


Article Figures & Data
Figures
- Fig. 1
Preoperative anteroposterior and postoperative radiographic views show a 53° degenerative scoliosis, disk space collapse, and neural foraminal narrowing from L1 to L5. Grade II subluxation laterally at L3 to the left of L4 with degenerative lateral listhesis is also seen at L3–4 with a rotatory component. The central sacral vertical line indicates that the patient's trunk is 2 cm out of balance toward the left compared with the coronal plumb line (case 5). The postoperative scoliosis correction was from 53° down to 7°.
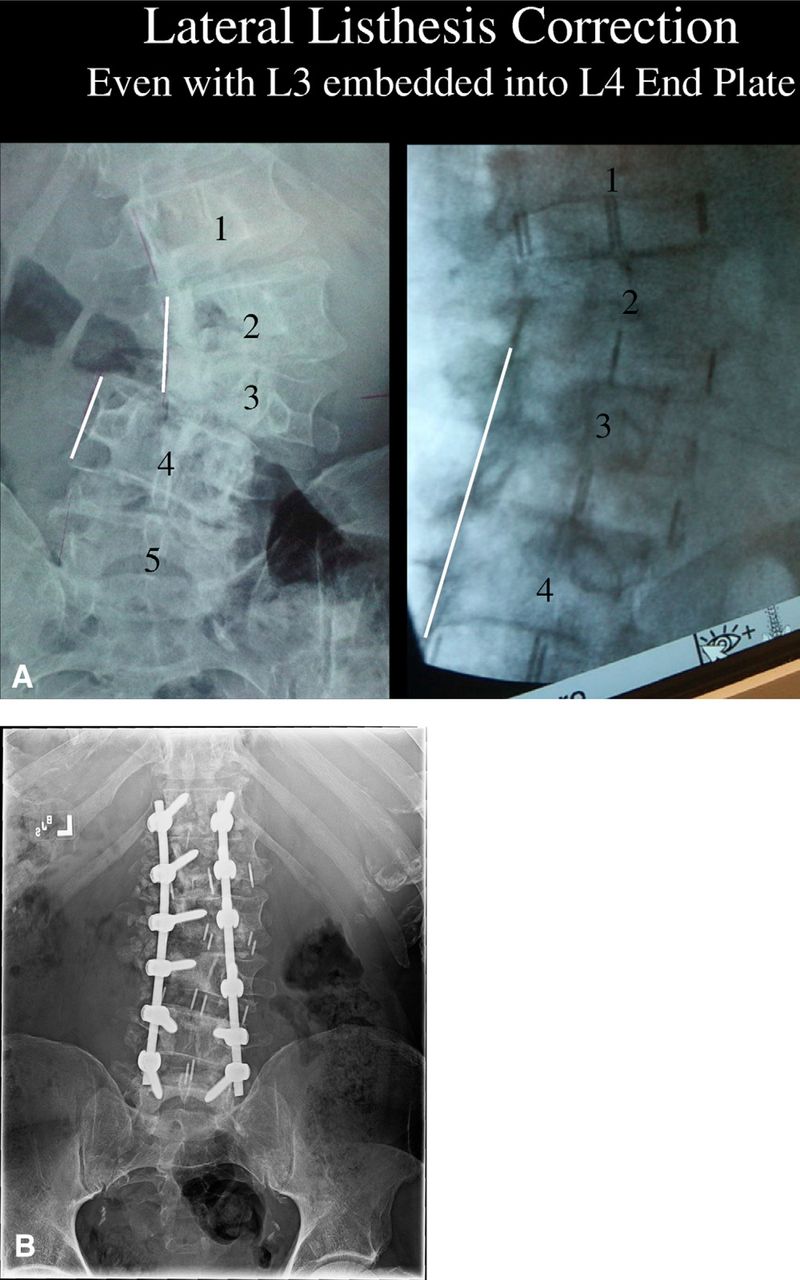
- Fig. 2
Lateral listhesis correction is possible with minimally invasive multiple-level XLIF. Even with the L3 vertebra embedded within the superior end plate of L4, this grade II lateral listhesis was reduced with the first-stage XLIF. The major reduction techniques include hinging the operating table such that the patient is bent toward the convexity, complete circumferential annulotomy, and XLIF performed from the concave side. In contrast to open traditional anterior scoliosis procedures, which are approached from the convex side, multilevel XLIF is performed from the concave side. Even the most severe cases of lateral listhesis can be corrected via the concave side. The trajectory to each of the L1–2, L2–3, L3–4, and L4–5 disks can be reached through a minimally invasive surgery incision 5 cm or shorter in length. Preoperative axial magnetic resonance imaging views showed severe stenosis at L3–4 with compression of the thecal sac, severe ligamentum flavum hypertrophy, and facet arthropathy, which were corrected through XLIF. However, a synovial cyst and soft-tissue compression of the nerve roots need to be directly decompressed through a posterior approach. (A) Correction of a coronal decompensation of 2 cm or more and sagittal decompensation of 10 cm or more needs to be achieved with posterior instrumentation. (B) Standing anteroposterior radiograph of same patient at follow-up. The pedicle orientation on the right side at L3 and L4 is now collinear, whereas in A, the right L3 pedicle is the oblique typical Scotty dog profile. It would require multiple postoperative CT cuts through the vertebra at different angles to quantitate the derotation more precisely, but the important point clinically is that the symptoms of radiculopathy from pedicular kinking of the convex apical nerve roots were alleviated. This 67-year-old man's neurogenic claudication was dramatically relieved postoperatively, and he could walk upright for extended periods.
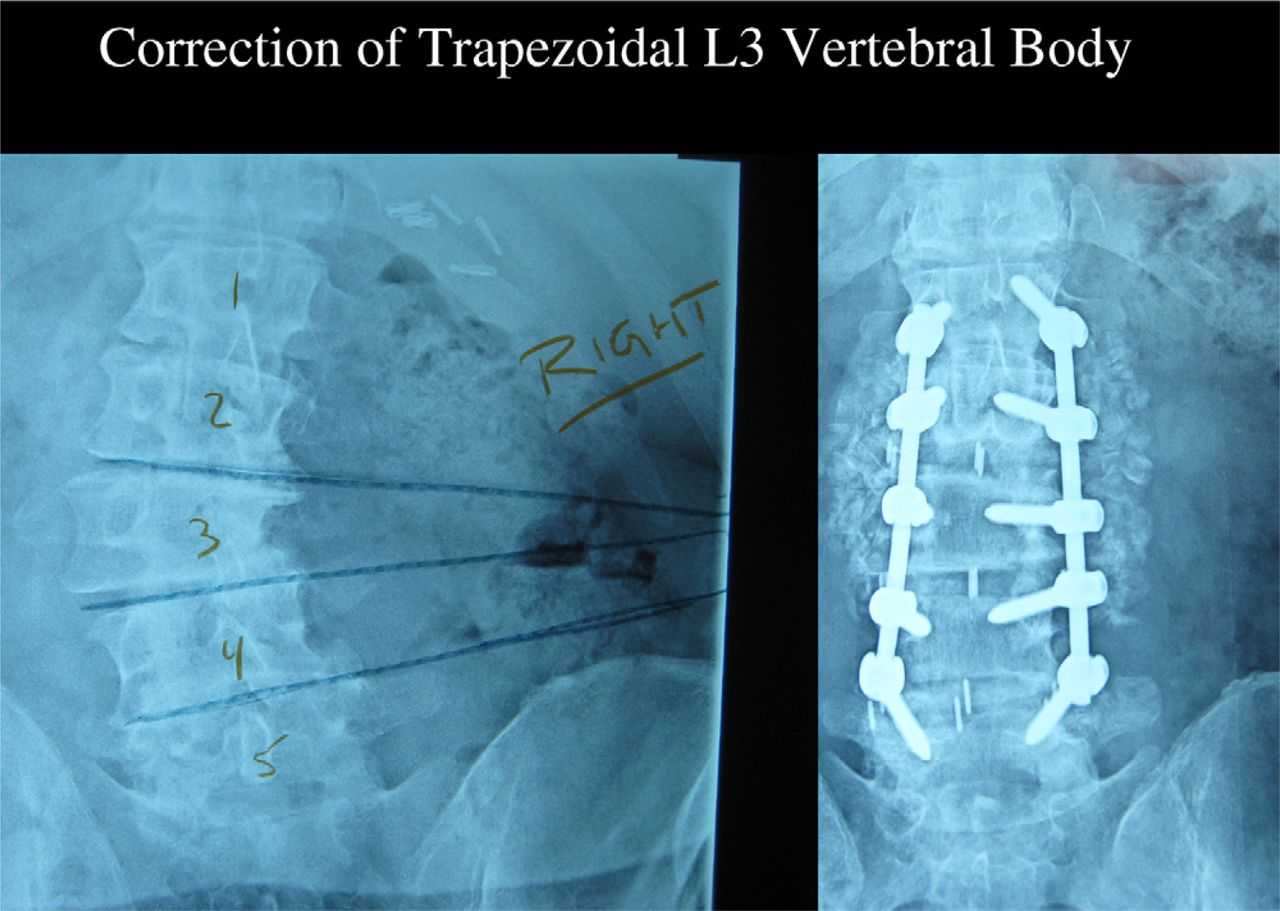
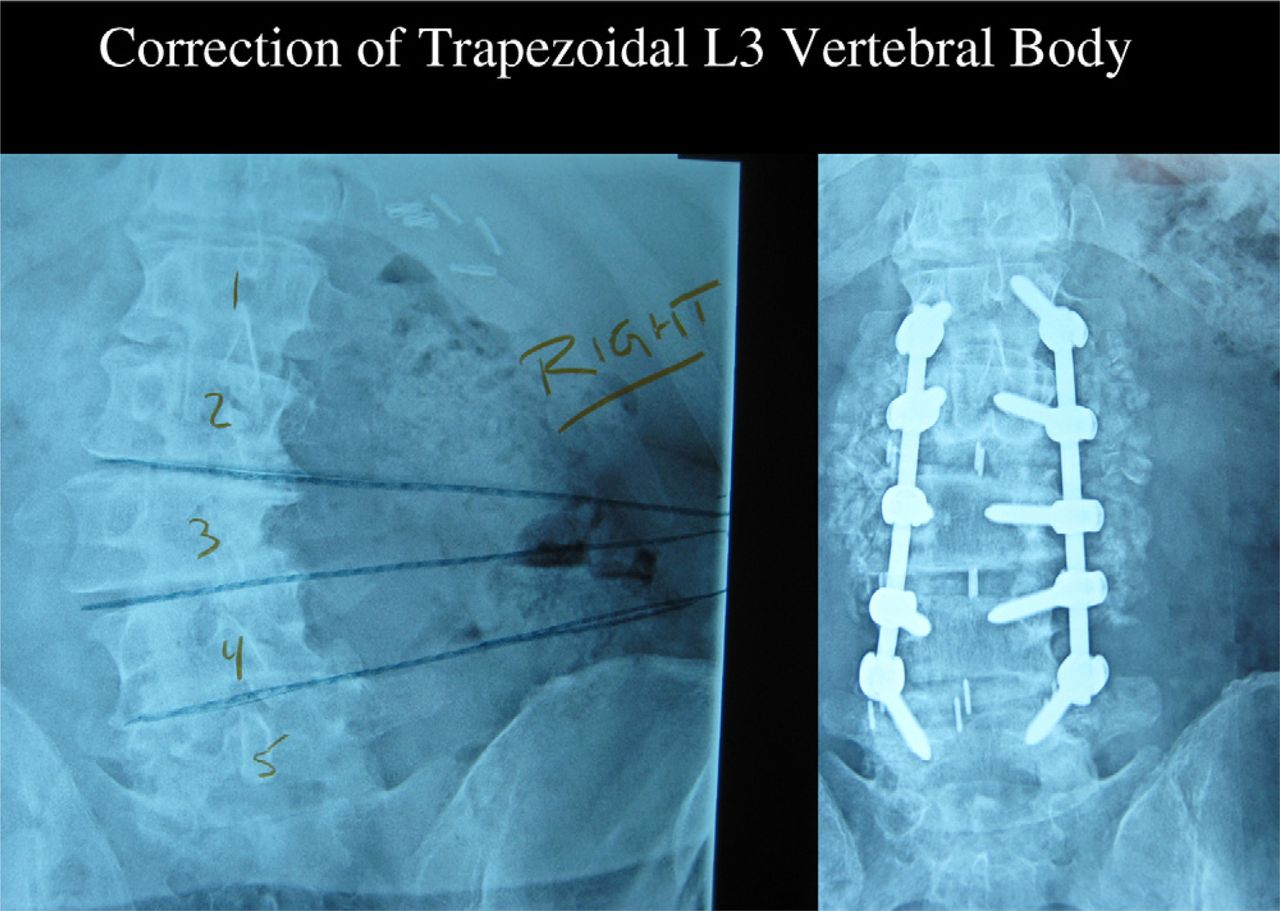
- Fig. 3
Correction of an L3 trapezoid-shaped vertebral body also needs to be performed by posterior shortening with multilevel osteotomies. Supplemental posterior osteotomies and pedicle screw instrumentation were necessary to restore 40° of physiologic lumbar lordosis.
- Fig. 4
Multiple-level XLIF with supplemental posterior instrumentation reduced the scoliotic deformity from 47° down to 5°, and the grade II L3–4 lateral listhesis was also well corrected. The combined 3-dimensional deformity correction added over 3 cm of lumbar height.
- Fig. 5
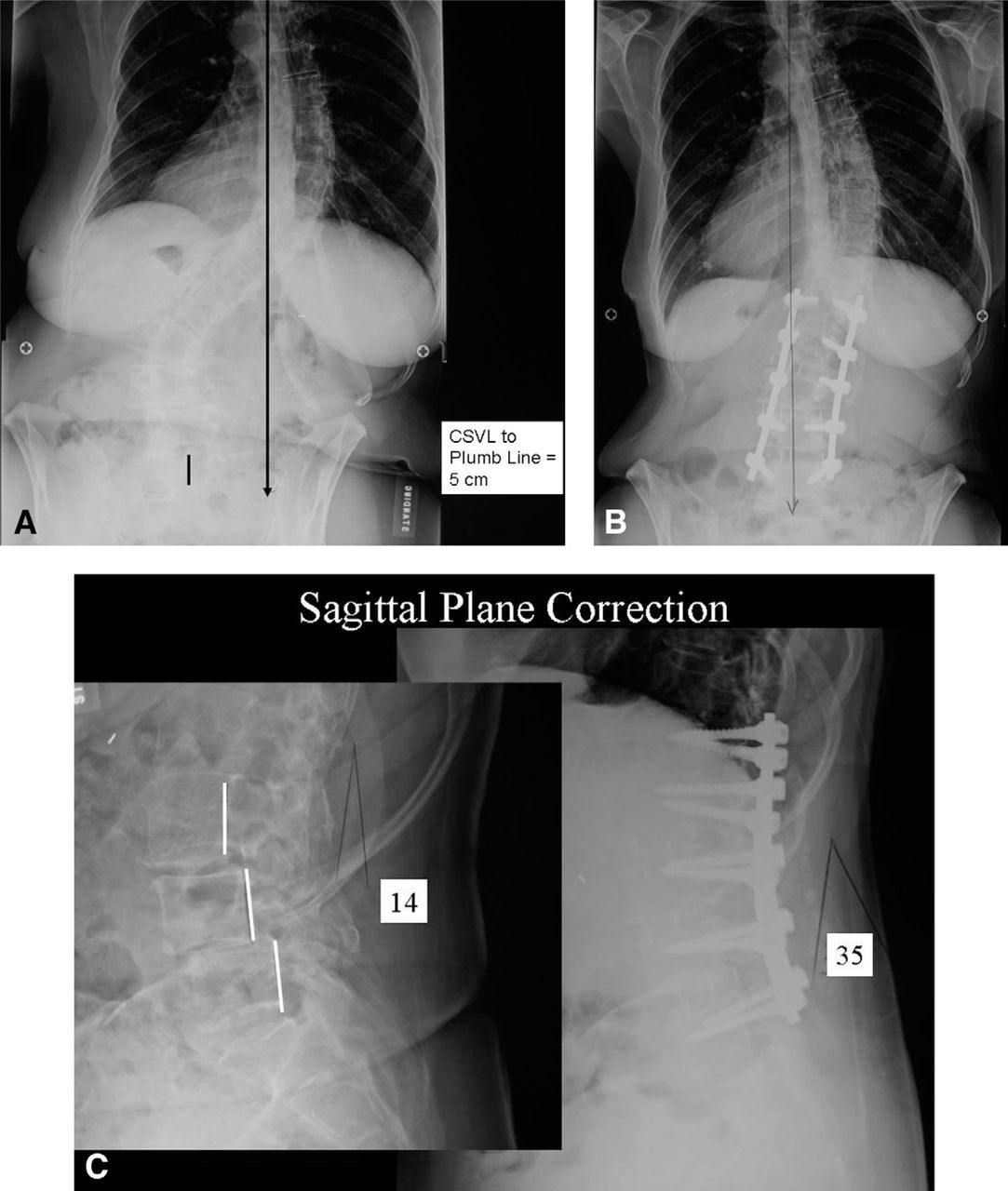
Case 8. (A) A 63-year-old woman presented with a 55° lumbar scoliosis, grade I L3–4 spondylolisthesis, and grade I L4–5 spondylolisthesis, and the central sacral vertical line (CSVL) distance to the vertical plumb line equaled 5 cm. (B) Postoperatively, the patient's sagittal vertical plumb line directly bisected her pelvis. Her scoliosis has been corrected to 15°. (C) Her lumbar lordosis of 14° was corrected to 35°.
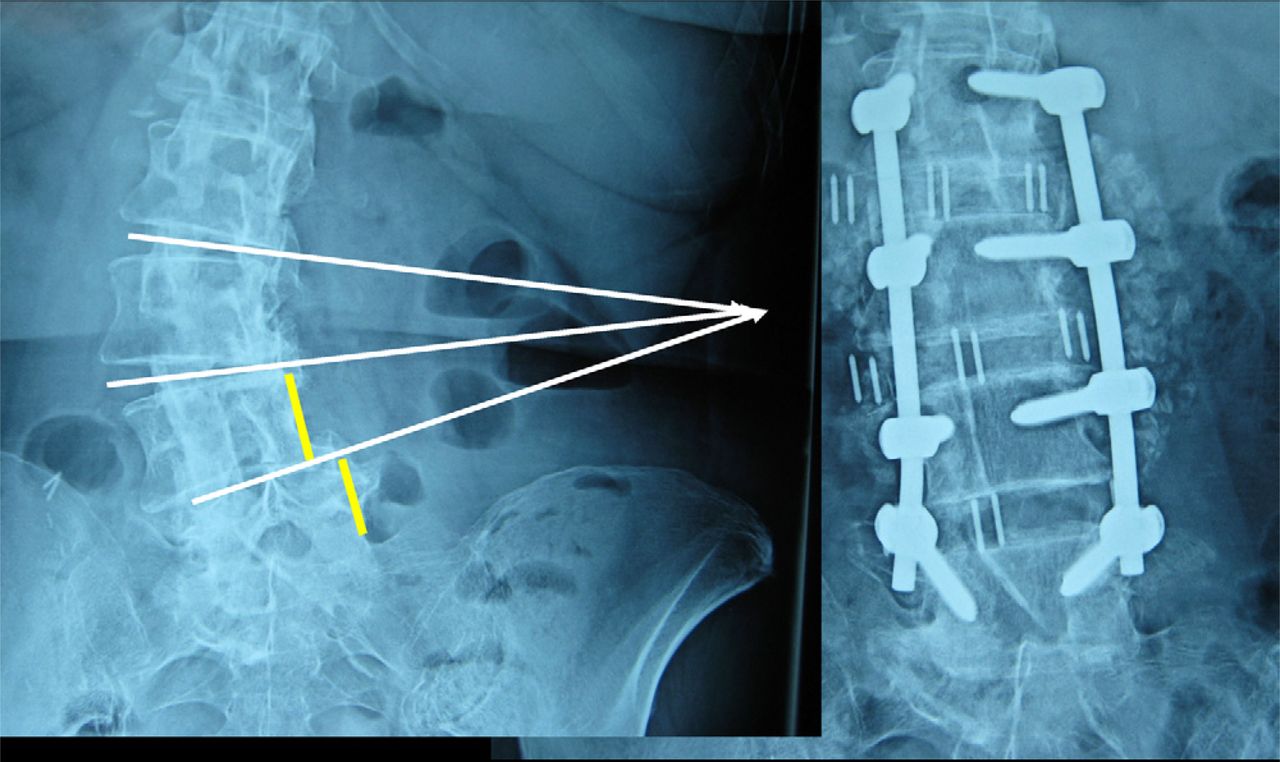
- Fig. 6
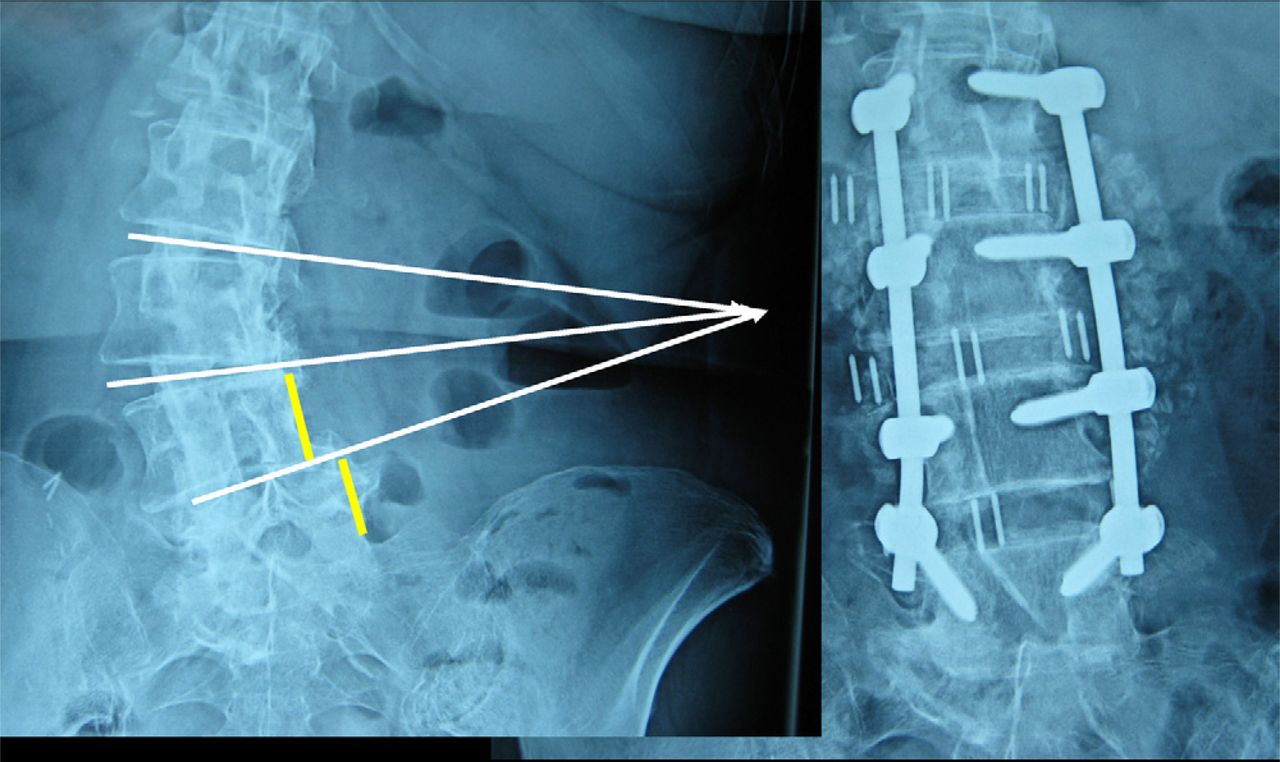
Case 3. The preoperative and postoperative lumbar radiographs show effective correction of both the lateral L4–5 listhesis and the 40° lumbar scoliosis using 3-level XLIF and L2–5 posterior instrumentation and fusion. One should note the convergence, or “pointing,” of the scoliotic disk spaces toward a confined area on the concave flank—this provides for a more minimally invasive surgery than the historical convex “extensile” approach.




Tables
Case No. Age (yr) Classification Preop diagnosis Operative detail No. of levels of XLIF spacers Levels of spacers Decompression laminectomy 1 67 Severe scoliosis + deformity, spondylosis Lateral listhesis cm out of balance, extreme claudication XLIF cage + Armada (Nuvasive, San Diego, CA) 4 L1–5 L3, L4, L5 2 66 Severe scoliosis + deformity, spondylosis Scoliosis, lateral listhesis, stenosis, instability XLIF cage Armada 4 L1–5 L3, L4, L5 3 76 Severe scoliosis deformity, spondylosis 40° lumbar scoliosis, synovial cyst at L4–5 XLIF cages + Armada 3 L2–5 L3, L4, L5 4 55 Severe scoliosis + deformity, spondylosis Spondylo at L4–42° scoliosis XLIF cages + Armada 4 L1–5 L3, L4, L5 5 68 Severe scoliosis + deformity, spondylosis 48° scoliosis, GII L3/lateral listhesis, stenosis XLIF cages + Armada 4 L1–5 L2, L3, L4, L5 6 69 Severe scoliosis + deformity, spondylosis Grade I spondylolisthesis, post-laminectomy syndrome, lumbar scoliosis XLIF cages + Armada 3 L2–5 L3, L4, L5 7 77 Scoliosis, spondylolisthesis + lateral subluxation GI L4–spondylo XLIF cage + Armada 3 L2–5 L4, L5 8 63 Post-laminectomy syndrome at L3, L4, L5 GI L3–and GII L4–5 spondylo 40° scoliosis XLIF cage + Armada 3 L2–5 L3, L4, L5 9 64 Scoliosis, spondylolisthesis + lateral subluxation GI L4–spondylo XLIF cages + Armada 3 L2–5 L3, L4, L5 10 48 Scoliosis, spondylolisthesis + lateral subluxation L2 retrolisthesis, L3 by 1 cm XLIF cages + percutaneous screws 2 L2–4 None 11 62 Scoliosis, spondylolisthesis + lateral subluxation Scoliosis and L3–4 spondylo XLIF cages Revere (Globus Medical, Audubon, PA) 3 L2–5 L3, L4, L5 12 71 Prior VSP instrumentation L2–3 and L4–5 retrolisthesis, 1 cm each XLIF cages + Armada 4 L1–S1 L3, L4, L5 13 71 Degenerative scoliosis Scoliosis and L3–4 spondylo XLIF cage + Armada 3 L1–5 L4, L5 14 78 Post-laminectomy syndrome and prior VSP at L3–5 L1–2 retrolisthesis and L2–3 retrolisthesis XLIF cage + Armada 2 L1–5 L3, L4, L5 15 41 Post-laminectomy syndrome and prior CD at L4–S1 Spondylo at L5-S1 and scoliosis XLIF cages + Armada 2 L2–S1 L4, L5 16 68 Scoliosis, spondylolisthesis + lateral subluxation Scoliosis and lateral listhesis at L2–3 and L4–5 XLIF cages + Armada 3 L1–S1 L3, L4, L5 17 66 Scoliosis, spondylolisthesis + lateral subluxation Scoliosis and L3–lateral, L2–3 1-cm retrolisthesis, OOB XLIF cages + Armada 4 L1–S1 L3, L4, L5 18 64 Scoliosis, spondylolisthesis + lateral subluxation Scoliosis on right side XLIF cages + Armada 3 L2–5 L3, L4, L5 19 61 Scoliosis, spondylolisthesis + lateral subluxation Retrolisthesis at L4–5 and scoliosis XLIF cage + Armada 3 L2–5 L4, L5 20 73 Post-laminectomy syndrome at L3, L4, L5 Scoliosis stenosis XLIF cage + Armada 3 L2–5 L4, L5 21 62 Scoliosis, spondylolisthesis + lateral subluxation GI L2–3 and L4–5 spondylo scoliosis XLIF cages + Armada 3 L2–5 L3, L4, L5 22 67 HNP at T12–L1 and adjacent segment with instrumentation GII retrolisthesis at L2–3 and HNP at T12–L1 XLIF cages + Armada 3 T12–L3 L2, L3, L4, L5 23 72 Scoliosis, spondylolisthesis + lateral subluxation L3–4 subluxation, post-laminectomy syndrome XLIF cages + Armada 4 T12–L5 L3, L4, L5 24 68 Scoliosis, spondylolisthesis + lateral subluxation Degenerative scoliosis XLIF cages + Armada 3 L2–5 L3, L4, L5 25 70 Scoliosis, spondylolisthesis + lateral subluxation Post-laminectomy syndrome XLIF cages + Armada 2 L2–4 L3, L4, L5 Mean 65.9 3.12 Abbreviations: GI, grade 1; GII, grade II; Postop, postoperative; Preop, preoperative; CD, Cotrel Dubousset; HNP, Herniated Nucleus Pulposis; OOB, out of bed; VAP, variable spinal plate. Levels of posterior instrumentation Lateral listhesis Preop scoliosis (°) Postop scoliosis Preop OOB (cm) Postop OOB Mean length of hospital stay (d) Mean blood loss (cc) Length of surgery (min) Preop VAS score Postop VAS score T12–L5 GII L3 to right of L4 47 5 2 0 6 3100 378 80 5 L1–5 GII L3 to left of L4 40 6 2 0 13 3600 393 85 3 L2–5 GI L4 to left of L5 40 3 3 0 4 900 234 60 7 L1–5 GI L3 to left of L4 42 4 3 0 7 1700 337 90 0 T12–L5 GII L3 to left of 48 7 3 0 4 600 266 60 5 L4 L1–5 GI L3 to right of L4 40 5 2 0 7 900 325 90 10 L2–5 GI L4–5 anterior and lateral 42 4 2 0 3 600 130 90 30 L1–5 GI L3–4 lateral, GI L4–5 lateral 55 15 5 0 4 800 259 80 10 L2–5 GI L4–5 anterior and lateral 40 2 0 9 (reoperation on day 5) 1100 268 90 30 L2–5 L2–3 40 0 2 0 4 150 192 90 20 L2–5 L4–5 1 cm 43 6 2 0 3 1700 315 100 10 L1–S1 L4–5 GI 41 3 2 0 3 50 120 60 40 L1–5 L3 right of GI L4 43 8 0 0 4 1500 278 60 40 L1–5 GI L1–2 and L2–3 40 0 2 0 5 350 143 90 20 L2–5 L2–3 + L3–4 40 4 2 0 3 50 75 80 60 L1–5 GI L–3, L3–4, and L4–5 48 10 2 0 5 550 377 60 0 L1–S1 GII L3–4 40 8 4 0 4 1100 344 70 80 L2–5 L2–3 42 0 2 0 7 700 218 100 50 L2–5 Retrolisthesis and lateral at L2–3 + L4–5, 1 cm each 45 10 2 0 3 600 136 90 30 L2–5 L3–4 40 0 2 0 7 750 201 90 70 L2–5 L4–5 40 5 2 0 3 500 150 40 80 T11–L5 GII retrolisthesis at L2–3 43 2 2 0 4 650 242 70 30 L2–5 GII L3–4 53 10 5 2 4 1400 263 90 50 L2–5 L4–5 40 4 2 0 4 300 143 30 0 L2–5 Retrolisthesis and lateral subluxation L3–4 41 3 2 0 3 300 123 100 80 42.9 5.08 2.32 0.08 4.75 958 236 77.8 30.4 Consideration Convex Concave Proponents Dwyer, Zielke, Kaneda McAfee, Pimenta, Akbarnia Distance from spine to skin Apex of curve is closer to skin incision Concave bridging osteophytes are closer to skin incision Size of approach More “extensile” due to diverging direction of disk Minimally invasive surgery due to converging pointing of spaces disk spaces (Fig. 6) OR positioning Flat lateral decubitus
Hinging OR table accentuates deformityHinged radiolucent table
OR table assists reduction of scoliosis and lateral subluxationBridging osteophytes Key area requiring osteotomies are on contralateral side of disk space Ipsilateral disk space Direct vision Instrumentation Instrumentation is on “tension” side of scoliotic curvature so rods bear correction force Load-bearing PEEK implants with large footprint maintain correction—spacers counteract compression Ideal curve More useful in thoracolumbar spine (apex T12 or L1) due to production of kyphosis Lumbar curves (apex L2 + below), more effective restoration of lumbar lordosis Abbreviations: OR, operating room; PEEK, polyetheretherketone.
Adult idiopathic scoliosis Adult degenerative scoliosis (de novo scoliosis) Younger age at presentation De novo scoliosis develops in 68% of adults aged >60 yr (Schwab et al.24) Can have associated congenital elements Disk space collapse, vertebral wedging Disk space height maintained Facet degeneration Thoracolumbar scoliosis (apex T12 or L1) Lumbar scoliosis (apex L2 or below) SRS definition Mechanical back pain predominates Radiculopathy and claudication Pedicular kinking and stretching of nerve roots Direct nerve root compression from spinal stenosis (magnetic resonance imaging required) Rotational deformity more pronounced Rotary subluxation more prominent Translation unusual Spondylolisthesis and lateral subluxation particularly at L3-4 and L4-5 are characteristic Coronal-plane deformity predominates Multiplanar 3-dimensional deformity (coronal, sagittal, and transverse) More apt to extend into thoracic spine Usually confined to lumbar spine as degenerative disk disease is more extensive Usually develops in absence of prior surgery Often associated with post-laminectomy syndrome due to prior degenerative changes Approach on convex side Approach on concave side SRS, Scoliosis Research Society.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}