


Article Figures & Data
Figures
- Figure 1
Postoperative standard x-ray images showing a patient who benefited from craniocervical fusion.
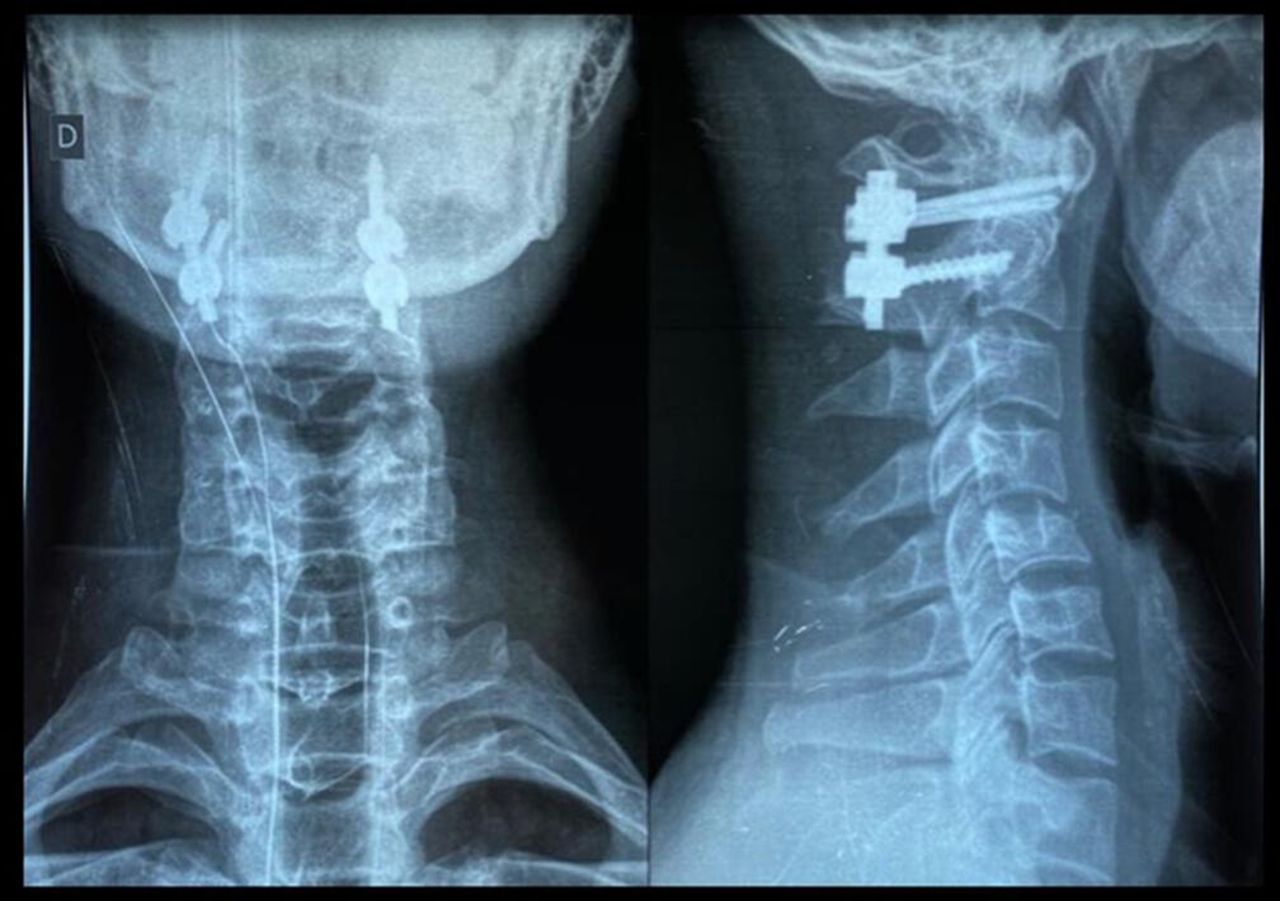
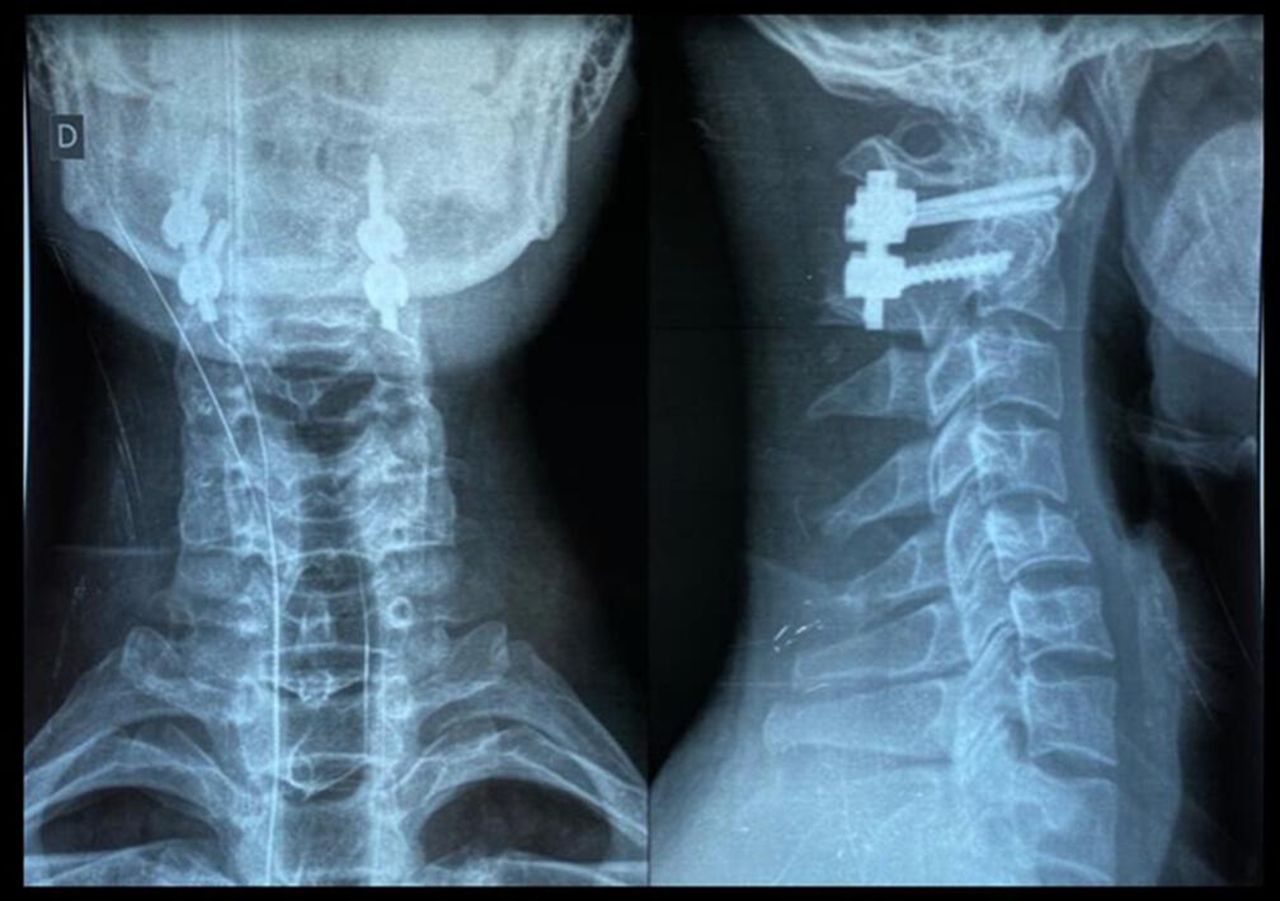
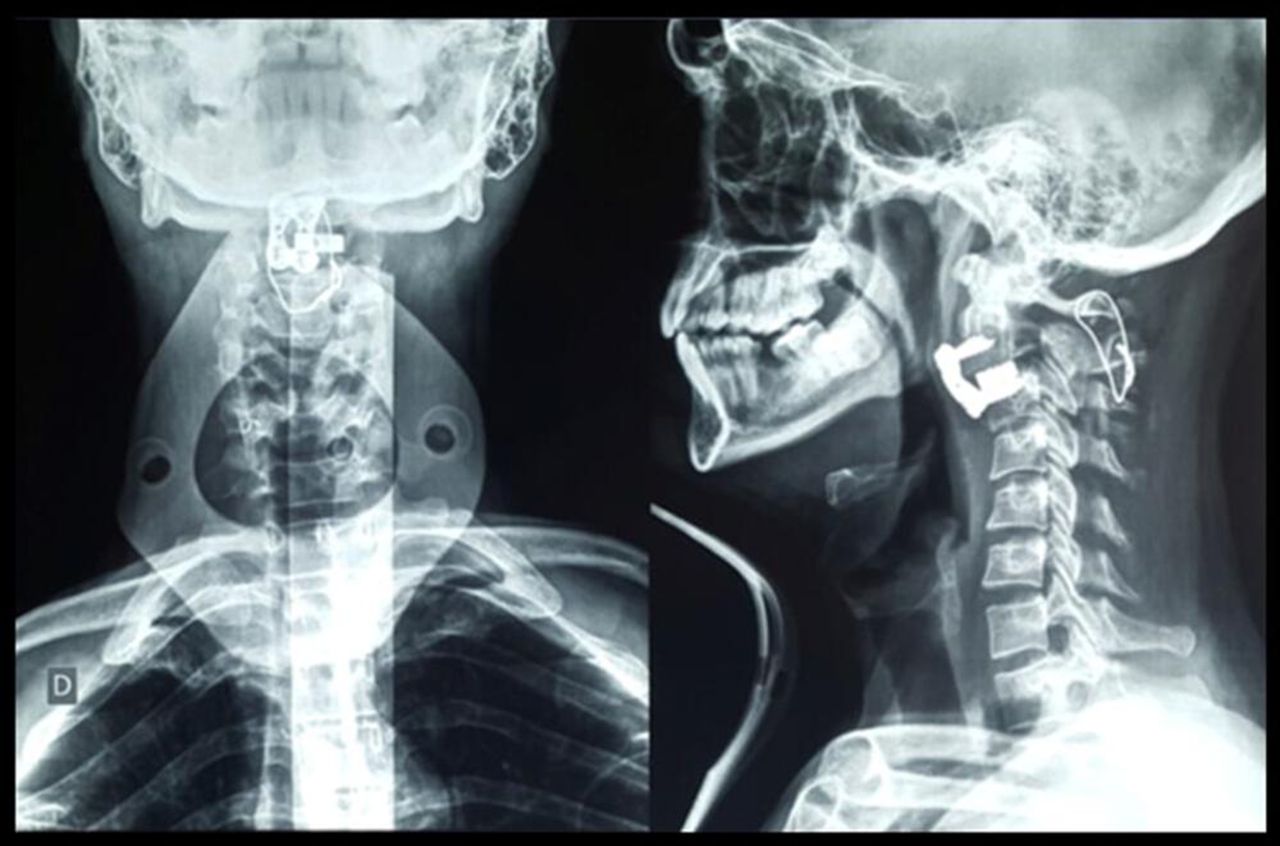
- Figure 2
Postoperative standard x-ray images showing a patient who underwent a C1-C2 posterior arthrodesis (Goel-Harms technique).
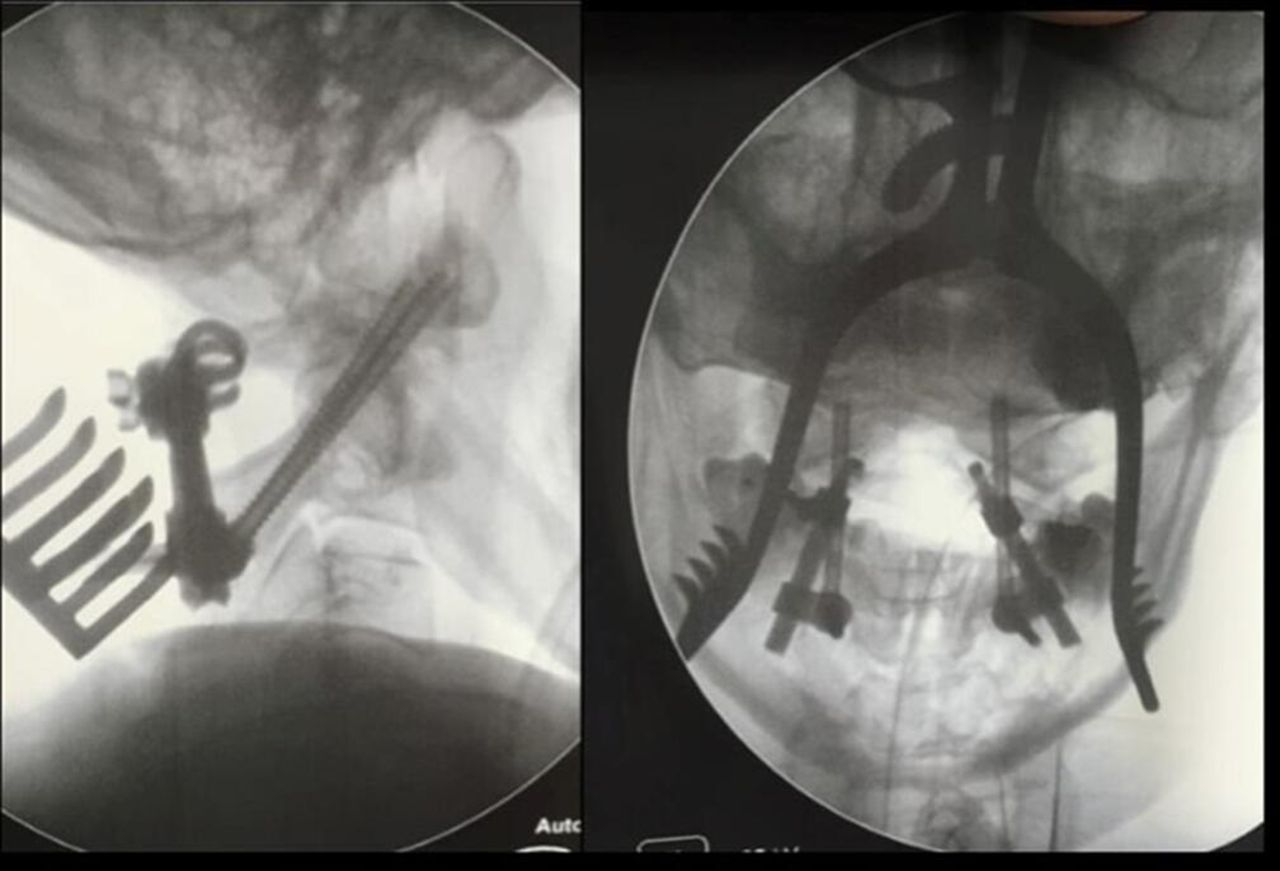
- Figure 3
Intraoperative fluoroscopy showing a type II odontoid fracture. The patient who underwent a transarticular C1-C2 posterior arthrodesis (Magerl technique).
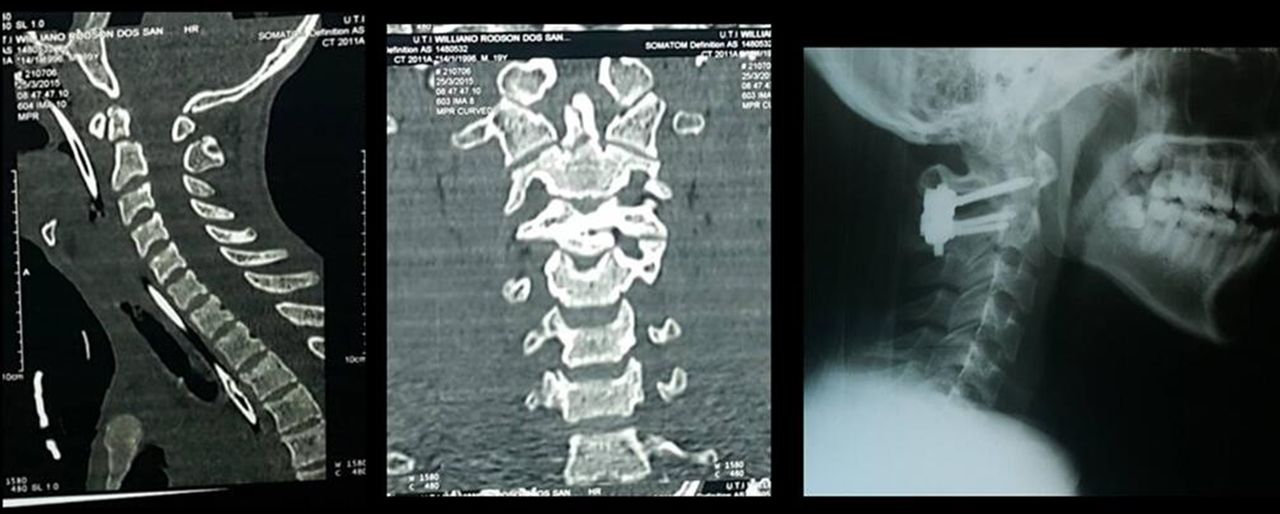
- Figure 4
Preoperative computed tomography images showing a patient with type II odontoid fracture presenting a split in the odontoid process. The patient underwent a C1-C2 posterior arthrodesis (Goel-Harms technique), which is shown on a postoperative standard x-ray image.
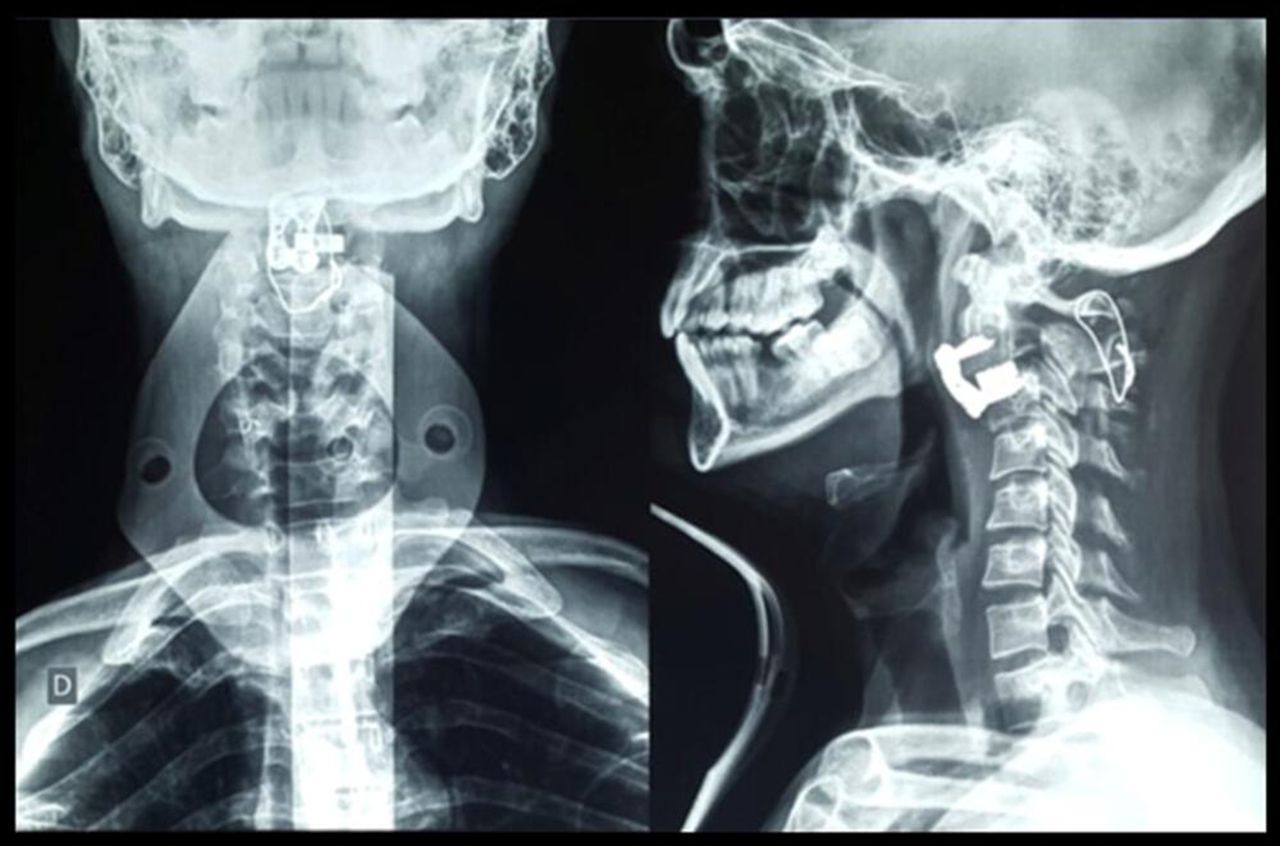
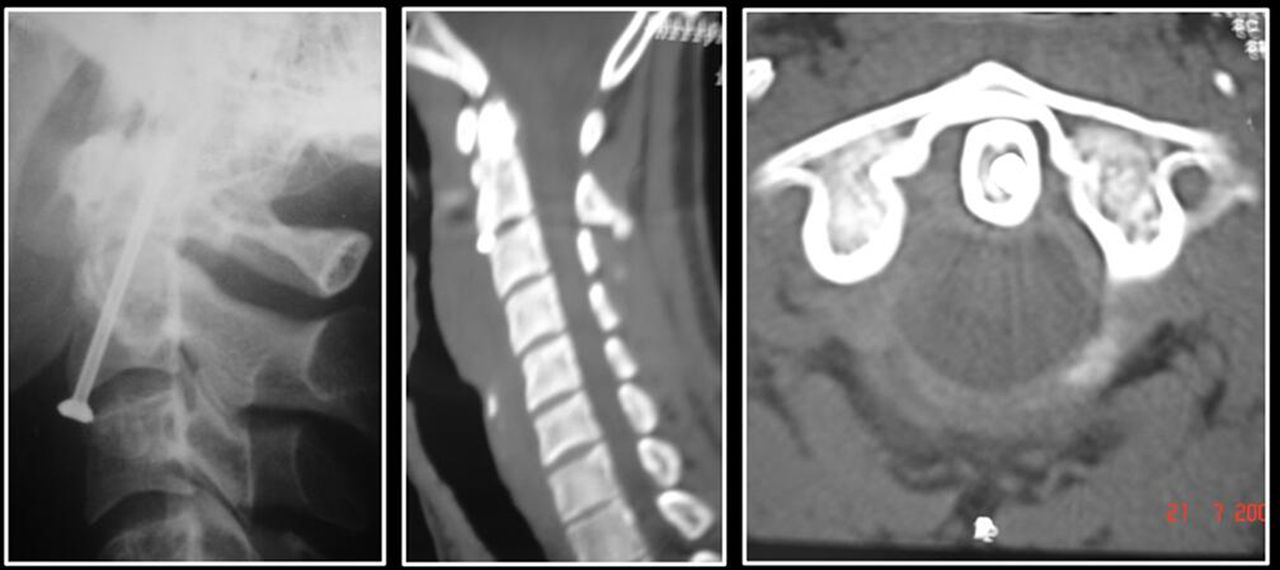
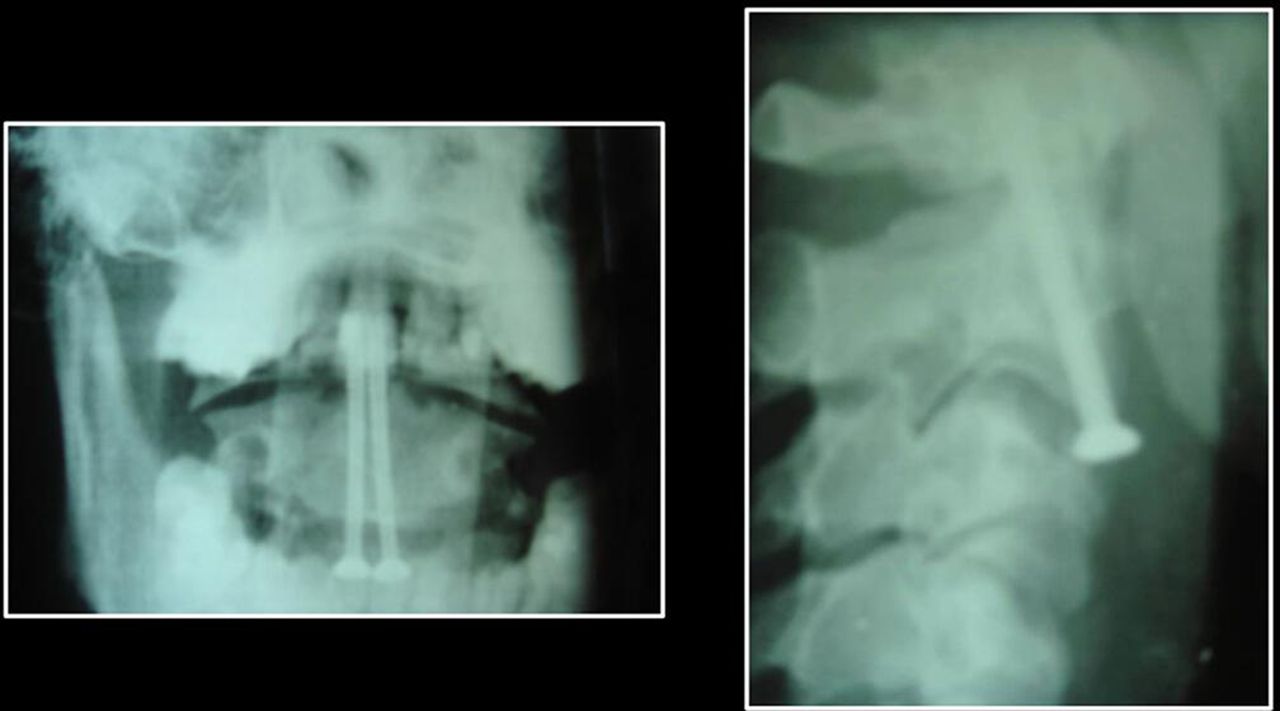
- Figure 5
Postoperative computed tomography images showing a patient with type II odontoid fracture who benefited from anterior odontoid screwing.
- Figure 6
Postoperative standard x-ray images showing a patient with type II odontoid fracture who benefited from anterior fixation of the odontoid process with 2 screws.
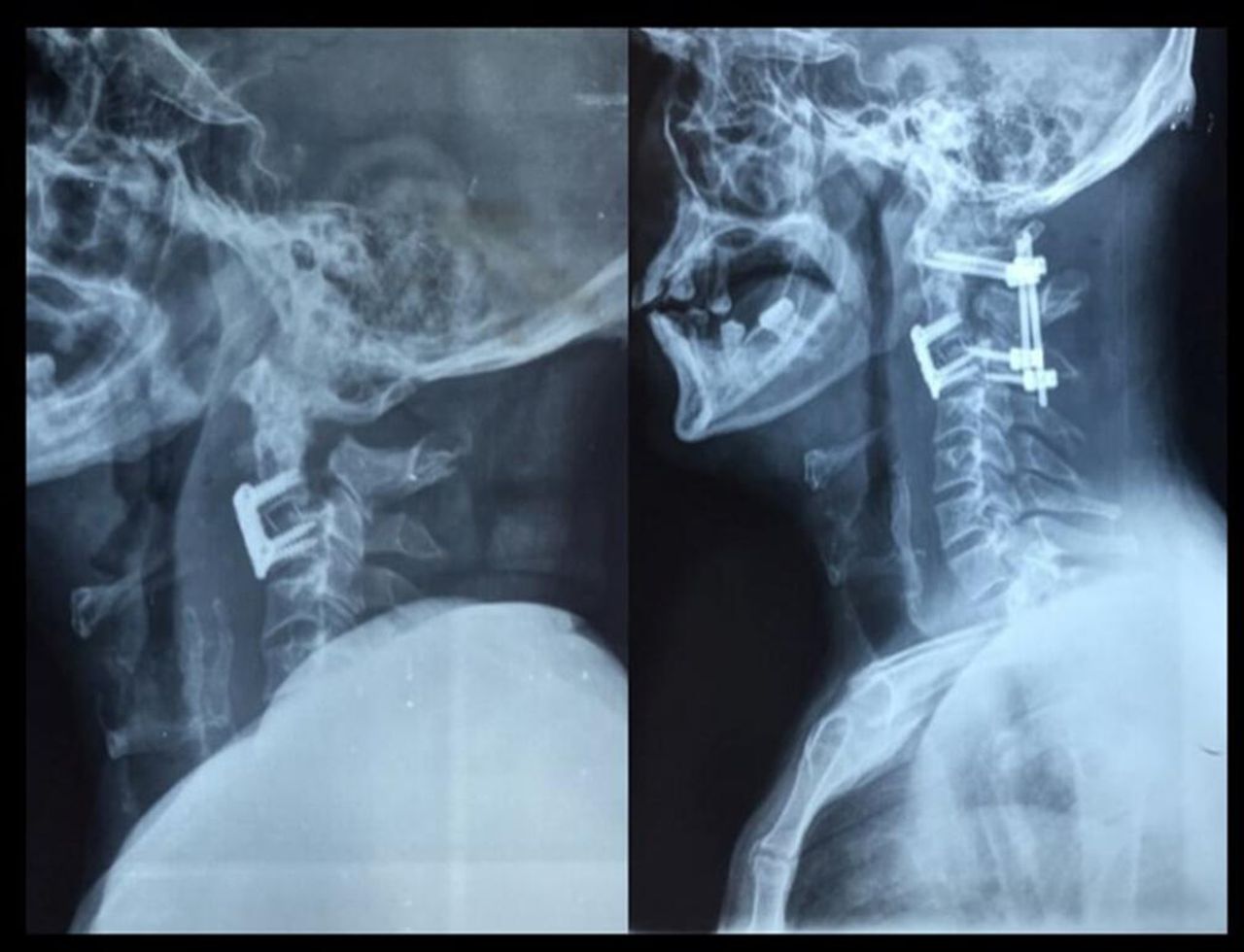
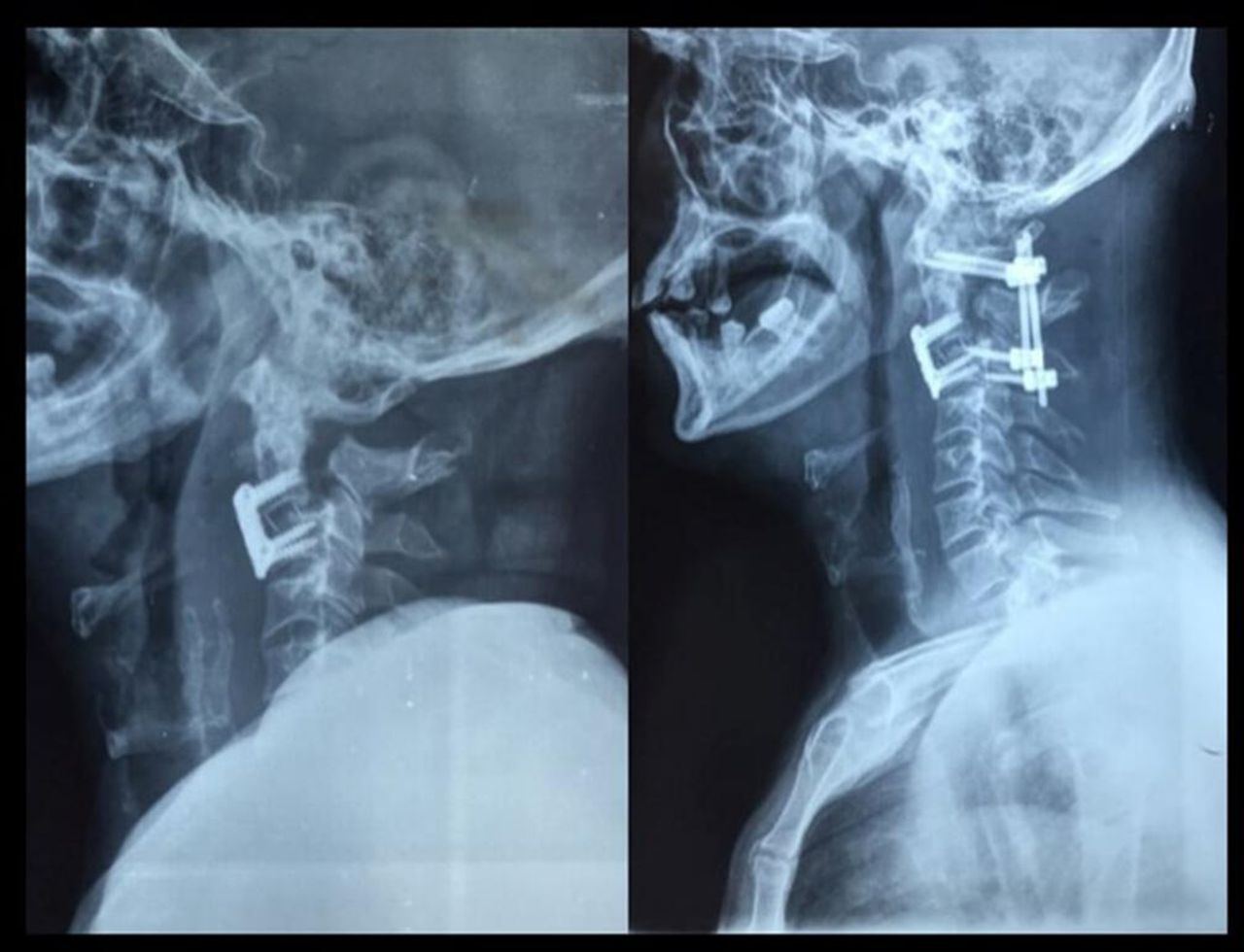
- Figure 7
Preoperative and postoperative standard x-ray images showing a patient with hangman’s fracture who benefited from C2-C3 discectomy and interbody fusion.
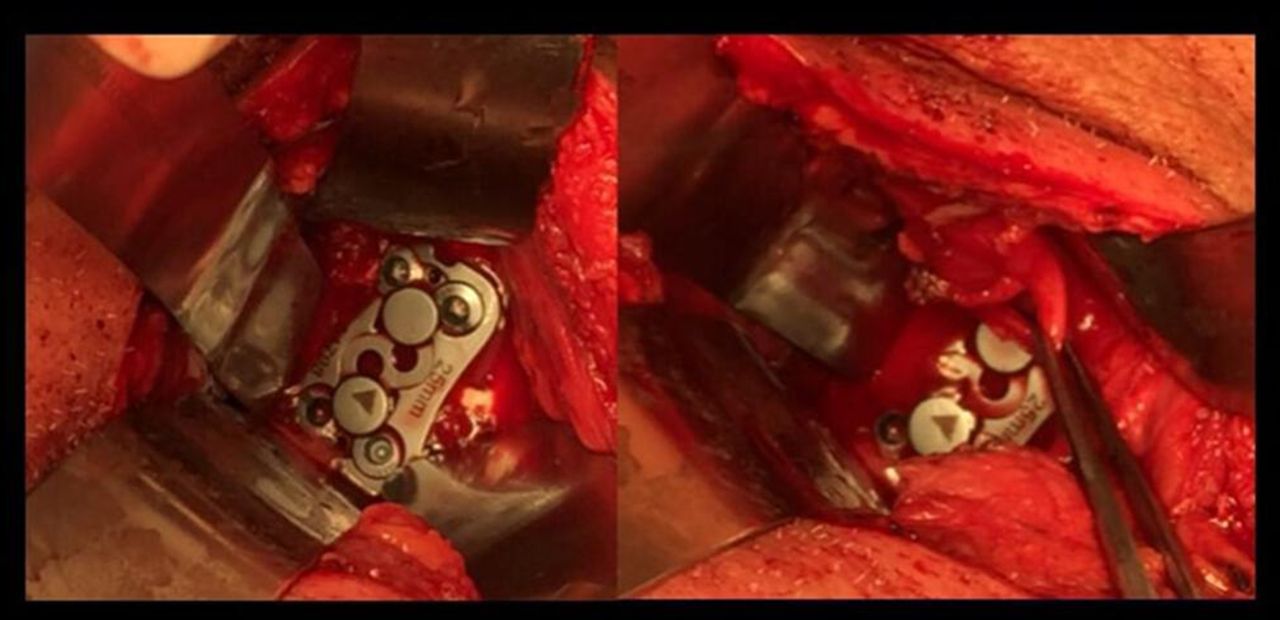
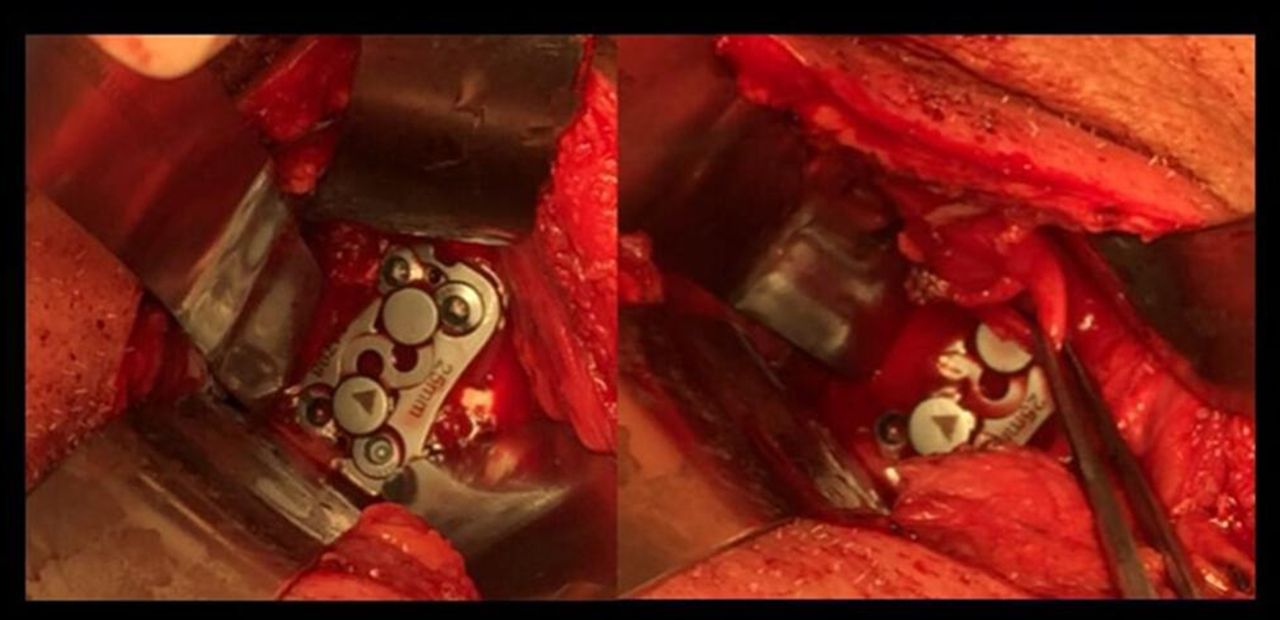
- Figure 8
Intraoperative view showing a case of anterior C2-C3 discectomy and interbody fusion. Recurrent laryngeal nerve was identified and preserved (right).
- Figure 9
Postoperative standard x-ray images showing a patient with hangman’s fracture who submitted to an anterior approach. The patient had an unsatisfactory large gap on fracture place (left) and who benefited from 360° fusion (right).
- Figure 10
Postoperative standard x-ray images showing a patient who benefited from C2-C3 discectomy and interbody fusion and posterior wiring.






Tables
Variable n (%) Injury level C1 11 (9.2) C2 84 (70.0) C1-C2 21 (17.5) C2-C3 4 (3.3) Injury classification Type I C1 fracture (ring fractures) 7 (5.8) Type II C1 fracture (Jefferson’s fracture) 2 (1.7) Type III C1 fracture (lateral mass fracture) 2 (1.7) Hangman’s fracture 16 (13.3) Type II odontoid fractures 35 (29.2) Type III odontoid fractures 4 (3.3) Miscellaneous C2 fractures 24 (20.0) C1-C2 dislocations 4 (3.3) C2-C3 dislocations 2 (1.7) Atlanto-occipital displacement 2 (1.7) Type II C1 fracture (Jefferson’s fracture) + type II odontoid fracture 2 (1.7) Type II odontoid fracture + atlanto-occipital displacement 2 (1.7) Type II odontoid fracture + hangman’s fracture 4 (3.3) Type III odontoid fracture + miscellaneous C2 fractures 2 (1.7) Type I C1 fracture + type II odontoid fractures 3 (2.5) Type III odontoid fracture + C1-C2 dislocations 2 (1.7) Type I odontoid fractures + C1-C2 dislocations + miscellaneous C2 fractures 3 (2.5) Type II C1 fracture (Jefferson’s fracture) + type III odontoid fracture 2 (1.7) Type III C1 fracture (lateral mass fracture) + miscellaneous C2 fractures 2 (1.7) Variable Injury Level P Valuea C1 C2 C1-C2 C2-C3 Total n % n % n % N % Total 11 100.0 84 100.0 21 100.0 4 100.0 120 100.0 Age, y 0.510 16–29 8 72.7 31 36.9 9 42.9 3 75.0 51 42.5 30–39 1 9.1 17 20.2 3 14.3 - - 21 17.5 40–59 1 9.1 22 26.2 7 33.3 - - 30 25.0 60–82 1 9.1 14 16.7 2 9.5 1 25.0 18 15.0 Gender 0.696 Male 11 100.0 75 89.3 18 85.7 4 100.0 108 90.0 Female - - 9 10.7 3 14.3 - - 12 10.0 Trauma mechanisms 0.292 Car accident 3 27.3 21 25.0 3 14.3 2 50.0 29 24.2 Motorcycle accident 2 18.2 24 28.6 10 47.6 2 50.0 38 31.7 Gunshot injury 2 18.2 3 3.6 3 14.3 - - 8 6.7 Fall from standing height 1 9.1 13 15.5 - - - - 14 11.7 Fall from height 1 9.1 13 15.5 3 14.3 - - 17 14.2 Others 2 18.2 10 11.9 2 9.5 - - 14 11.7 Frankel Scale 0.128 A 1 9.1 1 1.2 1 4.8 1 25.0 4 3.3 B 1 9.1 - - - - - - 1 0.8 C 1 9.1 6 7.1 2 9.5 - - 9 7.5 D - - 4 4.8 - - - - 4 3.3 E 8 72.7 73 86.9 18 85.7 3 75.0 102 85.0 Neurologic deficit 0.426 Yes 3 27.3 11 13.1 3 14.3 1 25.0 18 15.0 No 8 72.7 73 86.9 18 85.7 3 75.0 102 85.0 Management/outcome <0.001b Surgical 1 9.1 54 64.3 17 81.0 3 75.0 75 62.5 Conservative 10 90.9 30 35.7 3 14.3 1 25.0 44 36.7 Death - - - - 1 4.8 - - 1 0.8 Variable Neurological Deficit P Valuea Yes No Total n % n % n % Total 18 100.0 102 100.0 120 100.0 Age, y 0.837 16–29 9 50.0 42 41.2 51 42.5 30–39 3 16.7 18 17.6 21 17.5 40–59 3 16.7 27 26.5 30 25.0 60–82 3 16.7 15 14.7 18 15.0 Gender 0.387 Male 15 83.3 93 91.2 108 90.0 Female 3 16.7 9 8.8 12 10.0 Trauma mechanisms 0.107 Car accident 4 22.2 25 24.5 29 24.2 Motorcycle accident 3 16.7 35 34.3 38 31.7 Gunshot injury 4 22.2 4 3.9 8 6.7 Fall from standing height 3 16.7 11 10.8 14 11.7 Fall from height 2 11.1 15 14.7 17 14.2 Others 2 11.1 12 11.8 14 11.7 Management/outcome = 0.117 Surgical 12 68.7 63 61.8 75 62.5 Conservative 5 27.7 39 38.2 44 36.7 Death 1 5.6 - - 1 0.8 ↵a Fisher’s exact test.
Variable n (%) Type of injury Isolated hangman’s fracture 16 (13.3) Isolated odontoid fracture 42 (35.0) Isolated C1 fracture 11 (9.2) Combined C1-C2 fracture 9 (7.5) Miscellaneous C2 fracture 30 (25.0) Ligament injury 8 (6.7) Odontoid fracture + hangman’s fracture 4 (3.3) Management C0-C3 posterior fusion 3 (2.5) C0-C4 posterior fusion 1 (0.8) C1-C2 posterior fusion 30 (25.0) C1-C3 posterior fusion 8 (6.7) C1-C4 posterior fusion 2 (1.7) C2-C3 discectomy 9 (7.5) C2-C3 posterior fusion 1 (0.8) C2-C3 discectomy + C1-C3 posterior fusion 3 (2.5) Conservative management 44 (36.7) Occipital craniectomy + bullet removal 1 (0.8) Transoral odontoidectomy + C0-C4 posterior fusion 2 (1.7) Transoral odontoidectomy + C1-C2 posterior fusion 1 (0.8) Odontoid screwing 14 (11.7) Deatha 1 (0.8) ↵a One patient died due to hemodynamic instability before surgery.
ManagementType of Injury Isolated Fracture Combined Fracture Hangman’s Fracture Odontoid Fracture C1 Fracture Ligament Injury Combined C1- C2 Fracture Miscellaneous Fracture of C2 Combined Odontoid Fracture and Hangman's Fracture C0-C3 posterior fusion - - - - 3 - - C0-C4 posterior fusion - 1 - - - - - C1-C2 posterior fusion 1 17 - 5 3 2 2 C1-C3 posterior fusion 1 1 - - 5 1 - C1-C4 posterior fusion 1 1 - - - - - C2-C3 discectomy 5 - - - 1 1 2 C2-C3 posterior fusion - 1 - - - - - C2-C3 discectomy + C1-C3 posterior fusion 2 - - - 1 - - Odontoid screwing - 12 - 2 - - - Occipital craniectomy + bullet removal - - 1 - - - - Transoral odontoidectomy + C0-C4 posterior fusion - 1 - - - 1 - Transoral odontoidectomy + C1-C2 posterior fusion - 1 - - - - - Conservative managementb 6 7 10 2 16 3 - Deatha - - - - 1 - - Total 16 42 11 9 30 8 4
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.