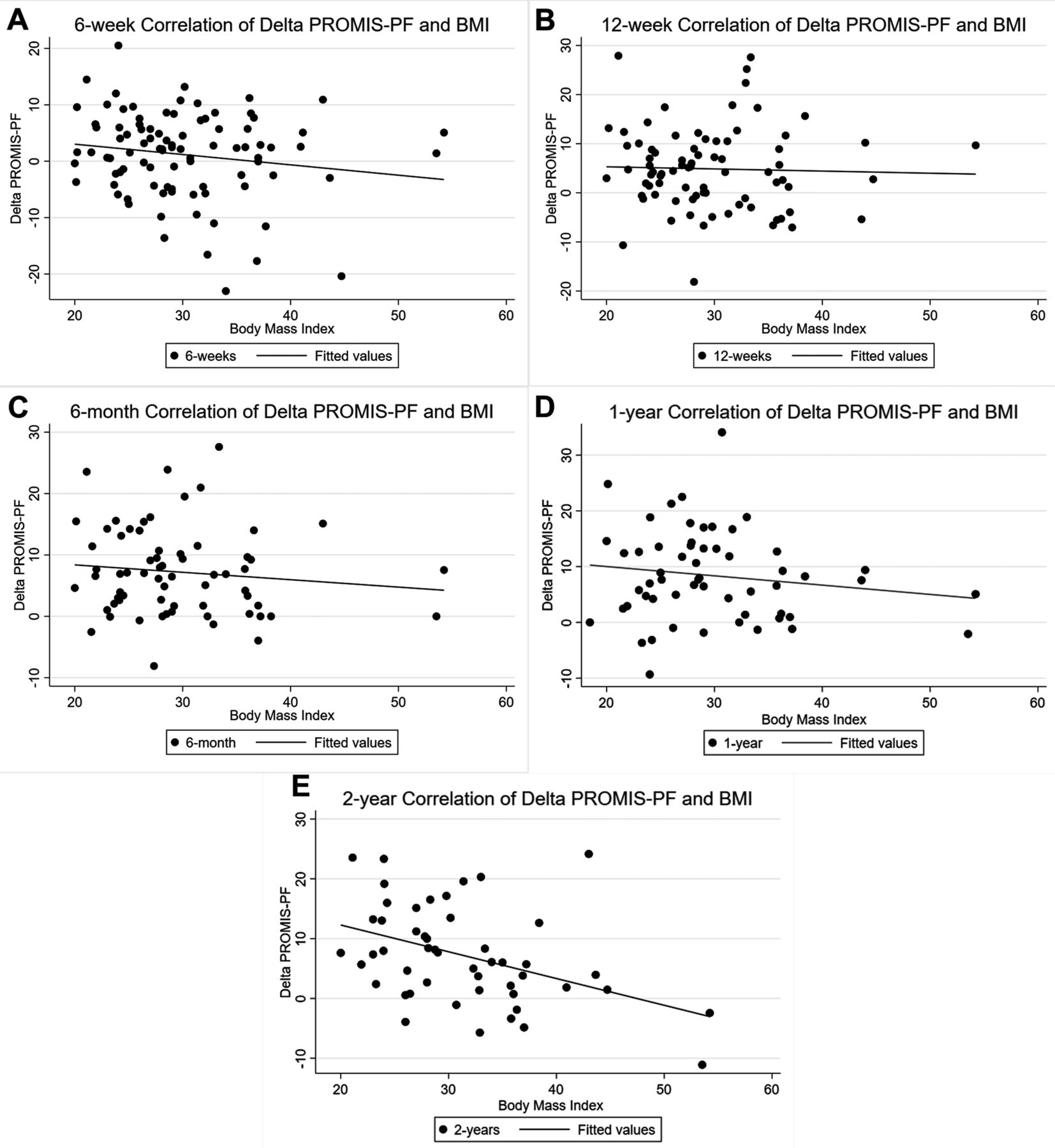
Correlation of Delta Patient-Reported Outcomes Measurement Information System physical function (PROMIS-PF) and body mass index (BMI) at (A) 6 weeks, (B) 12 weeks, (C) 6 months, (D) 1 year, and (E) 2 years.
DISCUSSION
Obesity, as measured by BMI, is an increasingly present health issue, not only in the United States but also globally, that is forcing spinal surgeons to reassess its impact on patient care and surgical outcomes. As the healthcare environment continues to shift toward a patient-centered approach, PROMs are becoming key evaluators of postoperative improvements. While previous studies have investigated the impact of BMI on postoperative improvements, few have done so using PROMIS-PF. This study investigated the relationship between BMI and PROMIS-PF and was able to demonstrate significant changes in postoperative physical function improvement.
Studying the effects of BMI on a patient population requires adequate balance in terms of patient demographics. While patient selection is considered an important determinant of successful surgical outcomes, its use could predispose a study toward selection of a nonuniform demographic. As such, this practice may unintentionally select for patients with healthier baseline characteristics. However, our study’s patient cohort reflected similar attributes as a recent epidemiological study by the NHCS. More specifically, our cohort had a mean age of 50.0 years with a majority being male which aligns well with Hales et al report of the population with the highest incidence of obesity.https://paperpile.com/c/NUwmG6/RFNs5 Our study also found a significant difference in the diabetic population based on BMI group, with the majority of our cohort being nondiabetic. While it is assumed that BMI correlates well with diabetes, there are numerous studies that outline the complexity of this relationship and emphasize the idea that the two are not mutually inclusive. In addition to diabetic status, CCI demonstrated significant differences among the BMI groups with a higher mean value associated with a greater severity of obesity. Although BMI is not specifically included in the calculation of comorbidity scores, previous studies have established the relationship between obesity and increasing CCI values.https://paperpile.com/c/NUwmG6/ERQPZ One area that should be considered as a potential effector of outcomes is smoking status. While our cohort demonstrated independence between groups with regard to smoking status, there is a noticeably higher proportion of individuals who were smokers in the nonobese group as compared to the obesity groups. Previous studies in ACDF patients have suggested that smoking may impact the rates of fusion as compared to nonsmokers (62% vs 81%);https://paperpile.com/c/NUwmG6/W79M however, this negative effect did not appear to carry through and impact health-related QOL outcome measures.https://paperpile.com/c/NUwmG6/Cc7s
Beyond the influence of BMI on postoperative complications, few studies have investigated the impact of obesity on physical function improvement for spine procedures. While other studies have similarly established a difference in physical function based on BMI,https://paperpile.com/c/NUwmG6/i0Eeg+oyVaE our study is among the first to report this relationship using PROMIS-PF. Both Sielatycki et al and Wilson et al reported that obese patients had a lower 12-Item Short Form Health Survey (SF-12) score at the 1-year time point than patients with normal weight.https://paperpile.com/c/NUwmG6/i0Eeg+oyVaE Similarly, a study assessing the impact of obesity on QOL reported a significantly lower SF-12 score at the 2-year time point.https://paperpile.com/c/NUwmG6/QTC1J All 3 studies are consistent with our findings that PROMIS-PF was significantly lower for individuals categorized as Obese II or III, compared to nonobese and Obese I patients, not only at 1 year but also 2 years. However, the underlying reasoning has not been thoroughly investigated and may be a result of patients with a higher BMI being inherently limited in physical function regardless of spine pathology. For example, Yoo et alhttps://paperpile.com/c/NUwmG6/4NLQ demonstrated that baseline physical function scores were inversely proportional to BMI among transforaminal lumbar interbody fusion patients which may be explained by a Samartzis et alhttps://paperpile.com/c/NUwmG6/ZFLh study where evidence indicated that increasing BMI is a significant contributor to degenerative disc disease and may contribute to the worsening preoperative symptoms that obese patients report. Moreover, vascular studies have indicated that metabolic syndrome, a common disorder among morbidly obese patients, impairs physical function and health-related QOL.https://paperpile.com/c/NUwmG6/0e6t Although only speculative, the results from this study and others suggest that obesity may limit the extent to which patients can improve, such that obese patients may reach their peak improvement by an intermediate time point while nonobese patients continue to improve more longitudinally. While this information may be beneficial for clinicians during preoperative counseling and reviewing expectations with patients, there may be an underlying reason for the difference in physical function only at long-term postoperative time points.
To complement the evaluation of BMI’s impact on physical function, our study also was able to calculate the magnitude of change from preoperative baseline scores. A significant difference in delta improvement was observed at both an acute time point of 12 weeks and a long-term time point of 2 years. Acute improvement in PROMIS-PF has been shown in patients undergoing ACDF up to the 6-month time point and is consistent with our study.https://paperpile.com/c/NUwmG6/oAcIp Additionally, the observed differences in delta improvement between BMI groups may be a result of varying degrees of pain reduction following surgery as previous studies have established that a negative correlation exists between physical function and pain, as measured by either visual analog scale or PROMIS-pain interference.https://paperpile.com/c/NUwmG6/b33ML+DiTtW+SZ7gK Although this was beyond the scope of our study, future studies exploring the impact of pain improvement on magnitude of physical function improvement assessed by PROMIS-PF may help further elucidate this relationship.
In terms of the long-term delta improvement at 2 years, patients who were categorized as obese had a significantly lower delta improvement which further supports our observation of significantly lower PROMIS-PF in obesity patients at both the 1- and 2-year time point. This difference in delta improvement could be explained by significantly different baseline PROMIS-PF scores because it would alter the potential gain in physical function; however, all groups demonstrated similar baseline scores. Comparison to other studies proved difficult as few have compared the impact obesity has on the magnitude of physical function improvement using PROMIS-PF. However, other groups have reported no difference in SF-12 score change between nonobese and obese patients at the 2-year time point.https://paperpile.com/c/NUwmG6/QTC1J Interestingly, we observed that the mean delta improvement demonstrated by nonobese and Obese I groups met the minimal clinically important difference (MCID) value previously established by Steinhaus et al,https://paperpile.com/c/NUwmG6/qjm2M whereas Obese II and III failed to meet this threshold. While the current study established distinct differences between obesity groups in postoperative improvement of physical function at long-term time points (1 and 2 years), decreased compliance should also be considered as a potential effector. Across all obesity groups, compliance at the 2-year mark was approximately 25% of the preoperative participation. Although the decrease may play a small effect, it may highlight the fact that patients had reached an adequate satisfaction level and prompted a decreased interest in participation. Another possibility may also be a result of increased number of health-related outcome questionnaires, which is believed to cause decreased compliance;https://paperpile.com/c/NUwmG6/ouZs+6WIy however, PROMIS surveys were developed specifically to address this concern. Nevertheless, our results further strengthen the idea that patients with a higher BMI who are undergoing ACDF may require a more invested postoperative plan to accommodate a lengthier recovery timeline.
Limitations
Given the retrospective nature of our study, there are some inherent limitations. Specifically, the selection of a surgical cohort using retrospective analysis may introduce selection bias and will limit the ability for generalizability to other centers and populations. Additionally, all patients underwent their cervical spine procedures with 1 fellowship trained orthopaedic surgeon at a single institution and may again limit the ability to relate the findings to patients from other institutions. Another key limitation may be the use of the BMI measure. Although it is a commonly used metric for body habitus, there is evidence that other measures such as waist-to-hip ratios and waist circumference may better capture obesity.https://paperpile.com/c/NUwmG6/zExnM Lastly, analysis is dependent on sufficient cohort sizes; however, given the smaller number of patients among severe and morbidly obese groups, our analysis is limited. Although invasive spine procedures among morbidly obese patients occur with relative low frequency, a multicenter and multiprovider design may allow for a larger cohort to be captured and strengthen the study.
CONCLUSION
Despite stratification into different BMI groups, patients who underwent ACDF procedures did not significantly differ in their postoperative recovery of physical function for short-term postoperative time points. Assessment of physical function revealed a significant difference in obese vs nonobese patients at long-term time points and demonstrated a significantly lower change in score at the 2-year time point. These results suggest that obese patients may require a more involved road to recovery of physical function. Given the continued increase in incidence of obesity in the United States, this may become a more prevalent finding for ACDF patients and may force spinal surgeons to adapt their follow-up strategies and better counsel patients preoperatively.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest with respect to the research, authorship, and/or publication of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.