


Article Figures & Data
Figures
- Figure 1
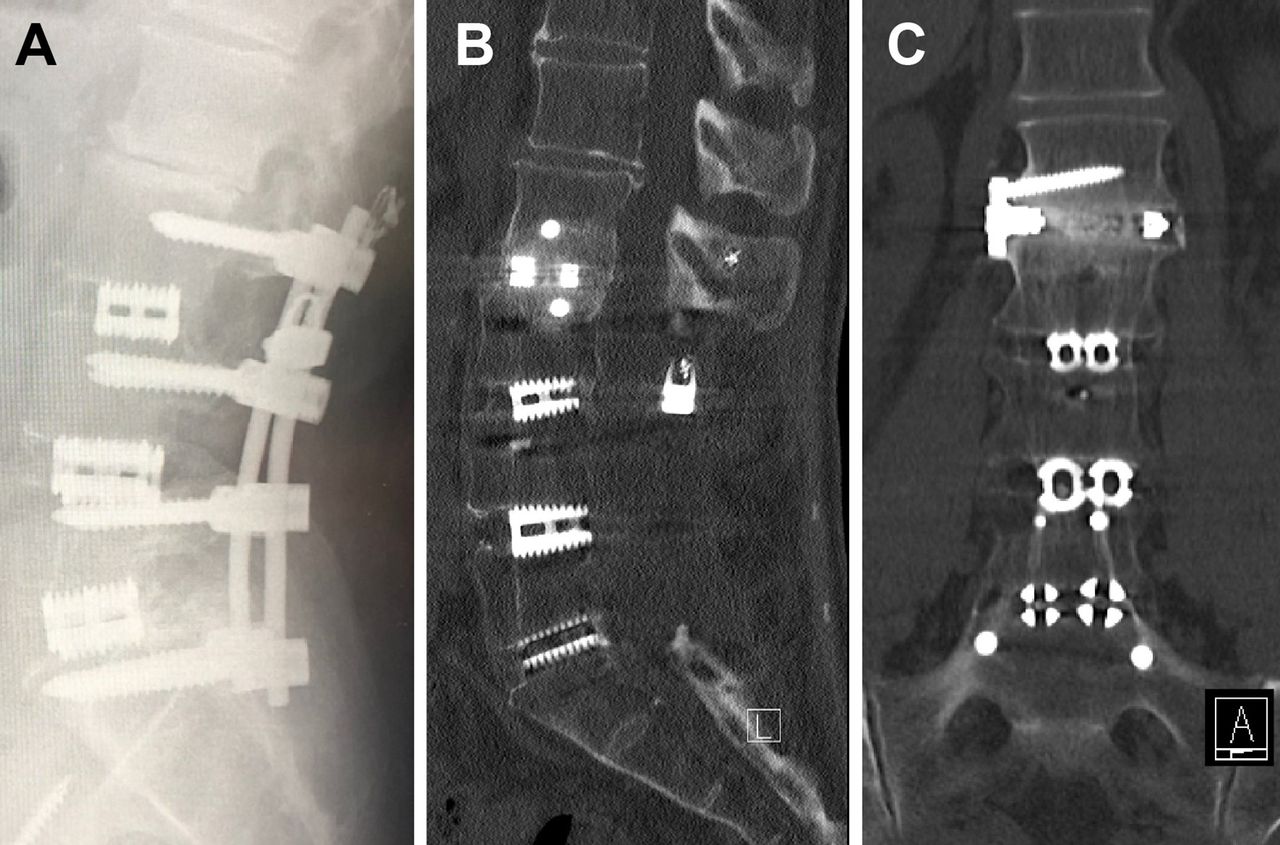
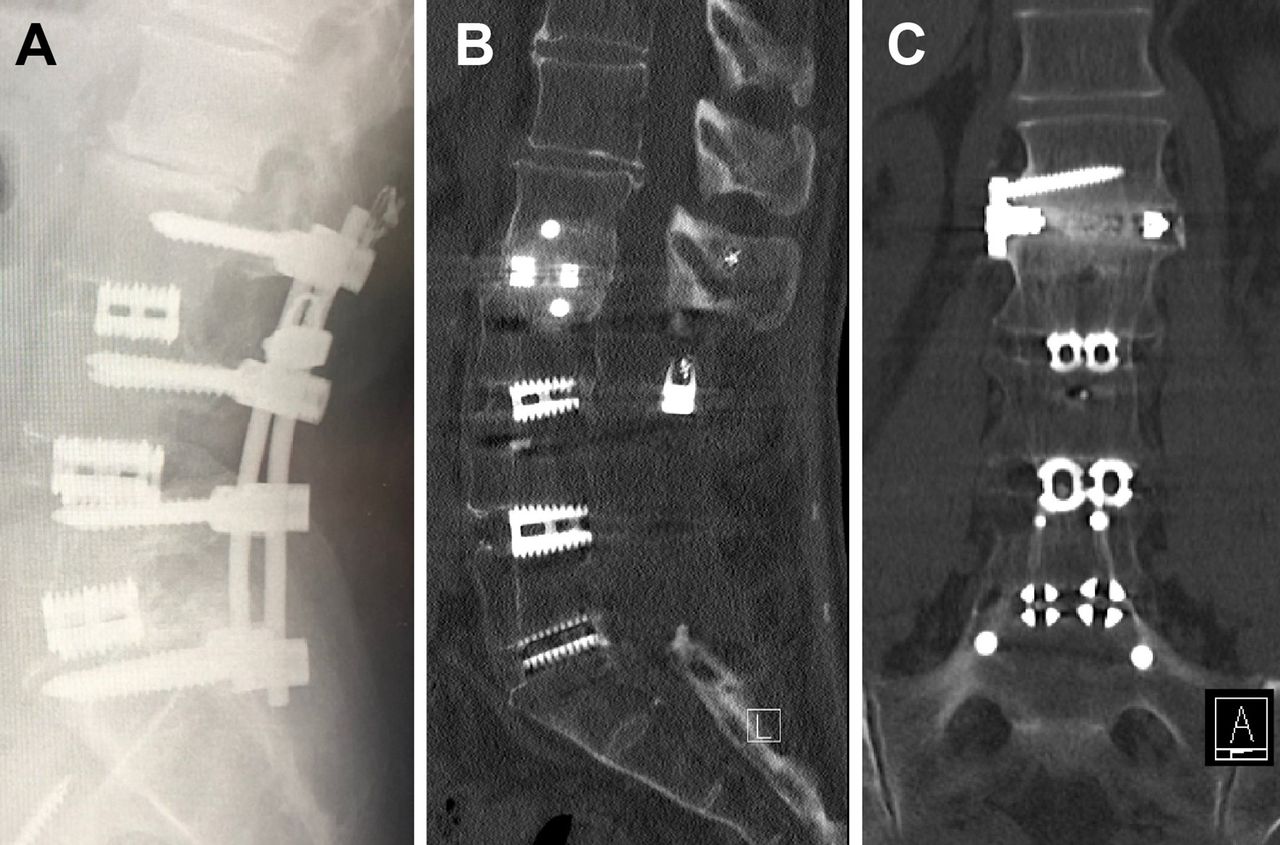
(A) L2-L3 adjacent segment disease above a previous L3-S1 posterior lumbar interbody fusion on a lateral radiograph. The expandable lateral titanium interbody cage with an integrated lateral fixation at the L2-L3 level with solid interbody fusion at 12 months noted on computed tomography. (B) Sagittal and (C) coronal views.
- Figure 2
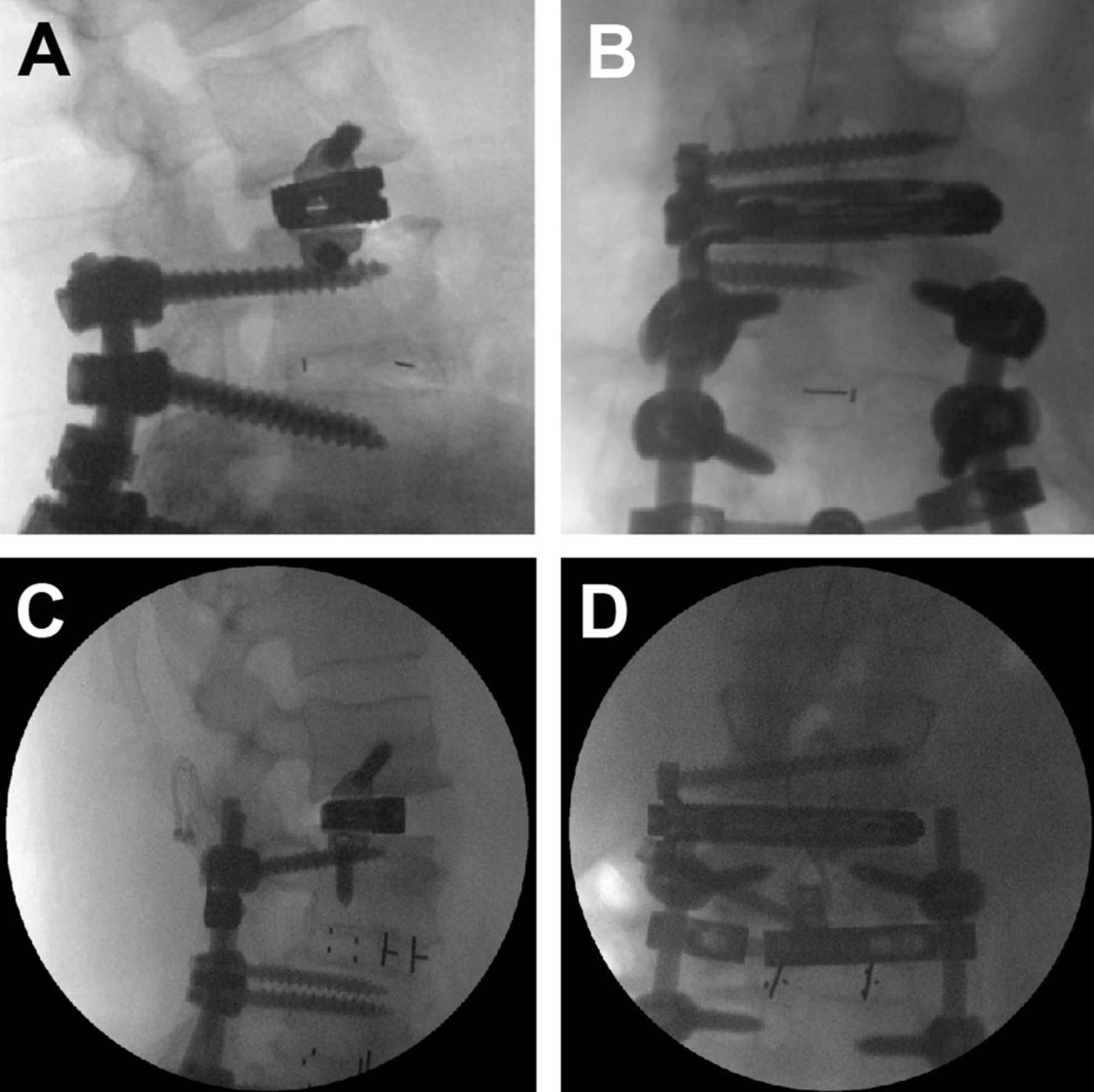
Radiograph of expandable lateral titanium interbody cage with an integrated lateral fixation at the L3-L4 level with the inferior screw of the lateral plate placed above (A, B) and below (C, D) the in situ superior pedicle screw: (A, C) lateral and (B, D) anteroposterior films.
Tables
- Table 1
Comparative cost analysis of single-level eLLIFp, LLIF with posterior fixation, TLIF, PLIF, PLF, and ALIF.
Procedure (Single-Level Adjacent Segment Disease/Extension of Construct) Implant Implant Charges Total Implant Charges OR Charges (Mean OR Time @ $2500/h) Inpatient Hospital Charges (Mean LOS @ $1335/d) Total Specialist (Surgeon + Anesthetist @ $19.80/unit) Medicare Charges67 Cell Saver Intraoperative Neural Monitoring Mean Total Costa Cost Relativity (Using eLLIFp as Index) eLLIFp Expandable lateral cage with plate screws $6021; $186 × 2 (2 screws) $6393 $5000 (2 h) $4005 (3 d) $2817 ($2193 + $614 [31 units]) N/A $1500 $19,715 1 LLIF with posterior fixation Expandable lateral cage; Polyaxial screws; Caps/blockers; Prelordosed rods $3335; $1232 × 2 (2 screws); $560 × 6 (6 caps); $410 × 2 (2 rods) $9979 $7500 (3 h) $4005 (3 d) $3656 ($2923 + $733 [37 units]) N/A $1500 $26,640 1.4 TLIF Expandable TLIF cage; Polyaxial screws; Caps/blockers; Prelordosed rods $3335; $1232 × 2 (2 screws)b; $560 × 6 (6 caps); $410 × 2 (2 rods) $9979 $7500 (3 h) $6675 (5 d) $3514 ($2663 + $851 [43 units]) Optional N/A $27,668 1.4 PLIF Expandable PLIF cage; Polyaxial screws; Caps/blockers; Prelordosed rods $2780 × 2 (2 cages); $1232 × 2 (2 screws)b; $560 × 6 (6 caps); $410 × 2 (2 rods) $12,204 $7500 (3 h) $6675 (5 d) $3514 ($2663 + $851 [43 units]) $500 N/A $30,393 1.5 PLF Polyaxial screws; Caps/blockers; Prelordosed rods $1232 × 2 (2 screws)b; $560 × 6 (6 caps); $410 × 2 (2 rods) $6644 $6250 (2.5 h) $5340 (4 d) $3232 ($2499 + $733 [37 units]) $500 N/A $21,966 1.1 ALIF Integrated static cage; Screws $6021; $186 × 3 (3 screws) $6579 $7500 (3 h) $6675 (5 d) $2613 ($1880 + $733 [37 units]) plus vascular surgeon: $1186 $500 N/A $25,053 1.3 Abbreviations: ALIF, anterior lumbar interbody fusion; eLLIFp, expandable lateral titanium interbody cages with integrated lateral plate fixation; LLIF, lateral lumbar interbody fusion; LOS, length of stay; N/A, not applicable; OR, operating room; PLF, posterolateral instrumented fusion; PLIF, posterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion.
Note: All costs given in Australian dollars.
↵a Total cost does not include charges for bone graft substitutes (which depend on the surgeon’s preference).
↵b Assumes posterior fixation with 2 new screws above the construct and using the existing screws below with new caps.
Characteristic Value (N = 33) Age, y, mean (range) 64.9 (34–82) Female, n (%) 18 (55) Body mass index, kg/m2, mean (range) 29.5 (20.0–38.5) Current smoker, n (%) 4 (12) Previous posterior fusion level, n (%) L5-S1 (1-level) 8 (24) L4-S1 (2-level) 15 (46) L3-S1 (3-level) 8 (24) L2-S1 (4-level) 2 (6) Time from fusion to ASD, y, mean (range) 7.8 (1–25) ASD pathology (35 devices), n (%) Degenerative spondylolisthesis 12 (34) Foraminal stenosis 10 (29) Canal stenosis 8 (23) Degenerative disc disease 5 (14) ASD level treated (35 devices) L1-L2, n (%) 4 (11) L2-L3, n (%) 10 (29) L3-L4, n (%) 14 (40) L4-L5, n (%) 7 (20) Psoas retraction time, min, mean (range) Total time 30.8 (15–40) Time with retractor open to 22 mm 14.4 (8–24) Time with retractor open to 25 mm 13.9 (7–22) Abbreviation: ASD, adjacent segment disease.
Outcome Measure Preop 6 wk 6 mo 12 mo P (Preop vs 12 mo) Back VAS pain score 7.8 ± 1.4 2.1 ± 0.6 1.3 ± 0.8 1.2 ± 0.8 <0.0001 Leg VAS pain score 6.9 ± 2.8 1.8 ± 1.7 1.4 ± 1.2 1.4 ± 1.3 <0.0001 Oswestry Disability Index 61.0 ± 11.5 39.0 ± 6.2 30.9 ± 16.4 32.2 ± 12.2 <0.0001 SF-12 physical component score 30.1 ± 6.4 44.5 ± 7.8 49.0 ± 8.3 50.9 ± 5.4 <0.0001 SF-12 mental component score 39.0 ± 7.3 50.1 ± 7.6 52.7 ± 8.1 55.3 ± 4.3 <0.0001 Abbreviations: Preop, preoperative; SF-12, Short Form 12-item health survey; VAS, visual analog scale.
Note: Data are presented as mean ± SD.
Time % Solid Interbody Fusion (n Fused/n Total) 6 mo 53 (18/34) 12 mo 94 (32/34) Abbreviation: n, number of cages.
Complication Number Minor Anterior thigh sensory change 1 Anterior thigh pain 1 Atelectasis 0 Ileus 0 Superficial wound infection 0 Hematoma 0 Incisional hernia 0 Total 2 Major Radiculopathy (motor deficit) 1 Femoral neuropathy 0 Pneumothorax 0 Deep wound infection 0 Bowel injury 0 Major vascular injury 0 Subsidence 0 Cage migration 0 Screw loosening or fracture 0 Vertebral fracture 0 Revision surgery 0 Total 1
In this issue




{kind=link}
{kind=link}