


ABSTRACT
Background: Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is a common surgical procedure for treatment of degenerative spondylolisthesis (DS) but remains controversial for treatment of isthmic spondylolisthesis (IS). Few studies have compared IS and DS outcomes after MIS TLIF. Therefore, the objective of the current study was to compare outcomes of patients with IS and DS after MIS TLIF.
Methods: A retrospective cohort analysis was performed on a prospectively maintained database of patients who underwent a primary, 1-level MIS TLIF for grade I or II IS or DS. Grade I and II DS and grade I IS patients were treated with MIS TLIF via a unilateral tubular approach, whereas the grade II IS patients were treated via a bilateral tubular approach. Differences in patient demographics and preoperative characteristics were assessed using independent sample t tests and χ2 tests. The type of spondylolisthesis and its effect on postoperative outcomes was analyzed using Poisson regression with robust error variance (binary outcomes) or linear regression (continuous outcomes) adjusted for preoperative characteristics. Subgroup analysis comparing grade I IS versus DS and grade II IS versus DS was performed.
Results: A total of 223 patients were included (IS: 62 [27.8%]; DS: 161 [72.2%]). IS patients were younger (P < .001), had a lower comorbidity burden (P < .001), and a greater incidence of grade II spondylolisthesis (P < .001) at L5–S1 (P < .001) than the DS cohort. Patients with IS experienced longer operative times (P < .001) and lower, but not statistically significant, arthrodesis rates compared to the DS cohort. No differences were observed in the remaining preoperative patient characteristics, perioperative or postoperative outcomes.
Conclusions: Despite being younger and having a lower comorbidity burden than the DS cohort, similar outcomes were observed after MIS TLIF for IS patients.
Level of Evidence: 3.
Clinical Relevance: These results suggest MIS TLIF is an appropriate treatment option for IS patients despite the increased instability inherent with IS.
- minimally invasive spine surgery
- transforaminal lumbar interbody fusion
- degenerative spondylolisthesis
- isthmic spondylolisthesis
- unilateral interbody cage
- bilateral interbody cage
- low-grade spondylolisthesis
INTRODUCTION
Spondylolisthesis is a common pathologic disorder of the spine defined by anterolisthesis of the cranial over the caudal vertebra. Several types of spondylolisthesis exist; however, the 2 most commonly observed forms are degenerative (DS) and isthmic (IS) spondylolisthesis (Figure 1).1 Occurring most often at L4–L5 in elderly females, DS is the result of intervertebral disc degeneration and arthritic changes to the facet joints resulting in segmental instability and subsequent anterolisthetic progression. This pathology commonly presents in the fourth and fifth decades of life.1–4 In contrast, IS most commonly occurs in healthy adolescent and young adult athletes as the result of repetitive, hyperextension trauma to the posterior elements. This often results in an acquired bilateral defect, or spondylolysis, of the pars interarticularis at L5 and anterolisthetic progression of L5 over S1.5,6 In conjunction with the intervertebral discs, the main function of the facet joints are to counteract anterior shear and torsion forces at their specific vertebral segment, acting as static stabilizers. Due to the interruption of the posterior elements, a low-grade IS patient has an inherent instability that may result in greater anterolisthetic progression compared to a low-grade DS patient.7–10

Preoperative radiographs demonstrating degenerative spondylolisthesis at L4–L5.
Often managed conservatively, a patient may experience refractory symptoms and elect to undergo surgical treatment, which often requires fusion surgery for definitive management. This can be accomplished in a variety of ways, one of which is minimally invasive (MIS) transforaminal lumbar interbody fusion (TLIF). Despite an initial surgical learning curve, MIS TLIF has enabled surgeons to perform fusion surgery with a reduction in incision size, iatrogenic soft tissue injury, operative time, estimated blood loss (EBL), postoperative pain, narcotic consumption, and perioperative complication rates compared to the open counterpart.11–17 The advantages afforded by the MIS TLIF technique have allowed a shift in surgical paradigm for several pathologic processes formerly treated via the open technique and have resulted in faster recovery time and a decreased length of hospitalization, among others.18–21
Several studies have examined the use of the MIS TLIF technique on low-grade DS (Meyerding grades I and II); however, the best approach for the surgical management of low-grade IS has not been fully elucidated.3 Similarly, few studies have compared the surgical outcomes of MIS TLIF between low-grade IS and DS. These studies are limited by underpowered patient populations, composed mainly of grade I spondylolisthesis patients.22–27 Therefore, the purpose of this study was to compare clinical outcomes of patients with IS and DS after MIS TLIF in the largest comparative study of its kind.
MATERIALS AND METHODS
Patient Population
After institutional review board approval (ORA#14051301), a prospectively maintained surgical database at a single academic institution was retrospectively reviewed. Patients who underwent a primary single-level MIS TLIF for the treatment of IS and DS between 2007 and 2015 were identified. Patients were excluded from the analysis if they radiographically demonstrated a spondylolisthesis grade III or above, were diagnosed with both IS and DS, or had less than 1 year of postoperative follow up.
Demographic and Outcome Analysis
Patients were stratified into either the IS or DS cohort (Figure 1) based on their presenting diagnosis. Patients were then analyzed by the following demographic, comorbidity, and perioperative variables: age, gender, body mass index (BMI, nonobese [BMI < 30], obese [BMI ≥ 30]), smoking status, and Charlson Comorbidity Index (CCI). Perioperative variables included spondylolisthesis level and grade, operative time, EBL, length of hospital stay (LOS), complication, arthrodesis, and revision rates, as well as the preoperative, postoperative, and change from preoperative to postoperative visual analogue scale (VAS) scores. Computed tomography (CT) scan was used to determine arthrodesis, defined by the presence of bony bridging on 3 sequential cuts in the sagittal and coronal planes. The presence of subchondral cysts, end plate sclerosis, or haloing around the interbody cage(s) or pedicle screws were also evaluated for possible pseudarthrosis. It is standard practice for the senior surgeon to obtain postoperative CT scans at the 6-month postoperative visit after all TLIFs. Additional CT scans are obtained at the 1-year postoperative visit if the patient underwent revision procedure, demonstrated incomplete fusion on the 6-month CT scan, or remained symptomatic.
Surgical Technique
Surgical treatment was based on the unique pathomechanical differences between IS and DS as well as the increasing degree of instability associated with progressively worsening grades of listhesis.28 Grade I and II DS and grade I IS patients were treated with MIS TLIF via a unilateral approach. Grade II IS patients were treated with a bilateral tubular approach. After paraspinal skin incision, the primary approach was obtained using the Wiltse technique under fluoroscopic guidance. For patients with either grade I or II DS, unilateral laminectomy and facetectomy were performed through a single 21-mm nonexpandable tubular retractor. For patients with grade I IS, unilateral laminectomy and facetectomy were performed, and for those with grade II IS, bilateral laminectomy and facetectomy were performed through bilateral 21-mm nonexpandable tubular retractors. After decompression, the intervertebral disc was identified, incised and removed; the end plates and bone graft were prepared. A mixture of autograft obtained from the laminectomy and facetectomy was morselized and mixed with 5 cc of bone marrow aspirate from the cannulated pedicles and 15 cc of allograft cancellous bone. This bone graft mixture was impacted into the front of the disc space before interbody cage placement. Additionally, the single interbody cage was prepared with an extra small kit rhBMP-2 (2.1 mg), and the bilateral interbody cages were prepared with a small kit rhBMP-2 (4.2 mg) divided between the 2 cages. A single interbody cage was impacted into place for grade I IS and grades I and II DS cohorts and bilateral interbody cages for grade II IS (Figures 2A and B). Although placement of bilateral interbody devices is often associated with a posterior lumbar interbody fusion, the procedure involved bilateral laminectomies and facetectomies allowing for a transforaminal approach through Kambin's triangle. Percutaneous pedicle screws were placed bilaterally over guide wires. No posterolateral fusion was performed, and preservation of the midline musculature and ligamentous structures was achieved. Of note, rhBMP-2 was used as an off-label bone graft substitute in all MIS TLIFs performed.
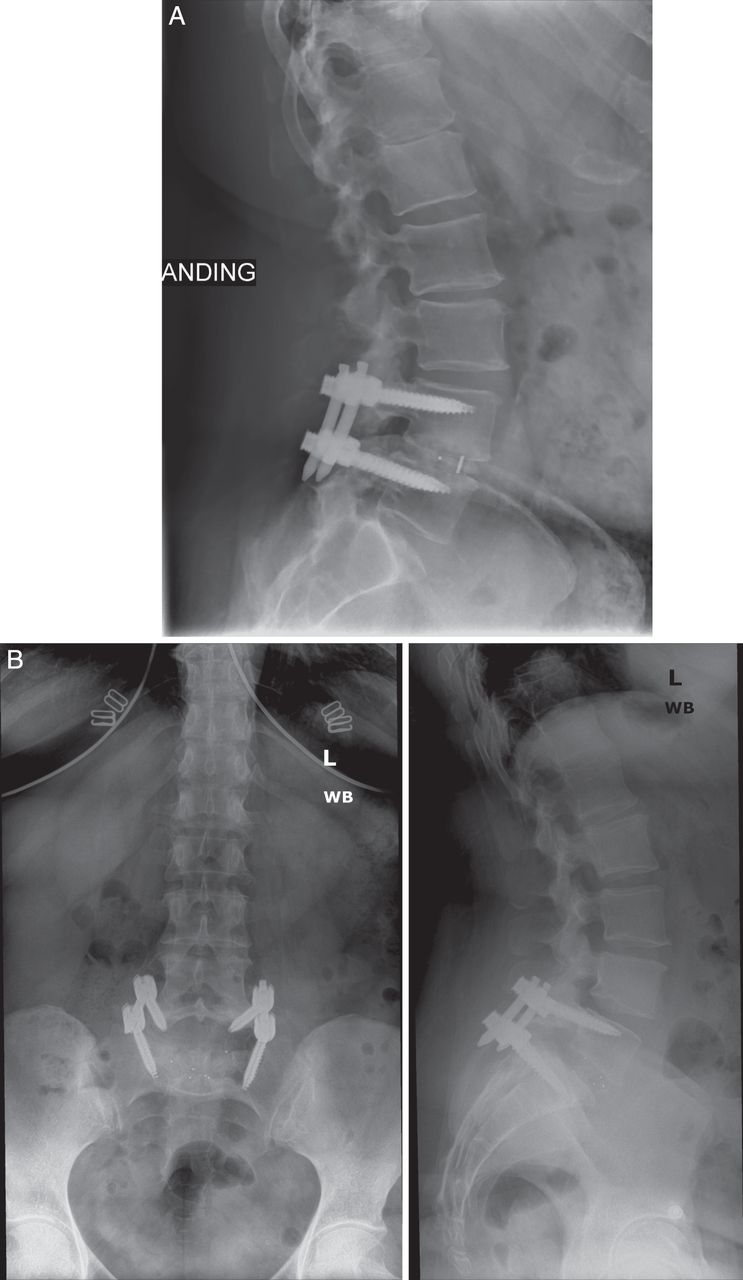
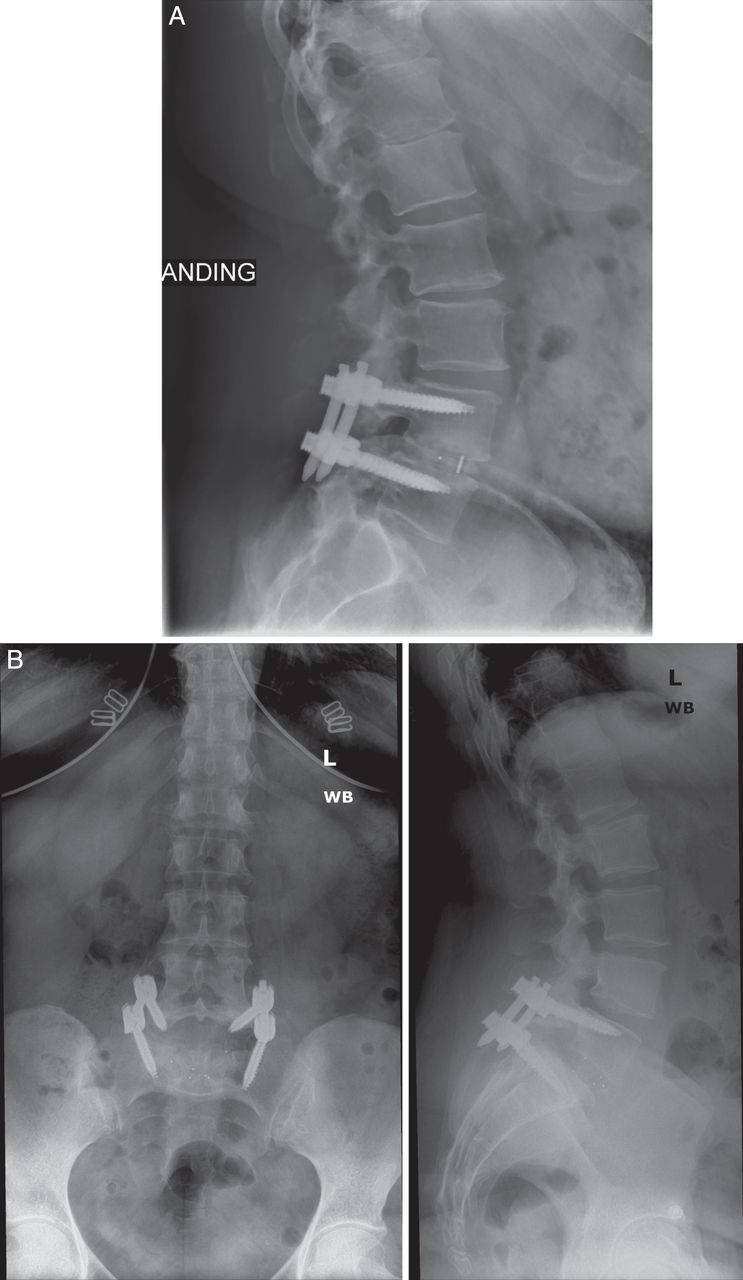
Postoperative radiographs demonstrating (A) a unilateral interbody cage in a patient with grade I degenerative spondylolisthesis and (B) a bilateral interbody cage in a patient with grade II isthmic spondylolisthesis.
Statistical Methods
Statistical analysis was performed using Stata/MP 13.1 for Mac (StataCorp LP, College Station, TX). Differences between patients in terms of demographics, comorbidities, and procedural characteristics were tested for using Pearson's χ2 test (for categorical characteristics) and independent sample t tests (for continuous characteristics). Multivariate linear regression (for continuous variables) and Poisson regression with robust error variance (for binary outcomes) were used to test for differences between IS and DS patients with respect to procedural variables (operative time, EBL, LOS, postoperative VAS, change in VAS) and postoperative outcomes (complication, arthrodesis, and revision rates).29 These regressions were each adjusted for baseline patient characteristics. Each of these analyses were performed when first comparing IS and DS as well as within the subgroup analyses between grade I IS and DS and grade II IS and DS. A P value< .05 was used to determine statistical significance.
RESULTS
Primary Analysis
A total of 223 patients were identified, of which 62 (27.8%) were diagnosed with IS and 161 (72.2%) were diagnosed with DS. Baseline characteristics are detailed in Table 1. The IS cohort was younger (47.3 ± 13.9 versus 56.9 ± 11.2 years, P < .001), had a lower comorbidity burden (2.2 ± 2.0 versus 3.6 ± 2.2, P < .001), and had a greater incidence of grade II spondylolisthesis (64.5% versus 7.5%, P < .001) at L5–S1 (71.0% versus 17.4%, P < .001) than the DS cohort. There were no significant differences in gender, body mass index, smoking status, or preoperative VAS pain scores between the 2 cohorts (P > .05).
Baseline characteristics.a
Table 2 contains perioperative and postoperative outcome comparisons. Patients with IS experienced longer operative times (146.6 ± 44.6 versus 122.6 ± 41.0 min, P < .001) compared to the DS cohort. The remainder of the perioperative and postoperative outcomes were similar between the IS and DS cohorts. These variables include: LOS; postoperative VAS pain scores at 6 weeks, 12 weeks, and 6 months; change in VAS from preoperative to postoperative time points; complication; arthrodesis (Figures 3A and B); and revision rates. Of note, a 73-year-old female experienced motor and sensory neuropraxia after her primary procedure. Weakened dorsiflexion and left dorsal foot numbness correlated with a reduced compound muscle action potential amplitude in the left common peroneal nerve on electromyography (EMG). The patient underwent a revision decompression for recurrent lateral stenosis at L4–L5, left lower extremity radiculopathy, and dorsiflexion weakness. After revision operation, the patient was reevaluated with EMG and noted to have denervation changes in the peroneal muscle, distal to the fibular head. Improved dorsiflexion strength was noted by 18 months postoperatively.
Outcomes.a

Postoperative (A) coronal and (B) sagittal computed tomographic scans demonstrating a bilateral interbody cage in a patient with grade II isthmic spondylolisthesis.
Of the 62 patients diagnosed with IS, 22 (35.5%) and 40 (64.5%) were radiographically diagnosed with grade I and grade II IS, respectively. Of the 161 patients with DS, 149 (92.5%) and 12 (7.5%) were radiographically diagnosed with grade I and grade II DS, respectively.
Subgroup Analysis
Subgroup analysis was performed comparing the grade I IS and DS subgroups as well as grade II IS and DS subgroups. The grade I IS cohort was younger (P < .001), had a lower comorbidity burden (P = .003), a greater incidence of spondylolisthesis at the L5–S1 vertebral level (P < .001; Table 3), and experienced longer operative times (P = .030) than the grade I DS cohort (Table 4). The remainder of the perioperative and postoperative outcomes did not differ between cohorts (Table 4).
Baseline characteristics of subgroup analyses.a
Outcomes of subgroup analyses.a
The grade II IS cohort was younger (P = .001), had a lower comorbidity burden (P < .001), a greater incidence of spondylolisthesis at the L5–S1 vertebral level (P < .001; Table 3), and experienced longer operative times (P = .011) than the grade II DS cohort (Table 4). The remainder of the perioperative and postoperative outcomes did not differ between cohorts (Table 4).
DISCUSSION
Surgical management of symptomatic low-grade spondylolisthesis using MIS TLIF is well established in the current literature.4,21–26,30–33 While evidence supporting the use of MIS TLIF for treatment of low-grade DS is robust, literature regarding the treatment of IS remains controversial, and data comparing MIS TLIF for low-grade IS and DS are limited.4,22–25,32,34
The results of this study suggest that MIS TLIF is a safe and effective procedure when using a single interbody cage and a unilateral tubular approach for grade I IS and grades I or II DS patients. Additionally, using bilateral interbody cages for grade II IS results in equivalent surgical outcomes. IS patients were statistically younger, had a lower comorbidity burden, and experienced spondylolisthesis at a more caudal vertebral level when compared to the DS cohort, but the most significant difference was an increased operative time. There are many explanations for this observation. The removal of excess fibrous connective and chondroid tissues from the fracture site often increases the operative times when compared to the DS dissection.35 Further, with disruption of the posterior arch and increased slippage, the anatomic relationships become further distorted and more difficult to visualize through a tubular approach. Moreover, grade II and higher IS requires a more extensive decompression that involves bilateral tubular approaches, laminectomies, and facetectomies in order to adequately alleviate foraminal stenosis and to obtain adequate disc space distraction. More extensive releases result in greater instability often requiring additional instrumentation (ie, bilateral interbody cages); prolonged operative times have been noted in several studies using this bilateral technique.35,36 Additionally, Pan et al35 reported that the bilateral technique was associated with increased intraoperative blood loss. Lastly, it has been well established that the MIS TLIF is associated with a significant procedural learning curve.14–17 As the surgeon becomes more comfortable with the MIS technique, the prolonged operative time and EBL may normalize.35 While there are many reasons for the observed increase in operative time, the clinical significance of this finding remains poorly understood as LOS, perioperative pain scores, and arthrodesis, complication, and revision rates were similar between cohorts.
The present study supports the results of several others. Before the adaptation of modern MIS techniques for TLIF, Lauber et al37 performed a prospective study comparing the clinical and radiographic outcomes between low-grade IS and DS after a traditional open TLIF. The authors reported comparable initial improvement in Oswestery Disability Index (ODI), VAS pain scores, and short-term radiographic outcomes at all follow-up visits before 2 years. The authors demonstrated a cumulative 94.8% arthrodesis rate and concluded that open TLIF was a safe and effective method to treat low-grade IS and DS.
In 2010, Wang et al27 performed a prospective analysis of clinical and radiographic factors between 39 IS and 46 DS cases after MIS and open TLIF. The authors observed no significant difference in operative time, VAS, or ODI preoperatively and at final follow up. However, the MIS cohort experienced reduced EBL, total blood transfusions, LOS, and pain in the immediate postoperative period as demonstrated by a reduced VAS score. The authors concluded that MIS TLIF demonstrated superior outcomes for low-grade IS and DS populations compared to the open cohort. Their investigation was limited, however, by the lack of stratification into grades I and II spondylolisthesis.
In a 2015 study performed by Kim et al,26 the authors compared clinical and radiographic outcomes between low-grade IS and DS after MIS TLIF in 41 patients (18 IS and 23 DS). The authors used a unilateral approach with single interbody cage placement and bilateral instrumentation resulting in similar clinical outcomes between cohorts. In contrast to the current study, the authors observed no difference in operative time between cohorts, as well as reduced arthrodesis rates in the DS cohort. The authors also reported VAS and ODI pain scores, and perioperative and postoperative clinical outcomes were no different between cohorts; however, of the radiographic parameters measured, the IS cohort demonstrated a greater restoration of disc height compared to the DS cohort. The authors concluded that MIS TLIF was an effective treatment option for low-grade IS and DS. However, the study was severely limited by the underpowered patient population. Only 2 of the 41 total patients were diagnosed with grade II spondylolisthesis.26 Based on the limited scope of pathology examined in the study of Kim et al, the current study aimed to analyze the outcomes between grade II IS and DS after MIS TLIF, endorsing the successful application of MIS TLIF for all low-grade patients.
Among the 223 patients included in the current study, 62 (27.8%) were diagnosed with IS and 161 (72.2%) were diagnosed with DS. To the best of the authors' knowledge, this is the largest study comparing low-grade IS and DS after MIS TLIF. The younger age, lower comorbidity burden, and difference in location of spondylolisthesis experienced by the IS compared to the DS cohort is intuitive and can be explained by the pathologic variation and age of presentation. IS and DS most commonly present in healthy adolescents at L5–S1, and in elderly women at L4–L5, respectively.1,3,4 The differences in age and location of spondylolisthesis observed between cohorts are therefore characteristic of their pathologic processes. Similarly, the age difference between cohorts explains the significant difference in comorbidity burden, as an increase in age is associated with increasing prevalence, number, and severity of comorbid conditions.38
This study has several limitations. Although different procedural techniques may have been used for each spondylolisthesis grade, a single surgeon performed them. This ultimately cut down on the operative variability within patients with the same diagnosis. Additionally, the consistency between operative outcomes suggests the successful application of both techniques among the patient population examined. However, the procedures were used on patients with varying pathologic difficulty, necessitating a subgroup analysis among spondylolisthesis grades. Secondly, the techniques described were all performed by a single surgeon at a single academic institution, limiting the generalizability. Finally, the study was performed retrospectively, introducing possible selection and information bias.
The results of this study demonstrate that MIS TLIF is an effective treatment option for both grade I and II DS and IS patients, despite the reduced stability inherent with IS. Although principally the senior surgeon's preferred technique, using a bilateral approach and bilateral interbody cages safely and effectively treated grade II IS with equivalent clinical outcomes compared to a unilateral approach and single interbody cage for grade I IS and DS and grade II DS. Future studies prospectively assessing additional risk factors as well as detailed radiographic analyses, including lordotic angle and subsidence rate, will allow for more accurate determination of the best candidates for MIS TLIF as the treatment for IS.
Footnotes
Disclosures and COI: No funds were received in support of this work. No benefits in any form have been or will be received from any commercial party related directly or indirectly to the subject of this manuscript. No Food and Drug Administration device or drug status to report. We will not discuss unlabeled or investigational uses of any commercial product or device.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.