


Article Figures & Data
Figures
- Figure 1
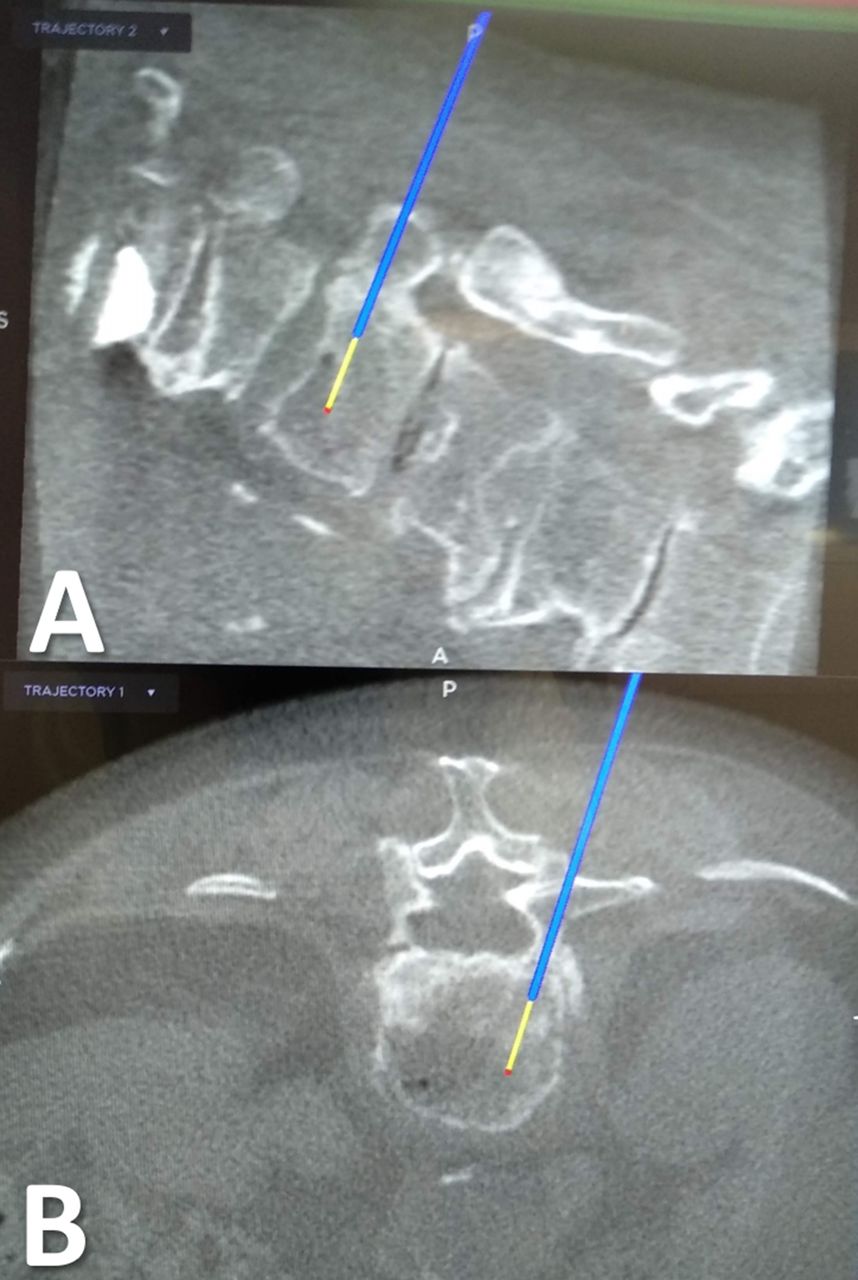
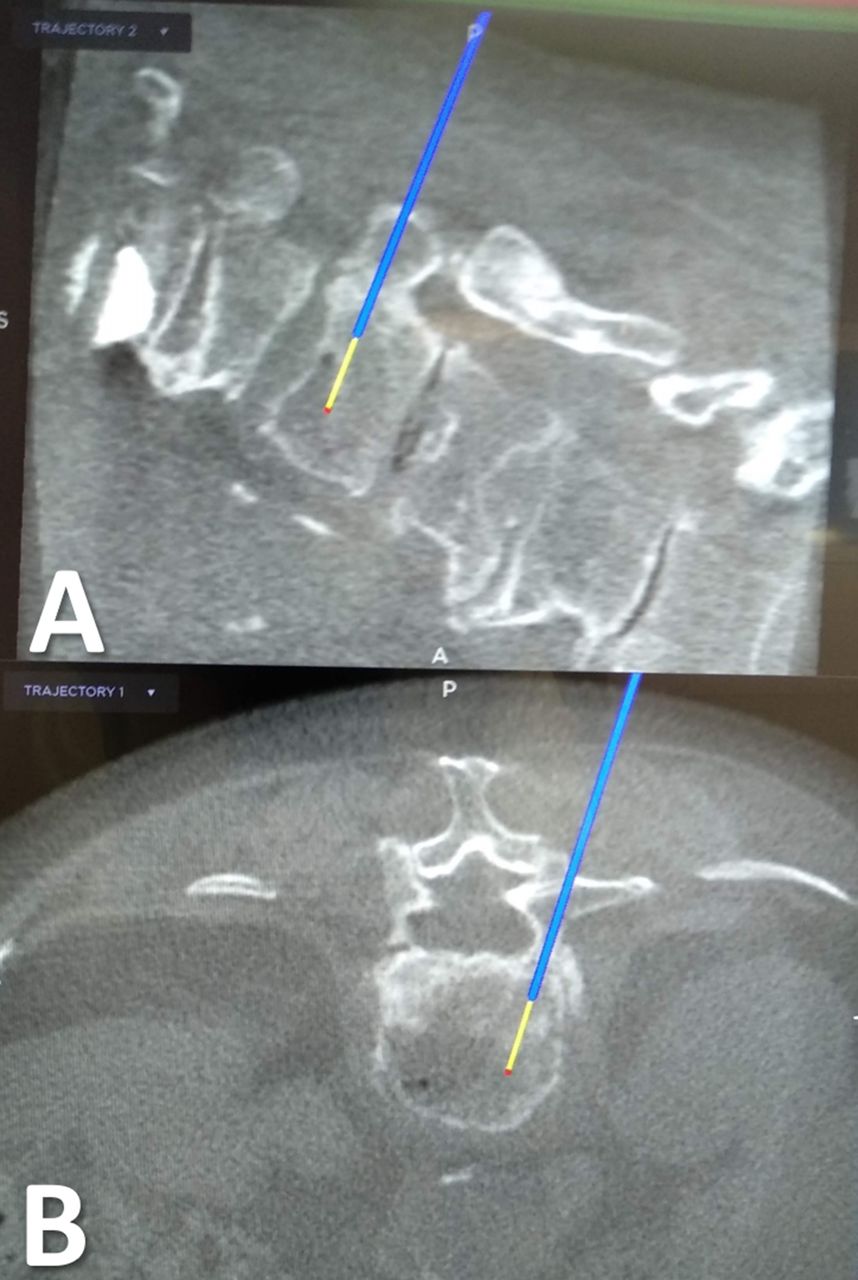
Intraoperative views of the 3D navigation on O-arm with the trajectory of the navigated Jamshidi needle. (A) Sagittal plane. (B) Axial plane.
- Figure 2
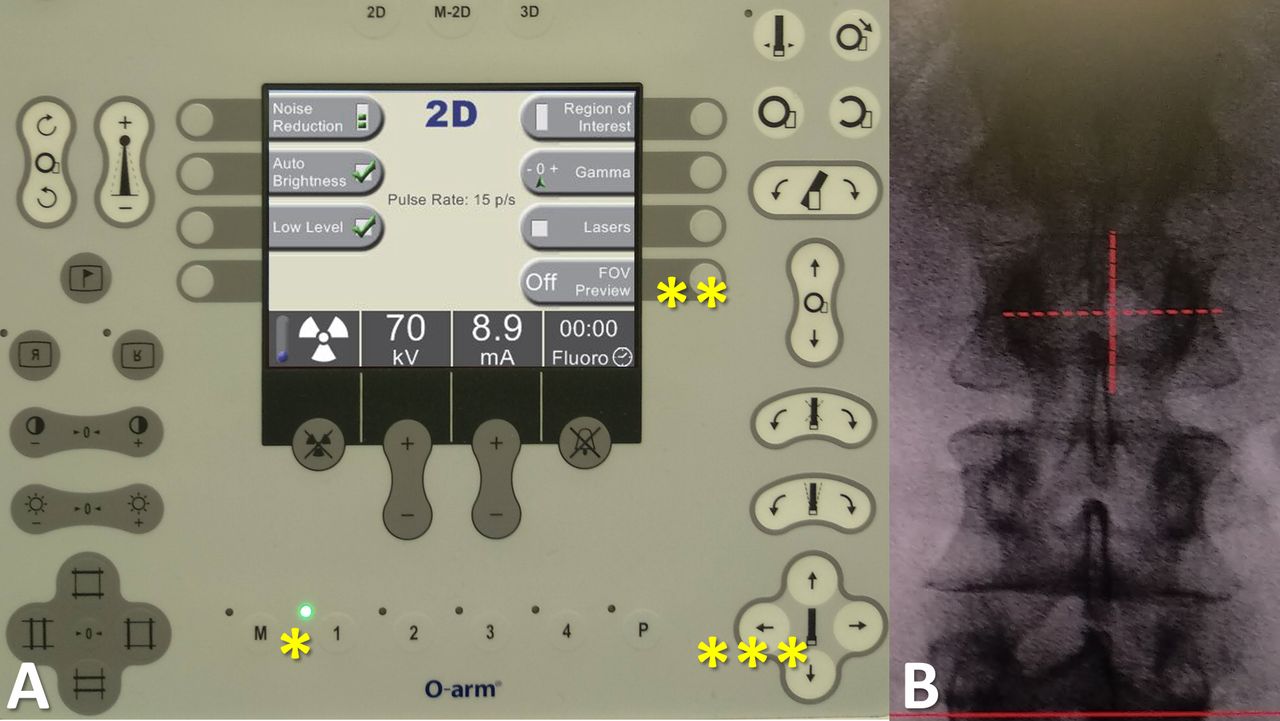
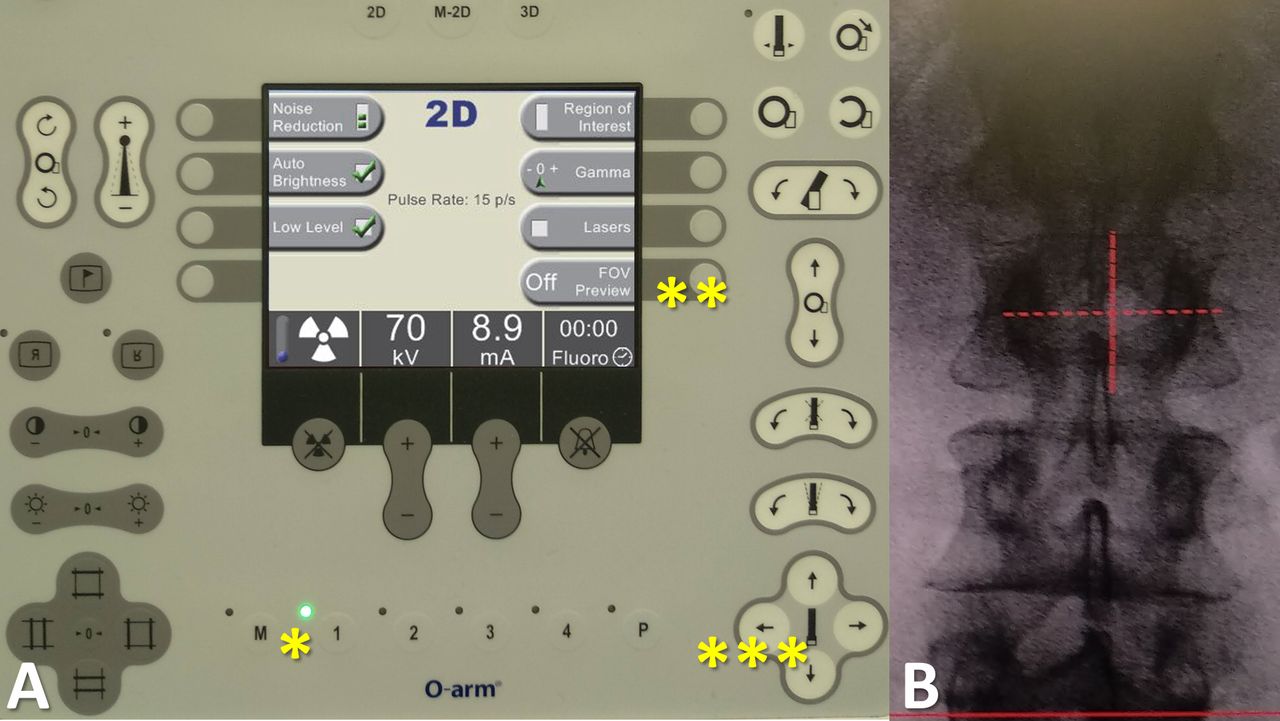
View of the control panel for settings of imaging acquisition. (A) First, an anteroposterior view can be taken. Then, the image and the O-arm position (*) are recorded. Second, the radiological technician can activate the navigation on the images by pressing the "FOV (field of view) Preview" button (**). Third, the radiological technician can navigate on the screen, using the position arrows of the control panel (***), especially in order to center the view on the fractured vertebra. (B) Finally, the lateral view is obtained and the height of the region of interest can be reached without another acquisition. Thus, a 3-dimensional navigated scan can be performed.
- Figure 3
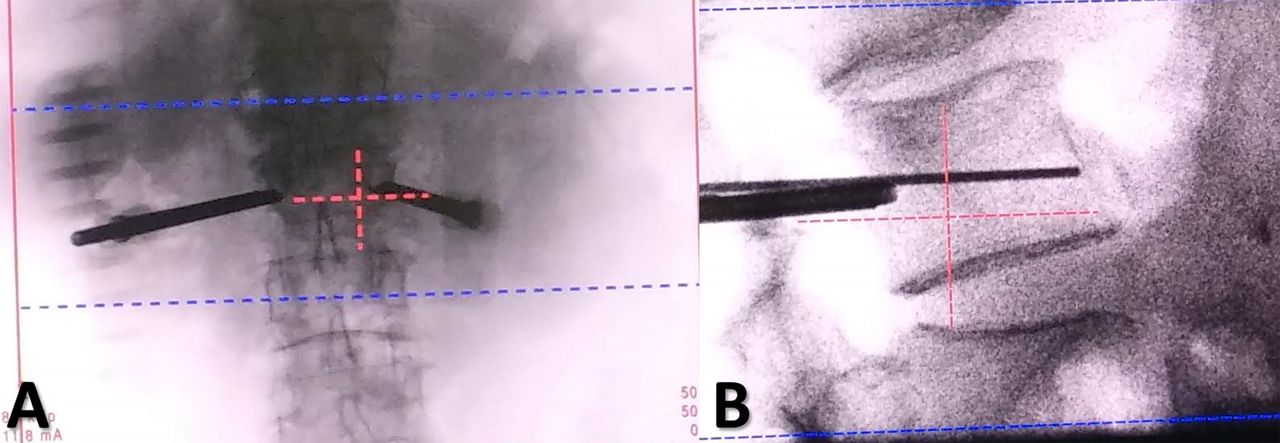
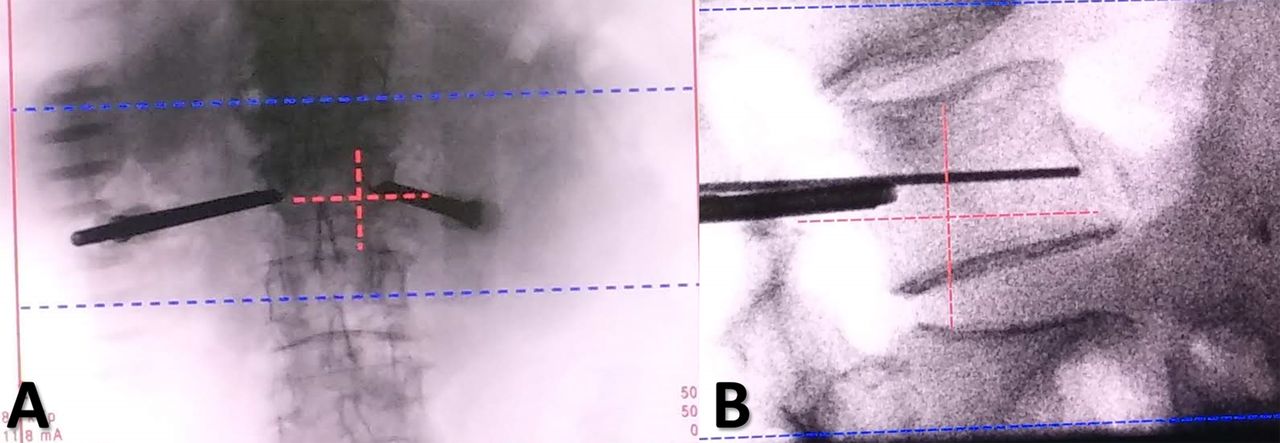
Intraoperative views of a cementoplasty procedure using the field of view (FOV) preview. (A) Anteroposterior view after placement of navigated Jamshidi needles in the fractured vertebra. (B) Lateral view. The region of interest may be reached with the FOV principle, allowing the fractured vertebra to be at the center of the image. Collimation can then be applied and also a zoom on the screen, to follow the cementoplasty procedure, and to decrease radiation exposure.
Tables
O-arm Setting Group A Group B 2D Mode (pulses/s) Fluorography (30) Low dose (15) Navigation on the FOV No Yes Collimation No Yes 3D Mode Standard Standard or low dose Abbreviations: 2D, 2-dimensional; 3D, 3-dimensional; FOV, field of view.
Patient Data Group A (n = 43) Group B (n = 27) P Value Sex ratio, female/male 25/18 19/8 0.32a Age, y, mean ± SD (range) 76 ± 11 (43–89) 67 ± 16 (34–96) 0.02b Body mass index, kg/m2, mean ± SD (range) 25 ± 3 (19–30) 24 ± 5 (17–33) 0.46b Magerl classification, n (%) 0.61a A1 50 (85) 45 (90) A2 2 (3) 2 (4) A3 7 (12) 3 (6) Location of the fractures 0.08a Thoracic spine, n (%) 32 (54) 18 (36) Lumbar spine, n (%) 27 (46) 32 (64) Operative time, min, mean ± SD (range) 34.6 ± 14.3 (15–90) 41.9 ± 19.0 (12–90) 0.13b Operative time per level, min, mean ± SD (range) 27.3 ± 10.9 (15–60) 28.9 ± 13.4 (4.4–60) 0.74b Cemented vertebrae, n 59 50 Vertebroplasties, n (%) 39 (66) 30 (60) 0.55a Kyphoplasties, n (%) 20 (34) 20 (40) Unipedicular approaches, n (%) 25 (42) 26 (52) 0.04a Surgeon experience, senior/junior 16/27 6/21 0.29a Cement volume injected, cc, mean ± SD (range) 6.8 ± 3.8 (2–18) 8.2 ± 3.5 (4–18) 0.13b Cement volume injected per level, cc, mean ± SD (range) 4.9 ± 1.5 (2–7) 5.3 ± 1.5 (2–8) 0.30b Garnier Classification Group A (n = 43) Group B (n = 27) P Valuea Cement filling n (%) 0.11 Satisfactory (Y3, Z2, Z3) 56 (95) 42 (84) - Acceptable (X2, X3, Y2) 2 (3) 1 (2) - Poor (X1, Y1, Z1) 1 (2) 7 (14) - Cement leakage, n 0.62 Spinal canal 2 1 - Intravascular 2 1 - Intradiscal 3 6 - Paravertebral 6 4 - Total, n (%) 13 (22) 12 (24) - ↵a Fisher exact test.
Radiation Exposure, mean ± SD (range) Group A
(n = 43)Group B(n = 27) P Valuea 2D Imaging duration, s 23.67 ± 15.32 (9.70–84.87) 17.82 ± 10.01 (2.82–46.07) 0.06 2D Imaging duration/level, s 18.56 ± 10.40 (4.41–62.61) 12.93 ± 8.49 (1.95–42.30) 0.02 Number of 3D acquisitions/patient 1.5 ± 1.0 (1–5) 1.4 ± 0.9 (1–4) 0.72 Dose length product, mGy·cm 534 ± 385 (175–1975) 271 ± 165 (88–769) <0.01 Dose area product, mGy·cm2 9173 ± 10,430 (1298–63,331) 1614 ± 1656 (332–9070) <0.01 Overall E, mSv 9.94 ± 6.67 (2.76–31.48) 4.34 ± 2.52 (1.41–11.33) <0.01 E per level, mSv 7.65 ± 4.82 (1.39–19.69) 2.97 ± 1.42 (0.49–5.67) <0.01 E2D, mSv 2.12 ± 2.66 (0.25–16.47) 0.37 ± 0.33 (0.06–1.72) <0.01 E3D, mSv 7.82 ± 5.67 (2.46–29.63) 3.97 ± 2.34 (1.23–10.77) <0.01 E per 3D acquisition, mSv 5.60 ± 3.14 (2.46–12.56) 2.90 ± 0.80 (1.23–4.12) <0.01 Absolute risk of radiation-induced cancer equivalent to a whole-body exposure, % 5.0 × 10−4 ± 3.3 × 10−4 (1.4 × 10−4–1.6 × 10−3) 2.2 × 10−4 ± 1.3 × 10−4 (7.1 × 10−5–5.7 × 10−4) <0.01 Abbreviations: 2D, 2-dimensional; 3D, 3-dimensional; E, effective dose.
↵a Student t test.
P Value Correlation Group A (n = 43) Group B (n = 27) Overall (n = 70) E and agea <0.01 0.13 0.31 E and body mass indexa 0.46 0.24 0.20 E and operative timea 0.28 0.01 0.43 E and imaging durationa <0.01 0.06 <0.01 E2D and imaging durationa <0.01 <0.01 <0.01 E and cement amounta 0.13 0.40 0.41 E2D and cement amounta 0.23 0.45 0.55 E and surgeon levelb 0.75 0.72 0.70 E2D and surgeon levelb 0.71 0.14 0.45 Surgeon level and operative timeb 0.74 0.61 0.41
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.