


Abstract
Background Revision spinal deformity surgery has a high rate of complications. Fixation may be challenging due to altered anatomy. Screws through a fusion mass are an alternative to pedicle screw fixation.
Objective The purpose of this retrospective study was to further elucidate the safety and efficacy of fusion mass screws (FMSs) in revision spinal deformity surgery.
Design Retrospective case series.
Methods Fifteen freehand FMSs were placed in 6 patients with adult spinal deformity between 2016 and 2018 by the senior author. FMSs were combined with pedicle screws, at times at the same level. FMSs were used to save distal levels from fusion, assist in closing a 3-column osteotomy and provide additional fixation in cases of severe instability. Computed tomography (CT) was used to assess bone mineral density (BMD) and thickness of each fusion mass preoperatively along with accuracy of FMS placement postoperatively.
Results The mean BMD of the fusion mass was 397 Hounsfield units (HU; range: 156–628 HU). The mean AP thickness of the fusion mass was 15.5 ± 4.8 mm (range: 8.6–24.4 mm). The mean FMS length was 35.3 ± 5.5 mm (range: 25–40 mm). There was no evidence of FMS loosening, breakage, or pseudarthrosis at latest follow-up (mean: 2.2 years, range: 1.4–3.1 years). No neurologic deficits were observed. 1/15 screws had a low-grade breach into the canal (<2 mm). No patients required revision surgery.
Conclusion FMSs may be used to augment fixation in revision spinal deformity cases when pedicle screw placement may be challenging. FMSs may also provide an additional anchor at levels with pedicular fixation.
Level of Evidence 3.
Introduction
Rates of revision in patients undergoing correction for adult spinal deformity have been found to range from 9% to 19.9%.1–3 A substantial portion of these cases require a revision of the old instrumentation.2 Revision spinal deformity instrumentation in a previously fused spine often presents a number of challenges.4 Conventional landmarks for pedicle screw placement may be obscured or nonexistent, increasing the potential for spinal cord or nerve root injury.4,5 Altered tactile feedback, complex anatomy, and dysplastic pedicles can further confound this process. These patients often require substantial deformity correction, which makes stable points of fixation paramount.4 A study of 10,912 patients demonstrated a statistically significant increase in risk of procedure-related complications, neurological complications, and vessel/nerve injury in the revision setting compared to the primary setting.6 A large report by the Scoliosis Research Society looking at 108,419 procedures found a 41% higher rate of a new neurological deficit in the revision setting.7
While techniques have been described to improve the accuracy of pedicle screw placement, pedicle screw misplacement has still been shown to occur 2.0% to 18.6% of the time.5,8,9 Furthermore, some of those techniques rely on computer-aided navigation and stereotactic image guidance, which may not be widely available.8,10 An additional method of screw fixation may have considerable utility where the traditional pedicle screw fixation appears challenging.
Fusion mass screws (FMSs) can provide an additional anchor for fixation in patients with a prior history of spinal fusion. These are screws that are placed coronally or obliquely across the posterior bone formed as a result of a prior spinal fusion. These screws may provide added stability while reducing the risk of a neurological injury during revision surgery. Two cases have been previously described in the literature, with successful results.4 We aim to further elucidate the use of FMSs in revision spinal deformity surgery.
Methods
A retrospective review was conducted of 6 patients who underwent revision spinal deformity surgery with FMS placement between 2016 and 2018 (Table 1) Our hospital’s Institutional Review Board had approved this study, and a waiver of informed consent was granted. Pedicle screws were preferentially placed when their safe placement was considered possible based on the preoperative imaging. Bone mineral density (BMD) and dimensions of the posterolateral fusion masses at different levels were determined on the preoperative CT to assess the possible levels for FMS placement. FMS screws were placed to augment the fixation with or without concurrent pedicle screws present at the same level. The indication for a revision was a fusion mass fracture in 2 cases, Charcot arthropathy in 1 case, distal junctional failure in 1 case, and iatrogenic sagittal imbalance in 2 cases. Four out of 6 patients had a 3-column osteotomy. Patients were followed clinically to monitor for pain, disability, or neurological symptoms. Screw placement and presence of pseudarthrosis were evaluated on postoperative CT scans.
Clinical data for 6 adult spinal deformity patients treated with FMS fixation during revision spine surgery.
FMS Technique
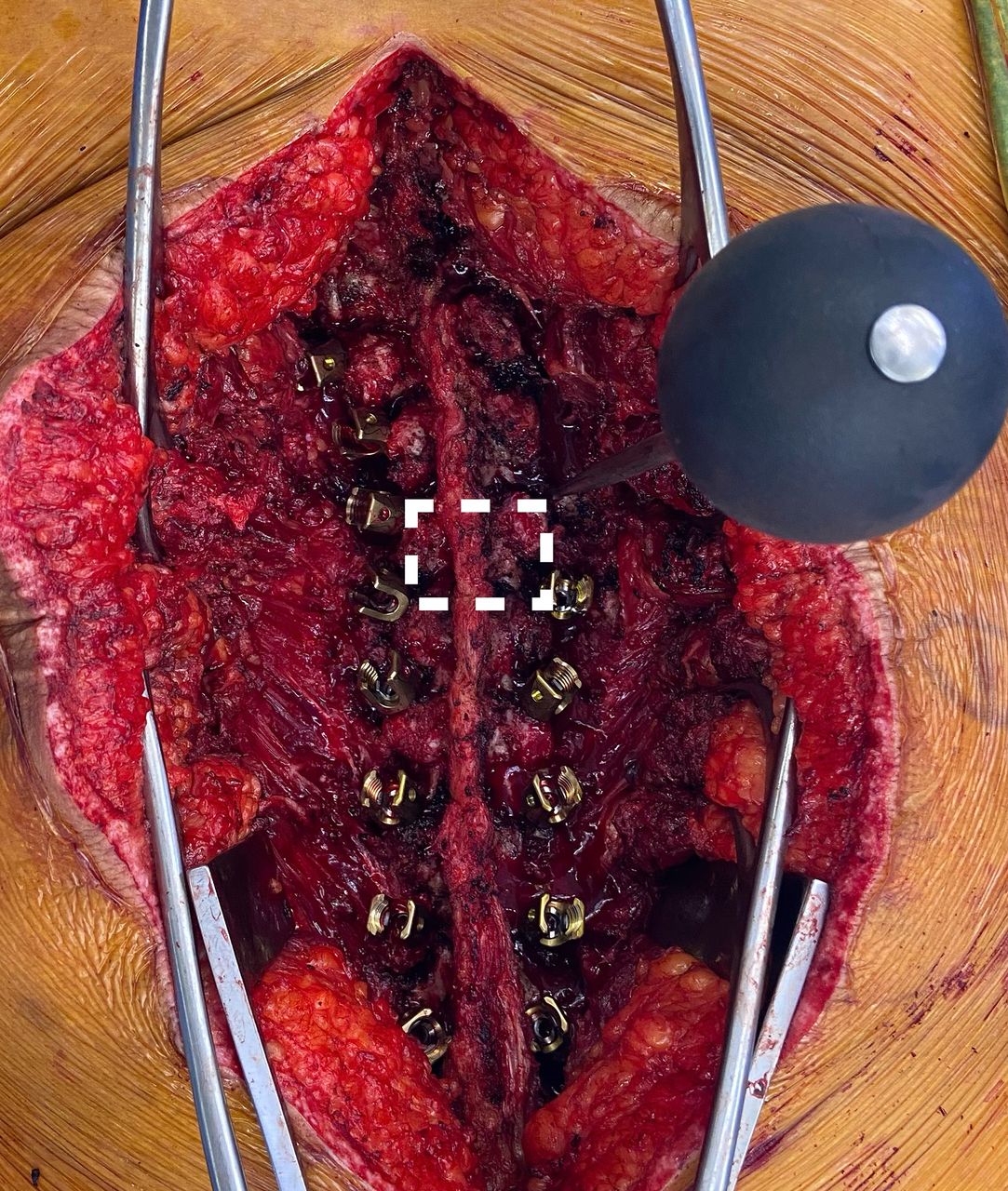
Standard 5.0- or 5.5-mm pedicle screws were placed medially across the posterolateral fusion mass (Figure 1). The starting points were chosen to line up with pedicle screws above and below the FMS to allow for easy connection to the rod. In other instances, FMSs were connected to other levels using an accessory rod construct. Adjacent pedicle screws were placed prior to the FMSs. FMSs were preferably inserted from the convex side of the curve since severe rotation of the vertebrae relative to the chest wall may result in an unsafe trajectory from the concave side.4 Since fusion masses are thinnest at the level of the interlaminar space, FMSs were placed proximal to this region. Screw position was confirmed using orthogonal fluoroscopic views. A high-speed burr was used to establish a starting point at a depth of approximately 5 mm. A standard pedicle probe was then inserted and directed medially across the fusion mass. A flexible ball-tipped probe was used to assess for cortical breaches, most importantly of the ventral wall adjacent to the spinal canal. After measuring the depth and under-tapping the screw path, standard 5.0-mm or 5.5-mm pedicle screws ranging from 25 mm to 50 mm in length were placed within the fusion mass. Somatosensory evoked potentials (SSEP) and motor-evoked potentials were monitored and recorded throughout each case. The threshold for stimulation was above 15 milliamps for all screws.
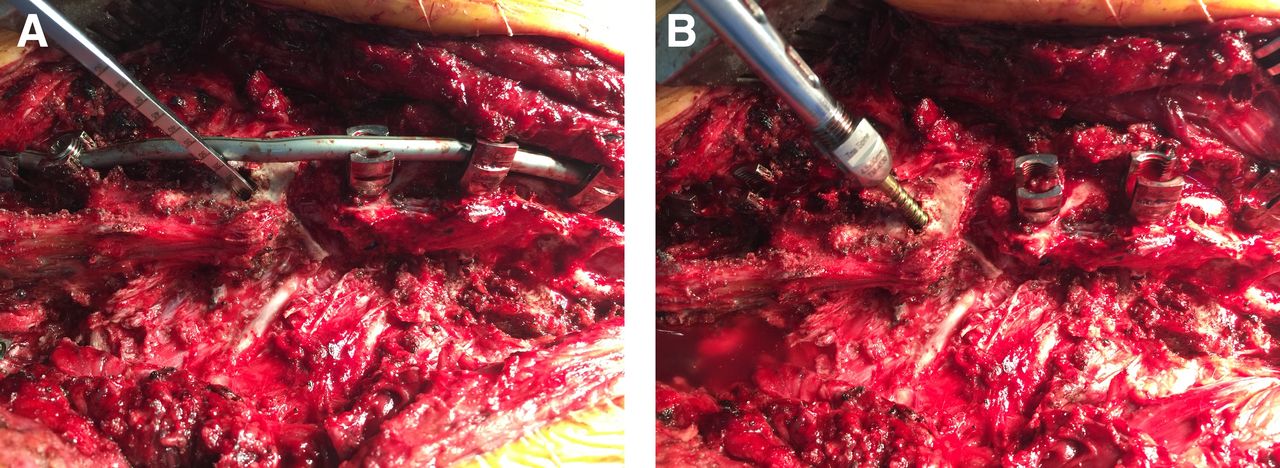
(A) Intraoperative photograph of fusion mass screw cannulation lateral to medial immediately inferior to a chevron posterior column osteotomy using a Lenke probe. (B) Intraoperative photograph of polyaxial screw placement into the fusion mass.
Results
Fifteen freehand FMSs were placed in 6 cases of adult spinal deformity. In all cases, FMSs were combined with pedicle screws, and 45% of the screws were placed concurrently with pedicle screws at the same level. All screws were either 5.0 or 5.5 mm in diameter. There were no neurophysiologic alerts observed during FMS placement and no neurologic deficits or complications postoperatively. On postoperative CT, 1/15 screws had a low-grade breach into the spinal canal (Figure 2). The mean BMD of the fusion mass was 397.2 ± 144.4 HU (range: 156–628 HU). The mean AP thickness of the fusion mass was 15.5 ± 4.8 mm (range: 8.6–24.4 mm) at the level of FMS placement. The mean FMS length was 35.3 ± 5.5 mm (range: 25–40 mm) (Table 2). BMP was utilized in 5/6 cases. There was no evidence of FMS loosening, breakage, or pseudarthrosis at latest follow-up (mean: 2.2 years, range: 1.4–3.1 years). The mean preoperative Oswestry Disability Index (ODI) was 48 (n = 4, range: 32–76). The mean postoperative ODI was 45 (n = 5, range: 24–63) at a mean follow-up of 8 months. None of the 6 patients required a revision surgery to date.
Comparison of fusion mass thickness, BMD, and screw length in 6 adult spinal deformity patients treated with FMS fixation during revision spine surgery.
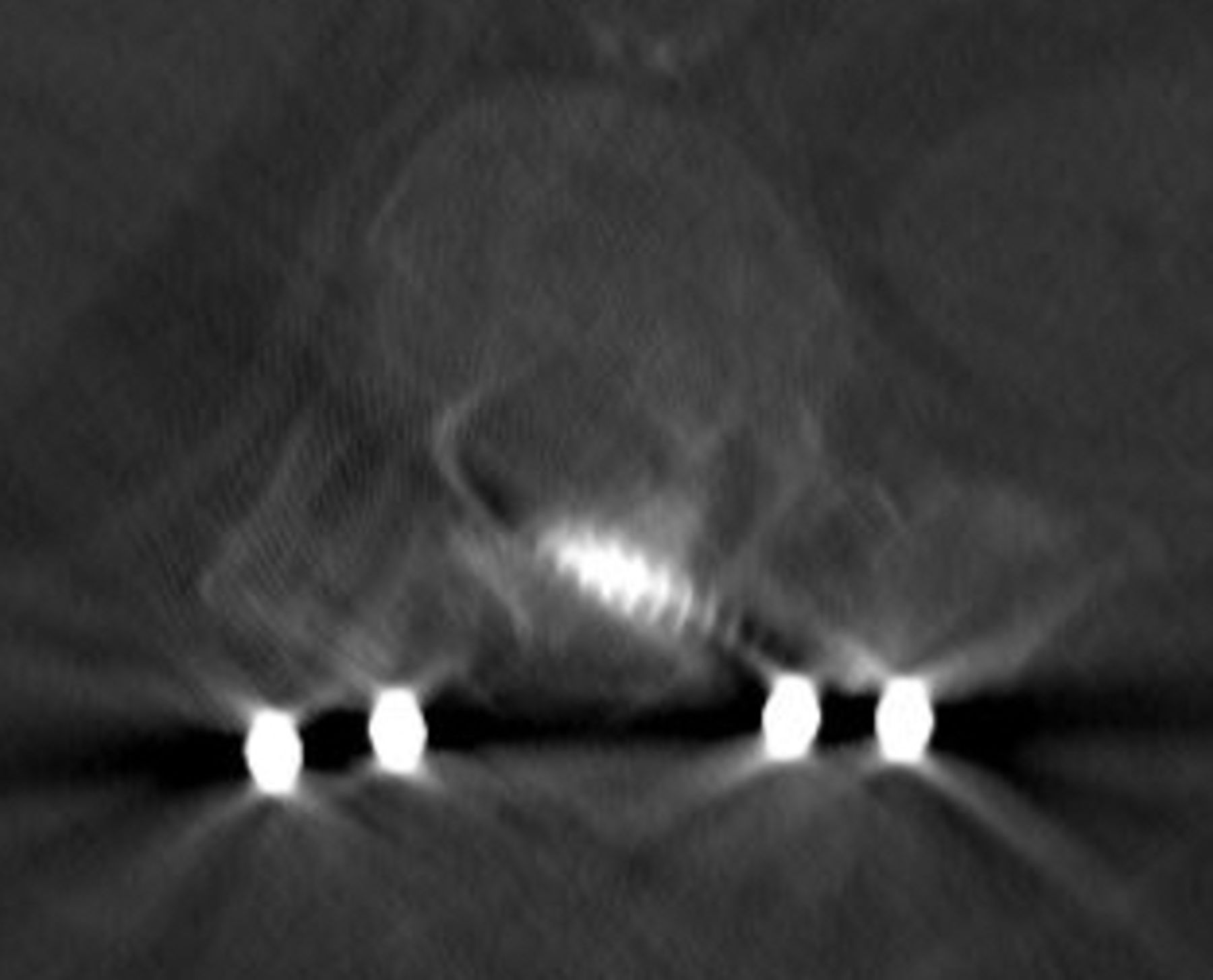
Axial computed tomography image showing low-grade breach (<2 mm) into spinal canal of a f fusion mass screw placed at T12, Case 4.
Case 1
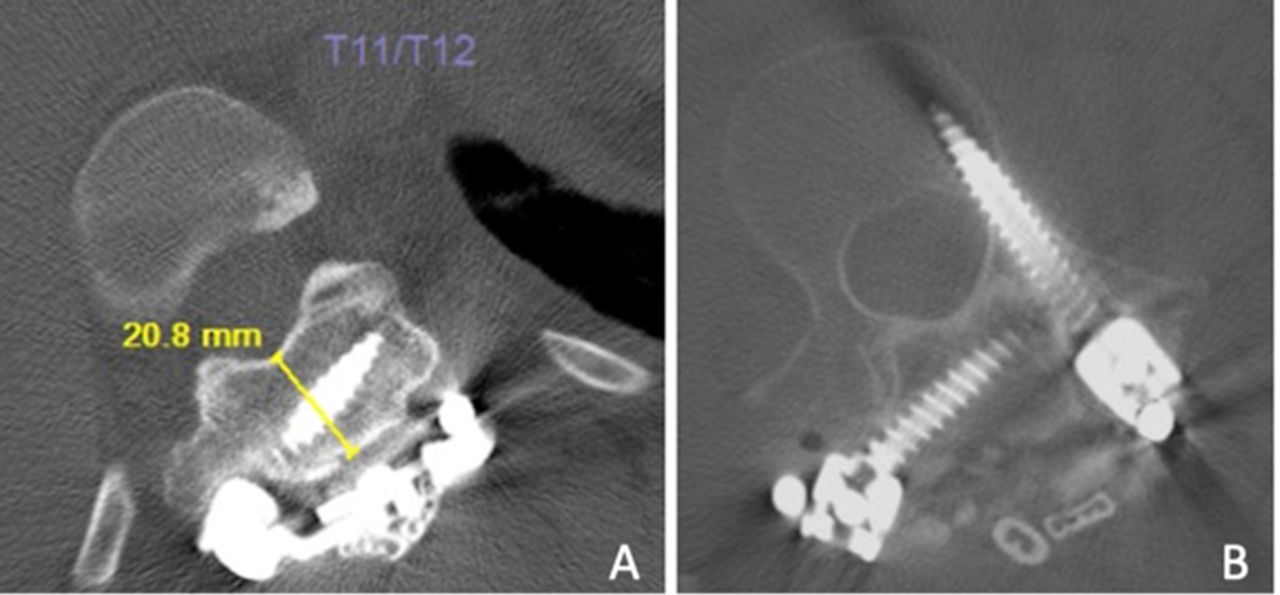
A 29-year-old man with a history of juvenile onset scoliosis and a prior posterior spinal fusion from T2 to L4 more than 10 years ago presented with a recurrent back pain and lower extremity weakness. His prior postoperative course was complicated by an infection, for which he underwent irrigation and debridement, as well as hardware revision 1 year following his original procedure. Imaging revealed a sagittal vertebral axis of 7 cm and a 15° mismatch between pelvic incidence and lumbar lordosis. He was also found to have a medial pedicle breach at one of the levels. The patient underwent a revision posterior spinal fusion from T2 to L4 with a pedicle subtraction osteotomy at L1. There was no evidence of a recurrent infection intraoperatively. Two 5.5-mm right-sided FMSs measuring 40 and 35 mm, respectively, were placed at T12 and L2 as those pedicles were found to be compromised by prior instrumentation (Figure 3). At both levels, the patient had an ample thickness and density of the fusion mass (Table 2, Figure 4). Two short rods were placed from T12 to L2, and 2 long rods were placed from T2 to L4. All screws were stimulated and found to be within normal limits. There were no neuromonitoring deficits noted. His sagittal vertebral axis was restored to within normal limits and lumbar lordosis was within 10° of pelvic incidence. There were no breaches noted on postoperative CT. At 2.4-year clinical follow-up, he demonstrated a resolution of preoperative symptoms with no new deficits or subjective complaints. The use of the FMSs below the 3-column osteotomy has augmented the distal fixation and obviated the need to go distal to L4.
Fusion mass screws (arrows) assisting in osteotomy closure and providing an additional anchor to save a distal fusion level below a 3-column osteotomy.
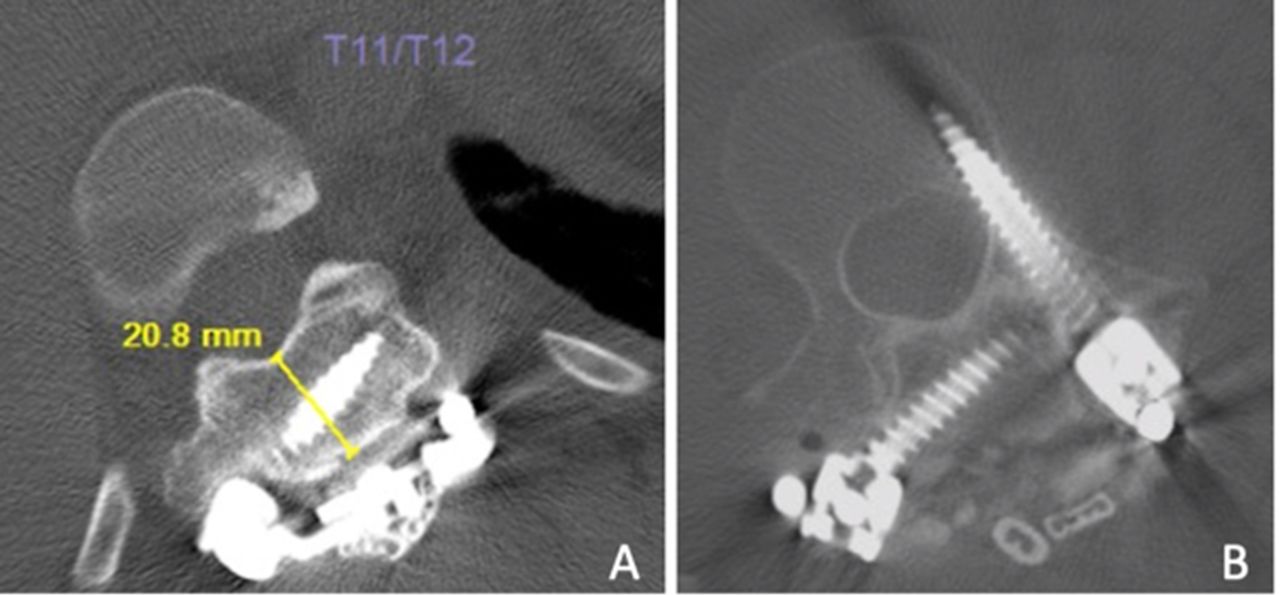
(A) Axial computed tomography (CT) image showing fusion mass screws (FMSs) placement at T12 through a thick fusion mass bed measuring 21.8 mm. (B) CT image showing right-sided FMS placement with a concurrent pedicle screw placement at L2.
Case 2
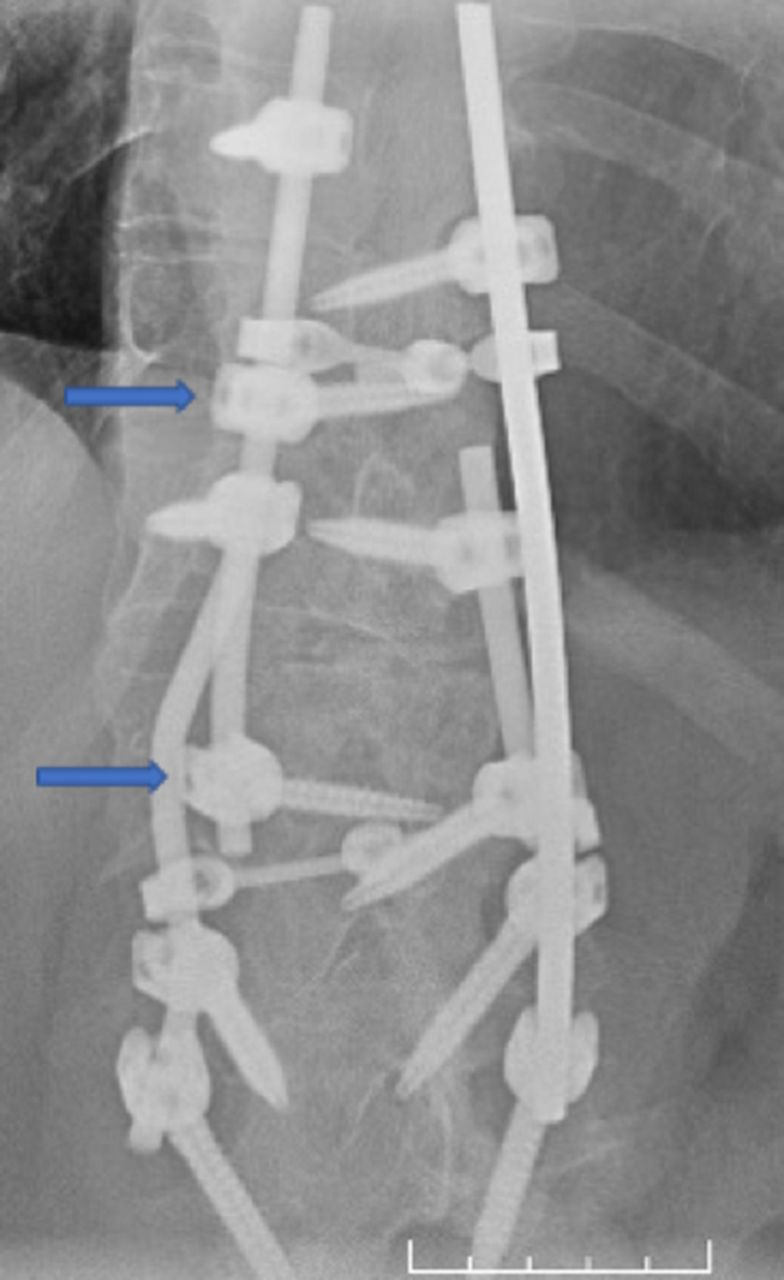
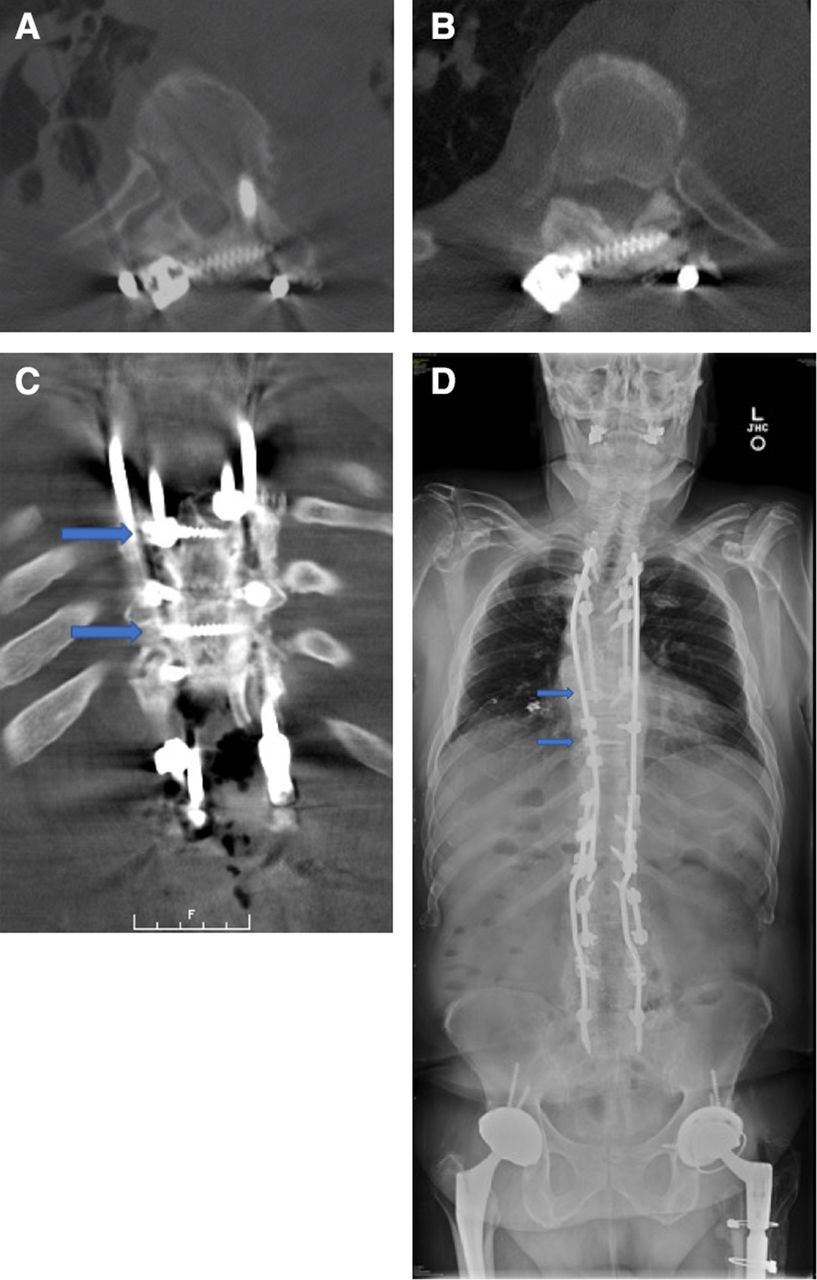
A 66-year-old man with a progressive adult spinal deformity following multiple prior surgeries including a prior pedicle subtraction osteotomy at L2 and a posterior spinal fusion from T3 to S1 4 years prior presented with a progressive back pain, difficulty walking, and recurrent fevers. His prior postoperative course had been complicated by multiple infections and symptomatic hardware requiring removal from T3 to T10. Imaging revealed evidence of recurrent osteomyelitis with a fusion mass fracture at T6 to T7. He underwent a vertebrectomy at T6 to T7 and a fusion from T3 to S1 (Figure 5). Two FMSs were placed at T8 and T10 concurrently with pedicle screws to aid with the osteotomy closure (Figure 6). At both levels, there was an ample fusion mass thickness (15.8 and 13.3 mm) to accommodate FMSs (Table 2). Screws of 40 mm were used and placed inferior to the pedicle screws at each level. A quadruple rod construct was used for the definitive fixation. All screws were stimulated and found to be within normal limits. There were no neuromonitoring deficits noted. The procedure was complicated by a right-sided pneumothorax requiring a chest tube. He had recovered well from the operation. No new neurological deficits were noted. The patient did have a chronic right lower extremity weakness that was present for several years before this operation, that had persisted. There were no breaches noted on the postoperative CT. At 1.7-year clinical follow-up, he had demonstrated improvement in his symptoms with no new deficits.
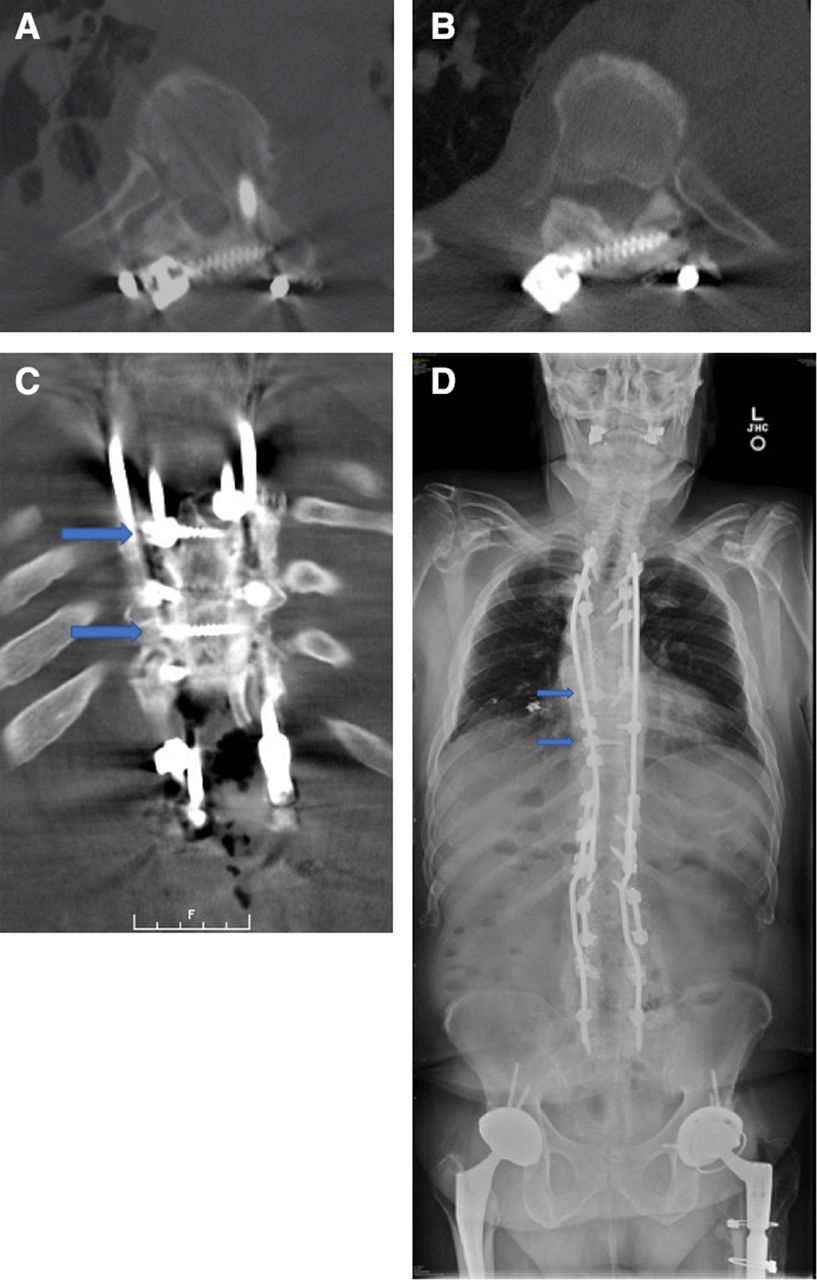
(A-C) CT and (D) full-length standing radiograph images demonstrating fusion mass screw placement at T8 and T10 (arrows) distal to the vertebral column resection to assist in osteotomy closure. Concurrent pedicle screw placement is also shown at T8.

(A) Axial computed tomography images of Patient 6 demonstrating pedicular dysplasia in the setting of neurofibromatosis-1 and juvenile onset scoliosis. (B) Fusion mass screw placed at T12. Pedicle screw placement was avoided due to dysplasia and obscured landmarks intraoperatively. The pedicles were 2.2 and 3.9 mm in width at this level.
Discussion
Spinal deformity surgery has a high rate of revision. The most common causes for revision include implant failure, infection, curve progression, pseudarthrosis, and a junctional disease.3 Patients have been shown to have a higher rate of complications and reoperation after every subsequent surgery.3,11 Each revision represents an additional significant cost burden on society.12,13 Many of these cases require a reinstrumentation with a subset of cases requiring corrective osteotomies.
Revision spinal fusion presents numerous challenges in fixation. Pedicle screws remain the gold standard of spinal fixation due to their biomechanical advantages in load-to-failure, pullout strength, and ability to control all 3 columns of the spine. However, in the revision setting, the screw placement can be more difficult due to obscured landmarks, complex anatomy, altered tactile feedback, and dysplastic pedicles. Achieving the necessary fixation in those cases has been correlated with a higher rate of neurologic and overall complications.
A mature fusion mass consists of a dense, spacious bone for screw fixation. The mean fusion mass thickness at the instrumented levels was 15.5 mm in this study, with the lowest thickness of 8.6 mm. It has been previously been described that a minimum thickness of 8 mm is required for fixation with a 4.5-mm screw.4 Screws of 5.0 or 5.5 mm were utilized for all the levels in this study. The reliability of Hounsfield units (HU) in determining BMD has previously been described.14 Measurements of 100.8 and 78.5 HU have been shown to correspond to osteopenia and osteoporosis respectively.14 The mean BMD in our series was 397 HU, with the lowest BMD of the instrumented fusion mass being 156 HU, well above the osteopenic/osteoporotic range. Although our series did not have any cases of a screw loosening or breakage, it is possible that this could be the case with lower bone densities. The placement of FMSs in the revision setting offers an increased construct strength with a potentially lower risk to the neural elements. FMSs may be used to achieve a stable fixation in revision spinal deformity cases when pedicles are dysplastic or when normal anatomical landmarks are obscured by an extensive fusion mass (Figure 6).
Additionally, FMSs may provide an additional anchor at a level where pedicle screws are already placed to increase the strength and rigidity of the construct, assist in osteotomy closure, provide an anchor for an additional rod and potentially shorten the construct. The quadruple rod constructs were used in each case of a 3-column osteotomy. In addition to the fusion mass fixation, there are several other techniques that have been described to this end.
The quadrangulation method is a freehand technique that uses instrumentation at adjacent levels to guide the placement of standard pedicle screws through a fusion mass (Figure 7).8 This technique relies on the meticulous exposure and initial screw placement at virgin levels, where landmarks are not obscured by the fusion mass. If only the fusion mass is being instrumented, the levels with the clearest landmarks are instrumented first and used as a guide for adjacent levels. The lateral aspect of the transverse processes can often be located even in the presence of most fusion masses. The fusion mass pedicle screw starting sites are located at the same distance from adjacent virgin screw holes to make a quadrangular shape (Figure 7). The general steps of a screw placement are then similar to those involving a freehand pedicle screw placement in the virgin spine. Palpation, intraoperative fluoroscopy, and stimulus-evoked electromyography (EMG) monitoring are used to confirm the accurate screw placement. Using this technique, Kim et al reported a pedicle screw misplacement rate of 1.99% on the intraoperative radiographic evaluation and 1.09% on the EMG evaluation.8 There were no screw-related neurological or vascular complications. However, there were no postoperative CT images to evaluate for a screw misplacement. They did not include any documented cases of a pedicular dysplasia. The quadrangulation method is a technically challenging, but an effective method of instrumentation in a previously fused spine.
Intraoperative photograph demonstrating identification of the pedicle screw starting point using a quadrangulation technique as described by Kim et al.8
Stereotactic image-guided navigation may also be used to aid with a pedicle screw placement in a mature fusion mass. Using preoperative CT scans, stereotaxy theoretically allows for an accurate localization of a starting point and a screw trajectory. A case series of 122 pedicle screws placed in a fusion mass using stereotaxy showed a 4.1% rate of cortical perforation on the postoperative CT imaging.9 The rate of a perforation was higher (13%) in patients with a scoliosis. None of those patients had postoperative neurological deficits. A cadaveric study using a fused spine model demonstrated a 0% perforation rate using the stereotactic CT-guided placement and an 8.33% perforation rate using the fluoroscopic-assisted placement.15 The non–image-guided group in this study had a 21.43% incidence of a cortical breach. Stereotactic guidance can certainly be helpful in the revision surgery, but the cost, added surgical time, and accessibility limit its widespread use. There is also the added downside of additional radiation to the patient.
Extrapedicular fixation using hooks into the fusion mass has also been described in the revision surgery setting. A case series of 8 patients undergoing a revision posterior spinal fusion in the setting of a spinal deformity showed that hooks can aid in providing a stable fixation at a 30-month follow-up with a concurrent pedicle screw fixation.10 The authors did not observe any hook loosening or failure at the latest follow-up.
Extrapedicular fixation in the thoracic spine with fixation of the transverse processes and vertebral bodies has also been described with good results.16 Intralaminar screw placement has also been presented as an alternative technique for a fixation in the setting of a difficult pedicle screw, in addition to a laminar hook placement in the revision setting.17 Translaminar screw placement in the thoracic spine has been described with good results for a short-segment fusion.18
Certain criteria must be met prior to a fusion mass fixation. A sufficient thickness, width, and density of the fusion mass is necessary for a safe FMS placement. A rotational deformity can further limit its placement, especially at the concavity of the curve.
Limitations of our study include a relatively small sample size and limited patient-reported outcomes. In addition, the FMSs used in our study were part of a larger construct, which included pedicle screws and interbody cages. It is unclear if FMS can be used in a standalone setting. Further studies are needed to better define the efficacy and safety of FMSs. Biomechanical testing could better elucidate the stability of those screws in various planes. While our mean follow-up was 2.2 years, a longer follow-up is likely needed to assess the stability of those screws over time.
Conclusion
FMSs can add stability and strength to spinal constructs in revision spinal deformity surgery. They provide a reliable and safe method to augment the pedicle screw fixation with a simple and cost-effective technique. They can be used at the same levels as pedicle screws for an additional fixation or without pedicle screws where their placement is difficult/impossible due to altered pedicle morphology.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Dimitriy G. Kondrashov reports receiving royalties and consulting fees from Spineart. The remaining authors have no relevant or material financial interests that relate to the research described in this paper.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.