


Article Figures & Data
Figures
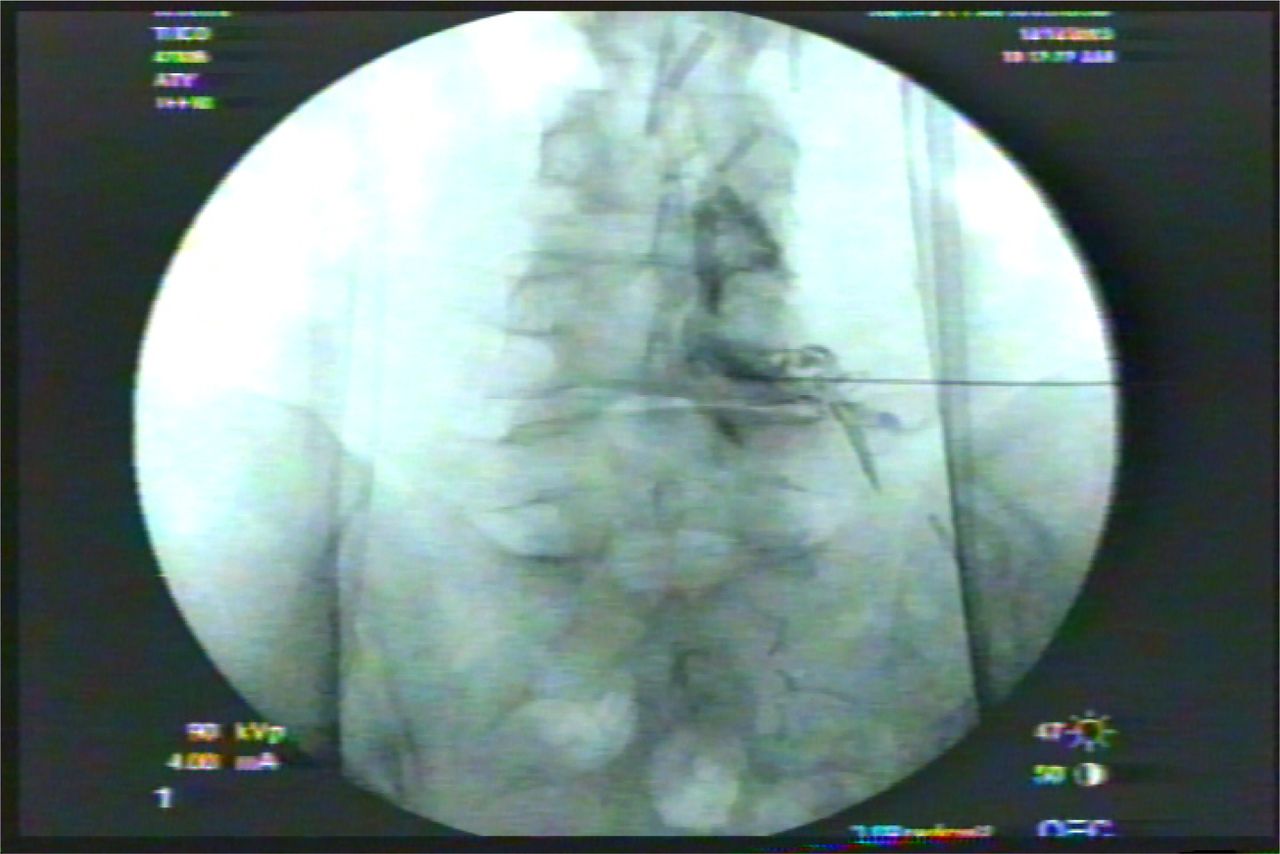
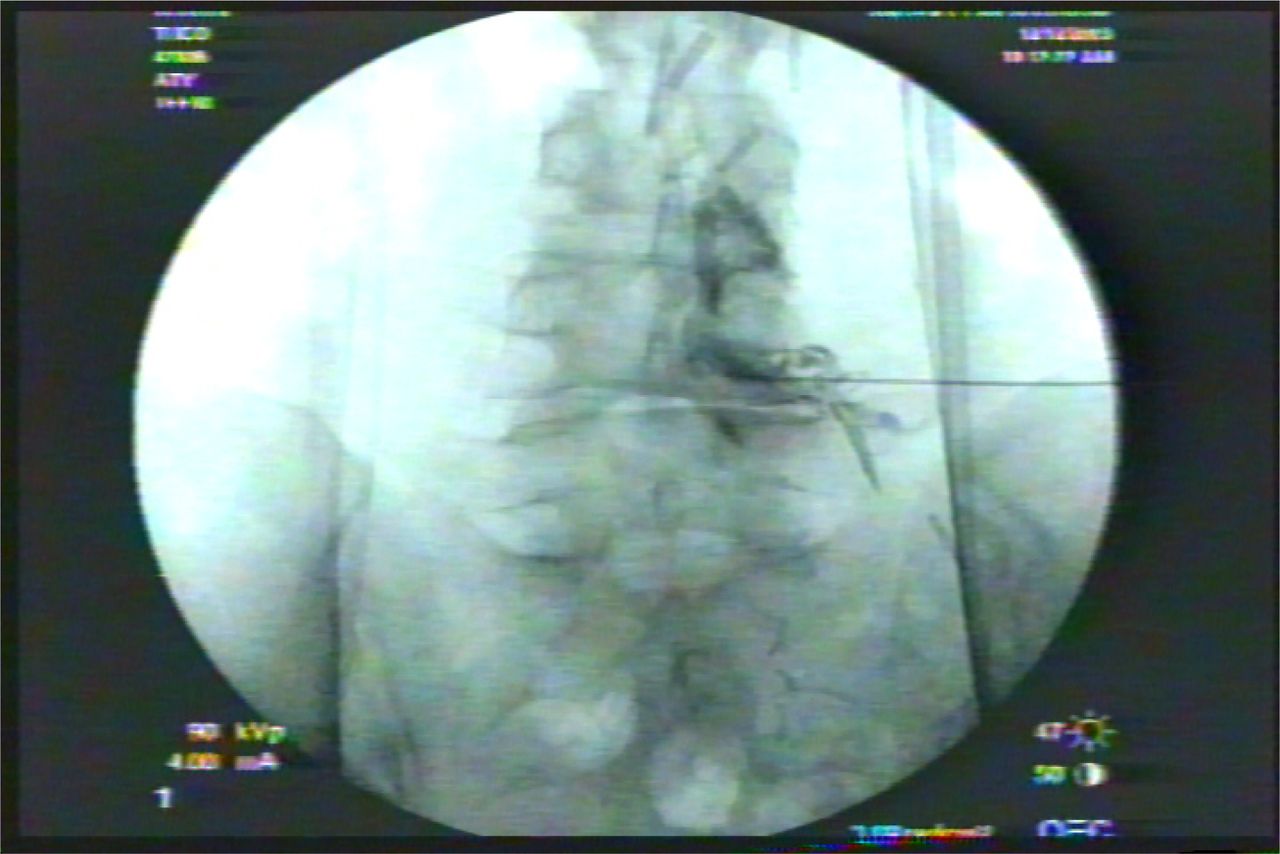
- Fig. 1
A diagnostic and therapeutic epidural gram may help identify unrecognized lateral recess stenosis underestimated by MRI. An excellent result from a therapeutic block lends excellent prognosis for a more lasting and “permanent” result from transforaminal endoscopic lateral recess decompression.
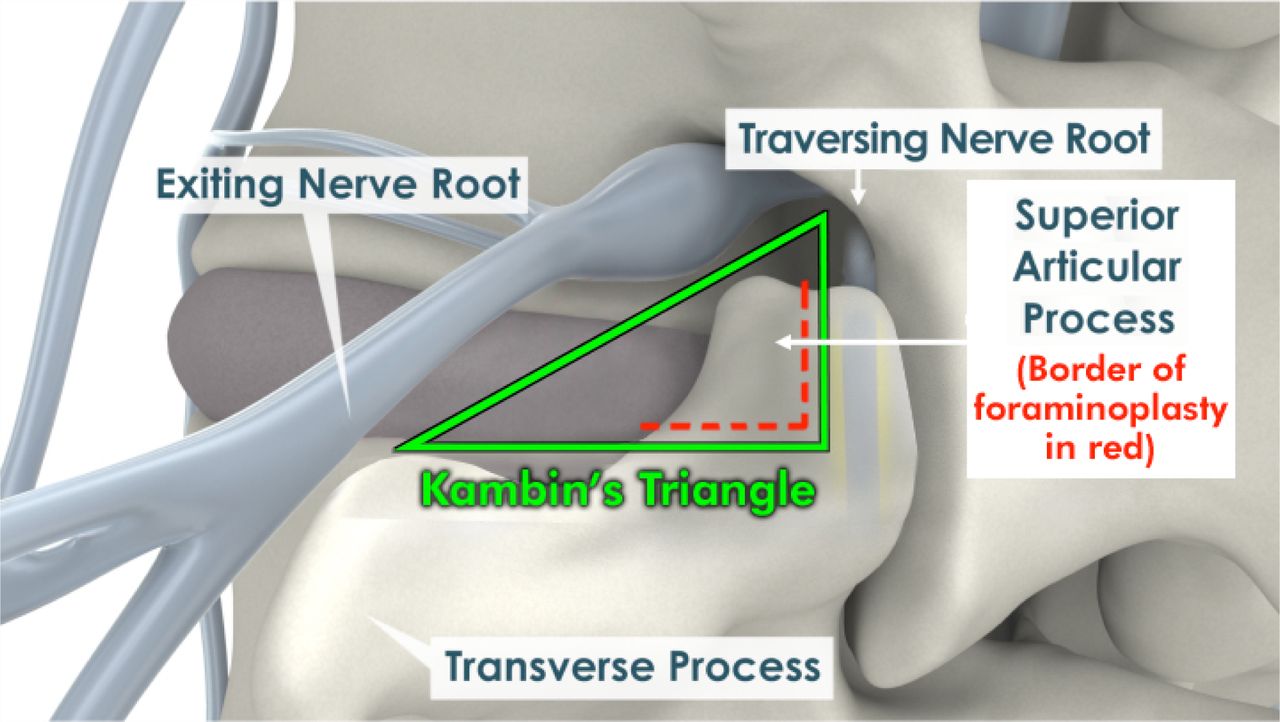
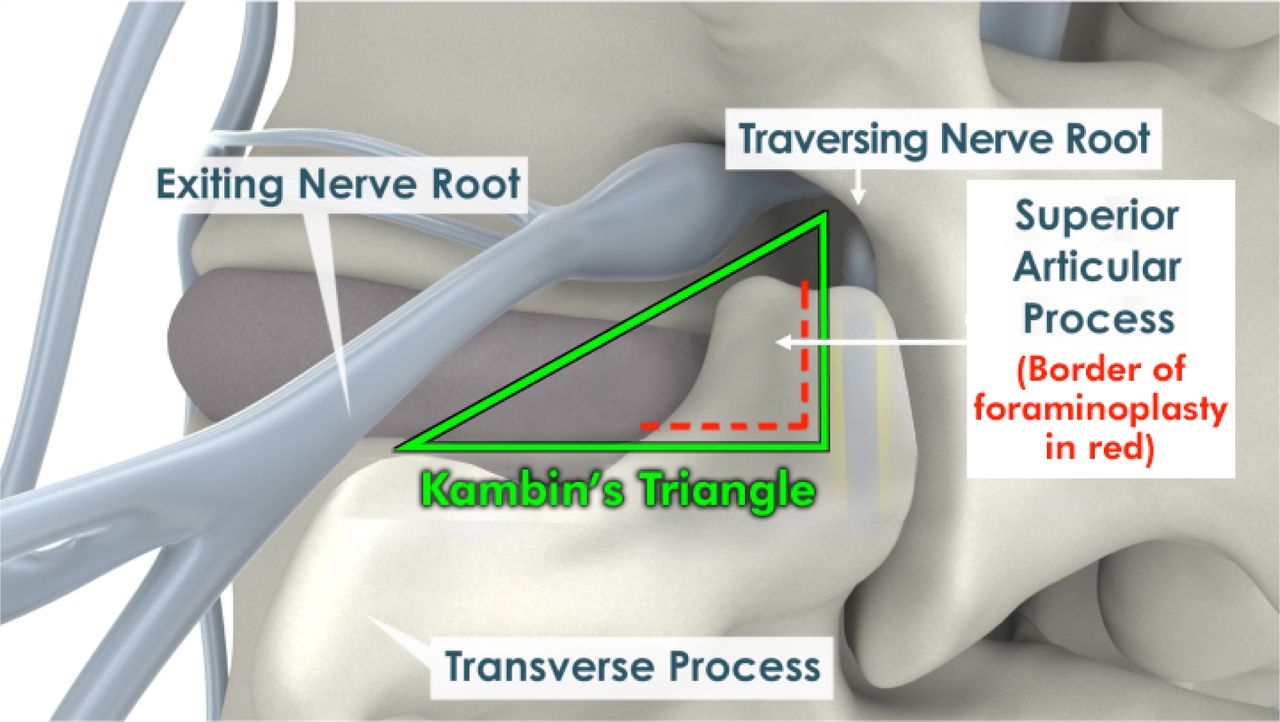
- Fig. 2
Kambin's Triangle provides access to the “hidden zone” of Macnab by foraminoplasty. The foramen and lateral recess is decompressed by removing the ventral aspect and tip of the superior articular process to gain access to the axilla between the traversing and exiting nerve. FBSS contains patho-anatomy in the axilla between the traversing and exiting nerve that hides the pain generators of FBSS.
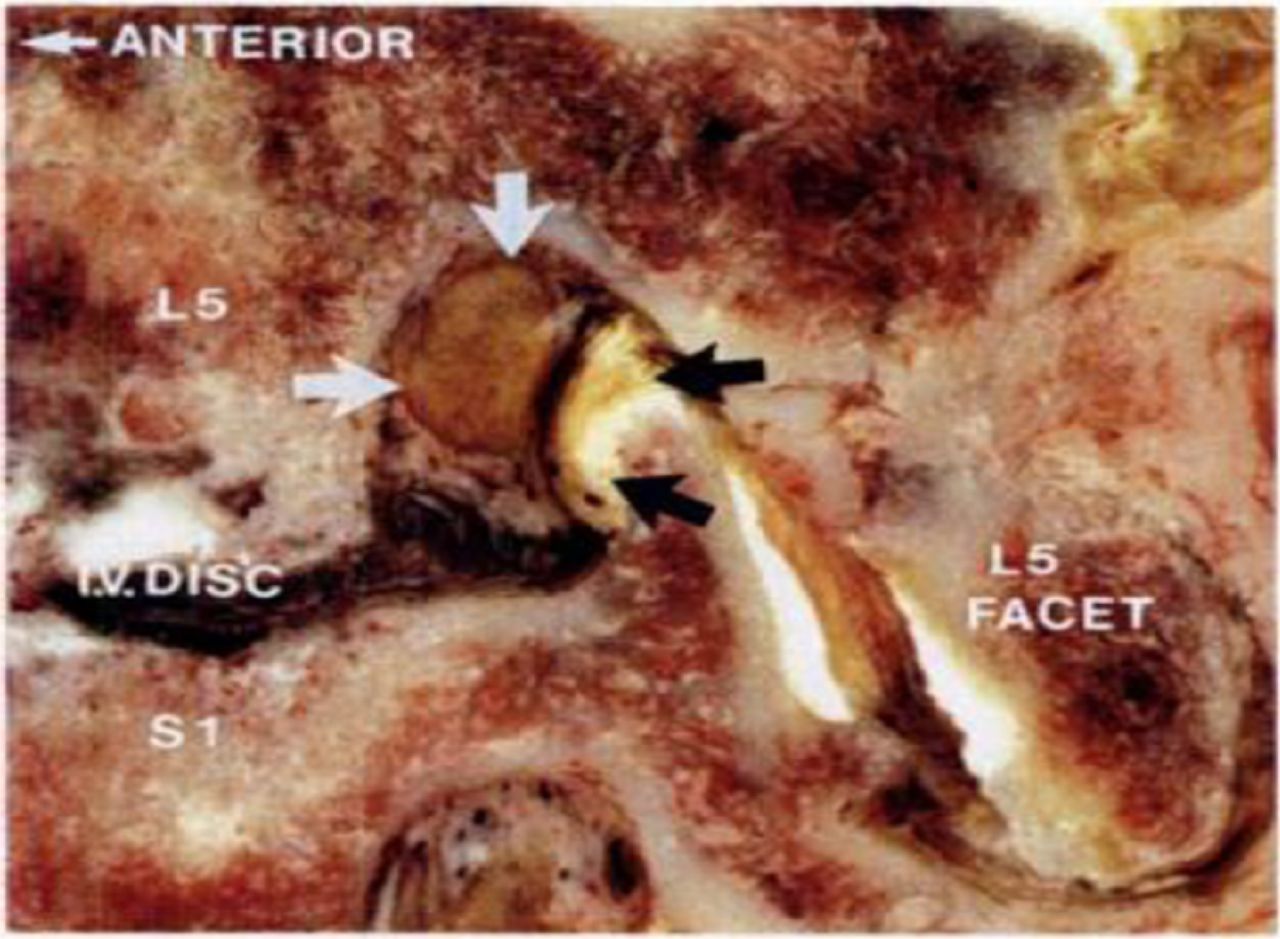
- Fig. 3
Cadaver Illustration of Foraminal Stenosis (courtesy of Wolfgang Rauschning). As the disc narrows, the superior articular process impinges on the exiting nerve and DRG, creating lateral recess stenosis, lumbar spondylosis, and facet arthrosis.
- Fig. 4
MRI of FBSS following two open decompressions from midline and Wiltse approach. Patient had residual symptoms of numbness from persistent lateral stenosis.
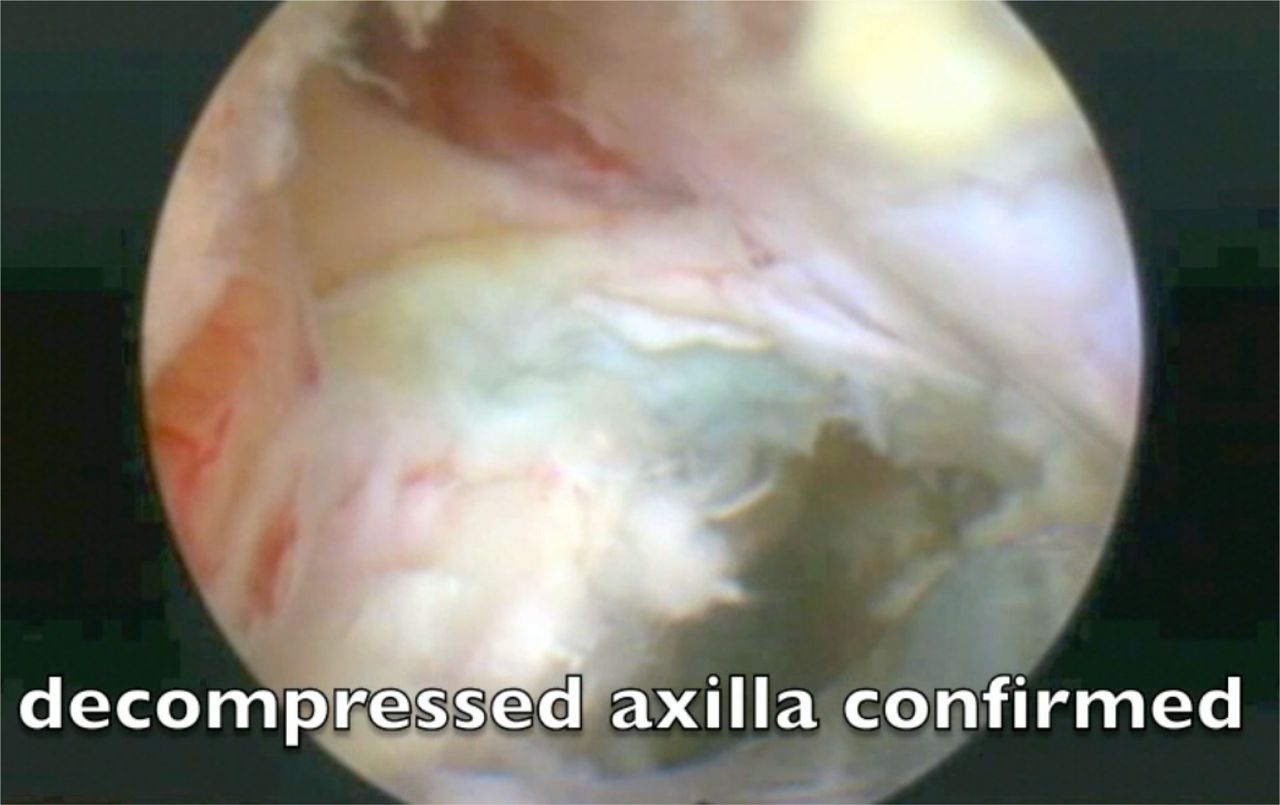
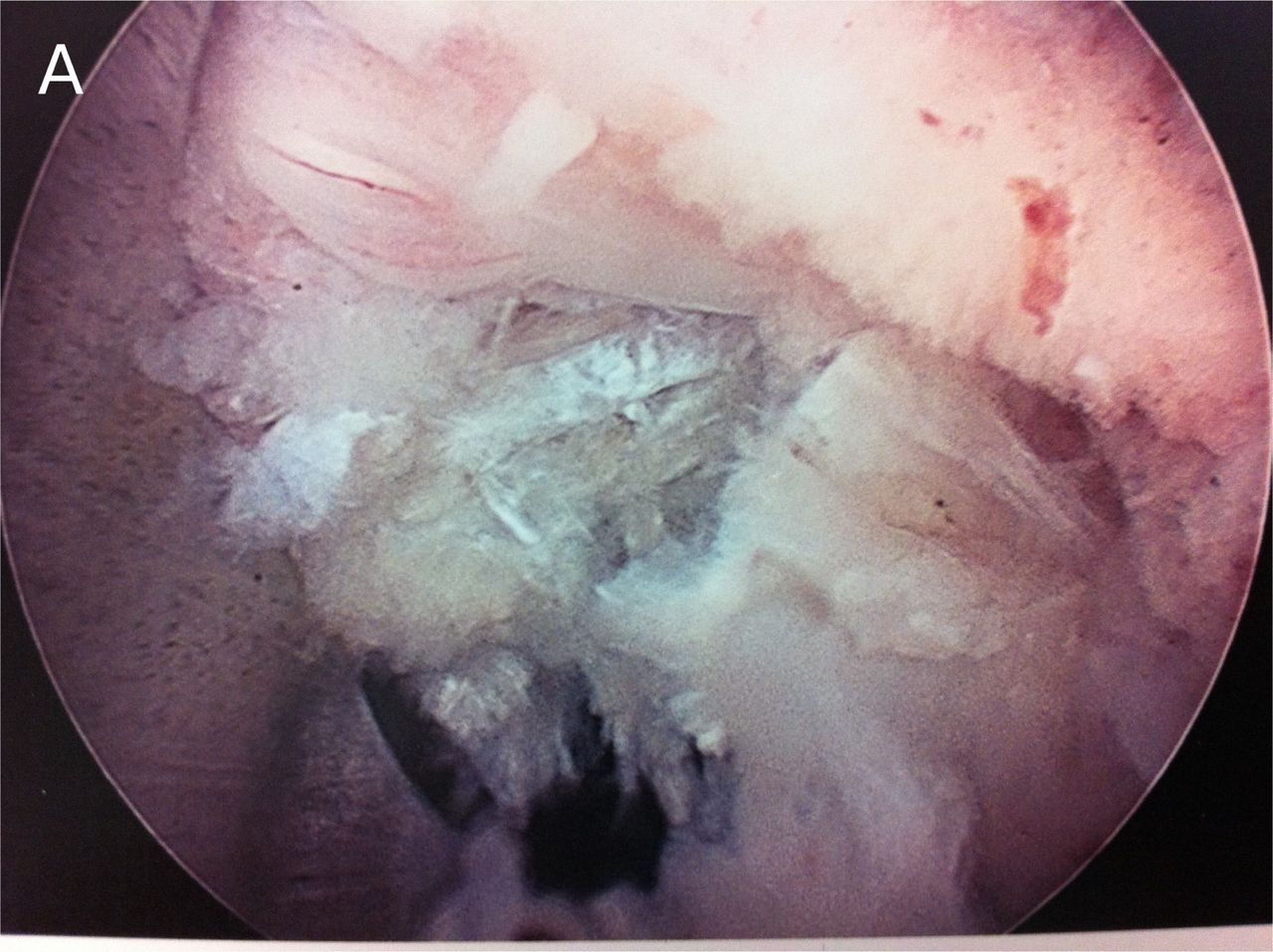
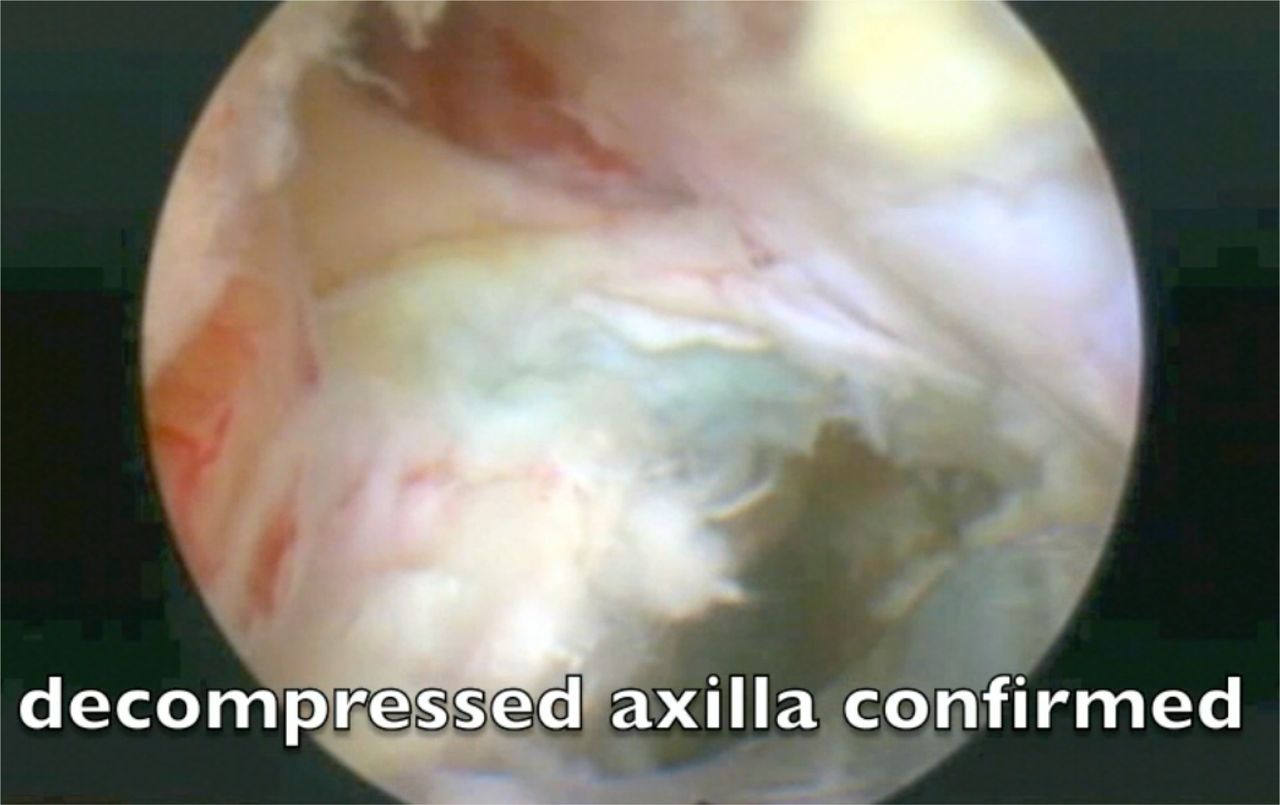
- Fig. 5
The axilla between the traversing and exiting nerve is the location of missed patho-anatomy in FBSS. Image of a completely decompressed axilla will allow the surgeon to see that both exiting and traversing nerve are decompressed, and FBSS from patho-anatomy in this zone known as the “hidden zone,” when decompressed, will resolve FBSS from residual/recurrent HNP and lateral recess stenosis.
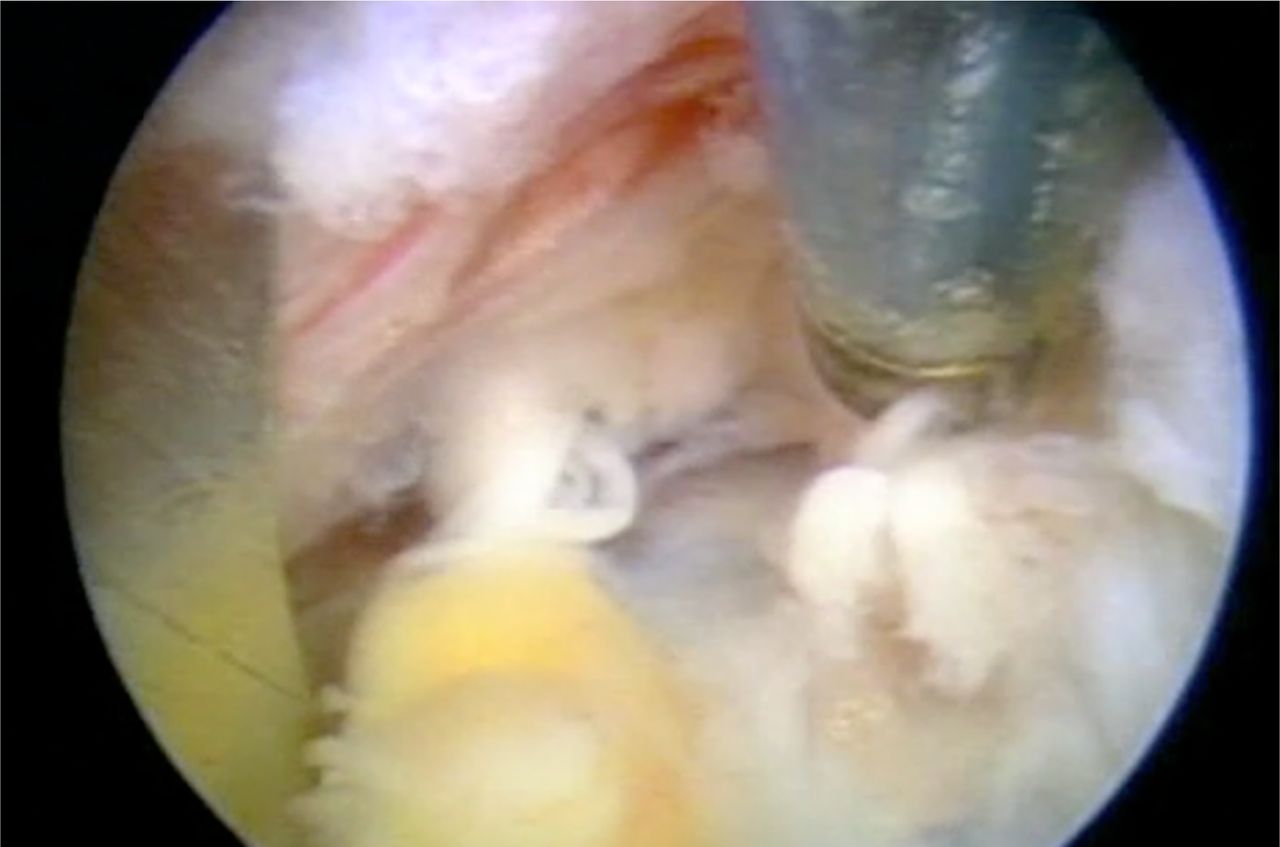
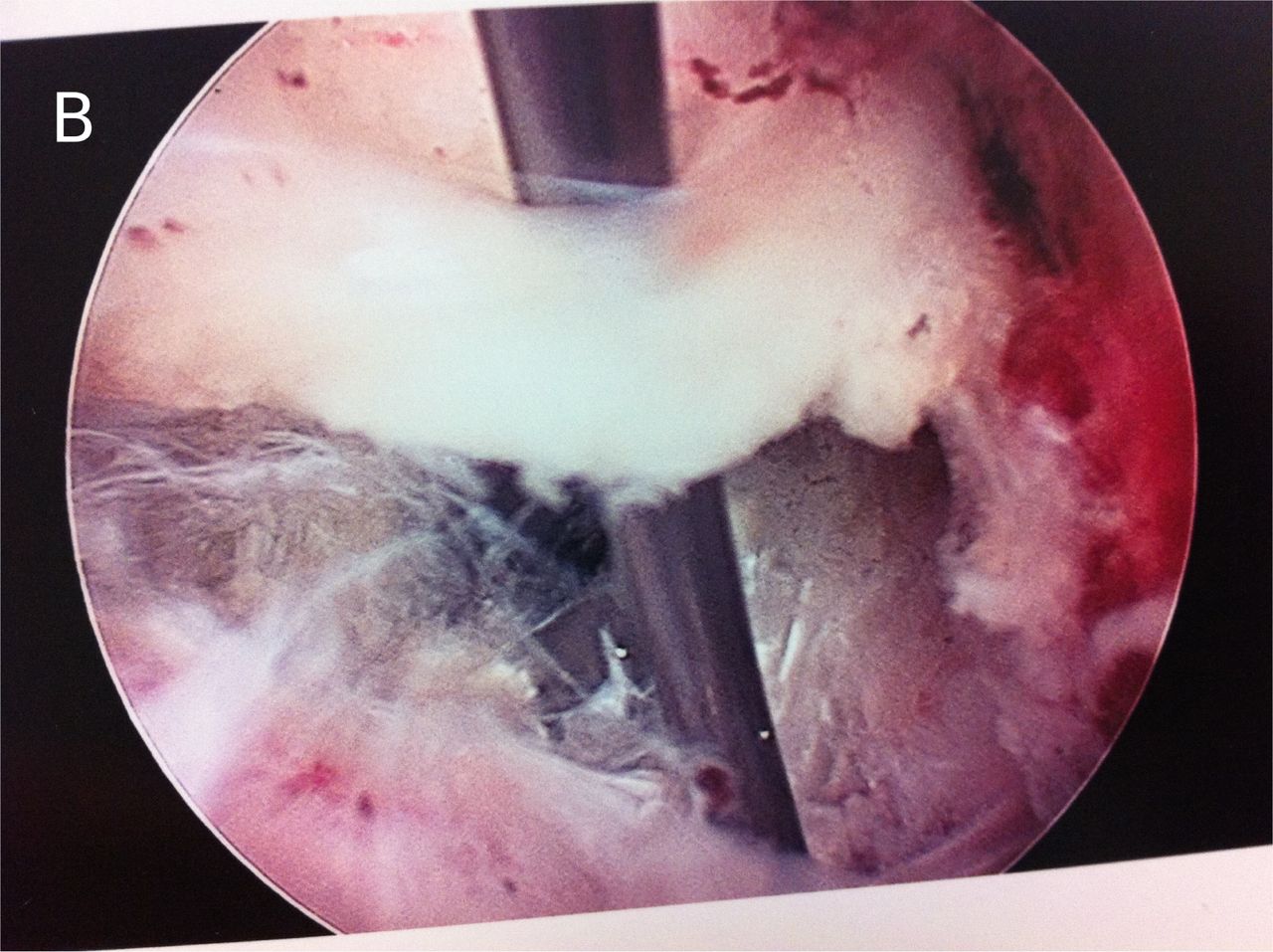
- Fig. 6
View after extensive decompressing the ventral SAP after FBSS. Although medial translaminar decompression provides good access to the medial epidural space and the traversing nerve, further decompression through a transforaminal approach is sometimes, needed. Here transforaminal decompression confirms complete decompression of the nerve and the dura above, in a patient with residual sciatica following traditional decompression, but improving the patient further with by decompressing the lateral recess further to expose the lateral aspect of the foramen. A calcified annulus was also found. The medial capsule and ligamentum flavum usually protects the lateral edge of the traversing nerve and dura. Here, it was lifted up to visualize the nerve in the epidural space.
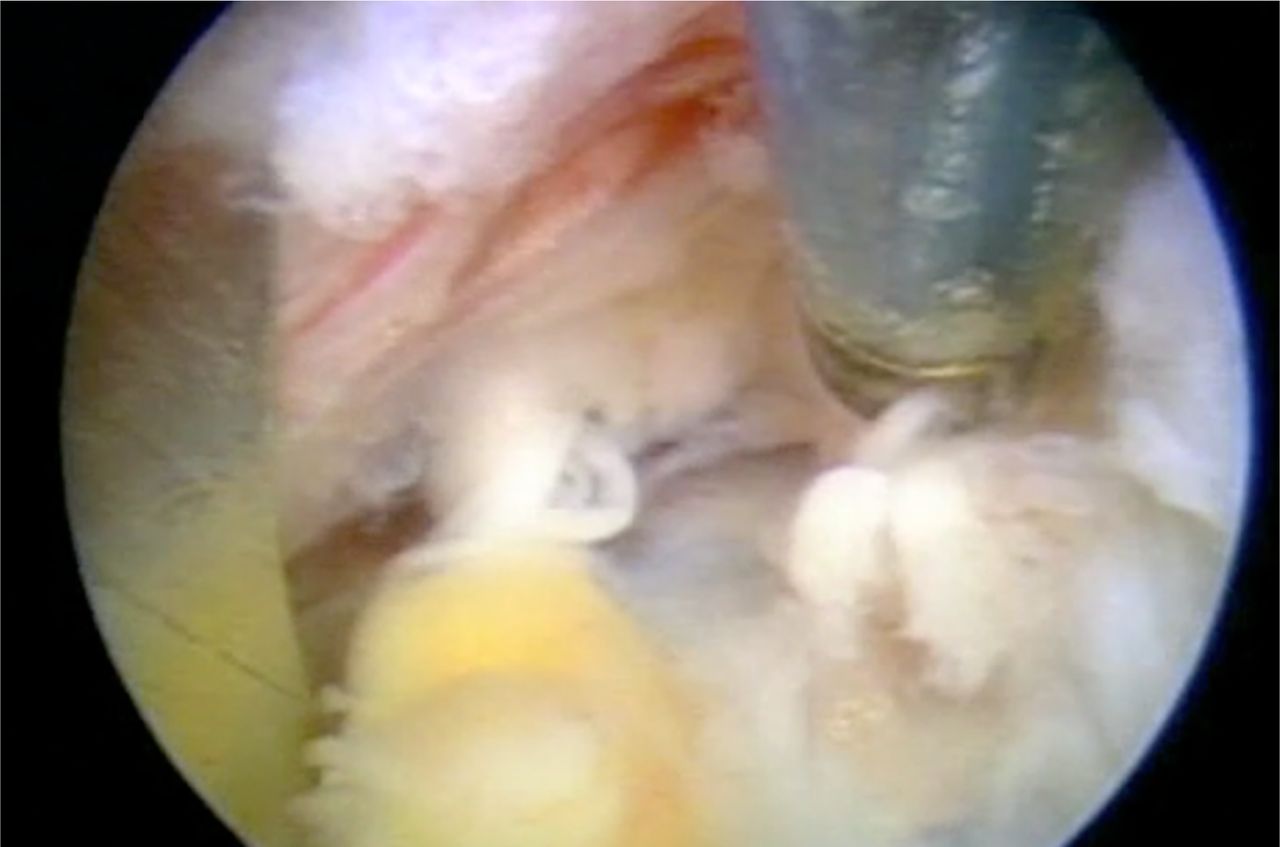
- Fig. 7
The axilla contains hidden patho-anatomy such as foraminal disc protrusions, synovial cysts and in this example a rare neuroma of the dorsal ramus is visualized in the in the axilla of the foramen at the L4-5 spinal level. The dorsal ramus is easily mistaken for a furcal nerve.
- Fig. 8
Cadaver dissection of the Dorsal Ramus and its branches ventral to the intertransverse ligament. One medial branch crosses the transverse process, as does the intermediate and lateral branch. Other branches are demonstrated to reach the facet from the foramen ventral to the intertransverse ligament. Location of the branches is most consistent as described by Bogduk, but various locations and configurations are common.
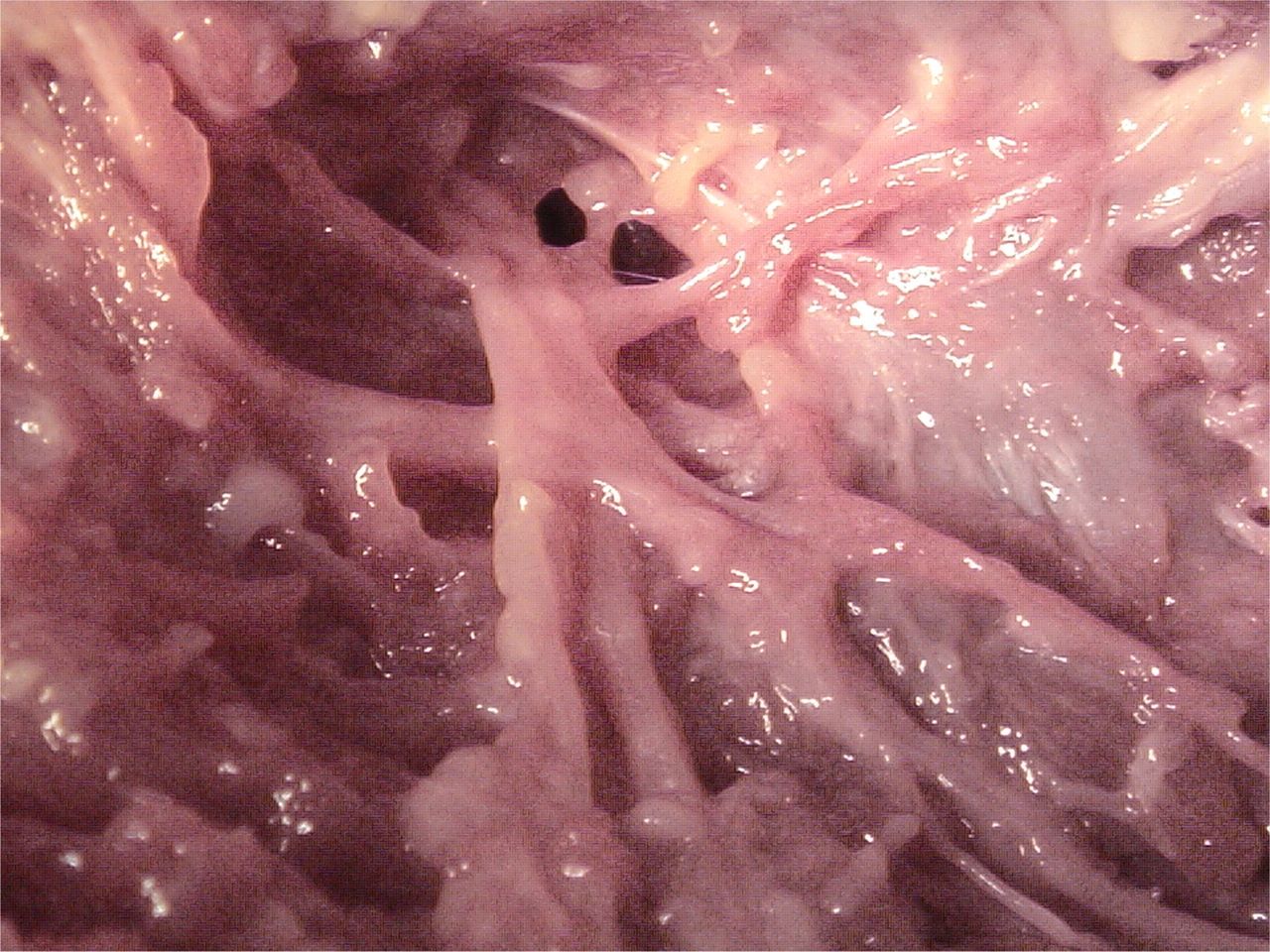
- Fig. 9a
Medial branch of the dorsal ramus visualized in the foramen before it exits the foramen to innervate the facet. This is easily mistaken for a furcal nerve. Complete transection or ablation will not produce dysesthesia as it is a pure sensory nerve. Injury or partial ablation of a furcal nerve will produce temporary dysesthesia.
- Fig. 9b
Medial branch of dorsal ramus in the foramen vs furcal nerve. It is not always possible to differentiate. If the nerve can be traced branching from a spinal nerve ablating it may cause dysesthesia. Usually very small nerves can be cut. It is better to completely transect that to partially ablate the nerve. The exiting nerve is partially visualized at 7 o'clock.
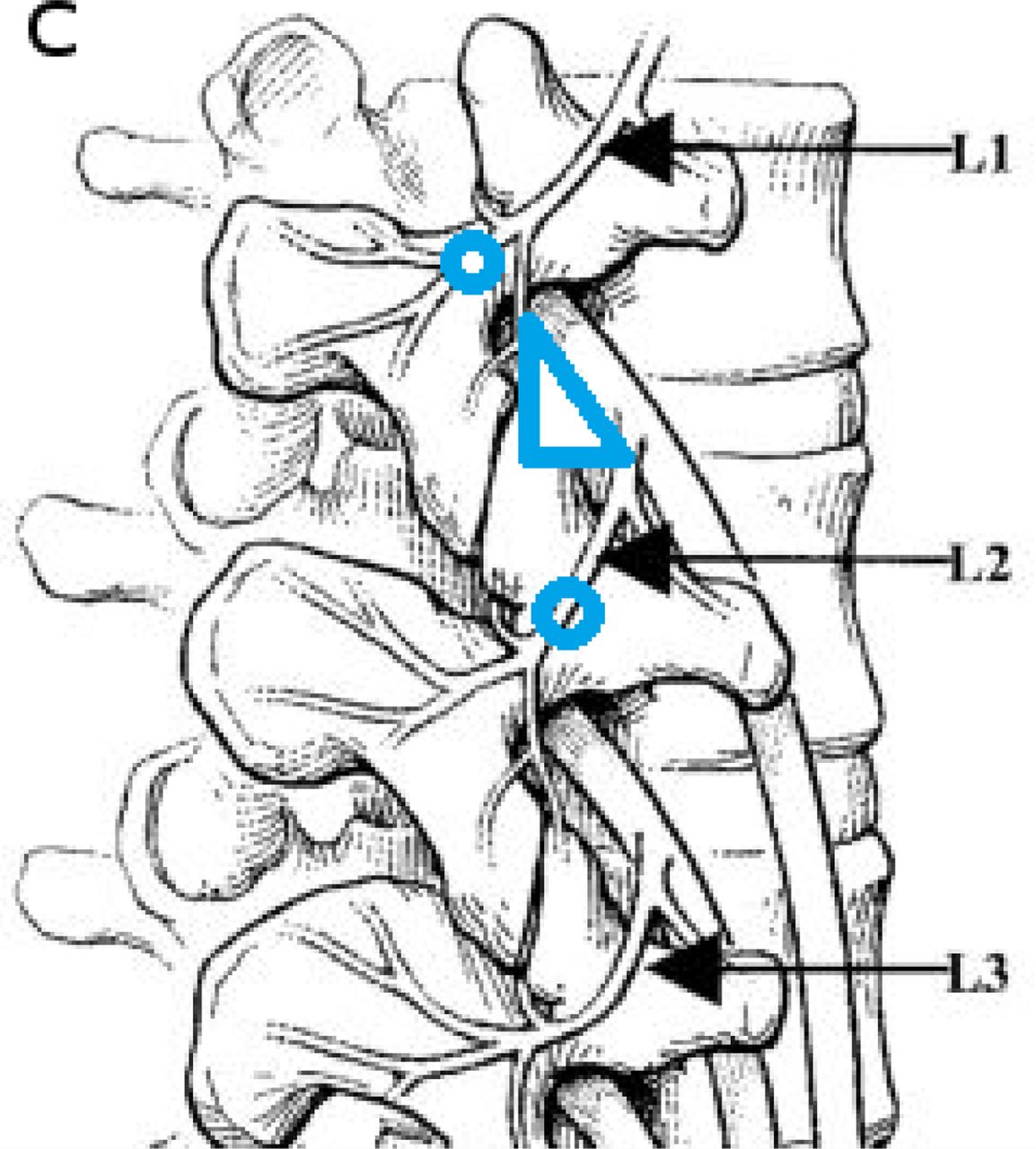
- Fig. 9c
Locations and variations of the branches of the dorsal ramus. Position of the medial branch dorsal ramus in Kambin's triangle (in blue). The target for medial branch ablation on the transverse process is highlighted by the blue circles. The medial branch can be transected or ablated in the foramen as it traverses along the foraminal ligament on the ventral facet before it exits to innervate the joint. The nerve, if transected and provide axial back pain relief during foraminoplasty. These nerves can be mistaken for furcal nerves, that, if less than 1-2 mm, can be ablated without causing dysesthesia. If the nerve causes pain when ablated with bipolar RF, It would be advisable to avoid injuring it, if possible.






In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Long-term Clinical Outcomes Following Endoscopic Foraminoplasty for Patients With Single-Level Foraminal Stenosis of the Lumbar Spine
- Percutaneous Endoscopic Lumbar Discectomy Versus Microdiscectomy for the Treatment of Lumbar Disc Herniation: Pain, Disability, and Complication Rate--A Randomized Clinical Trial